
JAK Inhibition with Ruxolitinib in Patients with COVID-19 and Severe Pneumonia: Multicenter Clinical Experience from a Compassionate Use Program in Italy

 ,
,  , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Experimental Section
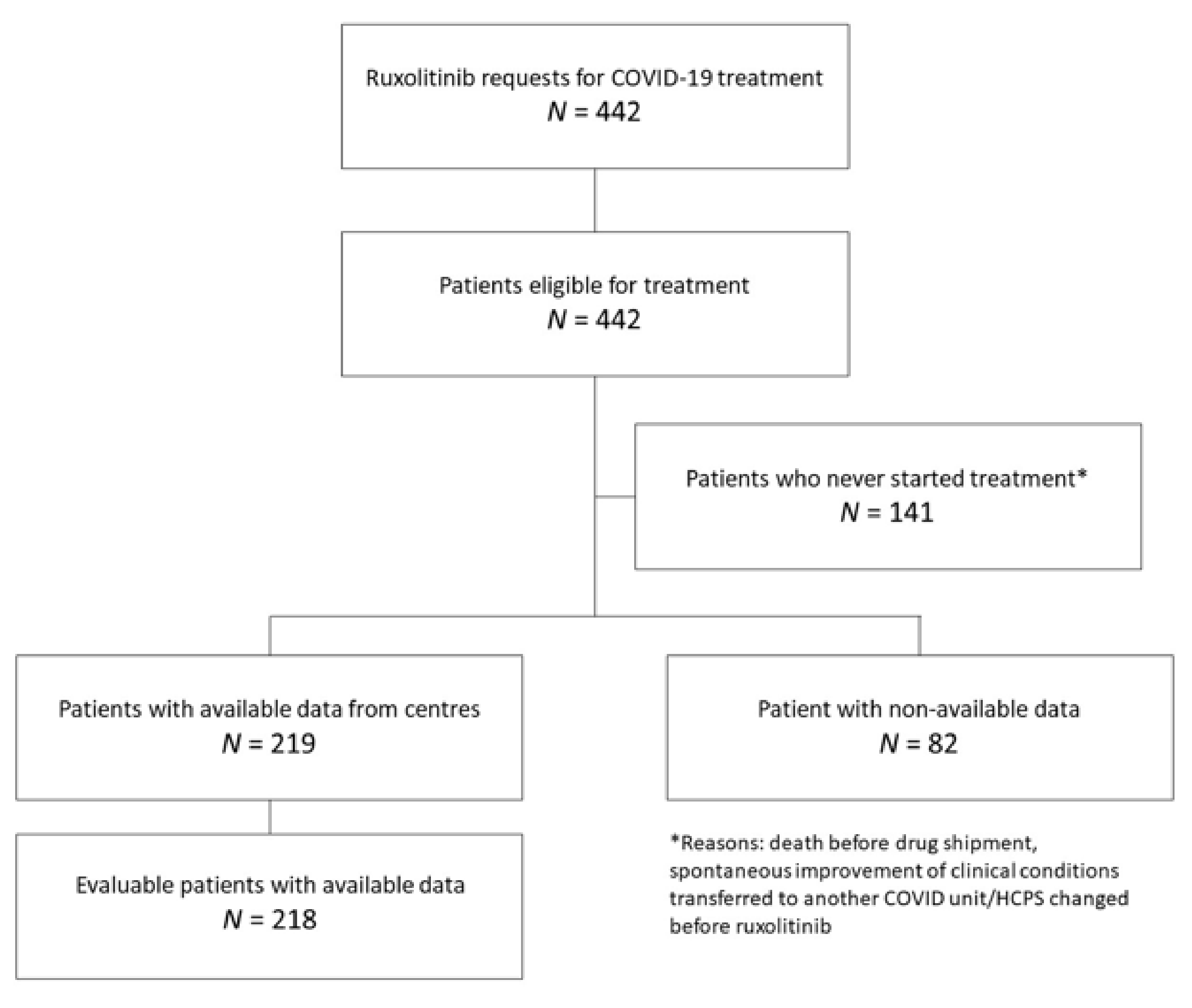
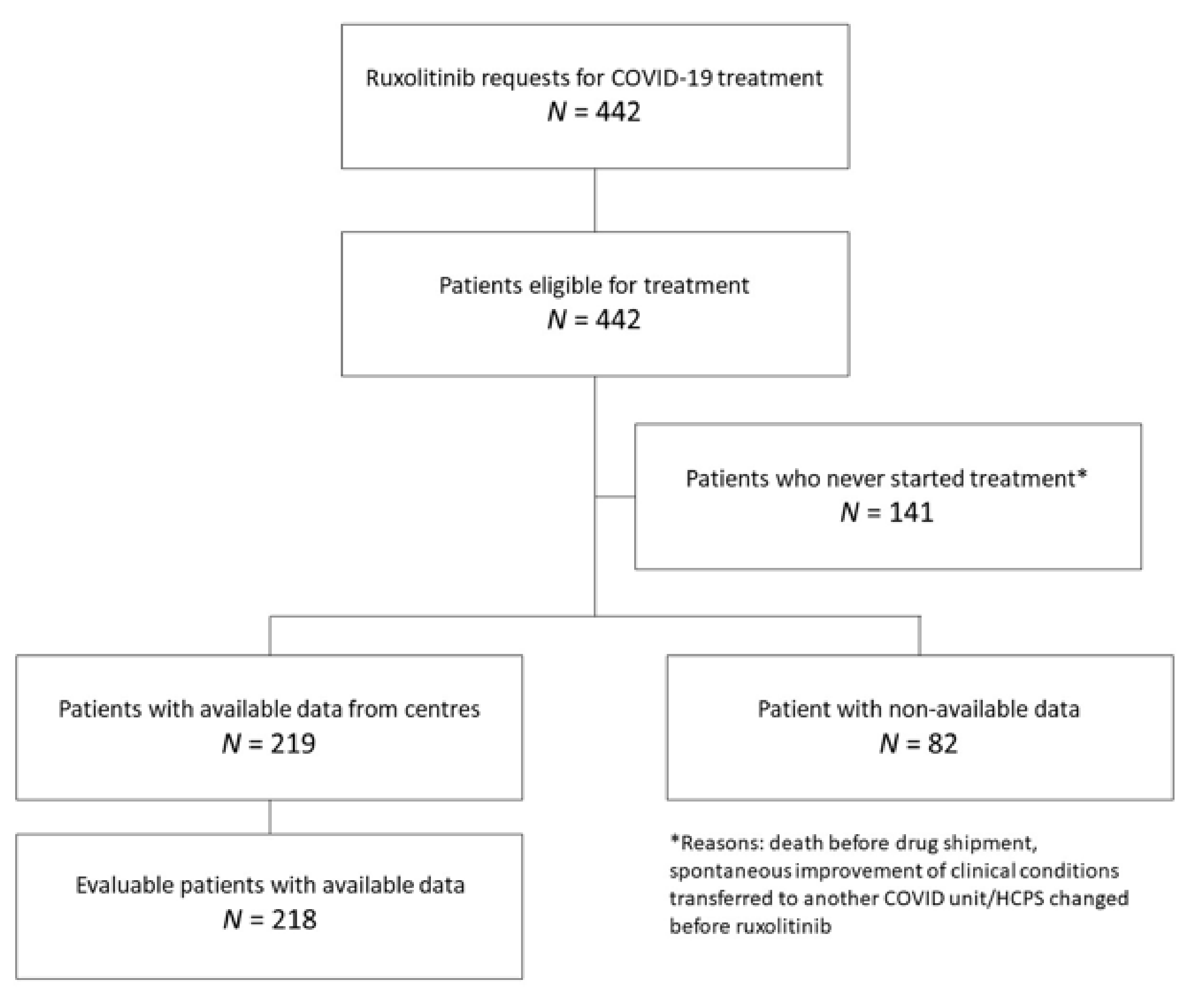
2.1. Study Design and Patients
2.2. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Clinical Status Following Treatment with Ruxolitinib
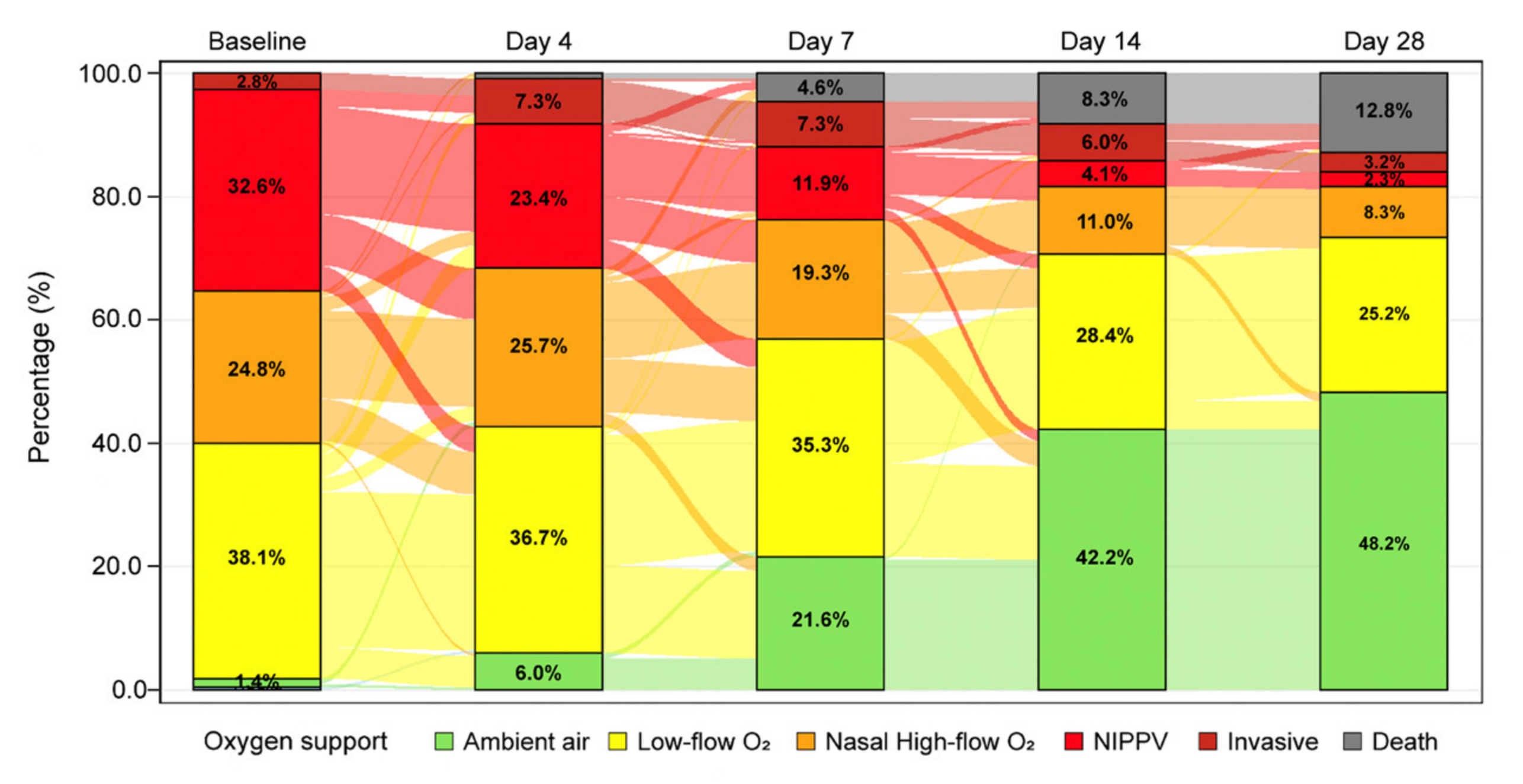
3.3. Changes in Oxygen Support
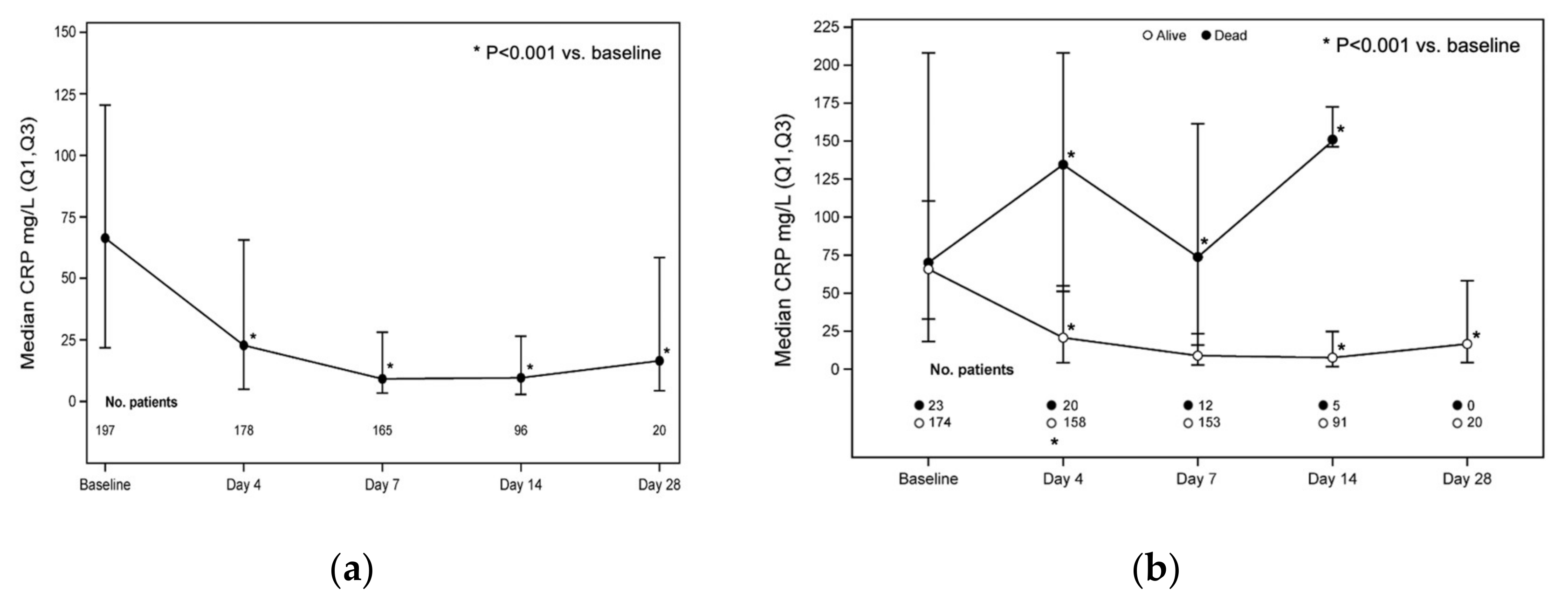
3.4. Laboratory Parameters
3.5. Mortality
3.6. Safety
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Meyerowitz, E.A.; Richterman, A.; Bogoch, I.I.; Low, N.; Cevik, M. Towards an accurate and systematic characterisation of persistently asymptomatic infection with SARS-CoV-2. Lancet Infect. Dis. 2021, 21, e163–e169. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Ruan, Q.; Yang, K.; Wang, W.; Jiang, L.; Song, J. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med. 2020, 46, 846–848. [Google Scholar] [CrossRef] [Green Version]
- Stebbing, J.; Phelan, A.; Griffin, I.; Tucker, C.; Oechsle, O.; Smith, D.; Richardson, P. COVID-19: Combining antiviral and anti-inflammatory treatments. Lancet Infect. Dis. 2020, 20, 400–402. [Google Scholar] [CrossRef]
- Liu, K.; Chen, Y.; Lin, R.; Han, K. Clinical features of COVID-19 in elderly patients: A comparison with young and middle-aged patients. J. Infect. 