
Efficacy of Statin Treatment According to Baseline Renal Function in Korean Patients with Acute Myocardial Infarction Not Requiring Dialysis Undergoing Newer-Generation Drug-Eluting Stent Implantation

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Method
2.1. Study Population
2.2. Percutaneous Coronary Intervention (PCI) Procedure and Medical Treatment
2.3. Study Definitions and Clinical Outcomes
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.1.1. Group A (Statin Users)
3.1.2. Group B (Statin Nonusers)
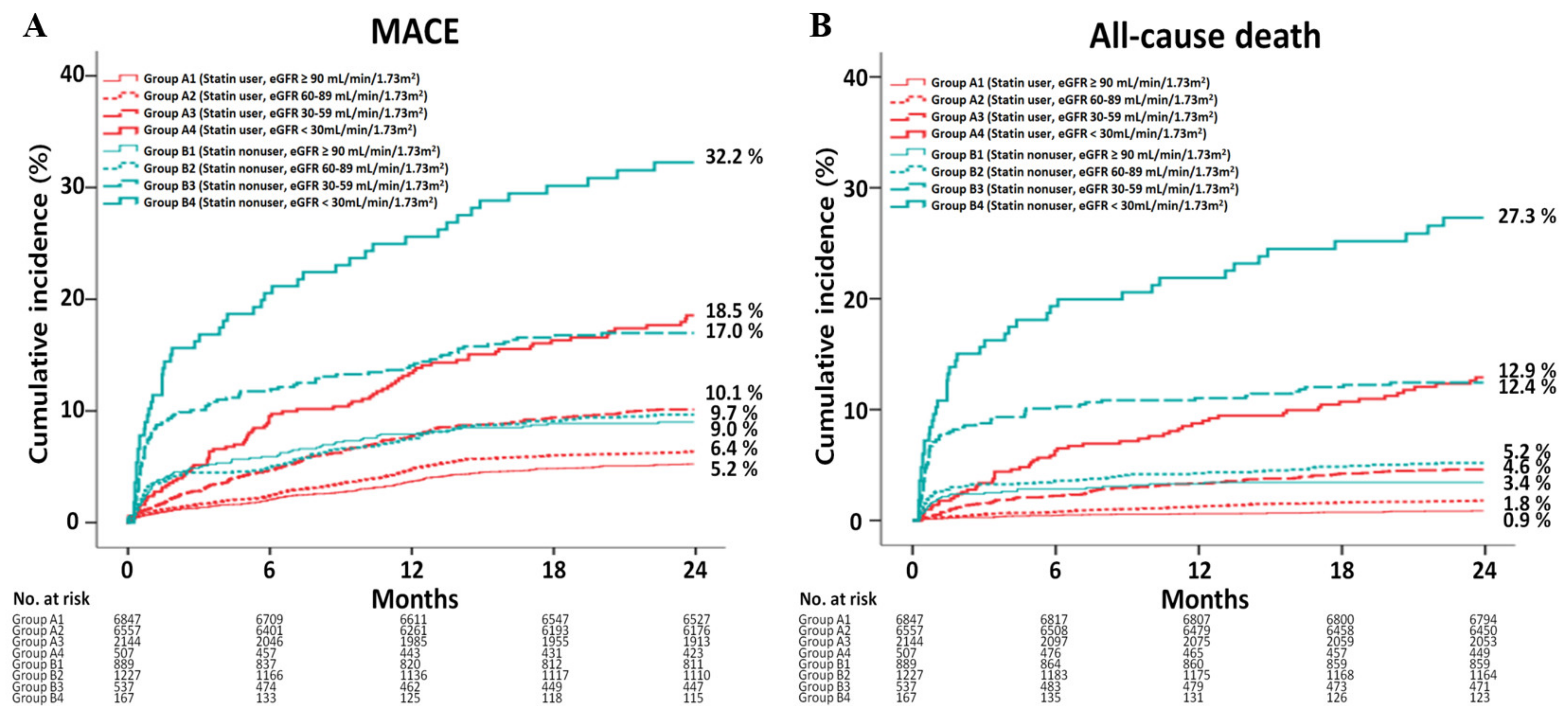
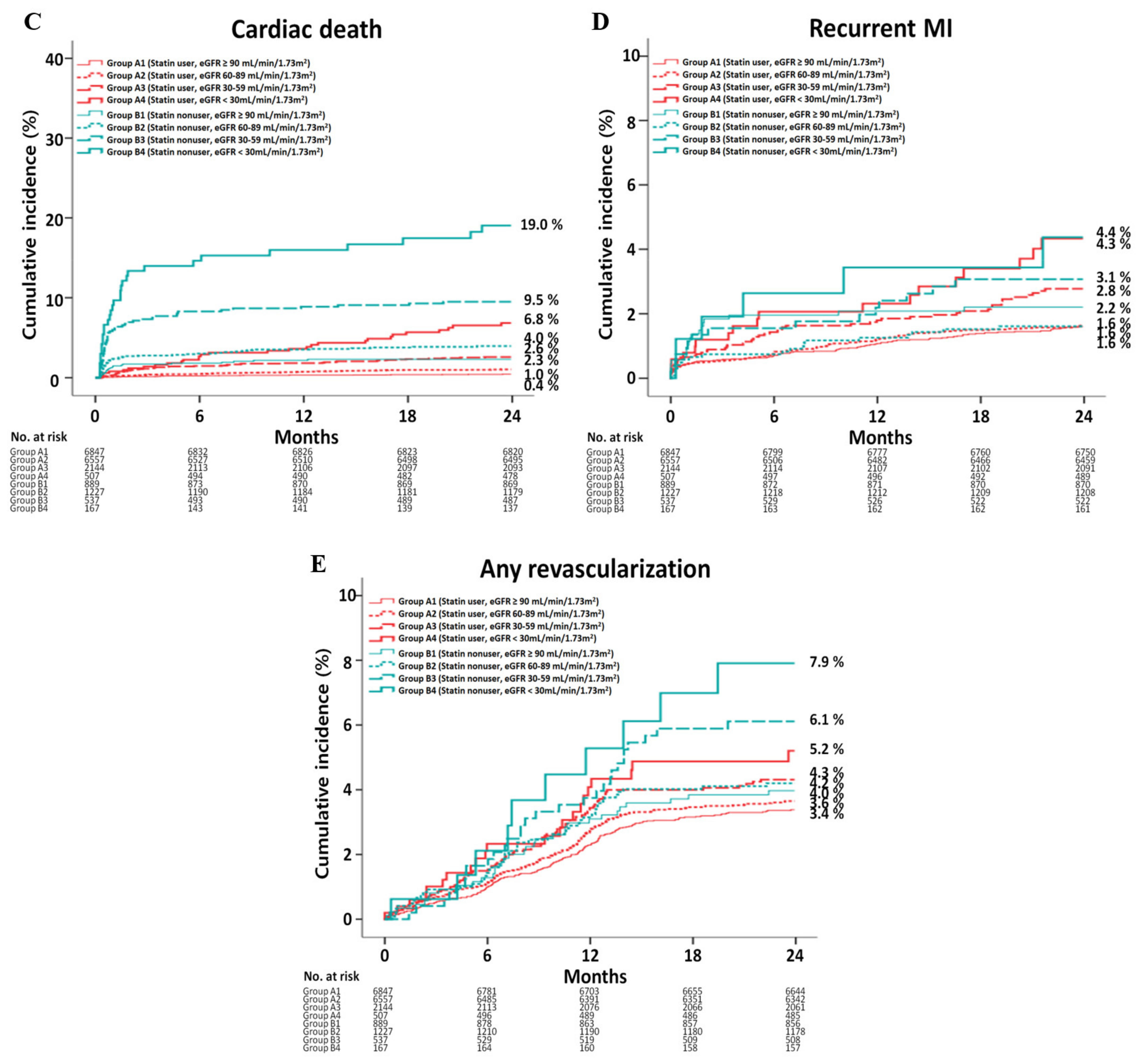
3.2. Clinical Outcomes
3.2.1. Group A
3.2.2. Group B
3.2.3. Group A vs. B
3.2.4. Independent Predictors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Szummer, K.; Wallentin, L.; Lindhagen, L.; Alfredsson, J.; Erlinge, D.; Held, C.; James, S.; Kellerth, T.; Lindahl, B.; Ravn-Fischer, A.; et al. Relations between implementation of new treatments and improved outcomes in patients with non-ST-elevation myocardial infarction during the last 20 years: Experiences from SWEDEHEART registry 1995 to 2014. Eur. Heart J. 2018, 39, 3766–3776. [Google Scholar] [CrossRef]
- Puymirat, E.; Simon, T.; Cayla, G.; Cottin, Y.; Elbaz, M.; Coste, P.; Lemesle, G.; Motreff, P.; Popovic, B.; Khalife, K.; et al. Acute Myocardial Infarction: Changes in Patient Characteristics, Management, and 6-Month Outcomes Over a Period of 20 Years in the FAST-MI Program (French Registry of Acute ST-Elevation or Non-ST-Elevation Myocardial Infarction) 1995 to 2015. Circulation 2017, 136, 1908–1919. [Google Scholar] [CrossRef] [PubMed]
- Townsend, N.; Wilson, L.; Bhatnagar, P.; Wickramasinghe, K.; Rayner, M.; Nichols, M. Cardiovascular disease in Europe: Epidemiological update 2016. Eur. Heart J. 2016, 37, 3232–3245. [Google Scholar] [CrossRef]
- Kim, Y.; Ahn, Y.; Cho, M.C.; Kim, C.J.; Kim, Y.J.; Jeong, M.H. Current status of acute myocardial infarction in Korea. Korean J. Intern. Med. 2019, 34, 1–10. [Google Scholar] [CrossRef]
