
Looking for a Tailored Therapy for Heart Failure: Are We Capable of Treating the Patient Instead of the Disease?

 , ,
, ,
Abstract
:1. Introduction
2. Angiotensin Receptor/Neprilysin Inhibitor (ARNI)
3. Sodium–Glucose Co-Transporters 2 Inhibitors (SGLT2i)
4. Soluble Guanylate Cyclase (SGC) Modulators
5. Myosin Activators: Omecamtiv Mecarbil
6. Consequences of the “New Era”
7. Our Proposal
- (1)
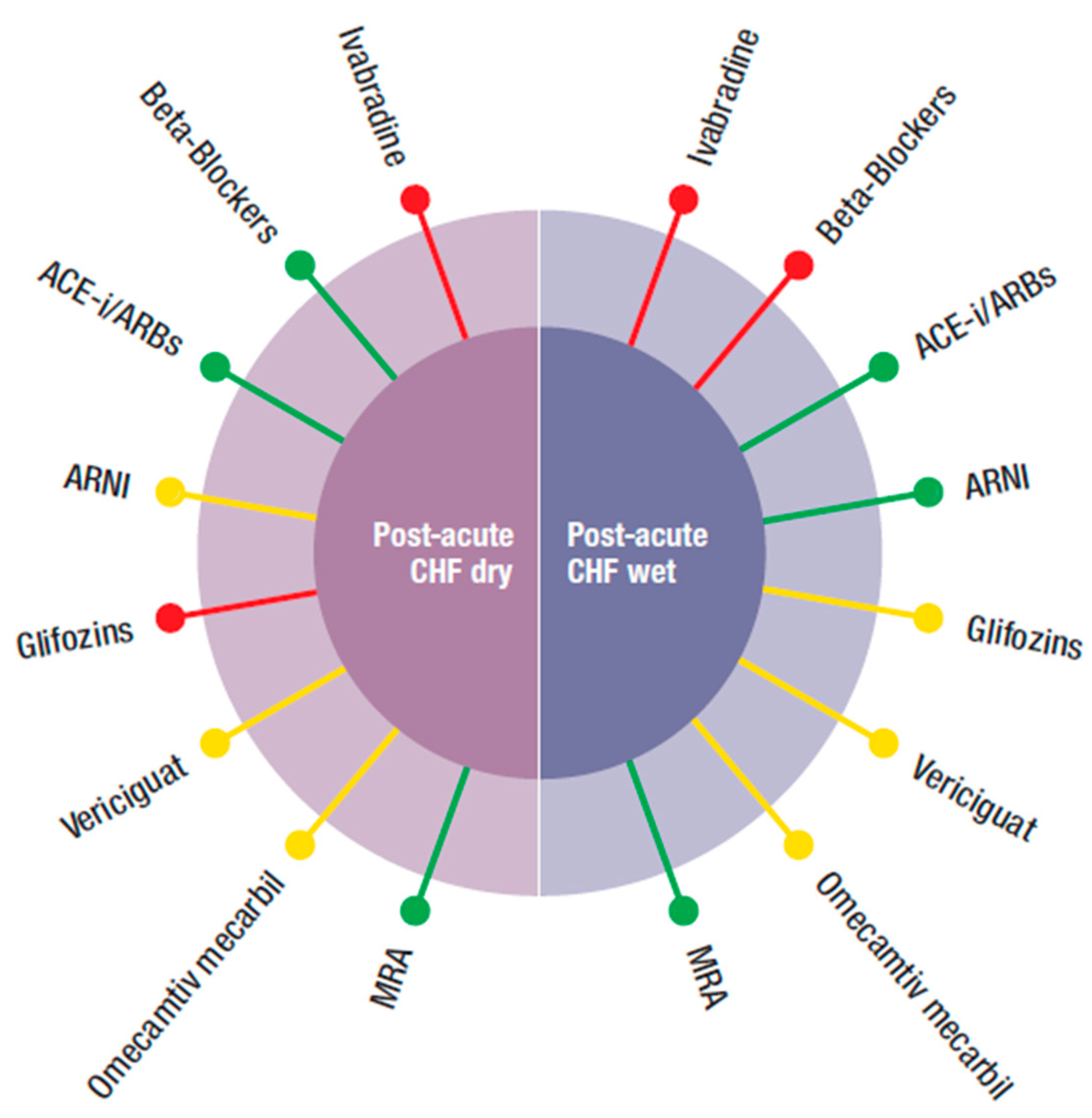
- Post-acute HF wet: often, during hospitalization, patients may be stabilized but remain congestive. In this condition, BBs were not suggested despite some positive data in the severely compromised patients enrolled in COPERNICUS [50]. These, however, were dry patients, without hypervolemia. ACEi/ARBS and MRA can be used if blood pressure is >100 mmHg. ARNI have been proven to reduce re-hospitalization and NT pro-BNP levels after discharge. For gliflozins, there were limited data, mainly from sotogliflozin in the SOLOIST trial. Ivabradine had no data for post-acute HF, independently from being dry or wet.