2020, 80, e14–e18. [Google Scholar] [CrossRef] [Green Version]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Q.; Meng, M.; Kumar, R.; Wu, Y.; Huang, J.; Deng, Y.; Weng, Z.; Yang, L. Lymphopenia is associated with severe coronavirus disease 2019 (COVID-19) infections: A systemic review and meta-analysis. Int. J. Infect. Dis. 2020, 96, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Conti, P.; Ronconi, G.; Caraffa, A.; Gallenga, C.E.; Ross, R.; Frydas, I.; Kritas, S.K. Induction of pro-inflammatory cytokines (IL-1 and IL-6) and lung inflammation by Coronavirus-19 (COVI-19 or SARS-CoV-2): Anti-inflammatory strategies. J. Biol. Regul. Homeost. Agents 2020, 34, 327–331. [Google Scholar] [CrossRef] [PubMed]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J.; HLH Across Speciality Collaboration, UK. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Seguin, A.; Galicier, L.; Boutboul, D.; Lemiale, V.; Azoulay, E. Pulmonary Involvement in Patients With Hemophagocytic Lymphohistiocytosis. Chest 2016, 149, 1294–1301. [Google Scholar] [CrossRef]
- Jamilloux, Y.; Henry, T.; Belot, A.; Viel, S.; Fauter, M.; El Jammal, T.; Walzer, T.; Francois, B.; Seve, P. Should we stimulate or suppress immune responses in COVID-19? Cytokine and anti-cytokine interventions. Autoimmun. Rev. 2020, 19, 102567. [Google Scholar] [CrossRef]
- Group, R.C.; Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; et al. Dexamethasone in Hospitalized Patients with Covid-19—Preliminary Report. N. Engl. J. Med. 2020, 384, 693–704. [Google Scholar] [CrossRef]
- Cavalli, G.; De Luca, G.; Campochiaro, C.; Della-Torre, E.; Ripa, M.; Canetti, D.; Oltolini, C.; Castiglioni, B.; Tassan Din, C.; Boffini, N.; et al. Interleukin-1 blockade with high-dose anakinra in patients with COVID-19, acute respiratory distress syndrome, and hyperinflammation: A retrospective cohort study. Lancet Rheumatol. 2020, 2, e325–e331. [Google Scholar] [CrossRef]
