
Characterisation of Drug-Induced Liver Injury in Patients with COVID-19 Detected by a Proactive Pharmacovigilance Program from Laboratory Signals

 ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
2.2. Hepatotoxicity Signal
2.3. Detection, Evaluation and Notification
2.4. Causality Assessment
- Hepatocellular (ratio (R) ALT/alkaline phosphatase (AP) ≥ 5)
- Cholestatic (R ALT/AP ≤ 2) or Mixed (2 < R < 5).
2.5. Collection of Patient Data
2.6. Expected Sample Size and Basis for Its Determination
2.7. Data Analysis
3. Results
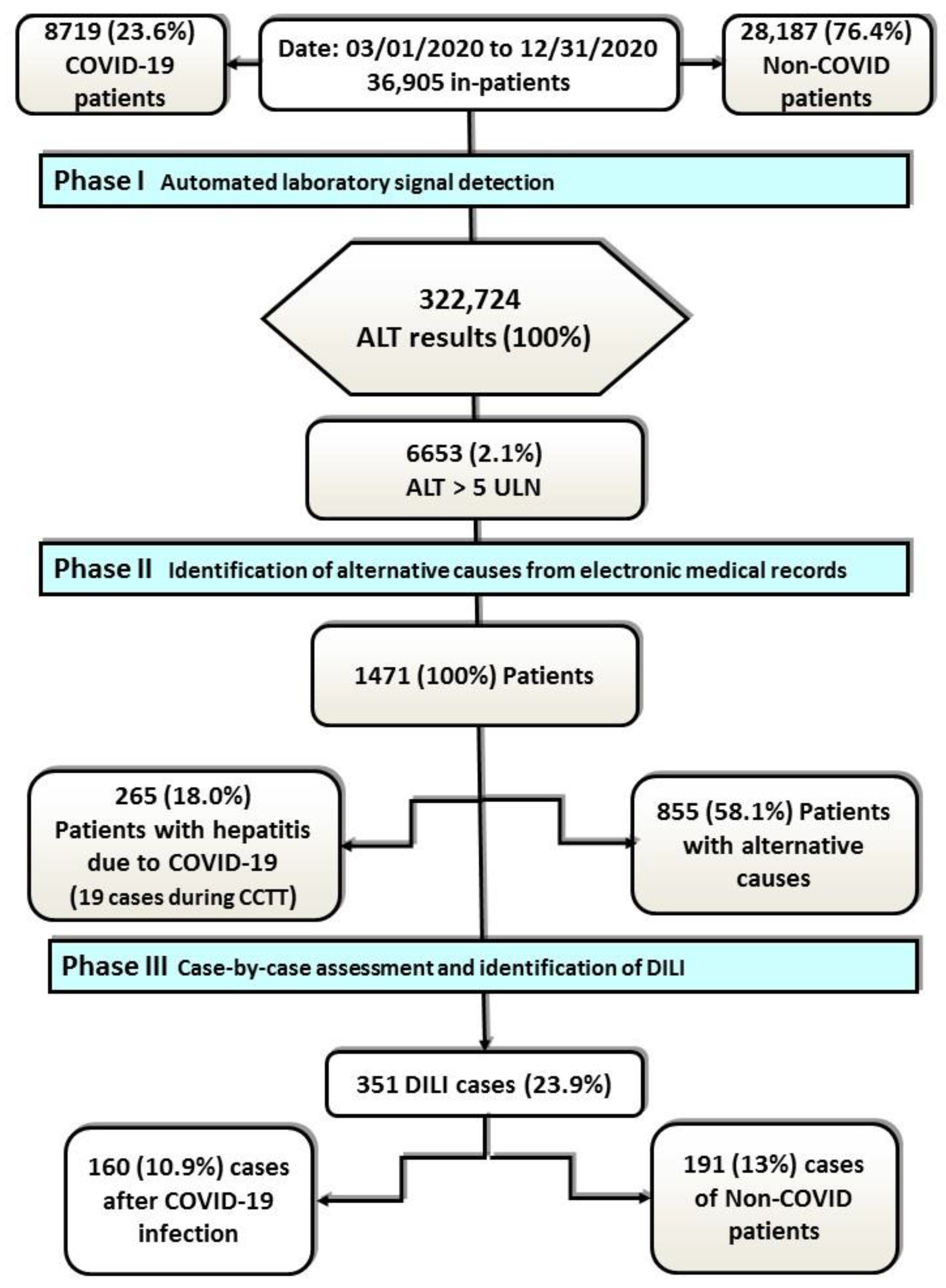
3.1. DILI Incidence
3.2. General Characteristics of the Cohort
3.3. Characteristics of DILI Cases
3.4. Culprit Drugs
3.5. Lymphocyte Transformation Test Results and Concordance with RUCAM
4. Discussion
4.1. Incidence and Length of Stay
4.2. Characteristics of the Cohort
4.3. Culprit Drugs
4.4. Lymphocyte Transformation Test in the Causal Diagnosis of DILI
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alqahtani, S.A.; Schattenberg, J.M. Liver injury in COVID-19: The current evidence. United Eur. Gastroenterol. J. 2020, 8, 509–519. [Google Scholar] [CrossRef]
- Lei, P.; Zhang, L.; Han, P.; Zheng, C.; Tong, Q.; Shang, H.; Yang, F.; Hu, Y.; Li, X.; Song, Y. Liver injury in patients with COVID-19: Clinical profiles, CT findings, the correlation of the severity with liver injury. Hepatol. Int. 2020, 14, 733–742. [Google Scholar] [CrossRef]
- Ding, Z.Y.; Li, G.X.; Chen, L.; Shu, C.; Song, J.; Wang, W.; Wang, Y.W.; Chen, Q.; Jin, G.N.; Liu, T.T.; et al. Association of liver abnormalities with in-hospital mortality in patients with COVID-19. J. Hepatol. 2021, 74, 1295–1302. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Herrera-Lasso Regás, V.; Dordal Culla, M.T.; Lleonart Bellfill, R. Adverse reactions of drugs specifically used for treatment of SARS-CoV-2 infection. Med. Clin. (Barc.) 2020, 155, 448–453. [Google Scholar] [CrossRef] [PubMed]
- Cao, B.; Wang, Y.; Wen, D.; Liu, W.; Wang, J.; Fan, G.; Ruan, L.; Song, B.; Cai, Y.; Wei, M.; et al. A Trial of Lopinavir-Ritonavir in Adults Hospitalized with Severe Covid-19. N. Engl. J. Med. 2020, 382, 1787–1799. [Google Scholar] [CrossRef] [PubMed]
- Cai, Q.; Huang, D.; Yu, H.; Zhu, Z.; Xia, Z.; Su, Y.; Li, Z.; Zhou, G.; Gou, J.; Qu, J.; et al. COVID-19: Abnormal liver function tests. J. Hepatol. 2020, 73, 566–574. [Google Scholar] [CrossRef] [PubMed]
- Grein, J.; Ohmagari, N.; Shin, D.; Diaz, G.; Asperges, E.; Castagna, A.; Feldt, T.; Green, G.; Green, M.L.; Lescure, F.X.; et al. Compassionate Use of Remdesivir for Patients with Severe Covid-19. N. Engl. J. Med. 2020, 382, 2327–2336. [Google Scholar] [CrossRef]
- Grupo de Trabajo del CTSEFV-H Para el Seguimiento de Sospechas de RAM Notificados en Tratamientos Para la Infección por SARS-CoV-2. Agencia Española de Medicamentos y Productos Sanitarios (AEMPS) (2021): Sospechas de Reacciones Adversas Notificadas con Tratamientos Utilizados en COVID-19. Informe nº9: Datos del 1 de Marzo al 31 de Diciembre de. 2020. Available online: https://www.aemps.gob.es/la-aemps/ultima-informacion-de-la-aemps-acerca-del-covid%E2%80%9119/sospechas-de-reacciones-adversas-notificadas-con-tratamientos-utilizados-en-covid-19/ (accessed on 22 September 2021).