- (2)
- Post-acute HF dry: gliflozins, and ivabradine also had no data to support or exclude their use. The other “classical” drugs, such as BB, ACEi, MRA, and ARNI can be used, depending on the circumstances. Vericiguat and omecamtiv mecarbil also had no data in the post-acute phase independently from being hypervolemic or not. However, the two respective trials enrolled more severely hospitalized patients than in those for the other classes of drugs and their respective effects, so vasodilatation and increased inotropism might be important.
8. Limitations
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Remme, W.J.; Cleland, J.G.F.; Dargie, H.; Erdmann, E.; Ferrari, R.; Kjekshus, J.; Patrono, C. The treatment of heart failure. Task Force of the Working Group on Heart Failure of the European Society of Cardiology. Eur. Heart J. 1997, 18, 736–753. [Google Scholar] [CrossRef] [Green Version]
- Packer, M. How have millions of people with heart failure benefited from our research over the last 10–15 years? The sounds of dead silence. Eur. J. Heart Fail. 2017, 19, 1353–1354. [Google Scholar] [CrossRef] [Green Version]
- McMurray, J.J.; Packer, M. How Should We Sequence the Treatments for Heart Failure and a Reduced Ejection Fraction? A Redefinition of Evidence-Based Medicine. Circulation 2021, 143, 875–877. [Google Scholar] [CrossRef]
- Maddox, T.M.; Januzzi, J.L.; Allen, L.A.; Breathett, K.; Butler, J.; Davis, L.L.; Fonarow, G.C.; Ibrahim, N.E.; Lindenfeld, J.; Masoudi, F.A.; et al. 2021 Update to the 2017 ACC Expert Consensus Decision Pathway for Optimization of Heart Failure Treatment: Answers to 10 Pivotal Issues About Heart Failure With Reduced Ejection Fraction. J. Am. Coll. Cardiol. 2021, 77, 772–810. [Google Scholar] [CrossRef]
- Bauersachs, J. Heart failure drug treatment: The fantastic four. Eur. Heart J. 2021, 42, 681–683. [Google Scholar] [CrossRef]
- Rosano, G.M.; Moura, B.; Metra, M.; Böhm, M.; Bauersachs, J.; Ben Gal, T.; Adamopoulos, S.; Abdelhamid, M.; Bistola, V.; Čelutkienė, J.; et al. Patient profiling in heart failure for tailoring medical therapy. A consensus document of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2021, 23, 872–881. [Google Scholar] [CrossRef]
- Sinagra, G.; Pagura, L.; Stolfo, D.; Fabris, E.; Savarese, G.; Rapezzi, C.; Ferrari, R.; Merlo, M. Combining New Classes of Drugs for HFrEF: From Trials to Clinical Practice. Eur. J. Intern. Med. 2021, 90, 10–15. [Google Scholar] [CrossRef]
- Packer, M.; Metra, M. Guideline-directed medical therapy for heart failure does not exist: A non-judgmental framework for describing the level of adherence to evidence-based drug treatments for patients with a reduced ejection fraction. Eur. J. Heart Fail. 2020, 22, 1759–1767. [Google Scholar] [CrossRef]
- Ferrari, R.; Silva-Cardoso, J.; Fonseca, M.C. Understanding ARNIs. Eur. Heart J. 2019, 40, 1397–1398. [Google Scholar] [CrossRef]
- Mcmurray, J.; Packer, M.; Desai, A.S.; Gong, J.; Lefkowitz, M.P.; Rizkala, A.R.; Rouleau, J.L.; Shi, V.C.; Solomon, S.D.; Swedberg, K.; et al. Angiotensin–Neprilysin Inhibition versus Enalapril in Heart Failure. N. Engl. J. Med. 2014, 371, 993–1004. [Google Scholar] [CrossRef] [Green Version]