- Ucciferri, C.; Auricchio, A.; Di Nicola, M.; Potere, N.; Abbate, A.; Cipollone, F.; Vecchiet, J.; Falasca, K. Canakinumab in a subgroup of patients with COVID-19. Lancet Rheumatol. 2020, 2, e457–ee458. [Google Scholar] [CrossRef]
- Klopfenstein, T.; Zayet, S.; Lohse, A.; Balblanc, J.C.; Badie, J.; Royer, P.Y.; Toko, L.; Mezher, C.; Kadiane-Oussou, N.J.; Bossert, M.; et al. Tocilizumab therapy reduced intensive care unit admissions and/or mortality in COVID-19 patients. Med. Mal. Infect. 2020, 50, 397–400. [Google Scholar] [CrossRef]
- Xu, X.; Han, M.; Li, T.; Sun, W.; Wang, D.; Fu, B.; Zhou, Y.; Zheng, X.; Yang, Y.; Li, X.; et al. Effective treatment of severe COVID-19 patients with tocilizumab. Proc. Natl. Acad. Sci. USA 2020, 117, 10970–10975. [Google Scholar] [CrossRef]
- Furlow, B. COVACTA trial raises questions about tocilizumab’s benefit in COVID-19. Lancet Rheumatol. 2020, 2, e592. [Google Scholar] [CrossRef]
- Richardson, P.; Griffin, I.; Tucker, C.; Smith, D.; Oechsle, O.; Phelan, A.; Rawling, M.; Savory, E.; Stebbing, J. Baricitinib as potential treatment for 2019-nCoV acute respiratory disease. Lancet 2020, 395, e30–e31. [Google Scholar] [CrossRef] [Green Version]
- Jagasia, M.; Perales, M.A.; Schroeder, M.A.; Ali, H.; Shah, N.N.; Chen, Y.B.; Fazal, S.; Dawkins, F.W.; Arbushites, M.C.; Tian, C.; et al. Ruxolitinib for the treatment of steroid-refractory acute GVHD (REACH1): A multicenter, open-label phase 2 trial. Blood 2020, 135, 1739–1749. [Google Scholar] [CrossRef]
- Zeiser, R.; von Bubnoff, N.; Butler, J.; Mohty, M.; Niederwieser, D.; Or, R.; Szer, J.; Wagner, E.M.; Zuckerman, T.; Mahuzier, B.; et al. Ruxolitinib for Glucocorticoid-Refractory Acute Graft-versus-Host Disease. N. Engl. J. Med. 2020, 382, 1800–1810. [Google Scholar] [CrossRef] [PubMed]