- Ramirez, E.; Carcas, A.J.; Borobia, A.M.; Lei, S.H.; Piñana, E.; Fudio, S.; Frias, J. A pharmacovigilance program from laboratory signals for the detection and reporting of serious adverse drug reactions in hospitalized patients. Clin. Pharmacol. Ther. 2010, 87, 74–86. [Google Scholar] [CrossRef]
- Aithal, G.P.; Watkins, P.B.; Andrade, R.J.; Larrey, D.; Molokhia, M.; Takikawa, H.; Hunt, C.M.; Wilke, R.A.; Avigan, M.; Kaplowitz, N.; et al. Case definition and phenotype standardization in drug-induced liver injury. Clin. Pharmacol. Ther. 2011, 89, 806–815. [Google Scholar] [CrossRef]
- ATC/DDD Index 2021. Available online: https://www.whocc.no/atc_ddd_index/ (accessed on 22 September 2021).
- González-Muñoz, M.; Monserrat Villatoro, J.; Marín-Serrano, E.; Stewart, S.; Bardón Rivera, B.; Marín, J.; Martínez de Soto, L.; Seco Meseguer, E.; Ramírez, E. A case report of a drug-induced liver injury (DILI) caused by multiple antidepressants with causality established by the updated Roussel Uclaf causality assessment method (RUCAM) and in vitro testing. Clin. Case Rep. 2020, 8, 3105–3109. [Google Scholar] [CrossRef]
- Sun, J.; Deng, X.; Chen, X.; Huang, J.; Huang, S.; Li, Y.; Feng, J.; Liu, J.; He, G. Incidence of Adverse Drug Reactions in COVID-19 Patients in China: An Active Monitoring Study by Hospital Pharmacovigilance System. Clin. Pharmacol. Ther. 2020, 108, 791–797. [Google Scholar] [CrossRef]
- Chang, H.L.; Chen, K.T.; Lai, S.K.; Kuo, H.W.; Su, I.J.; Lin, R.S.; Sung, F.C. Hematological and biochemical factors predicting SARS fatality in Taiwan. J. Formos. Med. Assoc. 2006, 105, 439–450. [Google Scholar] [CrossRef] [Green Version]
- Zhao, L.F.; Xing, H.C.; Xu, L.P. Effect of SARS-associated coronavirus on peripheral blood picture and liver function. Zhongguo Wei Zhong Bing Ji Jiu Yi Xue 2004, 16, 660–663. [Google Scholar] [PubMed]
- Duan, Z.P.; Chen, Y.; Zhang, J.; Zhao, J.; Lang, Z.W.; Meng, F.K.; Bao, X.L. Clinical characteristics and mechanism of liver injury in patients with severe acute respiratory syndrome. Zhonghua Gan Zang Bing Za Zhi 2003, 11, 493–496. [Google Scholar] [PubMed]
- Fan, Z.; Chen, L.; Li, J.; Cheng, X.; Yang, J.; Tian, C.; Zhang, Y.; Huang, S.; Liu, Z.; Cheng, J. Clinical Features of COVID-19-Related Liver Functional Abnormality. Clin. Gastroenterol. Hepatol. 2020, 18, 1561–1566. [Google Scholar] [CrossRef]
- 19Kullar, R.; Patel, A.P.; Saab, S. Hepatic Injury in Patients with COVID-19. J. Clin. Gastroenterol. 2020, 54, 841–849. [Google Scholar] [CrossRef]
- Ferron, P.J.; Gicquel, T.; Mégarbane, B.; Clément, B.; Fromenty, B. Treatments in Covid-19 patients with pre-existing metabolic dysfunction-associated fatty liver disease: A potential threat for drug-induced liver injury? Biochimie 2020, 179, 266–274. [Google Scholar] [CrossRef]
- Cai, Q.; Huang, D.; Ou, P.; Yu, H.; Zhu, Z.; Xia, Z.; Su, Y.; Ma, Z.; Zhang, Y.; Li, Z.; et al. COVID-19 in a designated infectious diseases hospital outside Hubei Province, China. Allergy 2020, 75, 1742–1752. [Google Scholar] [CrossRef] [PubMed]
- Pedraza, L.; Laosa, O.; Rodríguez-Mañas, L.; Gutiérrez-Romero, D.F.; Frías, J.; Carnicero, J.A.; Ramírez, E. Drug Induced Liver Injury in Geriatric Patients Detected by a Two-Hospital Prospective Pharmacovigilance Program: A Comprehensive Analysis Using the Roussel Uclaf Causality Assessment Method. Front. Pharmacol. 2021, 11, 600255. [Google Scholar] [CrossRef]
- Borobia, A.M.; Carcas, A.J.; Arnalich, F.; Álvarez-Sala, R.; Monserrat-Villatoro, J.; Quintana, M.; Figueira, J.C.; Torres Santos-Olmo, R.M.; García-Rodríguez, J.; Martín-Vega, A.; et al. A Cohort of Patients with COVID-19 in a Major Teaching Hospital in Europe. J. Clin. Med. 2020, 9, 1733. [Google Scholar] [CrossRef]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; Barnaby, D.P.; Becker, L.B.; Chelico, J.D.; Cohen, S.L.; et al. Presenting Characteristics, Comorbidities, and Outcomes among 5700 Patients Hospitalized With COVID-19 in the New York City Area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef]