- Januzzi, J.L.; Prescott, M.F.; Butler, J.; Felker, G.M.; Maisel, A.S.; McCague, K.; Camacho, A.; Piña, I.L.; Rocha, R.A.; Shah, A.M.; et al. Association of Change in N-Terminal Pro–B-Type Natriuretic Peptide Following Initiation of Sacubitril-Valsartan Treatment With Cardiac Structure and Function in Patients With Heart Failure With Reduced Ejection Fraction. JAMA 2019, 322, 1085–1095. [Google Scholar] [CrossRef]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.-P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef]
- Velazquez, E.J.; Morrow, D.; Devore, A.D.; Duffy, C.I.; Ambrosy, A.P.; McCague, K.; Rocha, R.; Braunwald, E. Angiotensin–Neprilysin Inhibition in Acute Decompensated Heart Failure. N. Engl. J. Med. 2019, 380, 539–548. [Google Scholar] [CrossRef]
- Wachter, R.; Senni, M.; Belohlavek, J.; Straburzynska-Migaj, E.; Witte, K.K.; Kobalava, Z.; Fonseca, C.; Goncalvesova, E.; Cavusoglu, Y.; Fernandez, A.; et al. Initiation of sacubitril/valsartan in haemodynamically stabilised heart failure patients in hospital or early after discharge: Primary results of the randomised TRANSITION study. Eur. J. Heart Fail. 2019, 21, 998–1007. [Google Scholar] [CrossRef] [Green Version]
- Rohde, L.E.; Chatterjee, N.A.; Vaduganathan, M.; Claggett, B.; Packer, M.; Desai, A.S.; Zile, M.; Rouleau, J.; Swedberg, K.; Lefkowitz, M.; et al. Sacubitril/Valsartan and Sudden Cardiac Death according to Implantable Cardioverter-Defibrillator Use and Heart Failure Cause. JACC Heart Fail. 2020, 8, 844–855. [Google Scholar] [CrossRef]
- Mitchell, G.F.; Solomon, S.D.; Shah, A.M.; Claggett, B.L.; Fang, J.C.; Izzo, J.; Abbas, C.A.; Desai, A.S.; EVALUATE-HF Investigators*. Hemodynamic Effects of Sacubitril-Valsartan Versus Enalapril in Patients With Heart Failure in the EVALUATE-HF Study: Effect Modification by Left Ventricular Ejection Fraction and Sex. Circ. Heart Fail. 2021, 14, e007891. [Google Scholar] [CrossRef]
- Entresto (Sacubitril/Valsartan) Summary of Product Characteristics. Available online: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR-Product_Inform (accessed on 13 May 2018).
- Verma, S.; McMurray, J.J.V. SGLT2 inhibitors and mechanisms of cardiovascular benefit: A state-of-the-art review. Diabetologia 2018, 61, 2108–2117. [Google Scholar] [CrossRef] [Green Version]
- Packer, M. Reconceptualization of the Molecular Mechanism by Which Sodium-Glucose Cotransporter 2 Inhibitors Reduce the Risk of Heart Failure Events. Circulation 2019, 140, 443–445. [Google Scholar] [CrossRef]
- McMurray, J.J.; Solomon, S.D.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; Sabatine, M.S.; Anand, I.S.; Bělohlávek, J.; et al. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction. N. Engl. J. Med. 2019, 381, 1995–2008. [Google Scholar] [CrossRef] [Green Version]
- Packer, M.; Anker, S.D.; Butler, J.; Filippatos, G.; Pocock, S.J.; Carson, P.; Januzzi, J.; Verma, S.; Tsutsui, H.; Brueckmann, M.; et al. Cardiovascular and Renal Outcomes with Empagliflozin in Heart Failure. N. Engl. J. Med. 2020, 383, 1413–1424. [Google Scholar] [CrossRef]
- US Food and Drug Administration. FDA Approves New Treatment for a Type of Heart Failure. [Internet]. FDA; 2020. Available online: https://www.fda.gov/news-events/press-announcements/fda-approves-new-treatment-type-heart-failure (accessed on 13 May 2018).
