
Trends in the Incidence and Survival Rates of Colorectal Signet-Ring Cell Carcinoma in the South Korean Population: Analysis of the Korea Central Cancer Registry Database


Abstract
:1. Introduction
2. Materials and Methods
Ethics Statement
3. Results
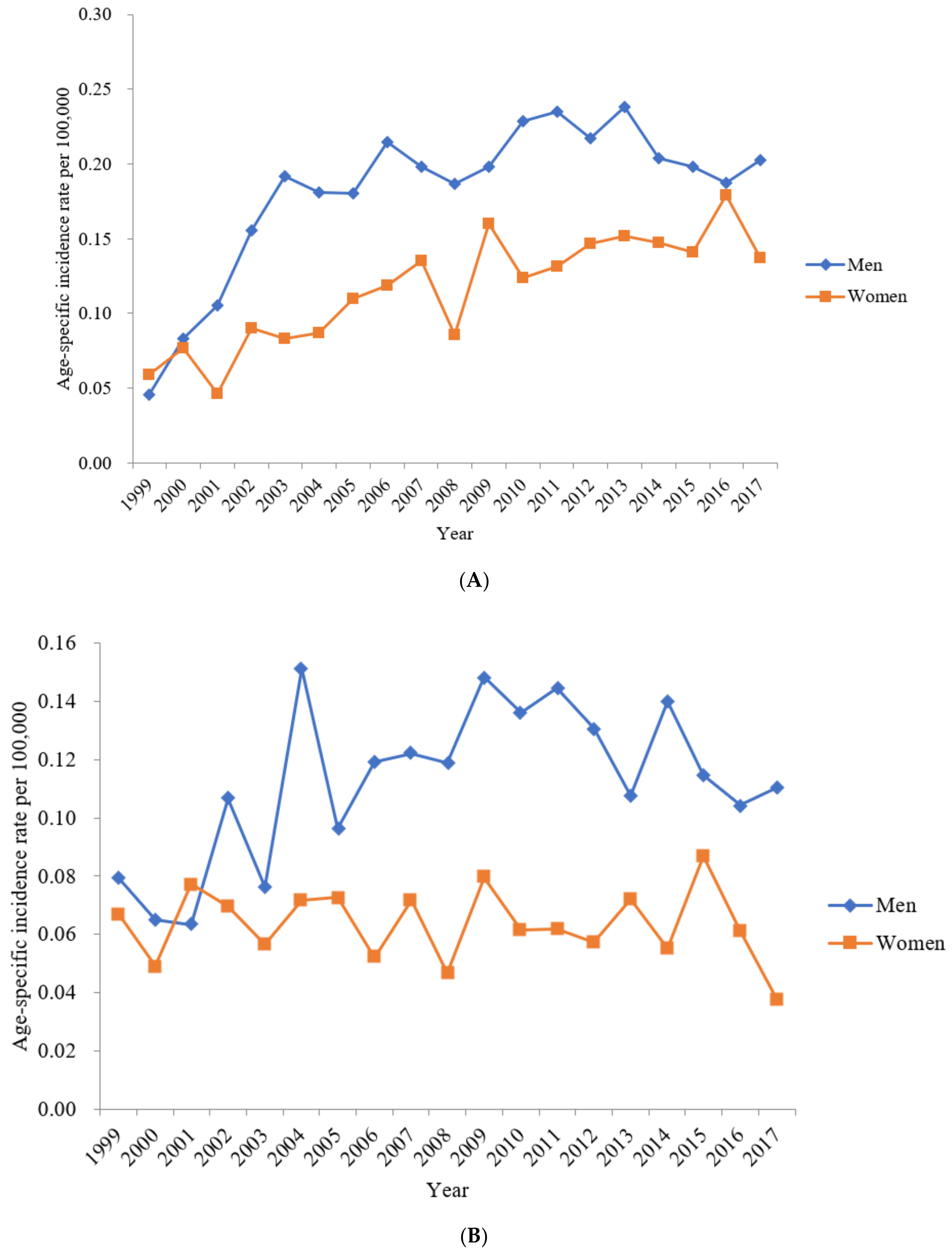
3.1. Incidence of Colon SRCC
3.2. Incidence of Rectum SRCC
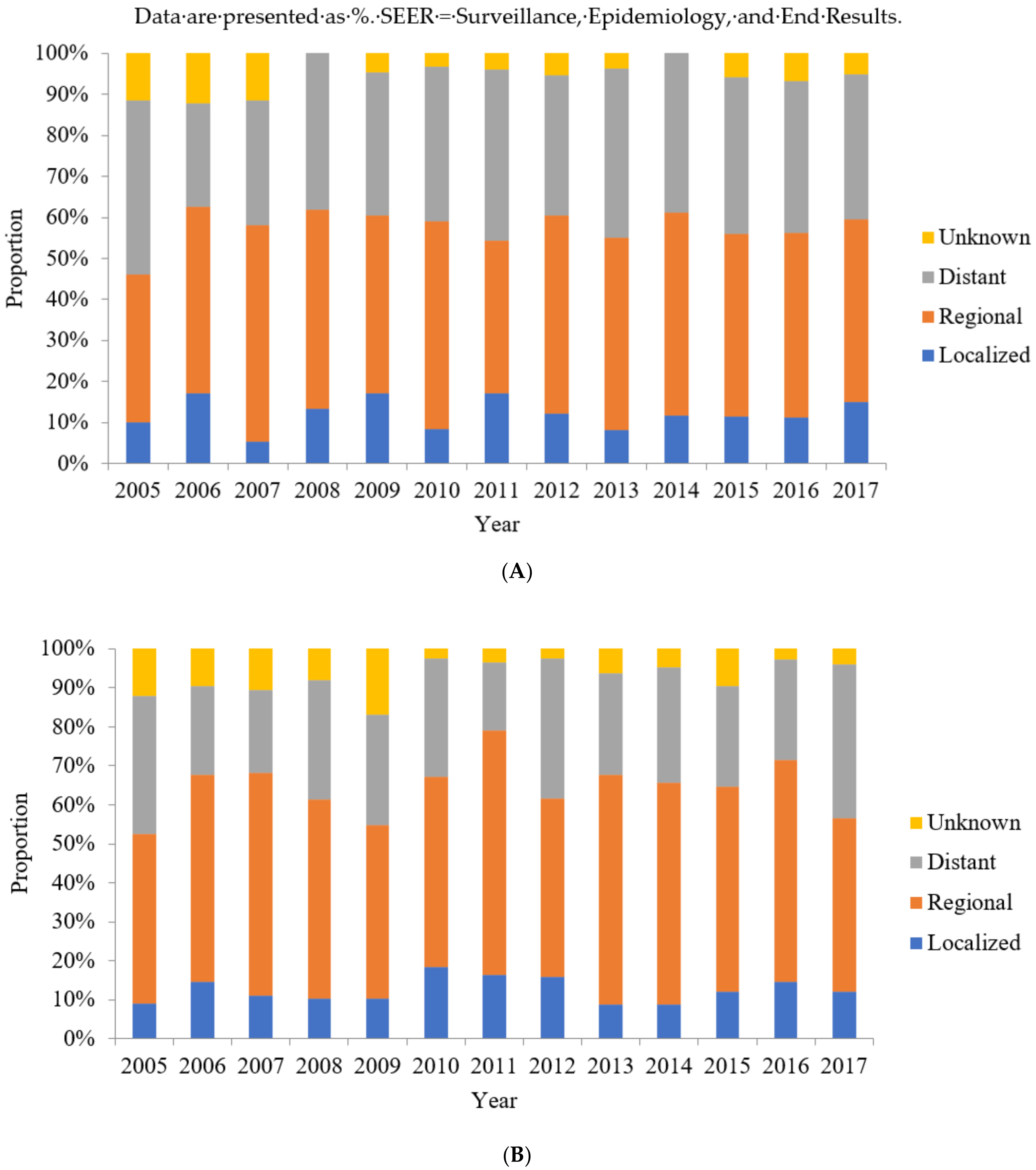
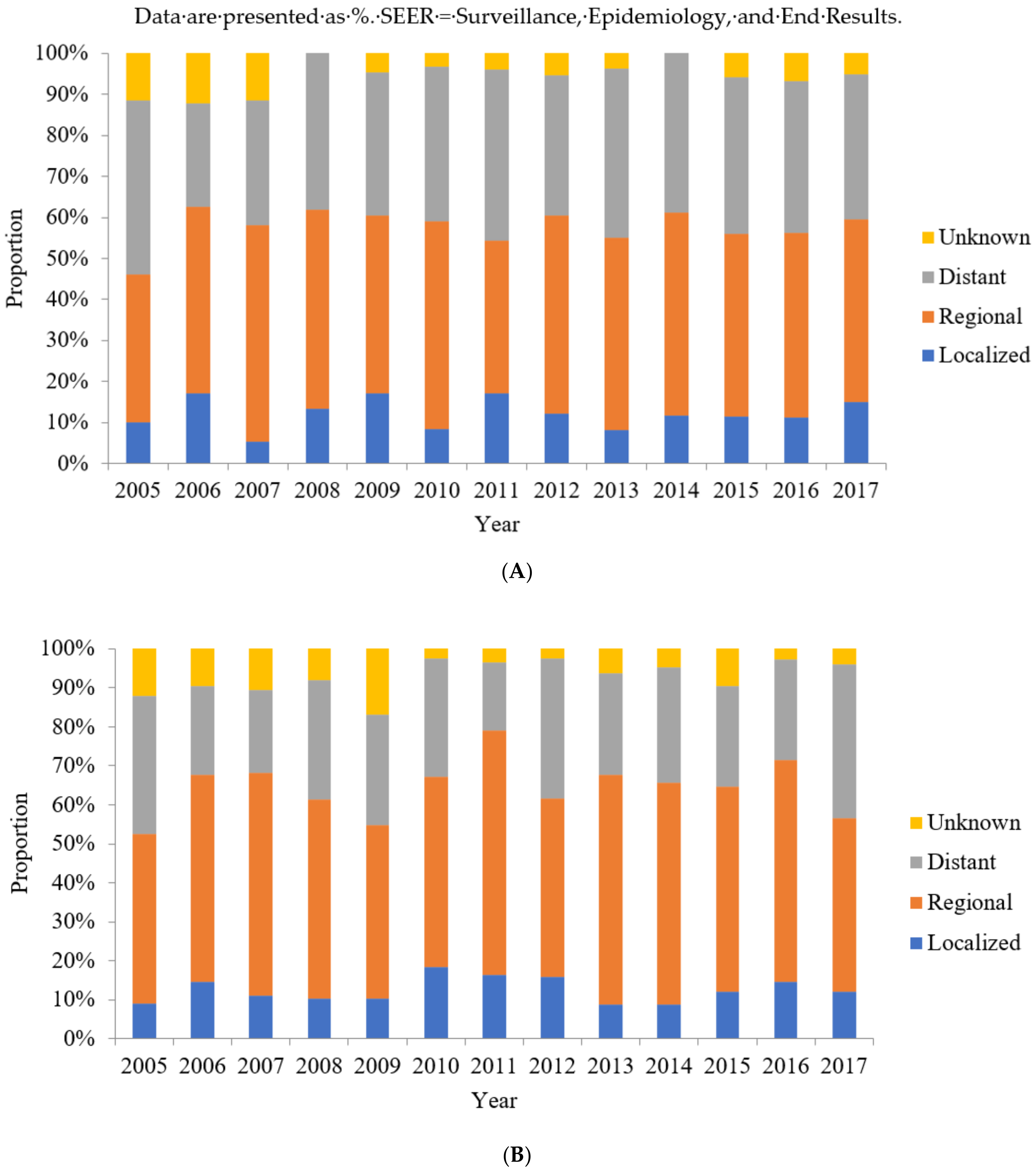
3.3. SEER Summary Stages of Colon SRCC between 2005 and 2017
3.4. SEER Summary Stages of Rectum SRCC between 2005 and 2017
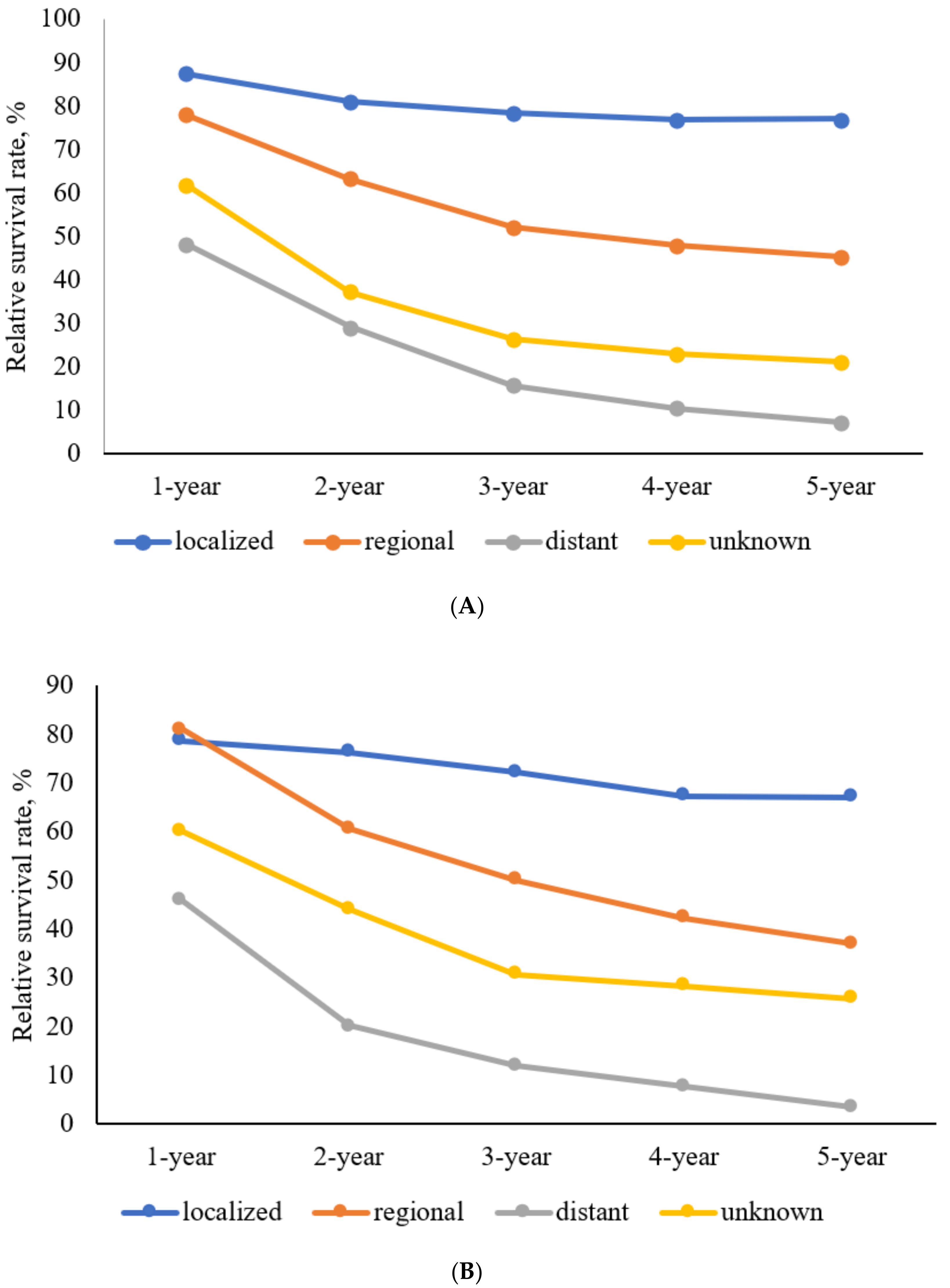
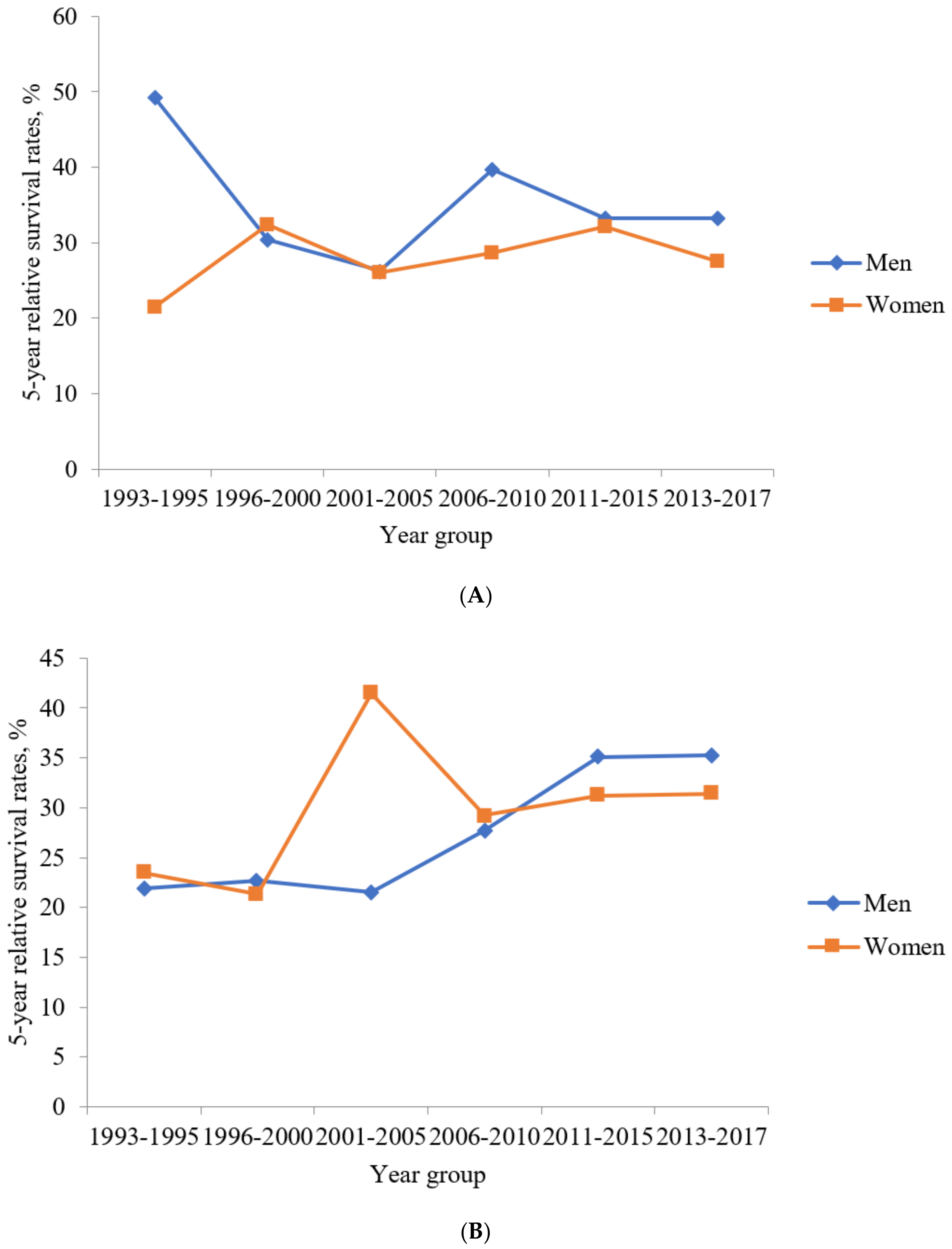
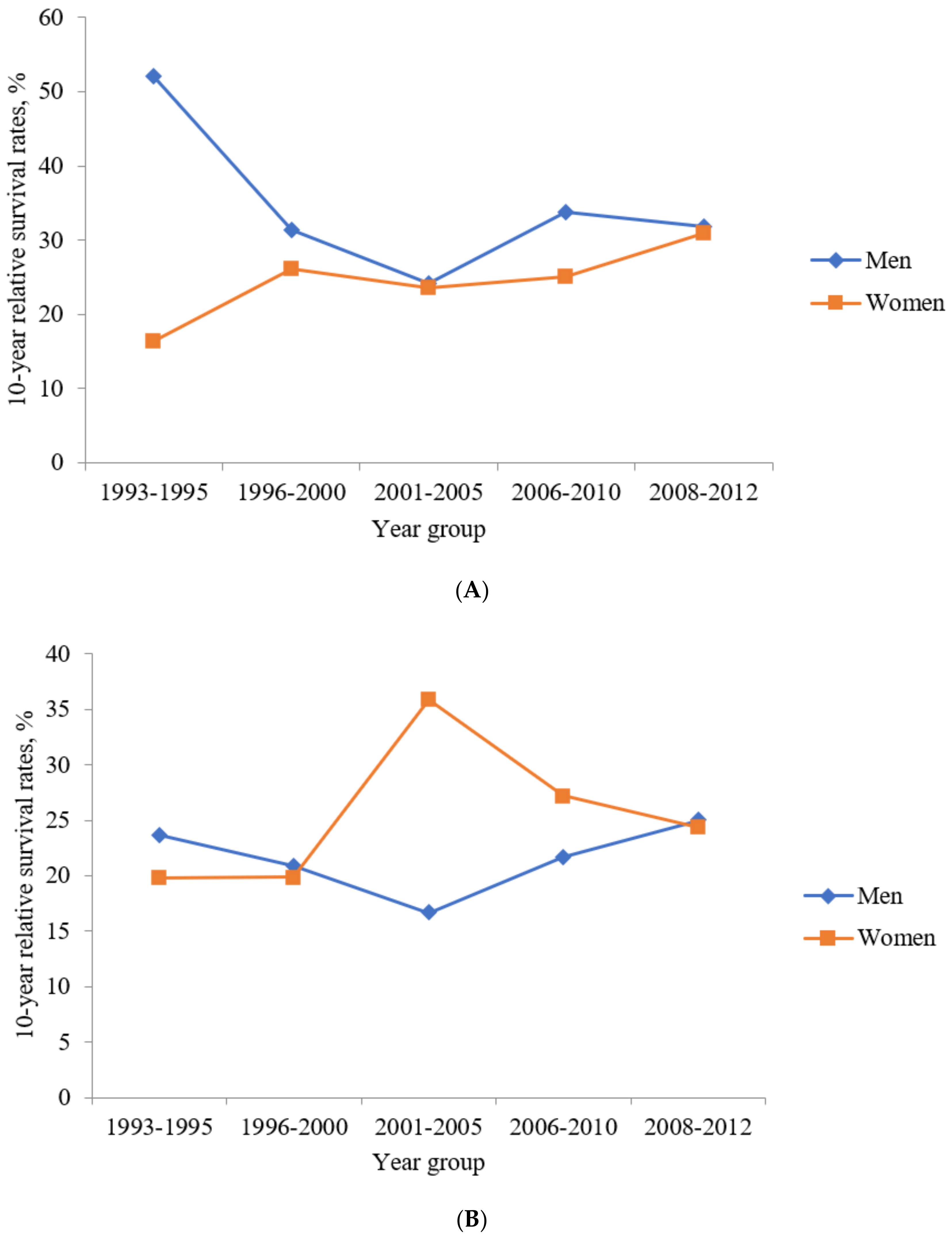
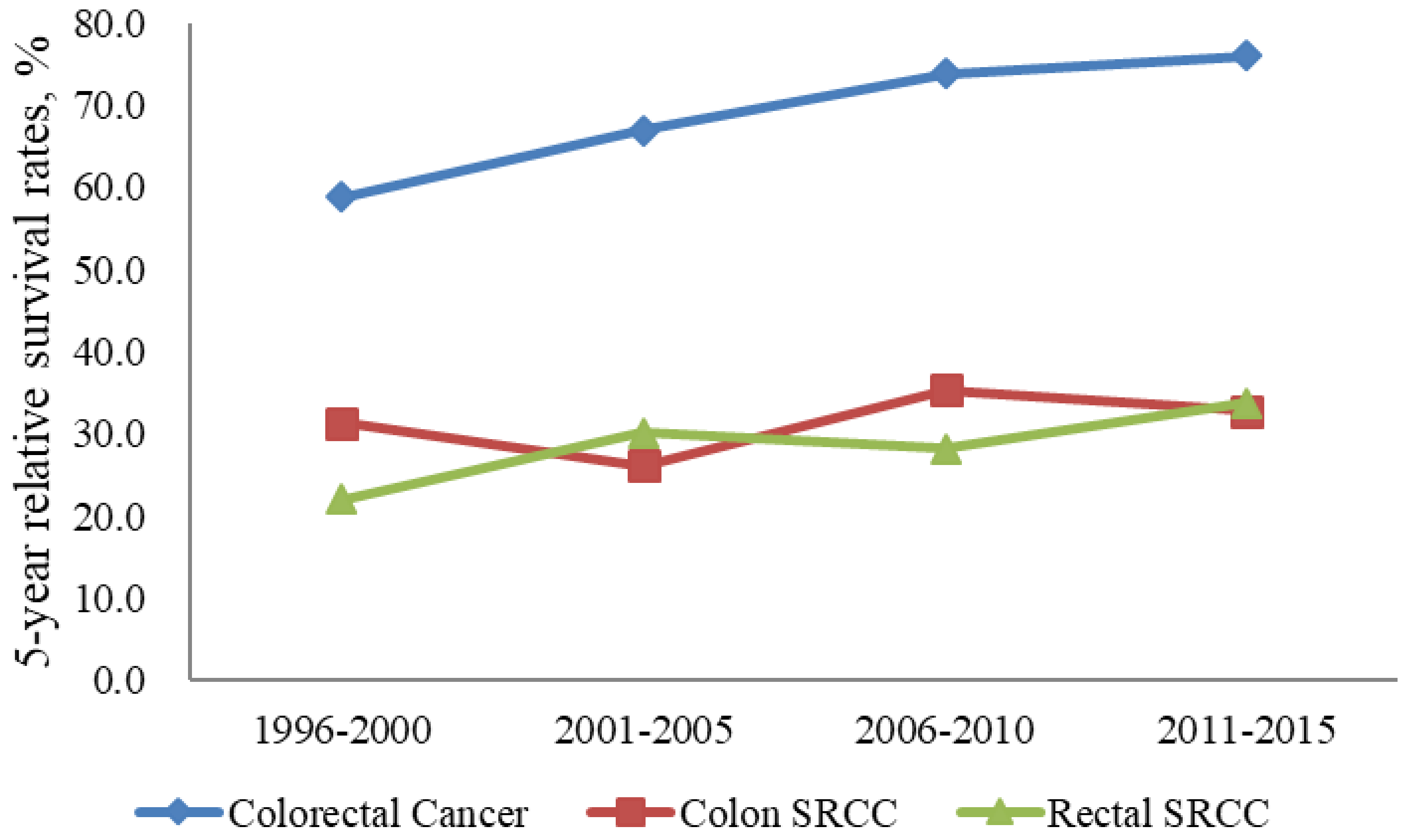
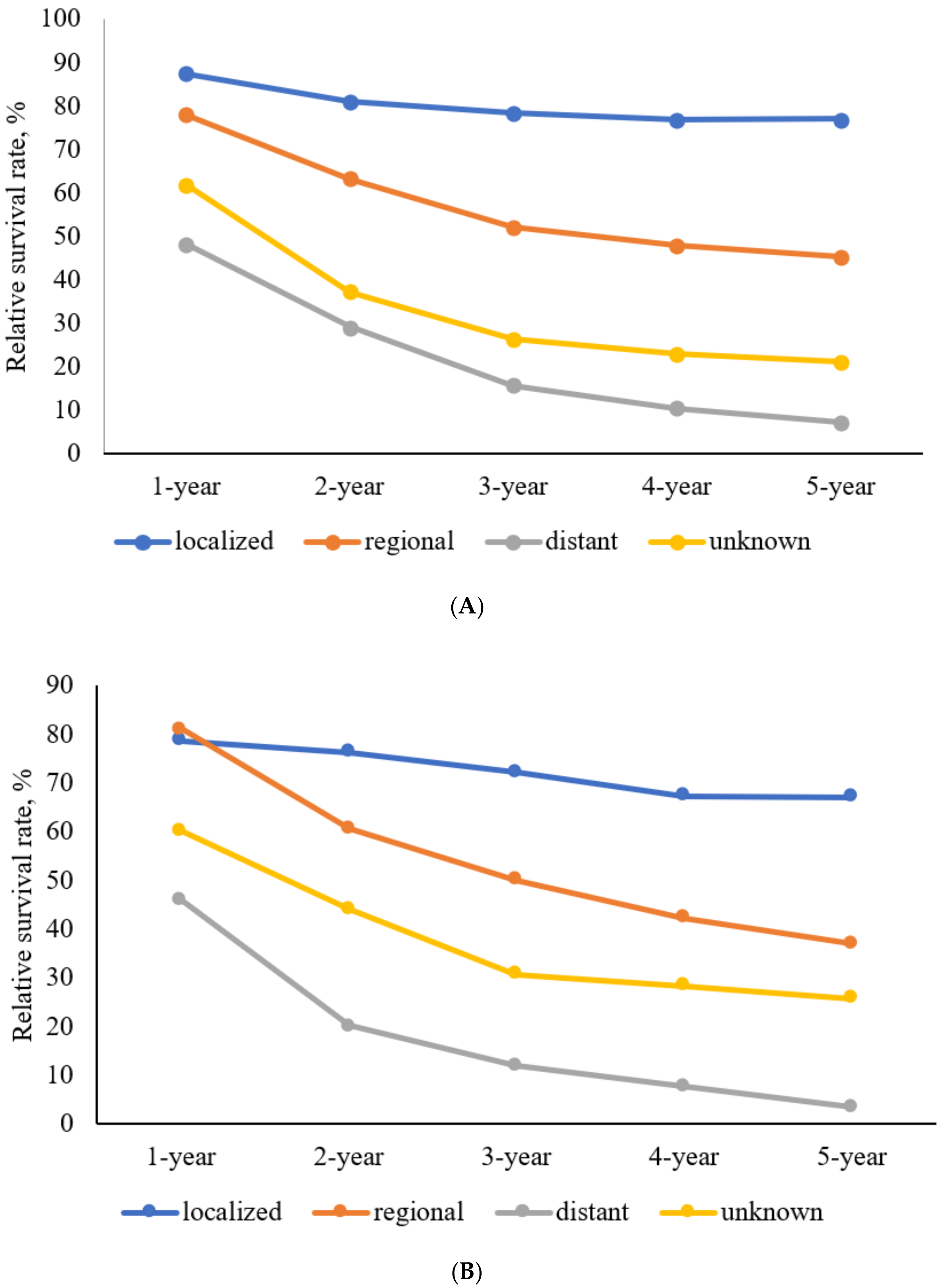
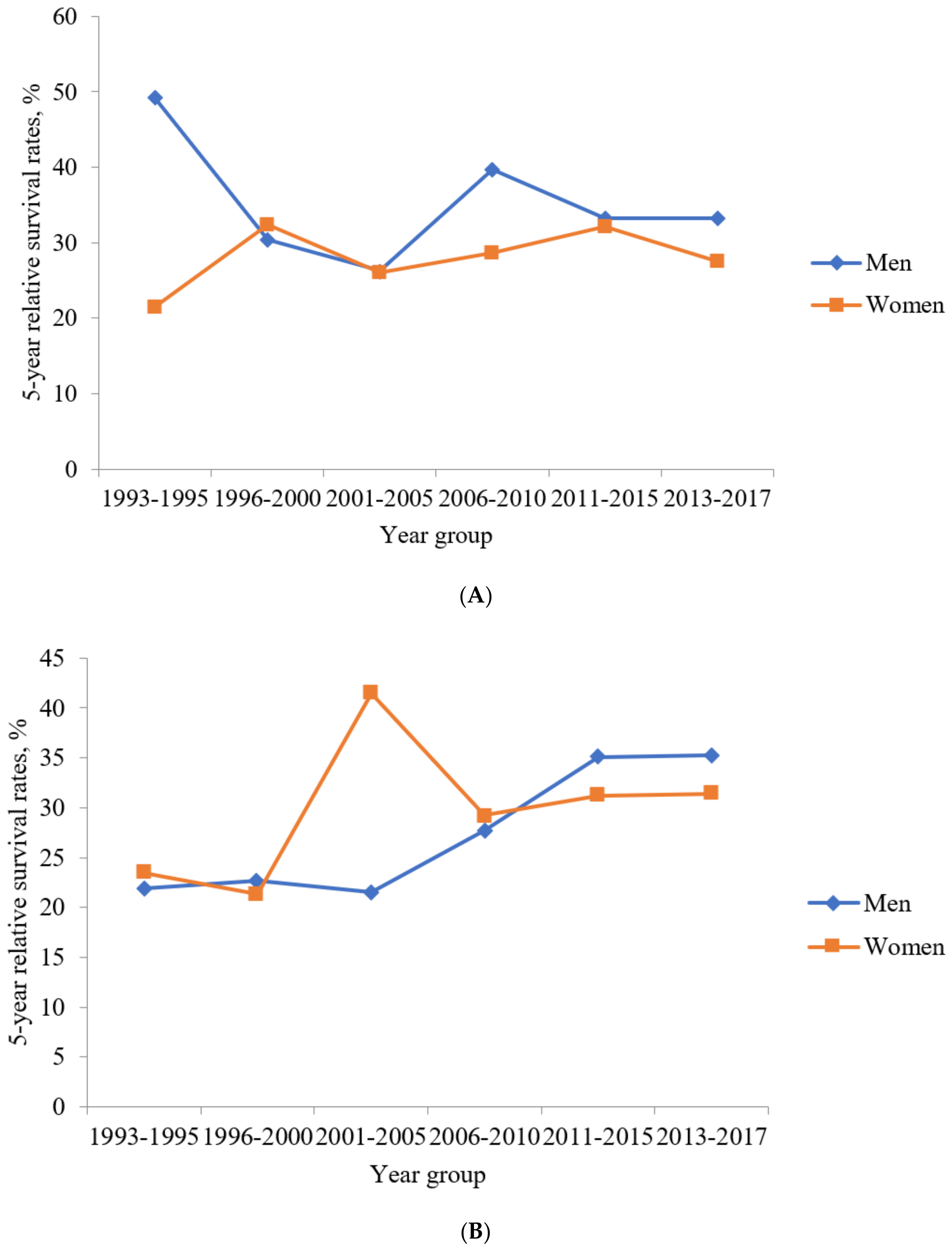
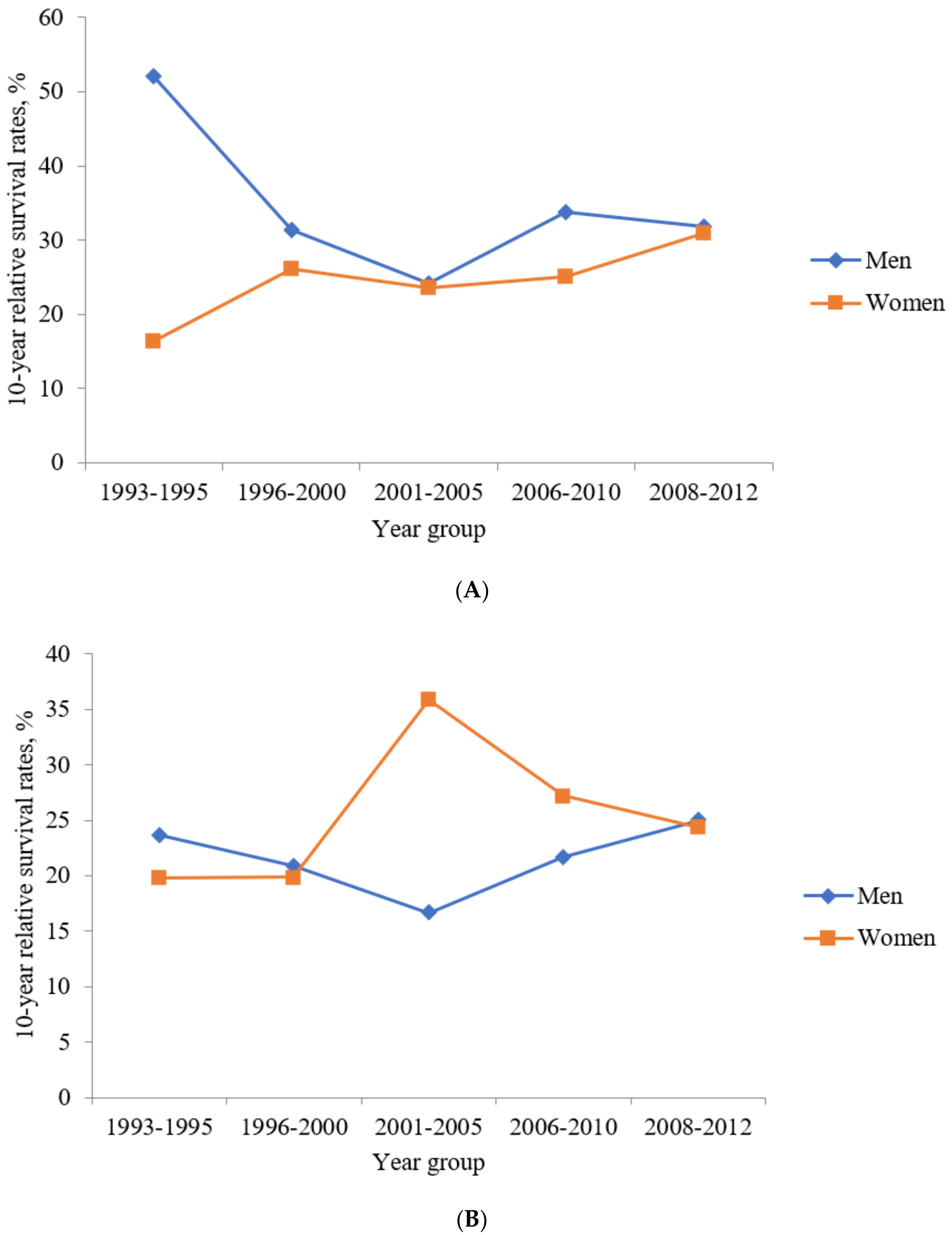
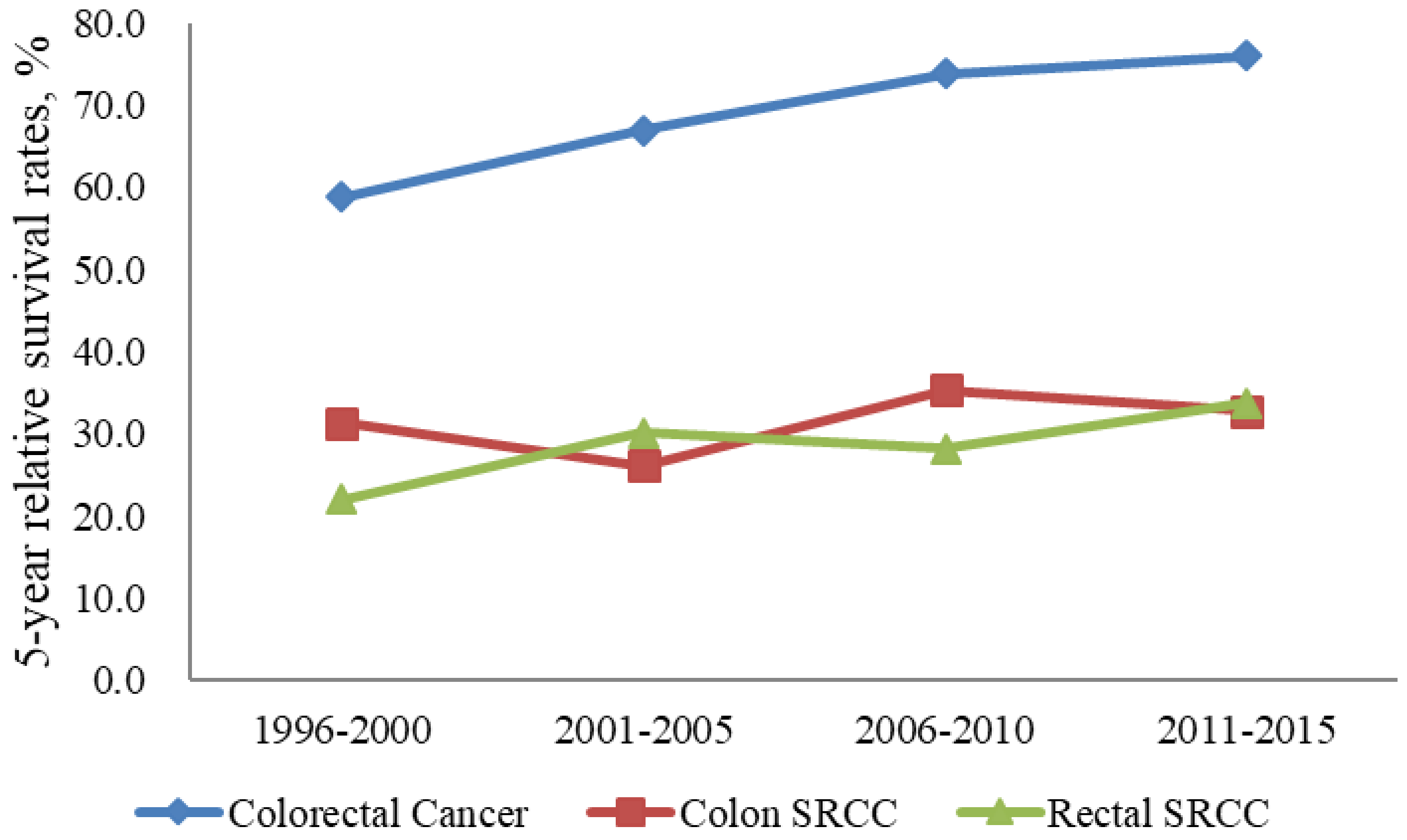
3.5. RSRs of Colon SRCC
3.6. RSRs of Rectum SRCC
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Byeon, J.S.; Yang, S.K.; Kim, T.I.; Kim, W.H.; Lau, J.Y.; Leung, W.K.; Fujita, R.; Makharia, G.K.; Abdullah, M.; Hilmi, I.; et al. Colorectal neoplasm in asymptomatic Asians: A prospective multinational multicenter colonoscopy survey. Gastrointest. Endosc. 2007, 65, 1015–1022. [Google Scholar] [CrossRef] [PubMed]
- Sung, J.J.; Lau, J.Y.; Goh, K.L.; Leung, W.K.; Asia Pacific Working Group on Colorectal Cancer. Increasing incidence of colorectal cancer in Asia: Implications for screening. Lancet Oncol. 2005, 6, 871–876. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Goding Sauer, A.; Fedewa, S.A.; Butterly, L.F.; Anderson, J.C.; Cercek, A.; Smith, R.A.; Jemal, A. Colorectal cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 145–164. [Google Scholar] [CrossRef] [Green Version]
- Hugen, N.; Verhoeven, R.H.; Lemmens, V.E.; van Aart, C.J.; Elferink, M.A.; Radema, S.A.; Nagtegaal, I.D.; de Wilt, J.H. Colorectal signet-ring cell carcinoma: Benefit from adjuvant chemotherapy but a poor prognostic factor. Int. J. Cancer 2015, 136, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Mizushima, T.; Nomura, M.; Fujii, M.; Akamatsu, H.; Mizuno, H.; Tominaga, H.; Hasegawa, J.; Nakajima, K.; Yasumasa, K.; Yoshikawa, M.; et al. Primary colorectal signet-ring cell carcinoma: Clinicopathological features and postoperative survival. Surg. Today 2010, 40, 234–238. [Google Scholar] [CrossRef]
