A Pharyngoplasty with a Dorsal Palatal Flap Expansion: The Evaluation of a Modified Surgical Treatment Method for Obstructive Sleep Apnea Syndrome—A Preliminary Report

 , , and
, , and
Abstract
:1. Introduction
1.1. Importance of OSAS
1.2. Management Options
1.3. Aim of This Study
2. Materials and Methods
2.1. Ethical Approval and Informed Consent
2.2. Study Design
2.2.1. Study Protocol
2.2.2. Sleep Study
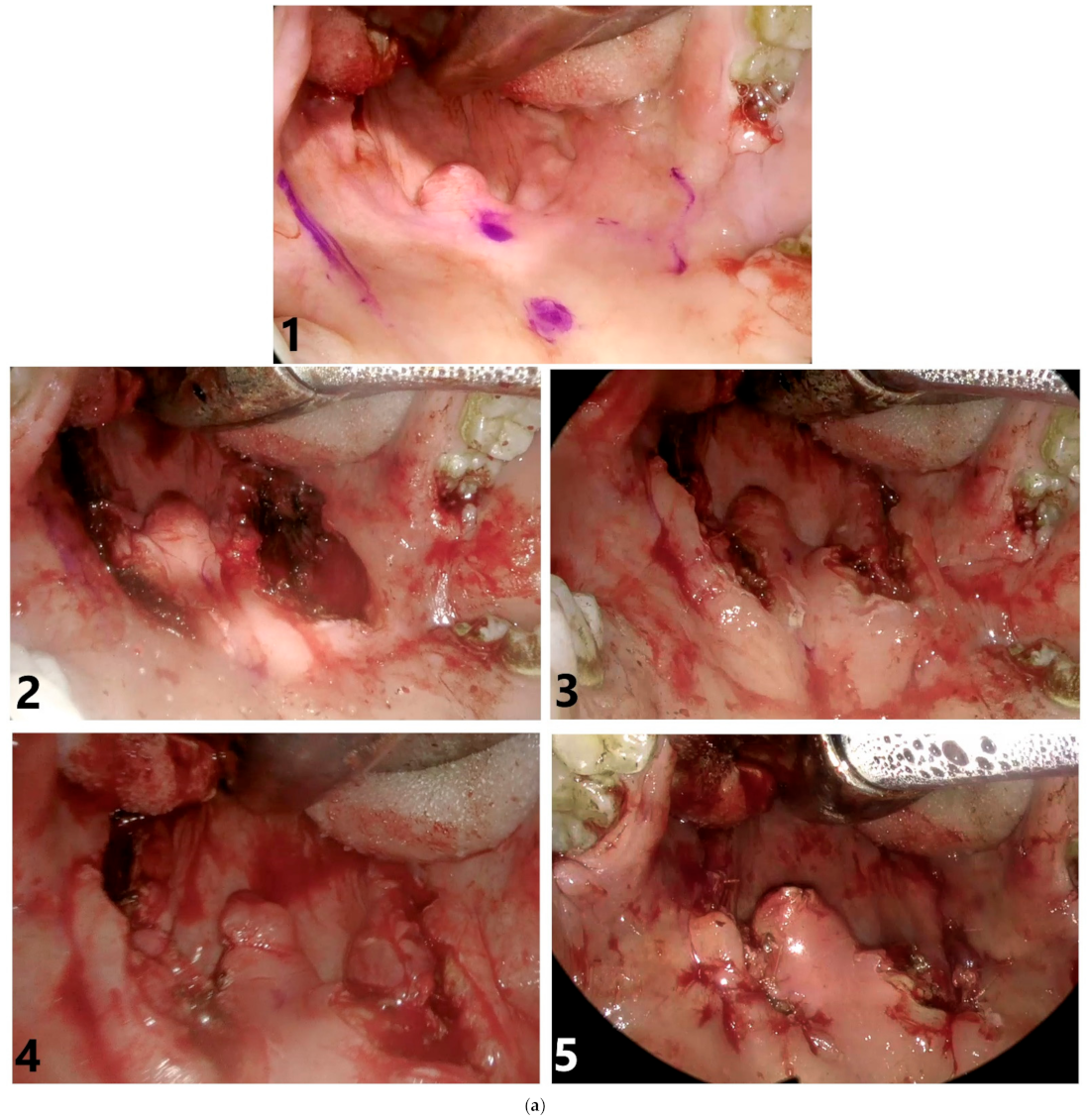
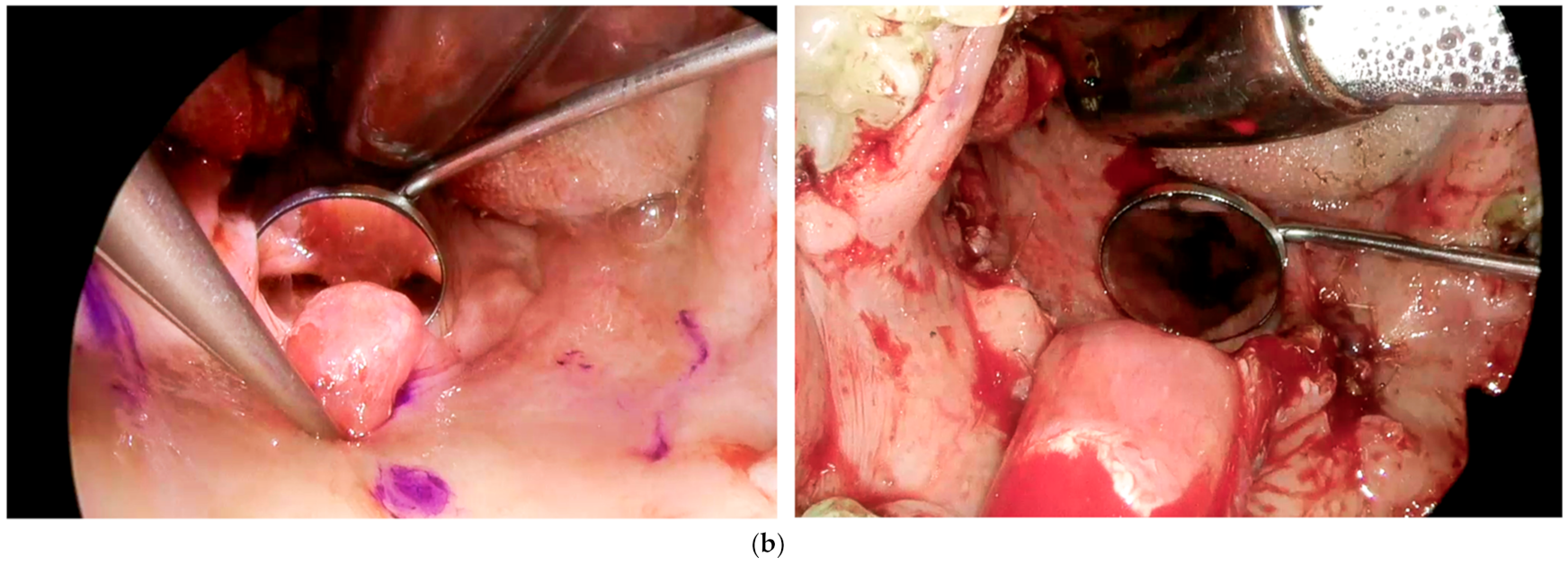
2.3. Description of the Surgical Procedure
2.4. Study Assessments
2.5. Post-Operative Patient Care
2.6. Study Outcomes
2.7. Statistical Analysis
3. Results
3.1. Study Group
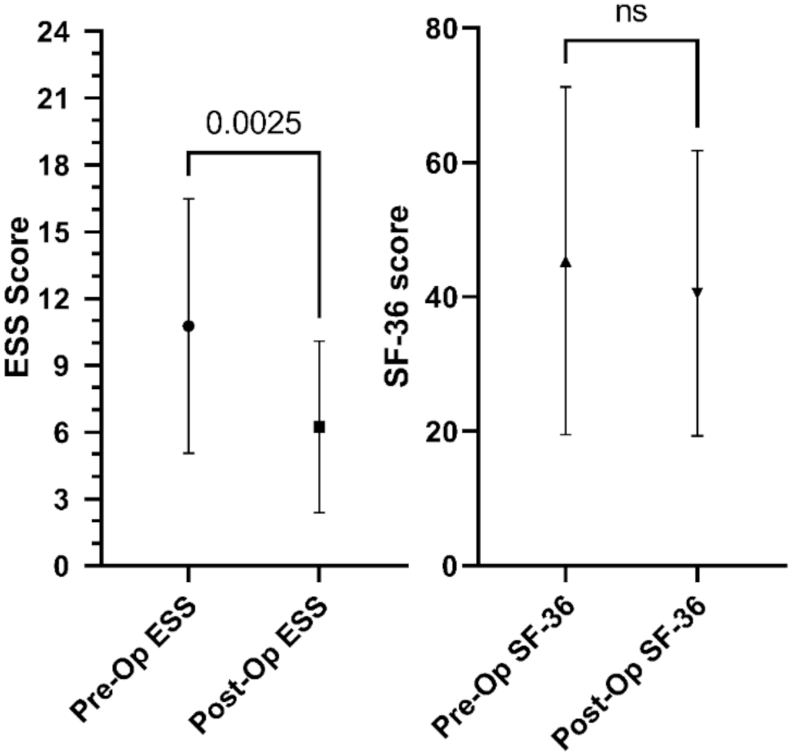
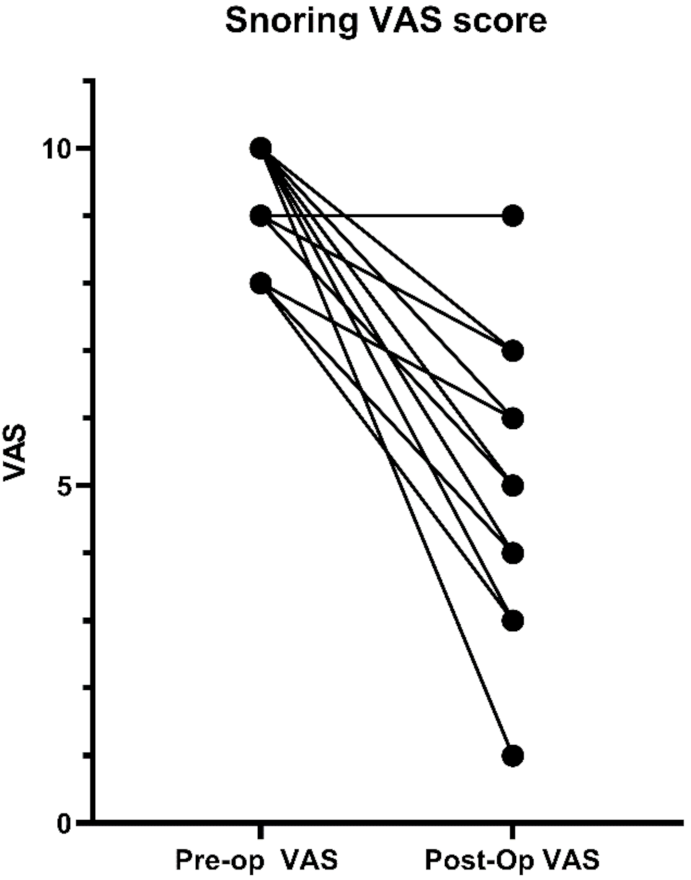
3.2. Study Outcomes
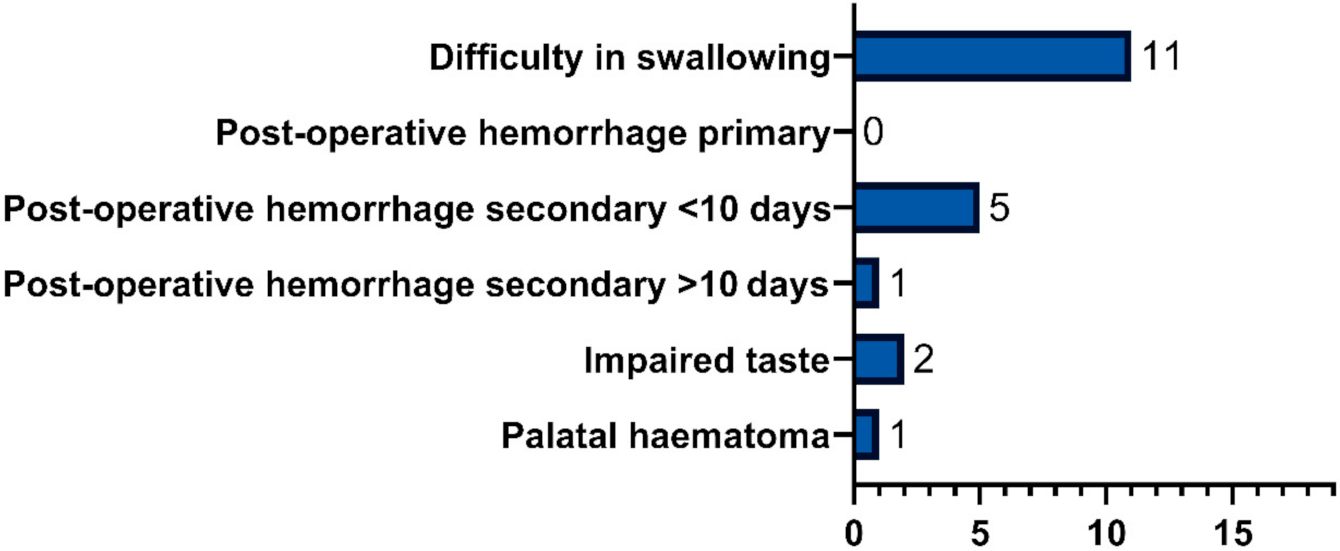
3.3. Post-Operative Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Morsy, N.E.; Farrag, N.S.; Zaki, N.F.W.; Badawy, A.Y.; Abdelhafez, S.A.; El-Gilany, A.-H.; El Shafey, M.M.; Pandi-Perumal, S.R.; Spence, D.W.; BaHammam, A.S. Obstructive sleep apnea: Personal, societal, public health, and legal implications. Rev. Environ. Health 2019, 34, 153–169. [Google Scholar] [CrossRef]
- Senaratna, C.V.; Perret, J.L.; Lodge, C.J.; Lowe, A.J.; Campbell, B.E.; Matheson, M.C.; Hamilton, G.S.; Dharmage, S.C. Prevalence of obstructive sleep apnea in the general population: A systematic review. Sleep Med. Rev. 2017, 34, 70–81. [Google Scholar] [CrossRef]
- Kapur, V.K.; Auckley, D.H.; Chowdhuri, S.; Kuhlmann, D.C.; Mehra, R.; Ramar, K.; Harrod, C.G. Clinical Practice Guideline for Diagnostic Testing for Adult Obstructive Sleep Apnea: An American Academy of Sleep Medicine Clinical Practice Guideline. J. Clin. Sleep Med. 2017, 13, 479–504. [Google Scholar] [CrossRef]