- Zannad, F.; Ferreira, J.P.; Pocock, S.J.; Anker, S.D.; Butler, J.; Filippatos, G.; Brueckmann, M.; Ofstad, A.P.; Pfarr, E.; Jamal, W.; et al. SGLT2 inhibitors in patients with heart failure with reduced ejection fraction: A meta-analysis of the EMPEROR-Reduced and DAPA-HF trials. Lancet 2020, 396, 819–829. [Google Scholar] [CrossRef]
- Vaduganathan, M.; Claggett, B.L.; Jhund, P.S.; Cunningham, J.W.; Ferreira, J.P.; Zannad, F.; Packer, M.; Fonarow, G.C.; McMurray, J.J.V.; Solomon, S.D. Estimating lifetime benefits of comprehensive disease-modifying pharmacological therapies in patients with heart failure with reduced ejection fraction: A comparative analysis of three randomised controlled trials. Lancet 2020, 396, 121–128. [Google Scholar] [CrossRef]
- Bhatt, D.L.; Szarek, M.; Steg, P.G.; Cannon, C.P.; Leiter, L.A.; McGuire, D.K.; Lewis, J.B.; Riddle, M.C.; Voors, A.A.; Metra, M.; et al. Sotagliflozin in Patients with Diabetes and Recent Worsening Heart Failure. N. Engl. J. Med. 2021, 384, 117–128. [Google Scholar] [CrossRef]
- Cowie, M.R.; Fisher, M. SGLT2 inhibitors: Mechanisms of cardiovascular benefit beyond glycaemic control. Nat. Rev. Cardiol. 2020, 17, 761–772. [Google Scholar] [CrossRef]
- Nikolic, M.; Zivkovic, V.; Jovic, J.J.; Sretenovic, J.; Davidovic, G.; Simovic, S.; Djokovic, D.; Muric, N.; Bolevich, S.; Jakovljevic, V. SGLT2 inhibitors: A focus on cardiac benefits and potential mechanisms. Heart Fail. Rev. 2021, 1–15. [Google Scholar] [CrossRef]
- Perkovic, V.; Jardine, M.J.; Neal, B.; Bompoint, S.; Heerspink, H.J.; Charytan, D.; Edwards, R.; Agarwal, R.; Bakris, G.; Bull, S.; et al. Canagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy. N. Engl. J. Med. 2019, 380, 2295–2306. [Google Scholar] [CrossRef] [Green Version]
- Heerspink, H.J.; Stefánsson, B.V.; Correa-Rotter, R.; Chertow, G.M.; Greene, T.; Hou, F.-F.; Mann, J.F.; McMurray, J.J.; Lindberg, M.; Rossing, P.; et al. Dapagliflozin in Patients with Chronic Kidney Disease. N. Engl. J. Med. 2020, 383, 1436–1446. [Google Scholar] [CrossRef]
- Stasch, J.-P.; Pacher, P.; Evgenov, O.V. Soluble Guanylate Cyclase as an Emerging Therapeutic Target in Cardiopulmonary Disease. Circulation 2011, 123, 2263–2273. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, P.W.; Pieske, B.; Anstrom, K.J.; Ezekowitz, J.; Hernandez, A.F.; Butler, J.; Lam, C.S.; Ponikowski, P.; Voors, A.A.; Jia, G.; et al. Vericiguat in Patients with Heart Failure and Reduced Ejection Fraction. N. Engl. J. Med. 2020, 382, 1883–1893. [Google Scholar] [CrossRef]
- Sweeney, H.L.; Houdusse, A. Structural and Functional Insights into the Myosin Motor Mechanism. Annu. Rev. Biophys. 2010, 39, 539–557. [Google Scholar] [CrossRef]