- Nitsche, U.; Zimmermann, A.; Spath, C.; Muller, T.; Maak, M.; Schuster, T.; Slotta-Huspenina, J.; Kaser, S.A.; Michalski, C.W.; Janssen, K.P.; et al. Mucinous and signet-ring cell colorectal cancers differ from classical adenocarcinomas in tumor biology and prognosis. Ann. Surg. 2013, 258, 775–782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thota, R.; Fang, X.; Subbiah, S. Clinicopathological features and survival outcomes of primary signet ring cell and mucinous adenocarcinoma of colon: Retrospective analysis of VACCR database. J. Gastrointest. Oncol. 2014, 5, 18–24. [Google Scholar] [CrossRef]
- Kang, H.; O’Connell, J.B.; Maggard, M.A.; Sack, J.; Ko, C.Y. A 10-year outcomes evaluation of mucinous and signet-ring cell carcinoma of the colon and rectum. Dis. Colon Rectum 2005, 48, 1161–1168. [Google Scholar] [CrossRef] [PubMed]
- Hyngstrom, J.R.; Hu, C.Y.; Xing, Y.; You, Y.N.; Feig, B.W.; Skibber, J.M.; Rodriguez-Bigas, M.A.; Cormier, J.N.; Chang, G.J. Clinicopathology and outcomes for mucinous and signet ring colorectal adenocarcinoma: Analysis from the National Cancer Data Base. Ann. Surg. Oncol. 2012, 19, 2814–2821. [Google Scholar] [CrossRef] [Green Version]
- Borger, M.E.; Gosens, M.J.; Jeuken, J.W.; van Kempen, L.C.; van de Velde, C.J.; van Krieken, J.H.; Nagtegaal, I.D. Signet ring cell differentiation in mucinous colorectal carcinoma. J. Pathol. 2007, 212, 278–286. [Google Scholar] [CrossRef] [PubMed]
- Bosman, F.T.; Carneiro, F.; Hruban, R.H.; Theise, N.D. WHO Classification of Tumours of the Digestive System; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Messerini, L.; Palomba, A.; Zampi, G. Primary signet-ring cell carcinoma of the colon and rectum. Dis. Colon Rectum 1995, 38, 1189–1192. [Google Scholar] [CrossRef]