- Ruiz, B.; García, M.; Aguirre, U.; Aguirre, C. Factors predicting hospital readmissions related to adverse drug reactions. Eur. J. Clin. Pharmacol. 2008, 64, 715–722. [Google Scholar] [CrossRef]
- Batteux, B.; Bodeau, S.; Gras-Champel, V.; Liabeuf, S.; Lanoix, J.P.; Schmit, J.L.; Andréjak, C.; Zerbib, Y.; Haye, G.; Masmoudi, K.; et al. Abnormal laboratory findings and plasma concentration monitoring of lopinavir and ritonavir in COVID-19. Br. J. Clin. Pharmacol. 2021, 87, 1547–1553. [Google Scholar] [CrossRef]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S.; et al. Remdesivir for the Treatment of Covid-19—Final Report. N. Engl. J. Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef]
- Montastruc, F.; Thuriot, S.; Durrieu, G. Hepatic Disorders with the Use of Remdesivir for Coronavirus 2019. Clin. Gastroenterol. Hepatol. 2020, 18, 2835–2836. [Google Scholar] [CrossRef]
- Livertox: Clinical and Research Information on Drug-Induced Liver Injury. Azythromycin. Available online: https://www.ncbi.nlm.nih.gov/books/NBK548434/ (accessed on 18 September 2021).
- Chalasani, N.; Bonkovsky, H.L.; Fontana, R.; Lee, W.; Stolz, A.; Talwalkar, J.; Reddy, K.R.; Watkins, P.B.; Navarro, V.; Barnhart, H.; et al. Features and Outcomes of 899 Patients with Drug-Induced Liver Injury: The DILIN Prospective Study. Gastroenterology 2015, 148, 1340–1352.e7. [Google Scholar] [CrossRef] [Green Version]
- Mahamid, M.; Mader, R.; Safadi, R. Hepatotoxicity of tocilizumab and anakinra in rheumatoid arthritis: Management decisions. Clin. Pharmacol. 2011, 3, 39–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muhović, D.; Bojović, J.; Bulatović, A.; Vukčević, B.; Ratković, M.; Lazović, R.; Smolović, B. First case of drug-induced liver injury associated with the use of tocilizumab in a patient with COVID-19. Liver Int. 2020, 40, 1901–1905. [Google Scholar] [CrossRef] [PubMed]
- Serviddio, G.; Villani, R.; Stallone, G.; Scioscia, G.; Foschino-Barbaro, M.P.; Lacedonia, D. Tocilizumab and liver injury in patients with COVID-19. Ther. Adv. Gastroenterol. 2020, 13, 1756284820959183. [Google Scholar] [CrossRef] [PubMed]
- Sulkowski, M.S. Drug-induced liver injury associated with antiretroviral therapy that includes HIV-1 protease inhibitors. Clin. Infect. Dis. 2004, 38 (Suppl. 2), S90–S97. [Google Scholar] [CrossRef]
- Dauner, D.G.; Dauner, K.N. Summary of adverse drug events for hydroxychloroquine, azithromycin, and chloroquine during the COVID-19 pandemic. J. Am. Pharm. Assoc. 2021, 61, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Melo, J.R.R.; Duarte, E.C.; Moraes, M.V.; Fleck, K.; Silva, A.S.D.N.E.; Arrais, P.S.D. Adverse drug reactions in patients with COVID-19 in Brazil: Analysis of spontaneous notifications of the Brazilian pharmacovigilance system. Cad. Saude Publica 2021, 37, e00245820. [Google Scholar] [CrossRef]
- Maiuri, A.R.; Wassink, B.; Turkus, J.D.; Breier, A.B.; Lansdell, T.; Kaur, G.; Hession, S.L.; Ganey, P.E.; Roth, R.A. Synergistic Cytotoxicity from Drugs and Cytokines In Vitro as an Approach to Classify Drugs According to Their Potential to Cause Idiosyncratic Hepatotoxicity: A Proof-of-Concept Study. J. Pharmacol. Exp. Ther. 2017, 362, 459–473. [Google Scholar] [CrossRef] [PubMed]
- Deng, X.; Luyendyk, J.P.; Ganey, P.E.; Roth, R.A. Inflammatory stress and idiosyncratic hepatotoxicity: Hints from animal models. Pharmacol. Rev. 2009, 61, 262–282. [Google Scholar] [CrossRef] [Green Version]