- Pang, K.P.; Baptista, P.M.J.; Olszewska, E.; Braverman, I.; Carrasco-Llatas, M.; Kishore, S.; Chandra, S.; Yang, H.C.; Chan, Y.H.; Pang, K.A.; et al. SLEEP-GOAL: A multicenter success criteria outcome study on 302 obstructive sleep apnoea (OSA) patients. Med. J. Malaysia 2020, 75, 117–123. [Google Scholar] [PubMed]
- Redline, S.; Yenokyan, G.; Gottlieb, D.J.; Shahar, E.; O’Connor, G.T.; Resnick, H.E.; Diener-West, M.; Sanders, M.H.; Wolf, P.A.; Geraghty, E.M.; et al. Obstructive sleep apnea–hypopnea and incident stroke: The sleep heart health study. Am. J. Respir. Crit. Care Med. 2010, 182, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Olszewska, E.; Panek, J.; O’Day, J.; Rogowski, M. Usefulness of snoreplasty in the treatment of simple snoring and mild obstructive sleep apnea/hypopnea syndrome—Preliminary report. Otolaryngol. Polska 2014, 68, 184–188. [Google Scholar] [CrossRef] [PubMed]
- Benjafield, A.V.; Ayas, N.T.; Eastwood, P.R.; Heinzer, R.; Ip, M.S.M.; Morrell, M.J.; Nunez, C.M.; Patel, S.R.; Penzel, T.; Pépin, J.-L.D.; et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: A literature-based analysis. Lancet Respir. Med. 2019, 7, 687–698. [Google Scholar] [CrossRef] [Green Version]
- Young, T.; Peppard, P.E.; Taheri, S. Excess weight and sleep-disordered breathing. J. Appl. Physiol. 2005, 99, 1592–1599. [Google Scholar] [CrossRef] [PubMed]
