
Rapid Response System Improves Sepsis Bundle Compliances and Survival in Hospital Wards for 10 Years

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethical Approval
2.2. Data Collection and Definitions
2.3. Role of Rapid Response Systems (RRS) in Sepsis
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rhee, C.; Jones, T.M.; Hamad, Y.; Pande, A.; Varon, J.; O’Brien, C.; Anderson, D.J.; Warren, D.K.; Dantes, R.B.; Epstein, L.; et al. Centers for Disease Control and Prevention (CDC) Prevention Epicenters Program: Prevalence, underlying causes, and preventability of sepsis-associated mortality in US acute care hospitals. JAMA Netw. Open 2019, 2, e187571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rivers, E.; Nguyen, B.; Havstad, S.; Ressler, J.; Muzzin, A.; Knoblich, B.; Peterson, E.; Tomlanovich, M. Early Goal-Directed Therapy Collaborative Group: Early goal-directed therapy in the treatment of severe sepsis and septic shock. N. Engl. J. Med. 2001, 345, 1368–1377. [Google Scholar] [CrossRef] [Green Version]
- Seymour, C.W.; Gesten, F.; Prescott, H.C.; Friedrich, M.E.; Iwashyna, T.J.; Phillips, G.S.; Lemeshow, S.; Osborn, T.; Terry, K.M.; Levy, M.M. Time to treatment and mortality during mandated emergency care for sepsis. N. Engl. J. Med. 2017, 376, 2235–2244. [Google Scholar] [CrossRef]
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving sepsis campaign: International guidelines for management of sepsis and septic shock: 2016. Crit. Care Med. 2017, 45, 486–552. [Google Scholar] [CrossRef] [PubMed]
- Levy, M.M.; Evans, L.E.; Rhodes, A. The surviving sepsis campaign bundle: 2018 update. Crit. Care Med. 2018, 46, 997–1000. [Google Scholar] [CrossRef]
- Levy, M.M.; Rhodes, A.; Phillips, G.S.; Townsend, S.R.; Schorr, C.A.; Beale, R.; Osborn, T.; Lemeshow, S.; Chiche, J.D.; Artigas, A.; et al. Surviving sepsis campaign: Association between performance metrics and outcomes in a 7.5-year study. Intensive Care Med. 2014, 40, 1623–1633. [Google Scholar] [CrossRef] [PubMed]
- Page, D.B.; Donnelly, J.P.; Wang, H.E. Community-, healthcare-, and hospital-acquired severe sepsis hospitalizations in the university healthsystem consortium. Crit. Care Med. 2015, 43, 1945–1951. [Google Scholar] [CrossRef]