- Niknahad, H.; Heidari, R.; Firuzi, R.; Abazari, F.; Ramezani, M.; Azarpira, N.; Hosseinzadeh, M.; Najibi, A.; Saeedi, A. Concurrent Inflammation Augments Antimalarial Drugs-Induced Liver Injury in Rats. Adv. Pharm. Bull. 2016, 6, 617–625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davies, M.J. Myeloperoxidase-derived oxidation: Mechanisms of biological damage and its prevention. J. Clin. Biochem. Nutr. 2011, 48, 8–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tafazoli, S.; Spehar, D.D.; O’Brien, P.J. Oxidative stress mediated idiosyncratic drug toxicity. Drug Metab. Rev. 2005, 37, 311–325. [Google Scholar] [CrossRef]
- Whritenour, J.; Ko, M.; Zong, Q.; Wang, J.; Tartaro, K.; Schneider, P.; Olson, E.; Van Volkenburg, M.; Serrano, J.; Hayashi, P.; et al. Development of a modified lymphocyte transformation test for diagnosing drug-induced liver injury associated with an adaptive immune response. J. Immunotoxicol. 2017, 14, 31–38. [Google Scholar] [CrossRef]
- Danan, G.; Teschke, R. RUCAM in Drug and Herb Induced Liver Injury: The Update. Int. J. Mol. Sci. 2016, 17, 14. [Google Scholar] [CrossRef]
- Woo, H.J.; Kim, H.Y.; Choi, E.S.; Cho, Y.H.; Kim, Y.; Lee, J.H.; Jang, E. Drug-induced liver injury: A 2-year retrospective study of 1169 hospitalized patients in a single medical center. Phytomedicine 2015, 22, 1201–1205. [Google Scholar] [CrossRef] [PubMed]
- Mantani, N.; Kogure, T.; Sakai, S.; Goto, H.; Shibahara, N.; Kita, T.; Shimada, Y.; Terasawa, K. Incidence and clinical features of liver injury related to Kampo (Japanese herbal) medicine in 2496 cases between 1979 and 1999: Problems of the lymphocyte transformation test as a diagnostic method. Phytomedicine 2002, 9, 280–287. [Google Scholar] [CrossRef] [PubMed]
- Takikawa, H.; Takamori, Y. Diagnosis of drug induced liver injury. Nihon Shokakibyo Gakkai Zasshi 2003, 100, 653–658. [Google Scholar] [PubMed]


{kind=link}
| Variable | |||
| Number of cases, n | 160 | ||
| Age (years), mean (SD) | 54.3 | (13.9) | |
| Sex (male), n (%) | 124 | (77.5) | |
| Country of origin, n (%) | Spain | 89 | 55.6 |
| Ecuador | 19 | 11.9 | |
| Peru | 8 | 5.0 | |
| Philippines | 6 | 3.7 | |
| Others | 38 | 23.8 | |
| Number of drugs, mean (SD) | 14.7 | (7.6) | |
| Polypharmacy *, n (%) | 157 | (98.1) | |
| History of ADR, n (%) | No | 142 | (88.7) |
| Yes | 18 | (11.3) | |
| Previous liver disease, n (%) | No | 145 | (91.6) |
| Yes Steatosis Hepatitis B chronic | 15 14 1 | (9.4) | |
| Previous COVID hepatitis (ALT > 5 ULN) | No | 64 | (40.0) |
| Yes | 96 | (60.0) | |
| Weight (kg), mean (SD) | 82.7 | (17.2) | |
| Height (cm), mean (SD) | 168.2 | (9.01) | |
| Serum albumin (g/dL, NR: 2.9–5.2), mean (SD) | 3.6 | (0.64) | |
| BMI (kg/m2), mean (SD) | 28.1 | (5.5) | |
| Hypertension, n (%) | No | 111 | (69.4) |
| Yes | 49 | (30.6) | |
| Dyslipidaemia, n (%) | No | 89 | (55.6) |
| Yes | 71 | (44.4) | |
| Diabetes mellitus, n (%) | No | 149 | (93.2) |
| Yes | 11 | (6.8) | |
| Smoking habit, n (%) | No | 301 | (81.2) |
| Smoker | 14 | (8.8) | |
| Former | 16 | (10.0) | |
| Alcoholic habit, n (%) | No | 153 | (95.6) |
| Alcoholism | 6 | (3.8) | |
| Former | 1 | (0.6) | |
| Drug abuse habit, n (%) | No | 159 | (99.4) |
| Yes | 1 | (0.6) | |
| CURB-65, n (%) | 0 | 51 | (31.9) |
| 1 | 49 | (30.6) | |
| 2 | 42 | (26.3) | |
| 3 | 1 | (0.6) | |
| 4 | 0 | (0.0) | |
| 5 | 0 | (0.0) | |
| Unknown | 17 | (10.6) | |
| ICU stay | Total (%) | 38 | (23.8) |
| Discharge n (% ICU) | 26 | (68.4) | |
| Death n (% ICU) | 12 | (31.6) | |
| Outcome of hospitalisation | Discharge | 101 | (63.1) |
| Transfer # | 39 | (24.4) | |
| Death | 19 | (11.9) | |
| Sequelae | 1 | (0.6) | |
| DRUG | |
|---|---|
| NSAIDS | ALLERGY |
| NSAIDS, METAMIZOLE, PENICILLIN, ACETYLSALICYLIC ACID | ALLERGY |
| AZITHROMYCIN, MACROLIDES, NSAIDS | ALLERGY |