- Harrison, C.; Kiladjian, J.J.; Al-Ali, H.K.; Gisslinger, H.; Waltzman, R.; Stalbovskaya, V.; McQuitty, M.; Hunter, D.S.; Levy, R.; Knoops, L.; et al. JAK inhibition with ruxolitinib versus best available therapy for myelofibrosis. N. Engl. J. Med. 2012, 366, 787–798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verstovsek, S.; Mesa, R.A.; Gotlib, J.; Levy, R.S.; Gupta, V.; DiPersio, J.F.; Catalano, J.V.; Deininger, M.; Miller, C.; Silver, R.T.; et al. A double-blind, placebo-controlled trial of ruxolitinib for myelofibrosis. N. Engl. J. Med. 2012, 366, 799–807. [Google Scholar] [CrossRef] [Green Version]
- Vannucchi, A.M.; Kiladjian, J.J.; Griesshammer, M.; Masszi, T.; Durrant, S.; Passamonti, F.; Harrison, C.N.; Pane, F.; Zachee, P.; Mesa, R.; et al. Ruxolitinib versus standard therapy for the treatment of polycythemia vera. N. Engl. J. Med. 2015, 372, 426–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magro, G. SARS-CoV-2 and COVID-19: Is interleukin-6 (IL-6) the ‘culprit lesion’ of ARDS onset? What is there besides Tocilizumab? SGP130Fc. Cytokine X 2020, 2, 100029. [Google Scholar] [CrossRef]
- Ahmed, A.; Merrill, S.A.; Alsawah, F.; Bockenstedt, P.; Campagnaro, E.; Devata, S.; Gitlin, S.D.; Kaminski, M.; Cusick, A.; Phillips, T.; et al. Ruxolitinib in adult patients with secondary haemophagocytic lymphohistiocytosis: An open-label, single-centre, pilot trial. Lancet Haematol. 2019, 6, e630–e637. [Google Scholar] [CrossRef]