- Baghdadi, J.D.; Brook, R.H.; Uslan, D.Z.; Needleman, J.; Bell, D.S.; Cunningham, W.E.; Wong, M.D. Association of a care bundle for early sepsis management with mortality among patients with hospital-onset or community-onset sepsis. JAMA Intern. Med. 2020, 180, 707–716. [Google Scholar] [CrossRef]
- Bhattacharjee, P.; Edelson, D.P.; Churpek, M.M. Identifying patients with sepsis on the hospital wards. Chest 2017, 151, 898–907. [Google Scholar] [CrossRef] [Green Version]
- Teles, F.; Rodrigues, W.G.; Alves, M.G.T.C.; Albuquerque, C.F.T.; Bastos, S.M.O.; Mota, M.F.A.; Mota, E.S.; Silva, F.J.L. Impact of a sepsis bundle in wards of a tertiary hospital. J. Intensive Care 2017, 5, 45. [Google Scholar] [CrossRef] [Green Version]
- Dellinger, R.P.; Levy, M.M.; Rhodes, A.; Annane, D.; Gerlach, H.; Opal, S.M.; Sevransky, J.E.; Sprung, C.L.; Douglas, I.S.; Jaeschke, R.; et al. Surviving Sepsis Campaign Guidelines Committee including the Pediatric Subgroup: Surviving sepsis campaign: International guidelines for management of severe sepsis and septic shock: 2012. Crit. Care Med. 2013, 41, 580–637. [Google Scholar] [CrossRef]
- Rhee, C.; Wang, R.; Zhang, Z.; Fram, D.; Kadri, S.S.; Klompas, M. CDC Prevention Epicenters Program: Epidemiology of hospital-onset versus community-onset sepsis in U.S. hospitals and association with mortality: A retrospective analysis using electronic clinical data. Crit. Care Med. 2019, 47, 1169–1176. [Google Scholar] [CrossRef]
- Baghdadi, J.D.; Wong, M.D.; Uslan, D.Z.; Bell, D.; Cunningham, W.E.; Needleman, J.; Kerbel, R.; Brook, R. Adherence to the SEP-1 sepsis bundle in hospital-onset v. community-onset sepsis: A multicenter retrospective cohort study. J. Gen. Intern. Med. 2020, 35, 1153–1160. [Google Scholar] [CrossRef] [PubMed]
- Rhee, C.; Filbin, M.; Massaro, A.F.; Bulger, A.; McEachern, D.; Tobin, K.A.; Kitch, B.; Thurlo-Walsh, B.; Kadar, A.; Koffman, A.; et al. Centers for Disease Control and Prevention (CDC) Prevention Epicenters Program: Compliance with the national SEP-1 quality measure and association with sepsis outcomes: A multicenter retrospective cohort study. Crit. Care Med. 2018, 46, 1585–1591. [Google Scholar] [CrossRef] [PubMed]