| CIPROFLOXACIN | ALLERGY |
| CHLOROQUINE | ALLERGY |
| DILTIAZEM | ALLERGY |
| HALOPERIDOL | ALLERGY |
| IBUPROFEN | ALLERGY |
| QUETIAPINE | INTOLERANCE |
| ISONIAZID | ALLERGY |
| METAMIZOLE | ALLERGY |
| METAMIZOLE | ALLERGY |
| METRONIDAZOLE | ALLERGY |
| PENICILLIN, TETRACYCLINE, CONTRAST AGENT | ALLERGY |
| TETRACYCLINE | ALLERGY |
| TRAMADOL | ALLERGY |
| TRAMADOL | ALLERGY |
| VANCOMYCIN, BETA-LACTAMS | ALLERGY |
| Variable | |||||
| Number of cases, n | 160 | ||||
| Type, n (%) | Hepatocellular | 92 | (57.5) | ||
| Mixed | 20 | (12.5) | |||
| Cholestatic | 6 | (3.8) | |||
| Not classified | 42 | (26.2) | |||
| RUCAM classification, n (%) | Highly probable | 0 | (0.0) | ||
| Probable | 82 | (51.2) | |||
| Possible | 78 | (48.8) | |||
| Severity, n (%) | Mild | 140 | (87.5) | ||
| Moderate | 11 | (6.9) | |||
| Severe | 8 | (5.0) | |||
| Fatal | 1 | (0.6) | |||
| Outcome, n (%) | Recovery | 141 | (88.1) | ||
| Transplant | 0 | (0.0) | |||
| Death | 1 | (0.6) | |||
| No associated death | 18 | (11.2) | |||
| Chronification of hepatitis, n (%) | No chronification | 117 | (83.0) | ||
| Chronification | 16 | (11.3) | |||
| Unknown | 8 | (5.7) | |||
| Recorded HT in DR, n (%) | No | 35 | (21.9) | ||
| Yes | 125 | (78.1) | |||
| Recorded DILI in DR, n (%) | No | 119 | (74.4) | ||
| Yes | 41 | (25.6) | |||
| Laboratory Parameters | Value | Number of Times ULN | |||
| Mean | SD | Mean | SD | ||
| ALT, U/L (NR < 35) | Baseline | 47.3 | 22.3 | 1.1 | 0.6 |
| Maximum | 465.8 | 769.0 | 13.3 | 22.0 | |
| Recovered | 197.4 | 766.0 | 5.6 | 21.8 | |
| LDH, U/L (NR, 100–190) | Baseline | 374.4 | 149.1 | 1.9 | 0.8 |
| Maximum | 886.7 | 2059.9 | 4.6 | 10.8 | |
| Recovered | 585.9 | 2114.4 | 3.1 | 11.1 | |
| AP, U/L (NR, 46–116) | Baseline | 97.9 | 56.8 | 0.8 | 0.5 |
| Maximum | 150.7 | 184.6 | 1.3 | 1.6 | |
| Recovered | 102.6 | 97.0 | 0.7 | 0.8 | |
| Creatinine, mg/dL (NR, 0.7–1.30) | Baseline | 0.9 | 0.3 | 0.7 | 0.2 |
| Maximum | 1.1 | 0.9 | 0.8 | 0.7 | |
| Recovered | 0.9 | 0.5 | 0.7 | 0.4 | |
| Total bilirubin, mg/dL (NR, 0.3–1.2) | Baseline | 0.7 | 0.3 | 0.6 | 0.3 |
| Maximum | 1.2 | 2.4 | 1.0 | 2.0 | |
| Recovered | 1.0 | 2.3 | 0.8 | 1.9 | |
| GGT, U/L (NR < 73) | Baseline | 99.4 | 128.5 | 1.4 | 1.8 |
| Maximum | 357.3 | 360.7 | 4.9 | 4.9 | |
| Recovered | 95.5 | 122.2 | 1.3 | 1.7 | |
| TPAC, (%) (NR, 70–120) | Baseline | 94.8 | 17.3 | 1.4 | 0.2 |
| Maximum | 98.4 | 26.1 | 1.4 | 0.4 | |
| Recovered | 94.2 | 19.9 | 1.3 | 0.3 | |
| pH (7.35–7.45) # | Baseline | 7.42 | 0.07 | 1.0 | 0.01 |
| Maximum | 7.33 | 0.19 | 1.0 | 0.03 | |
| Recovered | 7.33 | 0.14 | 1.0 | 0.02 | |
| Eosinophils, 10³/μL (NR, 0.02–0.65) # | Baseline | 0.10 | 0.13 | 0.15 | 0.19 |
| Maximum | 0.02 | 0.08 | 0.03 | 0.08 | |
| Recovered | 0.11 | 0.13 | 0.12 | 0.12 | |
| Variable | Azithromycin | Hydroxychloroquine/Chloroquine | Ceftriaxone | Tocilizumab | Remdesivir | R/Lopinavir | Paracetamol | Enoxaparin | p-Value | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Number of patients, n | 56 | 82 | 35 | 33 | 14 | 7 | 11 | 9 | ||||||||||
| Age (years), mean (SD) | 56.6 | 12.2 | 57.3 | 11.5 | 54.1 | 11.8 | 57.7 | 7.6 | 50.7 | 13.3 | 53.3 | 10.1 | 46.0 | 12.7 | 58.1 | 10.8 | <0.001 | |
| Sex (male), n (%) | 41 | 73.2 | 64 | 78.0 | 29 | 82.9 | 24 | 68.6 | 12 | 85.7 | 6 | 85.7 | 7 | 63.6 | 9 | 100 | 0.199 | |
| Hospital stay, mean (SD) | 19.8 | 22.2 | 18.8 | 22.1 | 14.9 | 10.5 | 22.5 | 18.8 | 19.8 | 17.1 | 16.4 | 9.9 | 16.1 | 4.5 | 75.4 | 129.7 | <0.001 | |
| History of ADR, n (%) | 5 | 8.9 | 10 | 12.2 | 2 | 5.7 | 3 | 9.1 | 14 | 100 | 1 | 14.3 | 1 | 9.1 | 2 | 22.2 | 0.421 | |
| Type, n (%) | Hepatocellular | 29 | 51.8 | 47 | 57.3 | 19 | 54.2 | 19 | 57.6 | 6 | 42.9 | 4 | 57.1 | 7 | 63.6 | 6 | 66.7 | 0.531 |