- Peppard, P.E.; Young, T.; Palta, M.; Dempsey, J.; Skatrud, J. Longitudinal study of moderate weight change and sleep-disordered breathing. JAMA 2000, 284, 3015–3021. [Google Scholar] [CrossRef] [Green Version]
- MacKay, S.; Carney, A.S.; Catcheside, P.G.; Chai-Coetzer, C.L.; Chia, M.; Cistulli, P.A.; Hodge, J.-C.; Jones, A.; Kaambwa, B.; Lewis, R.; et al. Effect of multilevel upper airway surgery vs medical management on the apnea-hypopnea index and patient-reported daytime sleepiness among patients with moderate or severe obstructive sleep apnea. The SAMS randomized clinical trial. JAMA 2020, 324, 1168–1179. [Google Scholar] [CrossRef]
- Friedman, M.; Ibrahim, H.; Bass, L. Clinical staging for sleep-disordered breathing. Otolaryngol. Head Neck Surg. 2002, 127, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Tingting, X.; Danming, Y.; Xin, C. Non-surgical treatment of obstructive sleep apnea syndrome. Eur. Arch. Oto Rhino Laryngol. 2018, 275, 335–346. [Google Scholar] [CrossRef] [PubMed]
- Olszewska, E.; Woodson, B.T. Palatal anatomy for sleep apnea surgery. Laryngoscope Investig. Otolaryngol. 2019, 4, 181–187. [Google Scholar] [CrossRef] [Green Version]
- Puccia, R.; Woodson, B.T. Palatopharyngoplasty and Palatal Anatomy and Phenotypes for Treatment of Sleep Apnea in the Twenty-first Century. Otolaryngol. Clin. N. Am. 2020, 53, 421–429. [Google Scholar] [CrossRef] [PubMed]
- Johns, M.W. A New Method for measuring daytime sleepiness: The epworth sleepiness scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johns, M.W. Reliability and factor analysis of the epworth sleepiness scale. Sleep 1992, 15, 