- Scheer, C.S.; Fuchs, C.; Gründling, M.; Vollmer, M.; Bast, J.; Bohnert, J.A.; Zimmermann, K.; Hahnenkamp, K.; Rehberg, S.; Kuhn, S.O. Impact of antibiotic administration on blood culture positivity at the beginning of sepsis: A prospective clinical cohort study. Clin. Microbiol. Infect. 2019, 25, 326–331. [Google Scholar] [CrossRef] [Green Version]
- Gu, W.J.; Zhang, Z.; Bakker, J. Early lactate clearance-guided therapy in patients with sepsis: A meta-analysis with trial sequential analysis of randomized controlled trials. Intensive Care Med. 2015, 41, 1862–1863. [Google Scholar] [CrossRef]
- Pan, J.; Peng, M.; Liao, C.; Hu, X.; Wang, A.; Li, X. Relative efficacy and safety of early lactate clearance-guided therapy resuscitation in patients with sepsis: A meta-analysis. Medicine 2019, 98, e14453. [Google Scholar] [CrossRef] [PubMed]
- Burston, J.; Adhikari, S.; Hayen, A.; Doolan, H.; Kelly, M.L.; Fu, K.; Jensen, T.O.; Konecny, P. A role for antimicrobial stewardship in clinical sepsis pathways: A prospective Interventional Study. Infect. Control Hosp. Epidemiol. 2017, 38, 1032–1038. [Google Scholar] [CrossRef] [Green Version]
- Rhee, C.; Brown, S.R.; Jones, T.M.; O’Brien, C.; Pande, A.; Hamad, Y.; Bulger, A.L.; Tobin, K.A.; Massaro, A.F.; Anderson, D.J.; et al. CDC Prevention Epicenters Program: Variability in determining sepsis time zero and bundle compliance rates for the centers for medicare and medicaid services SEP-1 measure. Infect. Control Hosp. Epidemiol. 2018, 39, 994–996. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sebat, F.; Musthafa, A.A.; Johnson, D.; Kramer, A.A.; Shoffner, D.; Eliason, M.; Henry, K.; Spurlock, B. Effect of a rapid response system for patients in shock on time to treatment and mortality during 5 years. Crit. Care Med. 2007, 35, 2568–2575. [Google Scholar] [CrossRef]
- Scheer, C.S.; Fuchs, C.; Kuhn, S.O.; Vollmer, M.; Rehberg, S.; Friesecke, S.; Abel, P.; Balau, V.; Bandt, C.; Meissner, K.; et al. Quality improvement initiative for severe sepsis and septic shock reduces 90-day mortality: A 7.5-year observational study. Crit. Care Med. 2017, 45, 241–252. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Variables | All (n = 976) |
|---|---|
| Measurement of lactate/3 h | 939 (96.2) |
| Obtain blood cultures/3 h | 791 (81.0) |
| Administer broad-spectrum intravenous antibiotics/3 h | 940 (96.3) |