- Cao, Y.; Wei, J.; Zou, L.; Jiang, T.; Wang, G.; Chen, L.; Huang, L.; Meng, F.; Huang, L.; Wang, N.; et al. Ruxolitinib in treatment of severe coronavirus disease 2019 (COVID-19): A multicenter, single-blind, randomized controlled trial. J. Allergy Clin. Immunol. 2020, 146, 137–146.e3. [Google Scholar] [CrossRef]
- Saraceni, F.; Scortechini, I.; Mancini, G.; Mariani, M.; Federici, I.; Gaetani, M.; Barbatelli, P.; Minnucci, M.L.; Bagnarelli, P.; Olivieri, A. Severe COVID-19 in a patient with chronic graft-versus-host disease after hematopoietic stem cell transplant successfully treated with ruxolitinib. Transpl. Infect. Dis. 2020, 23, e13401. [Google Scholar] [CrossRef]
- Koschmieder, S.; Jost, E.; Cornelissen, C.; Muller, T.; Schulze-Hagen, M.; Bickenbach, J.; Marx, G.; Kleines, M.; Marx, N.; Brummendorf, T.H.; et al. Favorable COVID-19 course despite significant comorbidities in a ruxolitinib-treated patient with primary myelofibrosis. Eur. J. Haematol. 2020, 105, 655–658. [Google Scholar] [CrossRef]
- Barbui, T.; Vannucchi, A.M.; Alvarez-Larran, A.; Iurlo, A.; Masciulli, A.; Carobbio, A.; Ghirardi, A.; Ferrari, A.; Rossi, G.; Elli, E.; et al. High mortality rate in COVID-19 patients with myeloproliferative neoplasms after abrupt withdrawal of ruxolitinib. Leukemia 2021, 35, 485–493. [Google Scholar] [CrossRef]
- La Rosee, F.; Bremer, H.C.; Gehrke, I.; Kehr, A.; Hochhaus, A.; Birndt, S.; Fellhauer, M.; Henkes, M.; Kumle, B.; Russo, S.G.; et al. The Janus kinase 1/2 inhibitor ruxolitinib in COVID-19 with severe systemic hyperinflammation. Leukemia 2020, 34, 1805–1815. [Google Scholar] [CrossRef]
- Innes, A.J.; Cook, L.B.; Marks, S.; Bataillard, E.; Crossette-Thambiah, C.; Sivasubramaniam, G.; Apperley, J.; Milojkovic, D. Ruxolitinib for tocilizumab-refractory severe COVID-19 infection. Br. J. Haematol 2020, 190, e198–e200. [Google Scholar] [CrossRef] [PubMed]