376–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pevernagie, D.A.; Gnidovec-Strazisar, B.; Grote, L.; Heinzer, R.; McNicholas, W.T.; Penzel, T.; Randerath, W.; Schiza, S.; Verbraecken, J.; Arnardottir, E.S. On the rise and fall of the apnea-hypopnea index: A historical review and critical appraisal. J. Sleep Res. 2020, 29. [Google Scholar] [CrossRef] [PubMed]
- Pang, K.P.; Woodson, B.T. Expansion sphincter pharyngoplasty: A new technique for the treatment of obstructive sleep apnea. Otolaryngol. Head Neck Surg. 2007, 137, 110–114. [Google Scholar] [CrossRef] [PubMed]
- Basheer, H.; Sharma, S.; Patel, M. Can we use the oxygen desaturation index alone to reliably diagnose obstructive sleep apnoea in obese patients? Eur. Respir. J. 2016, 48. [Google Scholar] [CrossRef]
- Mackay, S.G.; Carney, A.S.; Woods, C.P.D.; Antic, N.P.D.; McEvoy, R.D.; Chia, M.; Sands, T.; Jones, A.; Hobson, J.; Robinson, S. Modified Uvulopalatopharyngoplasty and Coblation Channeling of the Tongue for Obstructive Sleep Apnea: A Multi-Centre Australian Trial. J. Clin. Sleep Med. 2013, 9, 117–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plaza, G.; Baptista, P.; O’Connor-Reina, C.; Bosco, G.; Pérez-Martín, N.; Pang, K.P. Prospective multi-center study on expansion sphincter pharyngoplasty. Acta Otolaryngol. 2019, 139, 219–222. [Google Scholar] [CrossRef]
- El-Ahl, M.A.S.; El-Anwar, M.W. Expansion Pharyngoplasty by New Simple Suspension Sutures without Tonsillectomy. Otolaryngol. Head Neck Surg. 2016, 155, 1065–1068. [Google Scholar] [CrossRef]
- Pang, K.P.; Plaza, G.; Baptista, P.M.; O’Connor-Reina, C.; Chan, Y.H.; Pang, K.A.; Pang, E.B.; Wang, C.M.Z.; Rotenberg, B. Palate surgery for obstructive sleep apnea: A 17-year meta-analysis. Eur. Arch. Oto Rhino Laryngol. 2018, 275, 1697–1707. [Google Scholar] [CrossRef]