| Administer 30 mL/kg crystalloid/3 h | 885 (90.7) |
| Application of vasopressors/6 h | 976 (100.0) |
| Repeat the lactate measurement/6 h | 789 (80.8) |
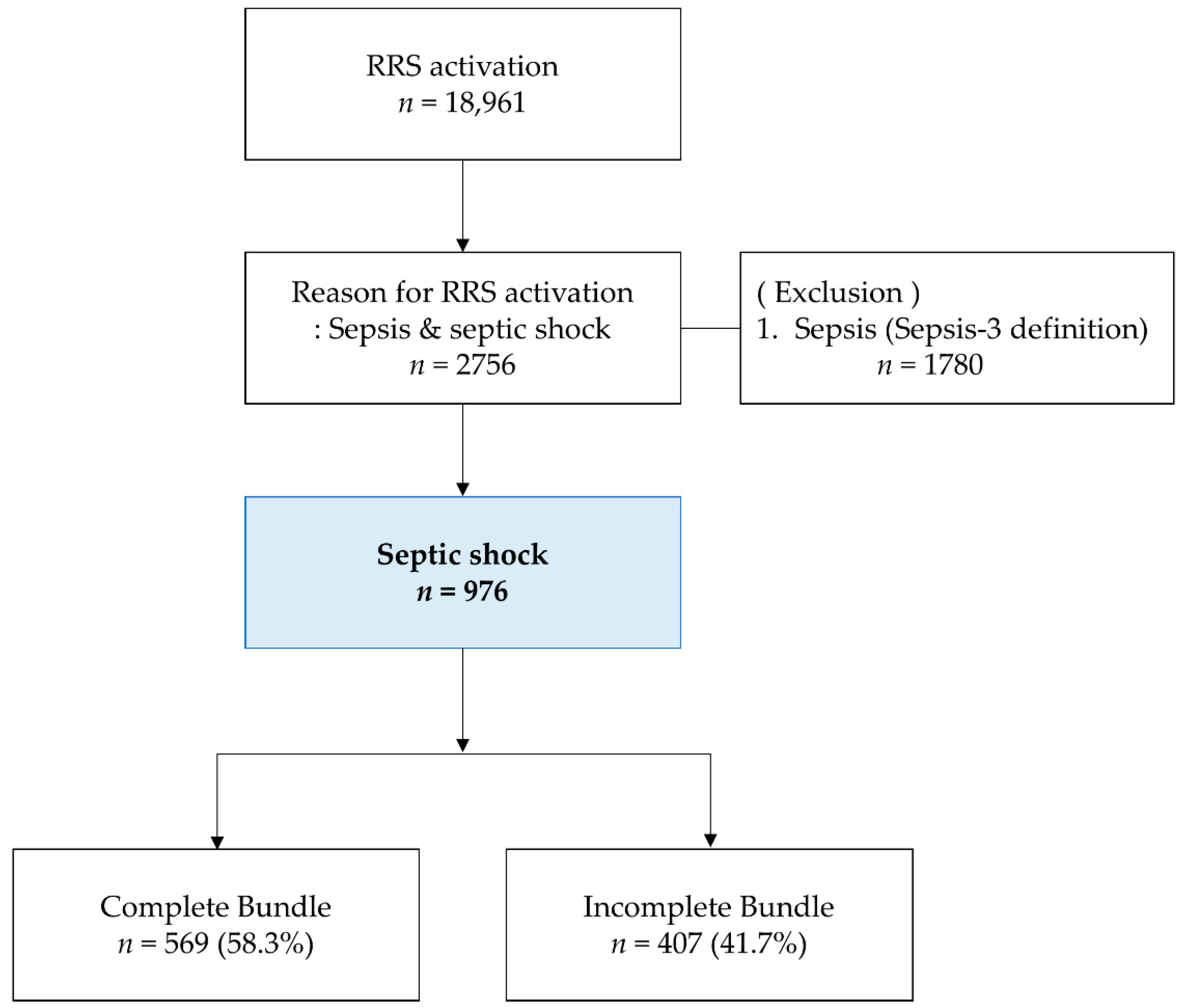
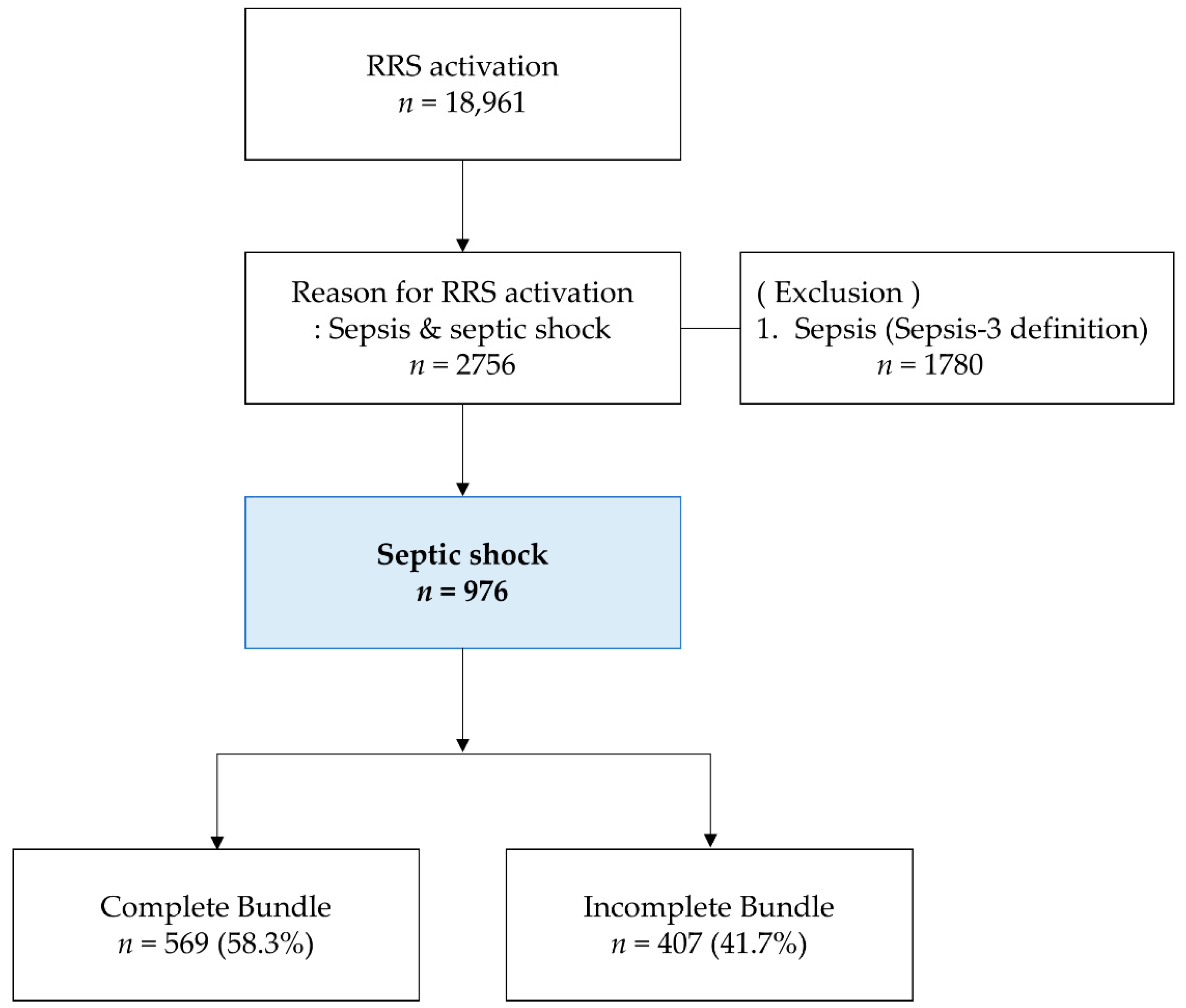
| Complete bundle. overall | 569 (58.3) |
| Variables | All (n = 976) | Complete Bundle (n = 569) | Incomplete Bundle (n = 407) | p-Value |
|---|---|---|---|---|
| 6hour total fluid (L), mean (SD) | 2.10 ± 1.33 | 2.34 ± 1.26 | 1.77 ± 1.36 | <0.001 |
| Use of vasopressor, n (%) | ||||
| Dopamine | 50 (5.1) | 23 (4.0) | 27 (6.6) | 0.049 |
| Norepinephrine | 969 (99.3) | 567 (99.6) | 402 (98.8) | 0.113 |
| Vasopressin | 321 (32.9) | 230 (40.4) | 91 (22.4) | <0.001 |
| Epinephrine | 96 (9.8) | 68 (12.0) | 28 (6.9) | 0.005 |
| Point of care ultrasound, n (%) | 359 (36.8) | 256 (45.0) | 103 (25.3) | <0.001 |
| Arterial catheter, n (%) | 66.1 (67.7) | 413 (72.6) | 248 (60.9) | <0.001 |
| Central venous catheter, n (%) | 774 (79.3) | 458 (80.5) | 316 (77.6) | 0.158 |
| Ventilator support, n (%) | 343 (35.1) | 184 (32.3) | 159 (39.1) | 0.018 |
| Use of inotropic agent, n (%) | 95 (9.7) | 49 (8.6) | 46 (11.3) | 0.099 |
| Transfusion of RBC, n (%) | 231 (23.7) | 141 (24.8) | 90 (22.1) | 0.187 |
| Use of corticosteroid therapy, n (%) | 266 (27.3) | 158 (27.8) | 108 (26.5) | 0.363 |
| Source control, n (%) | 169 (17.3) | 115 (20.2) | 54 (13.3) | 0.003 |
| Variables | All (n = 976) | Complete Bundle (n = 569) | Incomplete Bundle (n = 407) | p-Value |
|---|---|---|---|---|
| Transfer to ICU, n (%) | 578 (59.2) | 355 (62.4) | 223 (54.8) | 0.010 |
| 28-day mortality, n (%) | 429 (44.0) | 211 (37.1) | 218 (53.6) | <0.001 |
| Hospital mortality, n (%) | 473 (48.5) | 241 (42.4) | 232 (57.0) | <0.001 |
| Variables | Simple Logistic Regression | Multiple Logistic Regression | ||
|---|---|---|---|---|
| Unadjusted OR (95% CI) | p-Value | Adjusted OR (95% CI) | p-Value | |
| Age | 1.00 (0.99–1.01) | 0.823 | 1.01 (0.99–1.02) | 0.237 |
| Male | 0.95 (0.73–1.23) | 0.701 | 1.21 (0.83–1.78) | 0.325 |
| Call type (Screening/Direct call) | 1.35 (1.04–1.74) | 0.022 | 0.93 (0.63–1.36) | 0.691 |
| Complete bundle | 0.51 (0.40–0.66) | <0.001 | 0.61 (0.40–0.91) | 0.017 |