- Larsen, A.I.; Tomey, M.I.; Mehran, R.; Nilsen, D.W.; Kirtane, A.J.; Witzenbichler, B.; Guagliumi, G.; Brener, S.J.; Généreux, P.; Kornowski, R.; et al. Comparison of outcomes in patients with ST-segment elevation myocardial infarction discharged on versus not on statin therapy (from the Harmonizing Outcomes with Revascularization and Stents in Acute Myocardial Infarction Trial). Am. J. Cardiol. 2014, 113, 1273–1279. [Google Scholar] [CrossRef]
- Baigent, C.; Keech, A.; Kearney, P.M.; Blackwell, L.; Buck, G.; Pollicino, C.; Kirby, A.; Sourjina, T.; Peto, R.; Collins, R.; et al. Efficacy and safety of cholesterol-lowering treatment: Prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet 2005, 366, 1267–1278. [Google Scholar]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar]
- Roffi, M.; Patrono, C.; Collet, J.P.; Mueller, C.; Valgimigli, M.; Andreotti, F.; Bax, J.J.; Borger, M.A.; Brotons, C.; Chew, D.P.; et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2016, 37, 267–315. [Google Scholar] [PubMed]
- Mafham, M.; Emberson, J.; Landray, M.J.; Wen, C.P.; Baigent, C. Estimated glomerular filtration rate and the risk of major vascular events and all-cause mortality: A meta-analysis. PLoS ONE 2011, 6, e25920. [Google Scholar] [CrossRef]
- Sarnak, M.J.; Amann, K.; Bangalore, S.; Cavalcante, J.L.; Charytan, D.M.; Craig, J.C.; Gill, J.S.; Hlatky, M.A.; Jardine, A.G.; Landmesser, U.; et al. Chronic Kidney Disease and Coronary Artery Disease: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2019, 74, 1823–1838. [Google Scholar] [CrossRef] [PubMed]
- Sharma, K.; Ramachandrarao, S.; Qiu, G.; Usui, H.K.; Zhu, Y.; Dunn, S.R.; Ouedraogo, R.; Hough, K.; McCue, P.; Chan, L.; et al. Adiponectin regulates albuminuria and podocyte function in mice. J. Clin. Investig. 2008, 118, 1645–1656. [Google Scholar] [CrossRef]