- Gopalan, V.; Smith, R.A.; Ho, Y.H.; Lam, A.K. Signet-ring cell carcinoma of colorectum--current perspectives and molecular biology. Int. J. Colorectal. Dis. 2011, 26, 127–133. [Google Scholar] [CrossRef] [Green Version]
- Hugen, N.; van de Velde, C.J.H.; de Wilt, J.H.W.; Nagtegaal, I.D. Metastatic pattern in colorectal cancer is strongly influenced by histological subtype. Ann. Oncol. 2014, 25, 651–657. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.S.; Hsieh, P.S.; Hung, S.Y.; Tang, R.; Tsai, W.S.; Changchien, C.R.; Lin, P.Y.; Wang, J.Y.; Yeh, C.Y. Clinical significance of signet ring cell rectal carcinoma. Int. J. Colorectal. Dis. 2004, 19, 102–107. [Google Scholar] [CrossRef]
- Nozoe, T.; Anai, H.; Nasu, S.; Sugimachi, K. Clinicopathological characteristics of mucinous carcinoma of the colon and rectum. J. Surg. Oncol. 2000, 75, 103–107. [Google Scholar] [CrossRef]
- Secco, G.B.; Fardelli, R.; Campora, E.; Lapertosa, G.; Gentile, R.; Zoli, S.; Prior, C. Primary mucinous adenocarcinomas and signet-ring cell carcinomas of colon and rectum. Oncology 1994, 51, 30–34. [Google Scholar] [CrossRef]
- Tung, S.Y.; Wu, C.S.; Chen, P.C. Primary signet ring cell carcinoma of colorectum: An age-and sex-matched controlled study. Am. J. Gastroenterol. 1996, 91, 2195–2199. [Google Scholar] [PubMed]
- Li, H.; Zong, Z.; Zhou, T.; Sun, L.; Wang, A.; Zhang, K.; Yi, C. Trends of incidence and survival in patients with gastroenteropancreatic signet ring cell carcinoma: An analysis from the Surveillance, Epidemiology, and End Results program. J. Gastrointest. Oncol. 2019, 10, 979–988. [Google Scholar] [CrossRef] [PubMed]
- Nitsche, U.; Friess, H.; Agha, A.; Angele, M.; Eckel, R.; Heitland, W.; Jauch, K.W.; Krenz, D.; Nussler, N.C.; Rau, H.G.; et al. Prognosis of mucinous and signet-ring cell colorectal cancer in a population-based cohort. J. Cancer Res. Clin. Oncol. 2016, 142, 2357–2366. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.L.; Wang, M.; He, P. Clinicopathological characteristics and survival in colorectal signet ring cell carcinoma: A population-based study. Sci. Rep. 2020, 10, 10460. [Google Scholar] [CrossRef]