- Morgan, B.P.; Muci, A.; Lu, P.-P.; Qian, X.; Tochimoto, T.; Smith, W.W.; Garard, M.; Kraynack, E.; Collibee, S.; Suehiro, I.; et al. Discovery of Omecamtiv Mecarbil the First, Selective, Small Molecule Activator of Cardiac Myosin. ACS Med. Chem. Lett. 2010, 1, 472–477. [Google Scholar] [CrossRef] [Green Version]
- Teerlink, J.R.; Felker, G.M.; McMurray, J.J.V.; Solomon, S.D.; Adams, K.F.; Cleland, J.G.F.; Ezekowitz, J.A.; Goudev, A.; Macdonald, P.; Metra, M.; et al. Chronic Oral Study of Myosin Activation to Increase Contractility in Heart Failure (COSMIC-HF): A phase 2, pharmacokinetic, randomised, placebo-controlled trial. Lancet 2016, 388, 2895–2903. [Google Scholar] [CrossRef] [Green Version]
- Teerlink, J.R.; Felker, G.I.; McMurray, J.J.; Solomon, S.D.; Kurtz, C.E.; Monslavo, M.L.; Johnston, J.; Malik, F.I.; Honarpour, N. Effect of Omecamtiv Mecarbil in Patients with Ischemic and Non-Ischemic Heart Failure with Reduced Ejection Fraction: Results From COSMIC-HF. J. Card. Fail. 2017, 23, S11. [Google Scholar] [CrossRef]
- Teerlink, J.R.; Diaz, R.; Felker, G.M.; McMurray, J.J.; Metra, M.; Solomon, S.D.; Adams, K.F.; Anand, I.; Arias-Mendoza, A.; Biering-Sørensen, T.; et al. Cardiac Myosin Activation with Omecamtiv Mecarbil in Systolic Heart Failure. N. Engl. J. Med. 2021, 384, 105–116. [Google Scholar] [CrossRef]
- A McDonagh, T.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Hear. J. 2021. [Google Scholar] [CrossRef]
- Butler, J.; Anstrom, K.J.; Armstrong, P.W.; For the VICTORIA Study Group. Comparing the Benefit of Novel Therapies across Clinical Trials: Insights from the VICTORIA Trial. Circulation 2020, 142, 717–719. [Google Scholar] [CrossRef] [Green Version]
- Seferovic, P.M.; Ponikowski, P.; Anker, S.D.; Bauersachs, J.; Chioncel, O.; Cleland, J.G.; De Boer, R.A.; Drexel, H.; Ben Gal, T.; Hill, L.; et al. Clinical practice update on heart failure 2019: Pharmacotherapy, procedures, devices and patient management. An expert consensus meeting report of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2019, 21, 1169–1186. [Google Scholar] [CrossRef]
- Zannad, F.; Mcmurray, J.; Krum, H.; Van Veldhuisen, D.J.; Swedberg, K.; Shi, H.; Vincent, J.; Pocock, S.J.; Pitt, B. Eplerenone in Patients with Systolic Heart Failure and Mild Symptoms. N. Engl. J. Med. 2011, 364, 11–21. [Google Scholar] [CrossRef] [Green Version]
- Pitt, B.; Zannad, F.; Remme, W.J.; Cody, R.; Castaigne, A.; Perez, A.; Palensky, J.; Wittes, J. The Effect of Spironolactone on Morbidity and Mortality in Patients with Severe Heart Failure. N. Engl. J. Med. 1999, 341, 709–717. [Google Scholar] [CrossRef] [Green Version]