- Capochiani, E.; Frediani, B.; Iervasi, G.; Paolicchi, A.; Sani, S.; Roncucci, P.; Cuccaro, A.; Franchi, F.; Simonetti, F.; Carrara, D.; et al. Ruxolitinib Rapidly Reduces Acute Respiratory Distress Syndrome in COVID-19 Disease. Analysis of Data Collection From RESPIRE Protocol. Front. Med. 2020, 7, 466. [Google Scholar] [CrossRef] [PubMed]
- D’Alessio, A.; Del Poggio, P.; Bracchi, F.; Cesana, G.; Sertori, N.; Di Mauro, D.; Fargnoli, A.; Motta, M.; Giussani, C.; Moro, P.; et al. Low-dose ruxolitinib plus steroid in severe SARS-CoV-2 pneumonia. Leukemia 2021, 35, 635–638. [Google Scholar] [CrossRef] [PubMed]
- Mortara, A.; Mazzetti, S.; Margonato, D.; Delfino, P.; Bersano, C.; Catagnano, F.; Lauriola, M.; Grosso, P.; Perseghin, G.; Ippoliti, G. Compassionate use of Ruxolitinib in patients with SarsCov-2 infection not on mechanical ventilation. Short-term effects on inflammation and ventilation. Clin. Transl. Sci. 2021, 14, 1062–1068. [Google Scholar] [CrossRef]
- Vannucchi, A.M.; Sordi, B.; Morettini, A.; Nozzoli, C.; Poggesi, L.; Pieralli, F.; Bartoloni, A.; Atanasio, A.; Miselli, F.; Paoli, C.; et al. Compassionate use of JAK1/2 inhibitor ruxolitinib for severe COVID-19: A prospective observational study. Leukemia 2020, 31, 1121–1133. [Google Scholar] [CrossRef]
- Gaspari, V.; Zengarini, C.; Greco, S.; Vangeli, V.; Mastroianni, A. Side effects of ruxolitinib in patients with SARS-CoV-2 infection: Two case reports. Int. J. Antimicrob. Agents 2020, 56, 106023. [Google Scholar] [CrossRef]
- AIFA. Available online: https://www.aifa.gov.it/programmi-di-uso-compassionevole-covid-19 (accessed on 21 July 2021).