- Lin, J.Z.; Qiu, M.Z.; Xu, R.H.; Dobs, A.S. Comparison of survival and clinicopathologic features in colorectal cancer among African American, Caucasian, and Chinese patients treated in the United States: Results from the surveillance epidemiology and end results (SEER) database. Oncotarget 2015, 6, 33935–33943. [Google Scholar] [CrossRef] [Green Version]
- Shin, H.R.; Won, Y.J.; Jung, K.W.; Kong, H.J.; Yim, S.H.; Lee, J.K.; Noh, H.I.; Lee, J.K.; Pisani, P.; Park, J.G.; et al. Nationwide cancer incidence in Korea, 1999~2001; first result using the national cancer incidence database. Cancer Res. Treat. 2005, 37, 325–331. [Google Scholar] [CrossRef] [Green Version]
- Benesch, M.G.; Mathieson, A. Epidemiology of signet ring cell adenocarcinomas. Cancers 2020, 12, 1544. [Google Scholar] [CrossRef] [PubMed]
- Nam, S.; Kim, D.; Jung, K.; Choi, Y.J.; Kang, J.G. Analysis of the incidence and clinical features of colorectal nonadenocarcinoma in Korea: A national cancer registry-based study. Ann. Coloproctol. 2020, 36, 390. [Google Scholar] [CrossRef]
- Hong, S.; Won, Y.J.; Park, Y.R.; Jung, K.W.; Kong, H.J.; Lee, E.S. The Community of Population-Based Regional Cancer Registries. Cancer statistics in Korea: Incidence, mortality, survival, and prevalence in 2017. Cancer Res. Treat. 2020, 52, 335–350. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J. Age standardization. In Cancer Incidence in Five Continents Vol. X, IARC Scientific Publications No. 164; Forman, D., Bray, F., Brewster, D.H., Gombe Mbalawa, C., Kohler, B., Piñeros, M., Steliarova-Foucher, E., Swaminathan, R., Eds.; International Agency for Research on Cancer: Lyon, France, 2014; pp. 112–115. [Google Scholar]
- Ederer, F.; Heise, H. Instructions to IBM 650 Programmers in Processing Survival Computations; Methodological Note; National Cancer Institute: Bethesda, MD, USA, 1959. [Google Scholar]
- Arifi, S.; Elmesbahi, O.; Amarti Riffi, A. Primary signet ring cell carcinoma of the colon and rectum. Bull. Cancer 2015, 102, 880–888. [Google Scholar] [CrossRef] [PubMed]