- Despeghel, A.-S.; Mus, L.; Dick, C.; Vlaminck, S.; Kuhweide, R.; Lerut, B.; Speleman, K.; Vinck, A.-S.; Vauterin, T. Long-term results of a modified expansion sphincter pharyngoplasty for sleep-disordered breathing. Eur. Arch. Oto Rhino Laryngol. 2017, 274, 1665–1670. [Google Scholar] [CrossRef]
- Nilius, G.; Domanski, U.; Schroeder, M.; Franke, K.-J.; Hogrebe, A.; Margarit, L.; Stoica, M.; D’Ortho, M.-P. A randomized controlled trial to validate the Alice PDX ambulatory device. Nat. Sci. Sleep 2017, 9, 171–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chesson, A.L.; Berry, R.B.; Pack, A. Practice parameters for the use of portable monitoring devices in the investigation of suspected obstructive sleep apnea in adults. Sleep 2003, 26, 907–913. [Google Scholar] [CrossRef] [Green Version]
- Bibbins-Domingo, K.; Grossman, D.C.; Curry, S.J.; Davidson, K.W.; Epling, J.W.; Garcia, F.A.R.; Herzstein, J.; Kemper, A.R.; Krist, A.H.; Kurth, A.E.; et al. Screening for obstructive sleep apnea in adults. US preventive services task force recommendation statement. JAMA 2017, 317, 407–414. [Google Scholar] [CrossRef]
- Browaldh, N.; Nerfeldt, P.; Lysdahl, M.; Bring, J.; Friberg, D. SKUP3randomised controlled trial: Polysomnographic results after uvulopalatopharyngoplasty in selected patients with obstructive sleep apnoea. Thorax 2013, 68, 846–853. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sundman, J.; Friberg, D.; Bring, J.; Lowden, A.; Nagai, R.; Browaldh, N. Sleep Quality after Modified Uvulopalatopharyngoplasty: Results from the SKUP3 Randomized Controlled Trial. Sleep 2018, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Mean (SD)/n% | Min | Max |