| Mixed | 5 | 8.9 | 6 | 7.3 | 3 | 8.6 | 1 | 3.0 | 1 | 7.1 | 1 | 14.3 | 1 | 9.1 | 2 | 22.2 | ||
| Cholestatic | 3 | 5.4 | 3 | 3.7 | 3 | 8.6 | 2 | 6.1 | 1 | 7.1 | 1 | 14.3 | 1 | 9.1 | 0 | |||
| Not Classified | 19 | 33.9 | 26 | 31.7 | 10 | 28.6 | 11 | 33.3 | 6 | 42.9 | 1 | 14.3 | 2 | 18.2 | 1 | 11.1 | ||
| Number of drugs, mean (SD) | 13.1 | 4.6 | 13.3 | 4.8 | 11.9 | 3.8 | 15.7 | 6.0 | 13.4 | 8.4 | 14.1 | 3.5 | 14.0 | 2.8 | 12.9 | 5.8 | 0.650 | |
| Polypharmacy *, n (%) | 55 | 98.2 | 81 | 98.8 | 34 | 97.1 | 33 | 100 | 14 | 100 | 7 | 100 | 10 | 90.9 | 9 | 100 | 0.433 | |
| RUCAM classification, n (%) | Probable | 17 | 30.4 | 32 | 39.0 | 13 | 37.1 | 11 | 33.3 | 6 | 42.9 | 2 | 28.6 | 1 | 9.1 | 4 | 44.4 | 0.373 |
| Possible | 39 | 69.6 | 50 | 61.0 | 22 | 68.9 | 22 | 66.7 | 8 | 57.1 | 5 | 71.4 | 10 | 90.9 | 5 | 55.6 | ||
| Severity, n (%) | Mild | 53 | 94.6 | 75 | 91.5 | 32 | 91.4 | 31 | 94.0 | 12 | 85.7 | 7 | 100 | 11 | 100 | 8 | 88.9 | 0.416 |
| Moderate | 3 | 5.4 | 5 | 6.10 | 2 | 5.7 | 1 | 3.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | ||
| Severe | 0 | 0.0 | 2 | 2.4 | 1 | 2.9 | 1 | 3.0 | 2 | 14.3 | 0 | 0.0 | 0 | 0.0 | 1 | 11.1 | ||
| Outcome, n (%) | Recovered | 51 | 91.0 | 73 | 89.0 | 33 | 94.2 | 28 | 84.9 | 14 | 100 | 7 | 100 | 11 | 100 | 8 | 88.9 | 0.006 |
| Death | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | ||
| No associated death | 4 | 7.0 | 8 | 9.8 | 1 | 2.9 | 5 | 15.15 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 11.1 | ||
| Sequelae | 1 | 2 | 1 | 1.2 | 1 | 2.9 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | ||
| Previous liver disease, n (%) | 7 | 12.5 | 9 | 11 | 3 | 8.6 | 4 | 12.1 | 1 | 7.2 | 2 | 28.6 | 1 | 9.1 | 2 | 22.2 | 0.524 | |
| Weight (kg), mean (SD) | 79.2 | 18.3 | 78.6 | 19.1 | 83.4 | 15.1 | 78.6 | 8.3 | 82.8 | 12.6 | 68.0 | 4.2 | 78.0 | 93.3 | 9.9 | <0.001 | ||
| Height (cm), mean (SD) | 167.8 | 10.2 | 167.1 | 9.0 | 170.8 | 10.0 | 170.3 | 7.8 | 170.4 | 7.5 | 159.5 | 0.7 | 178.0 | 170.3 | 7.4 | <0.001 | ||
| Serum albumin (g/dL), mean (SD) | 3.7 | 0.7 | 3.6 | 0.7 | 3.7 | 0.8 | 3.4 | 0.6 | 3.6 | 0.4 | 4.0 | 0.4 | 3.8 | 0.4 | 3.6 | 0.9 | 0.611 | |
| BMI (kg/m2), mean (SD) | 25,8 | 5.8 | 26.3 | 5.8 | 27.2 | 3.9 | 26.9 | 3.4 | 28.9 | 4.4 | 26.7 | 1.9 | 24.6 | 32.4 | 5.4 | <0.001 | ||
| Hypertension, n (%) | 16 | 28.6 | 26 | 21.7 | 11 | 31.4 | 6 | 18.2 | 4 | 28.6 | 3 | 42.9 | 2 | 18.2 | 2 | 22.2 | 0.357 | |
| Dyslipidaemia, n (%) | 28 | 50 | 40 | 48.8 | 16 | 45.7 | 20 | 60.6 | 3 | 21.4 | 5 | 71.4 | 6 | 54.5 | 4 | 44.4 | 0.332 | |
| DM, n (%) | 2 | 3.6 | 5 | 6.1 | 2 | 5.7 | 0 | 0.0 | 0 | 0.0 | 2 | 28.6 | 0 | 0.0 | 1 | 11.1 | 0.481 | |
| Smoking Habit, n (%) | No | 45 | 80.4 | 64 | 78.0 | 32 | 91.4 | 30 | 90.9 | 11 | 78.6 | 6 | 85.7 | 8 | 72.7 | 6 | 66.7 | 0.341 |
| Smoker | 4 | 7.1 | 8 | 9.8 | 1 | 2.9 | 1 | 3.0 | 2 | 14.3 | 1 | 14.3 | 2 | 18.2 | 1 | 11.1 | ||
| Former | 7 | 12.5 | 10 | 12.2 | 2 | 5.7 | 2 | 6.1 | 1 | 7.1 | 0 | 0.0 | 1 | 9.1 | 2 | 22.2 | ||
| Alcoholic habit, n (%) | No Alcoholism Former | 53 | 94.4 | 79 | 96.3 | 34 | 97.1 | 32 | 97.0 | 13 | 92.9 | 7 | 100 | 10 | 91.0 | 9 | 100 | 0.608 |
| 2 | 3.4 | 2 | 2.5 | 1 | 2.9 | 1 | 3.0 | 1 | 7.1 | 0 | 0.0 | 1 | 9.0 | 0 | 0.0 | |||
| 1 | 1.8 | 1 | 1.2 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |||
| Hepatitis chronification, n (%) | 1 | 1.8 | 2 | 2.4 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 2 | 22.2 | 0.427 | |
| Recorded HT in DR, n (%) | 42 | 75 | 62 | 75.6 | 26 | 74.3 | 27 | 81.8 | 12 | 85.7 | 6 | 85.7 | 10 | 91.0 | 8 | 88.9 | 0.755 | |
| Recorded ADR in DR, n (%) | 15 | 26.8 | 26 | 31.7 | 11 | 31.4 | 11 | 33.3 | 4 | 28.6 | 4 | 57.1 | 4 | 36.4 | 3 | 33.3 | 0.893 | |
| ALT, U/L (NR < 35) | Baseline | 39.6 | 23.4 | 41.5 | 23.8 | 36.1 | 20.2 | 36.0 | 17.9 | 36.2 | 21.5 | 45.0 | 15.3 | 45.4 | 26.6 | 40.2 | 27.8 | 0.001 |