- Shi, T.; Huang, M.; Han, D.; Tang, X.; Chen, Y.; Li, Z.; Liu, C.; Xiang, D.; Wang, T.; Chen, Y. Chemotherapy is associated with increased survival from colorectal signet ring cell carcinoma with distant metastasis: A surveillance, epidemiology, and end results database analysis. Cancer Med. 2019, 8, 1930–1940. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, W.-S.; Chun, H.-K.; Lee, W.Y.; Yun, S.H.; Cho, Y.B.; Yun, H.-R.; Park, S.-H.; Song, S.Y. Treatment outcomes in patients with signet ring cell carcinoma of the colorectum. Am. J. Surg. 2007, 194, 294–298. [Google Scholar] [CrossRef]
- Pande, R.; Sunga, A.; LeVea, C.; Wilding, G.E.; Bshara, W.; Reid, M.; Fakih, M.G. Significance of signet-ring cells in patients with colorectal cancer. Dis. Colon Rectum 2008, 51, 50–55. [Google Scholar] [CrossRef]
- Jayanand, S.B.; Seshadri, R.A.; Tapkire, R. Signet ring cell histology and non-circumferential tumors predict pathological complete response following neoadjuvant chemoradiation in rectal cancers. Int. J. Colorectal Dis. 2011, 26, 23–27. [Google Scholar] [CrossRef]
- Kim, S.-E.; Paik, H.Y.; Yoon, H.; Lee, J.E.; Kim, N.; Sung, M.-K. Sex-and gender-specific disparities in colorectal cancer risk. World J. Gastroenterol. WJG 2015, 21, 5167. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Yan, N.; Pan, S.; Wang, D.-W.; Li, Z.-W. The value of adjuvant chemotherapy in stage II/III colorectal signet ring cell carcinoma. Sci. Rep. 2020, 10, 1–8. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | All (n) | Colon (C18) Signet-Ring Cell Carcinoma | |||||
|---|---|---|---|---|---|---|---|
| Crude Incidence Rate a | Age-Standardized Incidence Rate a | ||||||
| All | Men | Women | All | Men | Women | ||
| 1999 | 24 | 0.05 | 0.04 | 0.06 | 0.05 | 0.05 | 0.06 |
| 2000 | 38 | 0.08 | 0.08 | 0.08 | 0.08 | 0.08 | 0.08 |
| 2001 | 37 | 0.08 | 0.10 | 0.05 | 0.08 | 0.11 | 0.05 |
| 2002 | 62 | 0.13 | 0.16 | 0.10 | 0.12 | 0.16 | 0.09 |
| 2003 | 68 | 0.14 | 0.20 | 0.08 | 0.13 | 0.19 | 0.08 |
| 2004 | 71 | 0.15 | 0.19 | 0.10 | 0.13 | 0.18 | 0.09 |