- Willenheimer, R.; van Veldhuisen, D.J.; Silke, B.; Erdmann, E.; Follath, F.; Krum, H.; Ponikowski, P.; Skene, A.; van de Ven, L.; Verkenne, P.; et al. Effect on survival and hospitalization of initiating treatment for chronic heart failure with bisoprolol followed by enalapril, as compared with the opposite sequence: Results of the randomized Cardiac Insufficiency Bisoprolol Study (CIBIS) III. Circulation 2005, 112, 2426–2435. [Google Scholar] [CrossRef] [Green Version]
- Fox, K.; Ford, I.; Steg, P.G.; Tendera, M.; Ferrari, R.; on behalf of the BEAUTifUL Investigators. Ivabradine for patients with stable coronary artery disease and left-ventricular systolic dysfunction (BEAUTIFUL): A randomised, double-blind, placebo-controlled trial. Lancet 2008, 372, 807–816. [Google Scholar] [CrossRef]
- Fox, K.; Ford, I.; Steg, P.G.; Tardif, J.-C.; Tendera, M.; Ferrari, R. Bradycardia and atrial fibrillation in patients with stable coronary artery disease treated with ivabradine: An analysis from the SIGNIFY study. Eur. Heart J. 2015, 36, 3291–3296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okunrintemi, V.; Mishriky, B.M.; Powell, J.R.; Cummings, D.M. Sodium-glucose co-transporter-2 inhibitors and atrial fibrillation in the cardiovascular and renal outcome trials. Diabetes, Obes. Metab. 2021, 23, 276–280. [Google Scholar] [CrossRef] [PubMed]
- Kotecha, D.; Holmes, J.; Krum, H.; Altman, D.G.; Manzano, L.; Cleland, J.G.F.; Lip, G.Y.H.; Coats, A.J.S.; Andersson, B.; Kirchhof, P.; et al. Efficacy of β blockers in patients with heart failure plus atrial fibrillation: An individual-patient data meta-analysis. Lancet 2014, 384, 2235–2243. [Google Scholar] [CrossRef] [Green Version]
- Brachmann, J.; Sohns, C.; Andresen, D.; Siebels, J.; Sehner, S.; Boersma, L.; Merkely, B.; Pokushalov, E.; Sanders, P.; Schunkert, H.; et al. Atrial Fibrillation Burden and Clinical Outcomes in Heart Failure. JACC: Clin. Electrophysiol. 2021, 7, 594–603. [Google Scholar] [CrossRef]
- Mark, D.B.; Anstrom, K.J.; Sheng, S.; Piccini, J.P.; Baloch, K.N.; Monahan, K.H. Effect of catheter ablation vs. medical therapy on quality of life among patients with atrial fibrillation: The CABANA Randomized Clinical Trial. JAMA 2019, 321, 1275–1285. [Google Scholar] [CrossRef]
- Rillig, A.; Magnussen, C.; Ozga, A.-K.; Suling, A.; Brandes, A.; Breithardt, G.; Camm, A.J.; Crijns, H.J.; Eckardt, L.; Elvan, A.; et al. Early Rhythm Control Therapy in Patients with Atrial Fibrillation and Heart Failure. Circulation 2021, 383, 1305–1316. [Google Scholar] [CrossRef]