| Maximum | 331.7 | 297.9 | 383.5 | 427.1 | 301.8 | 111.0 | 559.2 | 1240.0 | 339.9 | 207.9 | 292.9 | 188.3 | 298.4 | 103.7 | 813.4 | 1514.3 | <0.001 | |
| Recovered | 89.2 | 262.7 | 141.1 | 434.9 | 70.7 | 67.9 | 315.6 | 1286.7 | 91.8 | 110.6 | 72.8 | 76.4 | 60.6 | 57.7 | 573.2 | 1599.8 | 0.002 | |
| LDH, U/L (NR, 100–190) | Baseline | 384.0 | 152.7 | 364.7 | 154.5 | 377.1 | 129.1 | 413.9 | 159.4 | 372.6 | 129.4 | 248.3 | 97.4 | 356.3 | 120.4 | 266.0 | 94.1 | <0.001 |
| Maximum | 613.1 | 498.6 | 786.6 | 1409.6 | 519.6 | 208.1 | 755.9 | 657.1 | 563.3 | 343.9 | 452.9 | 193.6 | 590.6 | 253.2 | 2655.3 | 6938.4 | <0.001 | |
| Recovered | 298.3 | 491.5 | 524.1 | 1496.2 | 237.4 | 86.0 | 393.1 | 703.1 | 202.7 | 35.6 | 197.3 | 28.3 | 194.1 | 36.2 | 2533.8 | 6983.4 | <0.001 | |
| AP, U/L (NR, 46–116) | Baseline | 94.0 | 62.0 | 86.7 | 60.7 | 110.5 | 76.4 | 74.9 | 14.0 | 157.0 | 105.0 | 71.7 | 20.9 | 76.0 | 14.9 | 88.1 | 21.3 | <0.001 |
| Maximum | 123.0 | 90.1 | 128.4 | 109.7 | 148.6 | 112.6 | 94.4 | 44.8 | 314.3 | 509.6 | 109.0 | 60.0 | 105.4 | 67.2 | 117.4 | 60.8 | <0.001 | |
| Recovered | 79.2 | 22.9 | 78.5 | 23.8 | 92.7 | 39.0 | 77.7 | 20.7 | 131.7 | 46.1 | 80.7 | 30.5 | 69.4 | 12.8 | 89.0 | 25.3 | <0.001 | |
| Cr, mg/dL (NR, 0.7–1.30) | Baseline | 0.9 | 0.4 | 0.9 | 0.4 | 0.9 | 0.2 | 0.8 | 0.2 | 0.9 | 0.2 | 0.9 | 0.2 | 0.8 | 0.2 | 0.9 | 0.2 | <0.001 |
| Maximum | 0.9 | 0.7 | 1.1 | 0.8 | 0.9 | 0.5 | 1.1 | 0.9 | 0.7 | 0.4 | 1.1 | 0.4 | 0.8 | 0.3 | 1.3 | 1.2 | <0.001 | |
| Recovered | 0.9 | 0.5 | 1.0 | 0.5 | 0.9 | 0.3 | 1.0 | 0.7 | 0.7 | 0.3 | 0.9 | 0.2 | 0.8 | 0.2 | 1.1 | 0.9 | <0.001 | |
| TB, mg/dL (NR, 0.3–1.2) | Baseline | 0.6 | 0.3 | 0.6 | 0.2 | 0.6 | 0.2 | 0.7 | 0.4 | 0.6 | 0.2 | 0.7 | 0.2 | 0.7 | 0.3 | 0.5 | 0.1 | <0.001 |
| Maximum | 1.0 | 0.7 | 1.1 | 0.9 | 0.8 | 0.5 | 1.2 | 1.0 | 0.7 | 0.8 | 1.0 | 0.6 | 1.1 | 0.7 | 1.0 | 0.3 | <0.001 | |
| Recovered | 0.7 | 0.5 | 0.8 | 0.7 | 0.6 | 0.3 | 0.9 | 0.8 | 0.6 | 0.2 | 0.6 | 0.2 | 0.7 | 0.2 | 0.9 | 0.3 | <0.001 | |
| GGT, U/L (NR < 73) | Baseline | 99.1 | 126.2 | 95.1 | 119.9 | 100.1 | 97.7 | 84.4 | 92.1 | 97.4 | 135.7 | 53.3 | 18.0 | 98.0 | 105.2 | 73.2 | 76.1 | <0.001 |
| Maximum | 373.0 | 402.6 | 367.0 | 384.5 | 409.7 | 368.3 | 357.0 | 410.6 | 343.2 | 295.7 | 425.3 | 457.7 | 544.0 | 518.1 | 219.4 | 136.9 | <0.001 | |
| Recovered | 81.6 | 113.6 | 99.5 | 139.2 | 108.6 | 121.2 | 89.6 | 136.3 | 95.2 | 66.4 | 101.8 | 121.7 | 78.4 | 90.8 | 63.3 | 25.1 | <0.001 | |
| TPAC, (%) (NR, 70–20) | Baseline | 90 | 19 | 90 | 19 | 91 | 16 | 92 | 18 | 108 | 9 | 87 | 29 | 94 | 11 | 90 | 11 | <0.001 |
| Maximum | 97 | 23 | 99 | 23 | 100 | 21 | 89 | 31 | 113 | 7 | 97 | 25 | 99 | 24 | 95 | 30 | <0.001 | |
| Recovered | 96 | 16 | 93 | 18 | 97 | 12 | 91 | 23 | 95 | 15 | 110 | 7 | 91 | 13 | 84 | 28 | 0.001 | |
| pH (7.35–7.45) | Baseline | 7.4 | 0.1 | 7.4 | 0.1 | 7.4 | 0.0 | 7.4 | 0.1 | 7.5 | 0.0 | 7.4 | 0.1 | 7.5 | 0.1 | <0.001 | ||
| Maximum | 7.3 | 0.2 | 7.3 | 0.1 | 7.4 | 0.1 | 7.3 | 0.2 | 7.4 | 0.1 | 7.4 | 0.2 | 7.3 | 0.2 | <0.001 | |||
| Recovered | 7.4 | 0.1 | 7.3 | 0.1 | 7.4 | 0.0 | 7.3 | 0.2 | 7.4 | 0.0 | 7.4 | 0.1 | 7.3 | 0.2 | <0.001 | |||
| Eo, 10³/μL NR, 0.02–0.65) | Baseline | 0.1 | 0.1 | 0.1 | 0.1 | 0.1 | 0.2 | 0.1 | 0.1 | 0.0 | 0.0 | 0.2 | 0.2 | 0.1 | 0.1 | 0.2 | 0.1 | 0.0321 |
| Maximum | 0.0 | 0.0 | 0.0 | 0.1 | 0.0 | 0.1 | 0.0 | 0.0 | 0.0 | 0.0 | 0.1 | 0.3 | 0.0 | 0.0 | 0.0 | 0.0 | 0.312 | |
| Recovered | 0.1 | 0.1 | 0.2 | 0.2 | 0.2 | 0.2 | 0.1 | 0.1 | 0.1 | 0.1 | 0.3 | 0.3 | 0.1 | 0.1 | 0.1 | 0.1 | 0.067 | |
| DRUG | Cases | ATC Code | DDD Value (U) Route | Consumption in DDDs in DILI DH * | Consumption During the Study Period # (DDDs) | Incidence Rate & (Per 10,000 DDDs) | 95% CI (Per 10,000 DDDs) |
|---|---|---|---|---|---|---|---|