| 2005 | 79 | 0.16 | 0.20 | 0.13 | 0.14 | 0.18 | 0.11 |
| 2006 | 92 | 0.19 | 0.24 | 0.14 | 0.17 | 0.21 | 0.12 |
| 2007 | 95 | 0.19 | 0.22 | 0.16 | 0.17 | 0.20 | 0.14 |
| 2008 | 79 | 0.16 | 0.21 | 0.11 | 0.13 | 0.19 | 0.09 |
| 2009 | 109 | 0.22 | 0.24 | 0.20 | 0.18 | 0.20 | 0.16 |
| 2010 | 108 | 0.22 | 0.28 | 0.16 | 0.17 | 0.23 | 0.12 |
| 2011 | 116 | 0.23 | 0.28 | 0.18 | 0.18 | 0.23 | 0.13 |
| 2012 | 118 | 0.23 | 0.27 | 0.19 | 0.18 | 0.22 | 0.15 |
| 2013 | 127 | 0.25 | 0.30 | 0.21 | 0.19 | 0.24 | 0.15 |
| 2014 | 117 | 0.23 | 0.27 | 0.19 | 0.17 | 0.20 | 0.15 |
| 2015 | 122 | 0.24 | 0.27 | 0.21 | 0.17 | 0.20 | 0.14 |
| 2016 | 135 | 0.26 | 0.26 | 0.27 | 0.18 | 0.19 | 0.18 |
| 2017 | 116 | 0.23 | 0.27 | 0.19 | 0.17 | 0.20 | 0.14 |
| Year | All (n) | Rectum (C19–20) Signet-Ring Cell Carcinoma | |||||
|---|---|---|---|---|---|---|---|
| Crude Incidence Rate a | Age-Standardized Incidence Rate a | ||||||
| All | Men | Women | All | Men | Women | ||
| 1999 | 34 | 0.07 | 0.08 | 0.07 | 0.07 | 0.08 | 0.07 |
| 2000 | 27 | 0.06 | 0.06 | 0.05 | 0.06 | 0.07 | 0.05 |
| 2001 | 35 | 0.07 | 0.06 | 0.08 | 0.07 | 0.06 | 0.08 |
| 2002 | 44 | 0.09 | 0.11 | 0.08 | 0.09 | 0.11 | 0.07 |
| 2003 | 34 | 0.07 | 0.08 | 0.06 | 0.07 | 0.08 | 0.06 |
| 2004 | 59 | 0.12 | 0.16 | 0.08 | 0.11 | 0.15 | 0.07 |
| 2005 | 45 | 0.09 | 0.10 | 0.08 | 0.08 | 0.10 | 0.07 |
| 2006 | 47 | 0.10 | 0.13 | 0.06 | 0.08 | 0.12 | 0.05 |
| 2007 | 56 | 0.11 | 0.14 | 0.09 | 0.10 | 0.12 | 0.07 |
| 2008 | 47 | 0.10 | 0.13 | 0.06 | 0.08 | 0.12 | 0.05 |
| 2009 | 71 | 0.14 | 0.18 | 0.10 | 0.11 | 0.15 | 0.08 |
| 2010 | 62 | 0.12 | 0.17 | 0.08 | 0.10 | 0.14 | 0.06 |
| 2011 | 69 | 0.14 | 0.19 | 0.09 | 0.10 | 0.14 | 0.06 |
| 2012 | 63 | 0.13 | 0.17 | 0.08 | 0.09 | 0.13 | 0.06 |
| 2013 | 61 | 0.12 | 0.14 | 0.10 | 0.09 | 0.11 | 0.07 |
| 2014 | 68 | 0.13 | 0.20 | 0.07 | 0.10 | 0.14 | 0.06 |
| 2015 | 67 | 0.13 | 0.16 | 0.10 | 0.10 | 0.11 | 0.09 |
| 2016 | 59 | 0.12 | 0.14 | 0.09 | 0.08 | 0.10 | 0.06 |
| 2017 | 52 | 0.10 | 0.15 | 0.05 | 0.07 | 0.11 | 0.04 |
| Year | Men | Women | ||||||
|---|---|---|---|---|---|---|---|---|