- Packer, M.; Coats, A.S.; Fowler, M.B.; Katus, H.A.; Krum, H.; Mohacsi, P.; Rouleau, J.L.; Tendera, M.; Castaigne, A.; Roecker, E.B.; et al. Effect of Carvedilol on Survival in Severe Chronic Heart Failure. New Engl. J. Med. 2001, 344, 1651–1658. [Google Scholar] [CrossRef] [Green Version]
 Preferred,
Preferred,  Possible,
Possible,  Not suggested or great caution needed.
Preferred, Possible, Not suggested or great caution needed.
Not suggested or great caution needed.
Preferred, Possible, Not suggested or great caution needed.
 Preferred,
Preferred,  Possible,
Possible,  Not suggested or great caution needed.
Preferred, Possible, Not suggested or great caution needed.
Not suggested or great caution needed.
Preferred, Possible, Not suggested or great caution needed.
 Preferred,
Preferred,  Possible,
Possible,  Not suggested or great caution needed.
Preferred, Possible, Not suggested or great caution needed.
Not suggested or great caution needed.
Preferred, Possible, Not suggested or great caution needed.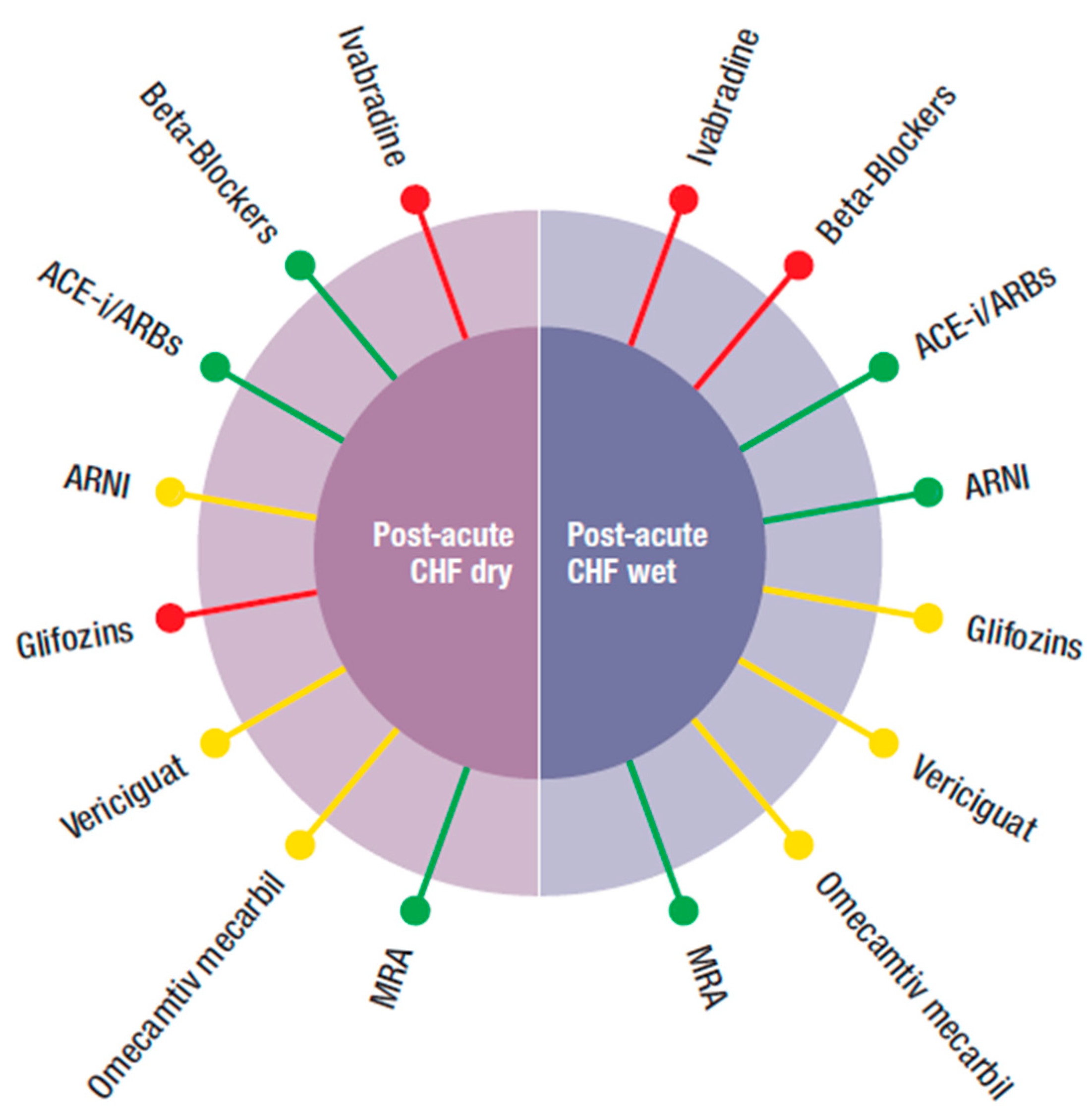

{kind=link}
{kind=link}
{kind=link}
|
PARADIGM HF (N = 8442) |
DAPA-HF (N = 4744) |
EMPEROR-reduced (N = 3730) |
VICTORIA (N = 5050) |
GALACTIC HF (N = 8256) |
SOLVD (N = 2569) |
CIBIS II (N = 2647) |
RALES (N = 1663) |
EMPHASIS (N = 2737) |
SHIFT (N = 6558) | |
|---|---|---|---|---|---|---|---|---|---|---|
| AGE (years) | 63.8 ± 11.5 | 66.2 ± 11 | 67.2 ± 10.8 | 67.5 ± 12.2 | 64.5 ± 11.3 | 60.7 | 61 ± 11 | 65 ± 12 | 68.7 ± 7.7 | 60.7 ± 11.2 |
| MALE (%) | 79 | 76.2 | 76.5 | 76 | 78.8 | 80.9 | 81 | 73 | 77.3 | 76 |
| BMI (kg/m2) | 28.1 ± 5.5 | 28.2 ± 6 | 28.0 ± 5.5 | 27.7 ± 5.8 | 28.5 ± 6.2 | NA | NA | NA | 27.5 ± 4.9 | 28 ± 5.1 |
| NYHA III-IV (%) | 23.9 | 32.3 | 24.9 | 41.4 | 46.7 | 31.8 | 100 | 99.6 | 0 | 52.0 |
| NYHA II-III (%) | 94.7 | 99.2 | 99.5 | 98.6 | 97 | 88 | 83 | 70 | 100 | 98 |
| NYHA IV (%) | 0.8 | 0.8 | 0.5 | 1.4 | 3 | 1.9 | 17 | 30 | 0 | 2 |
| LVEF (%) | 29 ± 6.1 | 31.2 ± 6.7 | 27.7± 6 | 29 ± 8.3 | 26.6 ± 6.3 | 24.8 ± 6.1 | 27.5 ± 6 | 25.2 ± 6.8 | 26.2 ± 4.6 | 29 ± 5.1 |
| HR AT ENTRY | 72 ± 12 | 71.5 ± 11.6 | 71.0 ± 11.7 | 73.1 ± 13 | 72.4 ± 12.2 | 80 ± 14 | 79.9 ± 15 | 81 ± 15 | 72 ± 12 | 79.7 ± 9.5 |
| NT-proBNP (pg/mL) | 1631 | 1428 | 1887 | 2816 | 1977 | NA | NA | NA | NA | NA |
| SERUM CREATININE (mg/dL) | 1.13 ± 0.3 | NA | NA | NA | NA | 1.2 ± 0.3 | NA | NA | 1.14 ± 0.3 | NA |
| eGFR (mL/min/1.73 m2) | 70 ± 20 | 66 ± 19.6 | 61.8 ± 21.7 | 61.5 ± 27.2 | 58.8 ± 14.5 | 65.7 ± 19.0 | 64 ± 26 | 65.3 ± 23 | 71.2 ± 21.9 | 74.6 ± 22.9 |
| SERUM POTASSIUM (mmol/L) | 4.5 ± 0.6 | NA | NA | 4.5 ± 0.5 | NA | 4.3 ± 0.4 | NA | 4.29 ± 0.5 | 4.3 ± 0.4 | NA |
| AF (%) | 36.2 | 38.6 | 35.6 | 44.9 | 27.8 | 11.5 | 21 | 27.8 | 30.8 | 0 |