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- WHO. COVID-19 Therapeutic Trial Synopsis. Available online: https://www.who.int/publications/i/item/covid-19-therapeutic-trial-synopsis (accessed on 22 September 2020).
- Signorelli, C.; Odone, A. Age-specific COVID-19 case-fatality rate: No evidence of changes over time. Int. J. Public Health 2020, 65, 1435–1436. [Google Scholar] [CrossRef]
- Zitek, T. The Appropriate Use of Testing for COVID-19. West. J. Emerg. Med. 2020, 21, 470–472. [Google Scholar] [CrossRef] [Green Version]
- Novartis. Press Release. Available online: https://www.novartis.com/news/media-releases/novartis-provides-update-ruxcovid-study-ruxolitinib-hospitalized-patients-covid-19 (accessed on 13 January 2021).




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | No. Patients | Main Endpoint | Outcome(s) |
|---|---|---|---|
| Capochiani et al. [32] | 18 | Reduction in respiratory impairment |
|
| D’Alessio et al. [33] | 32 (ruxolitinib) 43 (other *) | Clinical recovery without mechanical ventilation, admission to ICU for mechanical ventilation and death |
|
| Mortara et al. [34] | 31 | C-reactive protein (CRP) and PaO2/FiO2 ratio. |
|
| Vannucchi et al. [35] | 34 | – |
|
| Characteristic | Total (N = 218) |
|---|---|
| Age in years, median (Q1, Q3) | 70.5 (59–80) |
| Age categories, N (%) | |
| ≤50 years | 17 (7.8) |
| 50 to <70 years | 86 (39.5) |
| ≥70 years | 115 (52.8) |
| Sex, N (%) | |
| Female | 84 (38.5) |
| Male | 134 (61.5) |
| Comorbidities, N (%) * | |
| Any comorbidity | 153 (70.2) |
| No comorbidity/unknown | 65 (29.8) |
| 1 comorbidity | 50 (22.9) |
| 2 comorbidities | 39 (17.9) |
| >2 comorbidities | 64 (29.4) |
| Virology test for COVID-19, N (%) | |
| Negative § | 10 (4.6) |
| Positive | 208 (95.4) |
| Oxygen support, N (%) | |
| Ambient air | 3 (1.4) |
| Low-flow O2 | 83 (38.1) |
| Nasal high-flow O2 | 54 (24.8) |
| NIPPV | 71 (32.6) |
| Invasive | 6 (2.8) |
| Missing | 1 (0.5) |
| Ruxolitinib starting dosage, N (%) | |
| 5 mg BID | 192 (88.1) |
| Other dosage ** | 26 (11.9) |
| Concomitant treatment for SARS-CoV-2, N (%) | 206 (94.5) |
| Chloroquine/hydroxychloroquine | 155 (71.1) |
| Antivirals | 72 (33.0) |
| Glucocorticoids | 110 (50.5) |
| Antithrombotic agents *** | 53 (24.3) |
| Clinical Status at Most Recent Follow-Up *, n (%) | Oxygen Support at Baseline | |||||
|---|---|---|---|---|---|---|
| Ambient air (N = 3) | Low-flow O2 (N = 83) | Nasal high-flow O2 (N = 54) | NIPPV (N = 71) | Invasive (N = 6) | Total (N = 218) | |
| Died | 0 | 7 (8.4) | 7 (13.0) | 9 (12.7) | 5 (83.3) | 28 (12.8) |
| Worsened | 1 (33.3) | 1 (1.2) | 1 (1.9) | 3 (4.2) | 0 | 6 (2.8) |
| Stable | 1 (33.3) | 24 (28.9) | 8 (14.8) | 6 (8.5) | 0 | 39 (17.9) |
| Improved | 1 (33.3) | 51 (61.5) | 38 (70.4) | 53 (74.7) | 1 (16.7) | 145 (66.5) |
| Time to reach improvement § | ||||||