| Remdesivir | 14 | J05AB16 | 0.1 (g) P | 109.2 | 1100 | 992.7 | 932.2–1055.7 |
| Azithromycin | 56 | J01FA10 | 0.5 (g) P | 194.4 | 9207 | 211.1 | 184.4–241.5 |
| Hydroxychloroquine | 82 | P01BA02 | 0.516 (g) O | 336.5 | 17,245 | 195.1 | 169.5–224.4 |
| Ritonavir/lopinavir | 7 | J05AR10 | 0.8 (g) O | 24.6 | 1785 | 137.8 | 115.9–162.0 |
| Tocilizumab | 33 | L04AC07 | 20 (mg) P | 76.5 | 9920 | 77.1 | 61.7–96.2 |
| Ceftriaxone | 35 | J01DD04 | 2 (g) P | 148.5 | 23,586 | 63 | 48.4–80.6 |
| Enoxaparin | 9 | B01AB05 | 2 (TU) P | 170.2 | 107,660 | 15.8 | 9.1–24.7 |
| Paracetamol | 11 | N02BE01 | 3 (g) O/P/R | 176 | 219,410 | 8.0 | 3.5–15.8 |
| Drug 1 | Drug 2 | Drug 3 | Drug 4 | Drug 5 | Drug 6 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Code | LTT | RUCAM Score | LTT | RUCAM Score | LTT | RUCAM Score | LTT | RUCAM Score | LTT | RUCAM Score | LTT | RUCAM Score |
| 02 | Hydroxychloroquine | Lopinavir/Ritonavir | Ceftriaxone | |||||||||
| (−) | +3 | (+) | +4 | (−) | +1 | |||||||
| 03 | Lopinavir/ Ritonavir | Interferon beta-1b | Levofloxacin | Dexketoprofen | Hydroxychloroquine | |||||||
| (−) | +2 | (−) | +4 | (+) | +4 | (−) | +2 | (−) | +4 | |||
| 04 | Tocilizumab | Hydroxychloroquine | ||||||||||
| (+) | +6 | (−) | +6 | |||||||||
| 06 | Azithromycin | |||||||||||
| (+) | +6 | |||||||||||
| 08 | Azithromycin | Hydroxychloroquine | Lopinavir/ Ritonavir | Ceftriaxone | Pantoprazole | |||||||
| (−) | +5 | (+) | +6 | (−) | +5 | (−) | +6 | (+) | +4 | |||
| 09 | Azithromycin | Hydroxychloroquine | Tocilizumab | Paracetamol | Metamizole | |||||||
| (−) | +6 | (−) | +6 | (−) | +6 | (−) | +3 | (−) | +5 | |||
| 10 | Azithromycin | Hydroxychloroquine | Tocilizumab | Paracetamol | ||||||||
| (+) | +4 | (+) | +4 | (−) | +4 | (−) | +3 | |||||
| 13 | Levofloxacin | Azithromycin | Hydroxychloroquine | Tocilizumab | ||||||||
| (−) | +6 | (−) | +4 | (−) | +4 | (−) | +7 | |||||
| 17 | Hydroxychloroquine | Ceftriaxone | Piperacillin/Tazobactam | Metamizole | Paracetamol | Lopinavir/Ritonavir | ||||||
| (+) | (+4) | (+) | +4 | (+) | +4 | (−) | +3 | (−) | 4 | (−) | +4 | |
| 106 | Hydroxychloroquine | Azithromycin | Doxycycline | Dexketoprofen | Enoxaparin | Omeprazole | ||||||
| (−) | +4 | (+) | +4 | (−) | +4 | (+) | +4 | (−) | +4 | (−) | +4 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Delgado, A.; Stewart, S.; Urroz, M.; Rodríguez, A.; Borobia, A.M.; Akatbach-Bousaid, I.; González-Muñoz, M.; Ramírez, E. Characterisation of Drug-Induced Liver Injury in Patients with COVID-19 Detected by a Proactive Pharmacovigilance Program from Laboratory Signals. J. Clin. Med. 2021, 10, 4432. https://doi.org/10.3390/jcm10194432
Delgado A, Stewart S, Urroz M, Rodríguez A, Borobia AM, Akatbach-Bousaid I, González-Muñoz M, Ramírez E. Characterisation of Drug-Induced Liver Injury in Patients with COVID-19 Detected by a Proactive Pharmacovigilance Program from Laboratory Signals. Journal of Clinical Medicine. 2021; 10(19):4432. https://doi.org/10.3390/jcm10194432
Chicago/Turabian StyleDelgado, Ana, Stefan Stewart, Mikel Urroz, Amelia Rodríguez, Alberto M. Borobia, Ibtissam Akatbach-Bousaid, Miguel González-Muñoz, and Elena Ramírez. 2021. "Characterisation of Drug-Induced Liver Injury in Patients with COVID-19 Detected by a Proactive Pharmacovigilance Program from Laboratory Signals" Journal of Clinical Medicine 10, no. 19: 4432. https://doi.org/10.3390/jcm10194432
APA StyleDelgado, A., Stewart, S., Urroz, M., Rodríguez, A., Borobia, A. M., Akatbach-Bousaid, I., González-Muñoz, M., & Ramírez, E. (2021). Characterisation of Drug-Induced Liver Injury in Patients with COVID-19 Detected by a Proactive Pharmacovigilance Program from Laboratory Signals. Journal of Clinical Medicine, 10(19), 4432. https://doi.org/10.3390/jcm10194432