| Mechanical ventilator support | 2.77 (2.11–3.62) | <0.001 | 0.88 (0.88–1.43) | 0.611 |
| Positive blood culture | 0.73 (0.56–0.93) | 0.013 | 0.71 (0.48–1.04) | 0.086 |
| Lactate (time zero), mmol/L | 1.13 (1.08–1.18) | <0.001 | 0.93 (0.84–1.03) | 0.139 |
| Lactate (re-measurement), mmol/L | 1.20 (1.14–1.26) | <0.001 | 1.20 (1.12–1.29) | <0.001 |
| C-reactive protein, mg/L | 1.04 (1.03–1.06) | <0.001 | 1.04 (1.02–1.06) | <0.001 |
| Procalcitonin, ng/mL | 1.00 (1.00–1.00) | 0.574 | 1.00 (1.00–1.00) | 0.840 |
| 6 h total fluid, L | 1.00 (0.91–1.10) | 0.960 | 1.10 (0.53–1.29) | 0.200 |
| Arterial catheter | 1.35 (1.02–1.77) | 0.033 | 0.59 (0.38–0.91) | 0.018 |
| Central venous catheter | 1.10 (0.81–1.51) | 0.546 | 0.82 (0.49–1.37) | 0.439 |
| Point of care ultrasound | 0.84 (0.65–1.09) | 0.190 | 0.99 (0.37–1.45) | 0.953 |
| Use of inotropic agent | 1.40 (0.92–2.15) | 1.404 | 0.84 (0.45–1.55) | 0.569 |
| Transfusion of RBC | 1.42 (1.06–1.92) | 0.019 | 1.17 (0.75–1.83) | 0.489 |
| Use of corticosteroid therapy | 1.49 (1.12–1.98) | 0.006 | 0.89 (0.58–1.39) | 0.621 |
| Source control | 0.40 (0.28–0.58) | <0.001 | 0.50 (0.30–0.84) | 0.008 |
| SOFA score | 1.35 (1.29–1.42) | <0.001 | 1.33 (1.23–1.44) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, S.; Son, J.; Oh, D.K.; Huh, J.W.; Lim, C.-M.; Hong, S.-B. Rapid Response System Improves Sepsis Bundle Compliances and Survival in Hospital Wards for 10 Years. J. Clin. Med. 2021, 10, 4244. https://doi.org/10.3390/jcm10184244
Choi S, Son J, Oh DK, Huh JW, Lim C-M, Hong S-B. Rapid Response System Improves Sepsis Bundle Compliances and Survival in Hospital Wards for 10 Years. Journal of Clinical Medicine. 2021; 10(18):4244. https://doi.org/10.3390/jcm10184244
Chicago/Turabian StyleChoi, Sunhui, Jeongsuk Son, Dong Kyu Oh, Jin Won Huh, Chae-Man Lim, and Sang-Bum Hong. 2021. "Rapid Response System Improves Sepsis Bundle Compliances and Survival in Hospital Wards for 10 Years" Journal of Clinical Medicine 10, no. 18: 4244. https://doi.org/10.3390/jcm10184244
APA StyleChoi, S., Son, J., Oh, D. K., Huh, J. W., Lim, C.-M., & Hong, S.-B. (2021). Rapid Response System Improves Sepsis Bundle Compliances and Survival in Hospital Wards for 10 Years. Journal of Clinical Medicine, 10(18), 4244. https://doi.org/10.3390/jcm10184244