| HISTORY of HHF (%) | 62.3 | 47.4 | 31.0 (12 months) | 84 | 100 (12 months) | NA | NA | 53.2 | 52.3 | 100 (12 months) |
| In Hospital Randomization | 0 | 0 | 0 | NA | 25.2 | NA | 0 | NA | 0 | 0 |
| PARADIGM HF (N = 8442) | DAPA HF (N = 4744) | EMPEROR-reduced (N = 3730) | VICTORIA (N = 5050) | GALACTIC HF (N = 8256) | SOLVD (N = 2569) | CIBIS II (N = 2647) | RALES (N = 1663) | EMPHASIS (N = 2737) | SHIFT (N = 6558) | |
|---|---|---|---|---|---|---|---|---|---|---|
| AGE years | ≥18 | ≥18 | ≥18 | >18 | >18–<85 | ≤80 | 18–80 | >18 | ≥55 | >18 |
| NYHA | II-IV | II-IV | II-IV | II-IV | II-IV | I-IV | III-IV | III-IV | II | II-IV |
| LVEF % | ≤40 | ≤40 | ≤40 | <45 | ≤35 | ≤35 | ≤35 | <35 | <30 | ≤35 |
| creatinine mg/dl | NA | NA | NA | NA | NA | ≤2.5 | <3.4 | <2.5 | NA | NA |
| Potassium mmol/L | <5.2 | No limit | No limit | No limit | No limit | No limit | No limit | ≤5.0 | ≤5.0 | No limit |
| SBP mmHg | >100 | ≥95 | ≥100 | >100 | ≥85 | No limit | ≥100 | NA | >85 | ≥85 |
| eGFR mL/min/1.73 m2 | >30 | ≥30 | ≥20 | >15 | ≥20 | NA | NA | NA | ≥30 | ≥30 |
| NT-proBNP (pg/mL) | ≥600; ≥400 (with HHF 12mo) | ≥600; ≥900 (IF AF); ≥400 (IF HHF < 12mo); | ≥600;* ≥1000;** ≥2500; *** | ≥1000; ≥1600 (with AF) | ≥400; ≥1200 (with AF) | NA | NA | NA | ≥500 M and ≥750 F (without HHF < 6 mo) | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fucili, A.; Cimaglia, P.; Severi, P.; Giannini, F.; Boccadoro, A.; Micillo, M.; Rapezzi, C.; Tavazzi, L.; Ferrari, R. Looking for a Tailored Therapy for Heart Failure: Are We Capable of Treating the Patient Instead of the Disease? J. Clin. Med. 2021, 10, 4325. https://doi.org/10.3390/jcm10194325
Fucili A, Cimaglia P, Severi P, Giannini F, Boccadoro A, Micillo M, Rapezzi C, Tavazzi L, Ferrari R. Looking for a Tailored Therapy for Heart Failure: Are We Capable of Treating the Patient Instead of the Disease? Journal of Clinical Medicine. 2021; 10(19):4325. https://doi.org/10.3390/jcm10194325
Chicago/Turabian StyleFucili, Alessandro, Paolo Cimaglia, Paolo Severi, Francesco Giannini, Alberto Boccadoro, Marco Micillo, Claudio Rapezzi, Luigi Tavazzi, and Roberto Ferrari. 2021. "Looking for a Tailored Therapy for Heart Failure: Are We Capable of Treating the Patient Instead of the Disease?" Journal of Clinical Medicine 10, no. 19: 4325. https://doi.org/10.3390/jcm10194325
APA StyleFucili, A., Cimaglia, P., Severi, P., Giannini, F., Boccadoro, A., Micillo, M., Rapezzi, C., Tavazzi, L., & Ferrari, R. (2021). Looking for a Tailored Therapy for Heart Failure: Are We Capable of Treating the Patient Instead of the Disease? Journal of Clinical Medicine, 10(19), 4325. https://doi.org/10.3390/jcm10194325