|---|---|---|---|
| Biometrics | |||
| Age (y) | 49.9 (12.2) | 26 | 72 |
| Weight (kg) | 101.9 (10.2) | 85 | 120 |
| Body Mass Index (kg/m2) | 32.5 (3.4) | 26.3 | 39.7 |
| BMI group I * | 6–28.6% | ||
| BMI group II * | 10–47.6% | ||
| BMI group III * | 5–23.8% | ||
| Mean Blood Pressure (mmHg) | 105.4 (8.4) | 90.7 | 121.3 |
| Comorbidities | 15–71.4% | ||
| Hypertension | 15–71.4% | ||
| Diabetes Mellitus Type 2 | 4–19% | ||
| Heart Disease | 2–9.5% | ||
| Anatomy and OSAS | |||
| Friedman Tongue Position | 2 | 4 | |
| Friedman Tongue Position 2 | 3–14.3% | ||
| Friedman Tongue Position 3 | 16–76.2% | ||
| Friedman Tongue Position 4 | 2–9.5% | ||
| Friedman Palatine Tonsils Scale | 1 | 3 | |
| Friedman Palatine Tonsils Scale 1 | 9–42.9% | ||
| Friedman Palatine Tonsils Scale 2 | 7–33.3% | ||
| Friedman Palatine Tonsils Scale 3 | 5–23.8% | ||
| Epworth Sleepiness Scale | 10.8 (5.7) | 1 | 22 |
| Apnea–Hypopnea Index | 45.2 (15.9) | 15.2 | 71.6 |
| Moderate OSAS (15 ≤ AHI ˂ 30) | 4–19% | ||
| Severe OSAS (AHI > 30) | 17–81% | ||
| Snoring Visual Analog Scale | 9.4 (0.9) | 8 | 10 |
| Median Pre (IQR) | Median Post (IQR) | Significance | Effect Size r | |
|---|---|---|---|---|
| Biometric Characteristics | ||||
| Weight | 100.0 (92–111.5) | 100.0 (93.5–109) | 0.275 | 0.168 |
| BMI | 32.6 (29.7–34.8) | 32.3 (30.1–34.1) | 0.278 | 0.167 |
| MAP | 103.7 (98–111.4) | 101.7 (93–109.7) | 0.251 | 0.177 |
| Questionnaires | ||||