| Localized | Regional | Distant | Unknown | Localized | Regional | Distant | Unknown | |
| 2005 | 10.4 | 33.3 | 39.6 | 16.7 | 9.7 | 38.7 | 45.2 | 6.5 |
| 2006 | 13.8 | 46.6 | 24.1 | 15.5 | 20.6 | 44.1 | 26.5 | 8.8 |
| 2007 | 5.5 | 58.2 | 23.6 | 12.7 | 5.0 | 47.5 | 37.5 | 10.0 |
| 2008 | 18.9 | 47.2 | 34.0 | 0.0 | 7.7 | 50.0 | 42.3 | 0.0 |
| 2009 | 20.0 | 41.7 | 35.0 | 3.3 | 14.3 | 44.9 | 34.7 | 6.1 |
| 2010 | 11.6 | 58.0 | 29.0 | 1.4 | 5.1 | 43.6 | 46.2 | 5.1 |
| 2011 | 21.1 | 36.6 | 36.6 | 5.6 | 13.3 | 37.8 | 46.7 | 2.2 |
| 2012 | 10.1 | 43.5 | 37.7 | 8.7 | 14.3 | 53.1 | 30.6 | 2.0 |
| 2013 | 6.7 | 44.0 | 44.0 | 5.3 | 9.6 | 50.0 | 38.5 | 1.9 |
| 2014 | 13.2 | 60.3 | 26.5 | 0.0 | 10.2 | 38.8 | 51.0 | 0.0 |
| 2015 | 11.8 | 48.5 | 35.3 | 4.4 | 11.1 | 40.7 | 40.7 | 7.4 |
| 2016 | 13.6 | 37.9 | 42.4 | 6.1 | 8.7 | 52.2 | 31.9 | 7.2 |
| 2017 | 13.2 | 45.6 | 35.3 | 5.9 | 16.7 | 43.8 | 35.4 | 4.2 |
| Year | Men | Women | ||||||
|---|---|---|---|---|---|---|---|---|
| Localized | Regional | Distant | Unknown | Localized | Regional | Distant | Unknown | |
| 2005 | 8.0 | 52.0 | 36.0 | 4.0 | 10.0 | 35.0 | 35.0 | 20.0 |
| 2006 | 9.4 | 59.4 | 18.8 | 12.5 | 20.0 | 46.7 | 26.7 | 6.7 |
| 2007 | 17.1 | 57.1 | 14.3 | 11.4 | 4.8 | 57.1 | 28.6 | 9.5 |
| 2008 | 6.1 | 45.5 | 39.4 | 9.1 | 14.3 | 57.1 | 21.4 | 7.1 |
| 2009 | 8.9 | 46.7 | 37.8 | 6.7 | 11.5 | 42.3 | 19.2 | 26.9 |
| 2010 | 20.9 | 55.8 | 18.6 | 4.7 | 15.8 | 42.1 | 42.1 | 0.0 |
| 2011 | 19.1 | 61.7 | 17.0 | 2.1 | 13.6 | 63.6 | 18.2 | 4.5 |
| 2012 | 11.6 | 46.5 | 37.2 | 4.7 | 20.0 | 45.0 | 35.0 | 0.0 |
| 2013 | 5.6 | 50.0 | 36.1 | 8.3 | 12.0 | 68.0 | 16.0 | 4.0 |
| 2014 | 12.0 | 64.0 | 20.0 | 4.0 | 5.6 | 50.0 | 38.9 | 5.6 |
| 2015 | 4.9 | 51.2 | 36.6 | 7.3 | 19.2 | 53.8 | 15.4 | 11.5 |
| 2016 | 10.8 | 59.5 | 24.3 | 5.4 | 18.2 | 54.5 | 27.3 | 0.0 |
| 2017 | 2.6 | 60.5 | 28.9 | 7.9 | 21.4 | 28.6 | 50.0 | 0.0 |
| SEER Stage | Relative Survival Rates (%) | |||||
|---|---|---|---|---|---|---|
| 1-Year | 2-Year | 3-Year | 4-Year | 5-Year | ||
| Men | Localized | 88.5 | 81.8 | 79.5 | 78.1 | 79.3 |
| Regional | 78.2 | 65.4 | 54.0 | 49.3 | 46.5 | |