| Improved by Day 4 | 0 | 33 (64.7) | 20 (52.6) | 35 (66.0) | 1 (100.0) | 90 (62.1) |
| Improved by Day 7 | 1 (100.0) | 8 (15.7) | 11 (29.0) | 11 (20.8) | 0 | 31 (21.4) |
| Improved by Day 14 | 0 | 10 (19.6) | 6 (15.8) | 5 (9.4) | 0 | 21 (14.5) |
| Improved by Day 28 | 0 | 0 | 1 (2.6) | 2 (3.8) | 0 | 3 (2.1) |
| Total (N = 219) | ||
|---|---|---|
| All Grades | Grade 3/4 | |
| Total number of adverse events | 496 | 16 |
| Patients with any adverse event, N (%) | 203 (92.7) | 15 (6.9) |
| Patients with more than 1 adverse events, N (%) | 157 (71.7) | 1 (0.5) |
| Patients with hematologic adverse events, N (%): | ||
| Anemia | 153 (69.9) | 2 (0.9) |
| Thrombocytopenia | 35 (16.0) | 5 (2.3) |
| Thrombocytosis | 52 (23.7) | 0 |
| Leukopenia | 34 (15.4) | 2 (0.9) |
| Patients with non-hematologic adverse events, N (%): | ||
| Alanine aminotransferase increase | 103 (47.0) | 2 (0.9) |
| Aspartate aminotransferase increase | 64 (29.2) | 1 (0.5) |
| Creatinine increase | 44 (20.1) | 0 |
| Infections * | 4 (1.8) | 3 (1.4) |
| Other ** | 2 (0.9) | 1 (0.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vannucchi, A.M.; Mortara, A.; D’Alessio, A.; Morelli, M.; Tedeschi, A.; Festuccia, M.B.; Monforte, A.D.; Capochiani, E.; Selleri, C.; Simonetti, F.; et al. JAK Inhibition with Ruxolitinib in Patients with COVID-19 and Severe Pneumonia: Multicenter Clinical Experience from a Compassionate Use Program in Italy. J. Clin. Med. 2021, 10, 3752. https://doi.org/10.3390/jcm10163752
Vannucchi AM, Mortara A, D’Alessio A, Morelli M, Tedeschi A, Festuccia MB, Monforte AD, Capochiani E, Selleri C, Simonetti F, et al. JAK Inhibition with Ruxolitinib in Patients with COVID-19 and Severe Pneumonia: Multicenter Clinical Experience from a Compassionate Use Program in Italy. Journal of Clinical Medicine. 2021; 10(16):3752. https://doi.org/10.3390/jcm10163752
Chicago/Turabian StyleVannucchi, Alessandro Maria, Andrea Mortara, Andrea D’Alessio, Mara Morelli, Alberto Tedeschi, Moreno Benedetto Festuccia, Antonella D’Arminio Monforte, Enrico Capochiani, Carmine Selleri, Federico Simonetti, and et al. 2021. "JAK Inhibition with Ruxolitinib in Patients with COVID-19 and Severe Pneumonia: Multicenter Clinical Experience from a Compassionate Use Program in Italy" Journal of Clinical Medicine 10, no. 16: 3752. https://doi.org/10.3390/jcm10163752
APA StyleVannucchi, A. M., Mortara, A., D’Alessio, A., Morelli, M., Tedeschi, A., Festuccia, M. B., Monforte, A. D., Capochiani, E., Selleri, C., Simonetti, F., Saracino, A., Rapezzi, D., Badagliacca, M. R., Falasca, K., Molteni, A., Palazzolo, R., Schettino, G., Bocchia, M., Turrini, M., ... Saglio, G. (2021). JAK Inhibition with Ruxolitinib in Patients with COVID-19 and Severe Pneumonia: Multicenter Clinical Experience from a Compassionate Use Program in Italy. Journal of Clinical Medicine, 10(16), 3752. https://doi.org/10.3390/jcm10163752