| Snoring VAS | 10 (8.5–10) | 5 (4–6) | <0.0001 | 0.738 |
| ESS | 9.0 (7–17) | 7.0 (2.5–9.5) | 0.0025 | 0.442 |
| SF-36 | 41.0 (27.5–58) | 35.0 (19–53.3) | 0.715 | 0.056 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olszewska, E.; Fiedorczuk, P.; Stróżyński, A.; Polecka, A.; Roszkowska, E.; Woodson, B.T. A Pharyngoplasty with a Dorsal Palatal Flap Expansion: The Evaluation of a Modified Surgical Treatment Method for Obstructive Sleep Apnea Syndrome—A Preliminary Report. J. Clin. Med. 2021, 10, 3746. https://doi.org/10.3390/jcm10163746
Olszewska E, Fiedorczuk P, Stróżyński A, Polecka A, Roszkowska E, Woodson BT. A Pharyngoplasty with a Dorsal Palatal Flap Expansion: The Evaluation of a Modified Surgical Treatment Method for Obstructive Sleep Apnea Syndrome—A Preliminary Report. Journal of Clinical Medicine. 2021; 10(16):3746. https://doi.org/10.3390/jcm10163746
Chicago/Turabian StyleOlszewska, Ewa, Piotr Fiedorczuk, Adam Stróżyński, Agnieszka Polecka, Ewa Roszkowska, and B. Tucker Woodson. 2021. "A Pharyngoplasty with a Dorsal Palatal Flap Expansion: The Evaluation of a Modified Surgical Treatment Method for Obstructive Sleep Apnea Syndrome—A Preliminary Report" Journal of Clinical Medicine 10, no. 16: 3746. https://doi.org/10.3390/jcm10163746
APA StyleOlszewska, E., Fiedorczuk, P., Stróżyński, A., Polecka, A., Roszkowska, E., & Woodson, B. T. (2021). A Pharyngoplasty with a Dorsal Palatal Flap Expansion: The Evaluation of a Modified Surgical Treatment Method for Obstructive Sleep Apnea Syndrome—A Preliminary Report. Journal of Clinical Medicine, 10(16), 3746. https://doi.org/10.3390/jcm10163746