| Distant | 48.2 | 30.3 | 17.1 | 10.6 | 8.5 | |
| Unknown | 62.1 | 37.8 | 31.0 | 25.9 | 23.3 | |
| Women | Localized | 86.0 | 79.8 | 76.5 | 75.1 | 73.4 |
| Regional | 77.7 | 60.2 | 49.7 | 46.2 | 44.0 | |
| Distant | 48.6 | 27.9 | 14.1 | 10.3 | 5.9 | |
| Unknown | 61.4 | 36.3 | 17.1 | 17.3 | 17.4 | |
| SEER Stage | Relative Survival Rates (%) | |||||
|---|---|---|---|---|---|---|
| 1-Year | 2-Year | 3-Year | 4-Year | 5-Year | ||
| Men | Localized | 83.4 | 78.5 | 73.3 | 67.1 | 68.3 |
| Regional | 80.5 | 59.3 | 48.8 | 41.6 | 36.0 | |
| Distant | 46.7 | 21.0 | 11.3 | 8.0 | 4.0 | |
| Unknown | 48.0 | 40.5 | 30.7 | 25.4 | 25.7 | |
| Women | Localized | 72.0 | 73.2 | 71.0 | 68.2 | 65.2 |
| Regional | 82.8 | 63.6 | 52.6 | 44.0 | 39.2 | |
| Distant | 44.7 | 18.6 | 13.0 | 7.1 | 2.4 | |
| Unknown | 78.8 | 50.0 | 32.0 | 32.9 | 27.2 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.-H.; Kim, H.; Kim, J.W.; Kim, H.M. Trends in the Incidence and Survival Rates of Colorectal Signet-Ring Cell Carcinoma in the South Korean Population: Analysis of the Korea Central Cancer Registry Database. J. Clin. Med. 2021, 10, 4258. https://doi.org/10.3390/jcm10184258
Kim J-H, Kim H, Kim JW, Kim HM. Trends in the Incidence and Survival Rates of Colorectal Signet-Ring Cell Carcinoma in the South Korean Population: Analysis of the Korea Central Cancer Registry Database. Journal of Clinical Medicine. 2021; 10(18):4258. https://doi.org/10.3390/jcm10184258
Chicago/Turabian StyleKim, Ji-Hoon, Hyunil Kim, Jin Woo Kim, and Hee Man Kim. 2021. "Trends in the Incidence and Survival Rates of Colorectal Signet-Ring Cell Carcinoma in the South Korean Population: Analysis of the Korea Central Cancer Registry Database" Journal of Clinical Medicine 10, no. 18: 4258. https://doi.org/10.3390/jcm10184258
APA StyleKim, J.-H., Kim, H., Kim, J. W., & Kim, H. M. (2021). Trends in the Incidence and Survival Rates of Colorectal Signet-Ring Cell Carcinoma in the South Korean Population: Analysis of the Korea Central Cancer Registry Database. Journal of Clinical Medicine, 10(18), 4258. https://doi.org/10.3390/jcm10184258