- Mason, R.P.; Dawoud, H.; Jacob, R.F.; Sherratt, S.C.R.; Malinski, T. Eicosapentaenoic acid improves endothelial function and nitric oxide bioavailability in a manner that is enhanced in combination with a statin. Biomed. Pharmacother. 2018, 103, 1231–1237. [Google Scholar] [CrossRef]
- Ghayda, R.A.; Lee, J.Y.; Yang, J.W.; Han, C.H.; Jeong, G.H.; Yoon, S.; Hong, S.H.; Lee, K.H.; Gauckler, P.; Kronbichler, A.; et al. The effect of statins on all-cause and cardiovascular mortality in patients with non-dialysis chronic kidney disease, patients on dialysis, and kidney transplanted recipients: An umbrella review of meta-analyses. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 2696–2710. [Google Scholar]
- Herrington, W.G.; Emberson, J.; Mihaylova, B.; Blackwell, L.; Reith, C.; Solbu, M.D.; Mark, P.B.; Fellström, B.; Jardine, A.G.; Wanner, C.; et al. Impact of renal function on the effects of LDL cholesterol lowering with statin-based regimens: A meta-analysis of individual participant data from 28 randomised trials. Lancet Diabetes Endocrinol. 2016, 4, 829–839. [Google Scholar] [PubMed] [Green Version]
- Palmer, S.C.; Craig, J.C.; Navaneethan, S.D.; Tonelli, M.; Pellegrini, F.; Strippoli, G.F. Benefits and harms of statin therapy for persons with chronic kidney disease: A systematic review and meta-analysis. Ann. Intern. Med. 2012, 157, 263–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Major, R.W.; Cheung, C.K.; Gray, L.J.; Brunskill, N.J. Statins and Cardiovascular Primary Prevention in CKD: A Meta-Analysis. Clin. J. Am. Soc. Nephrol. 2015, 10, 732–739. [Google Scholar] [CrossRef] [Green Version]
- Baigent, C.; Landray, M.J.; Reith, C.; Emberson, J.; Wheeler, D.C.; Tomson, C.; Wanner, C.; Krane, V.; Cass, A.; Craig, J.; et al. The effects of lowering LDL cholesterol with simvastatin plus ezetimibe in patients with chronic kidney disease (Study of Heart and Renal Protection): A randomised placebo-controlled trial. Lancet 2011, 377, 2181–2192. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.H.; Her, A.Y.; Jeong, M.H.; Kim, B.K.; Hong, S.J.; Kim, J.S.; Ko, Y.G.; Choi, D.; Hong, M.K.; Jang, Y. Impact of stent generation on 2-year clinical outcomes in ST-segment elevation myocardial infarction patients with multivessel disease who underwent culprit-only or multivessel percutaneous coronary intervention. Catheter. Cardiovasc. Interv. 2020, 95, E40–E55. [Google Scholar] [CrossRef]
- Kim, Y.H.; Her, A.Y.; Jeong, M.H.; Kim, B.K.; Hong, S.J.; Kim, S.; Ahn, C.M.; Kim, J.S.; Ko, Y.G.; Choi, D.; et al. Effects of stent generation on clinical outcomes after acute myocardial infarction compared between prediabetes and diabetes patients. Sci. Rep. 2021, 11, 9364. [Google Scholar] [CrossRef]
- National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: Evaluation, classification, and stratification. Am. J. Kidney Dis. 2002, 39, S1–S266. [Google Scholar]
- Kim, J.H.; Chae, S.C.; Oh, D.J.; Kim, H.S.; Kim, Y.J.; Ahn, Y.; Cho, M.C.; Kim, C.J.; Yoon, J.H.; Park, H.Y.; et al. Multicenter Cohort Study of Acute Myocardial Infarction in Korea-Interim Analysis of the Korea Acute Myocardial Infarction Registry-National Institutes of Health Registry. Circ. J. 2016, 80, 1427–1436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grech, E.D. ABC of interventional cardiology: Percutaneous coronary intervention. II: The procedure. BMJ 2003, 326, 1137–1140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, K.Y.; Rha, S.W.; Li, Y.J.; Poddar, K.L.; Jin, Z.; Minami, Y.; Wang, L.; Kim, E.J.; Park, C.G.; Seo, H.S.; et al. Triple versus dual antiplatelet therapy in patients with acute ST-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention. Circulation 2009, 119, 3207–3214. [Google Scholar] [CrossRef]
- Lee, S.W.; Park, S.W.; Hong, M.K.; Kim, Y.H.; Lee, B.K.; Song, J.M.; Han, K.H.; Lee, C.W.; Kang, D.H.; Song, J.K.; et al. Triple versus dual antiplatelet therapy after coronary stenting: Impact on stent thrombosis. J. Am. Coll. Cardiol. 2005, 46, 1833–1837. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.M.; Rhee, T.M.; Hahn, J.Y.; Kim, H.K.; Park, J.; Hwang, D.; Choi, K.H.; Kim, J.; Park, T.K.; Yang, J.H.; et al. Multivessel Percutaneous Coronary Intervention in Patients With ST-Segment Elevation Myocardial Infarction With Cardiogenic Shock. J. Am. Coll. Cardiol. 2018, 71, 844–856. [Google Scholar] [CrossRef]
- Zhang, X.; Xiang, C.; Zhou, Y.H.; Jiang, A.; Qin, Y.Y.; He, J. Effect of statins on cardiovascular events in patients with mild to moderate chronic kidney disease: A systematic review and meta-analysis of randomized clinical trials. BMC Cardiovas. Disord. 2014, 14, 19. [Google Scholar] [CrossRef] [Green Version]
- Palmer, S.C.; Navaneethan, S.D.; Craig, J.C.; Johnson, D.W.; Perkovic, V.; Hegbrant, J.; Strippoli, G.F. HMG CoA reductase inhibitors (statins) for people with chronic kidney disease not requiring dialysis. Cochrane Database Syst. Rev. 2014, 31, Cd007784. [Google Scholar]
- Strippoli, G.F.; Craig, J.C.; Schena, F.P. The number, quality, and coverage of randomized controlled trials in nephrology. J. Am. Soc. Nephrpol. 2004, 15, 411–419. [Google Scholar] [CrossRef] [Green Version]
- Hashimoto, Y.; Ozaki, Y.; Kan, S.; Nakao, K.; Kimura, K.; Ako, J.; Noguchi, T.; Suwa, S.; Fujimoto, K.; Dai, K.; et al. Impact of Chronic Kidney Disease on In-Hospital and 3-Year Clinical Outcomes in Patients With Acute Myocardial Infarction Treated by Contemporary Percutaneous Coronary Intervention and Optimal Medical Therapy-Insights From the J-MINUET Study. Circ. J. 2021, CJ-20. [Google Scholar] [CrossRef]
- Herzog, C.A.; Littrell, K.; Arko, C.; Frederick, P.D.; Blaney, M. Clinical characteristics of dialysis patients with acute myocardial infarction in the United States: A collaborative project of the United States Renal Data System and the National Registry of Myocardial Infarction. Circulation 2007, 116, 1465–1472. [Google Scholar] [CrossRef] [Green Version]
- Tsutamoto, T.; Kawahara, C.; Yamaji, M.; Nishiyama, K.; Fujii, M.; Yamamoto, T.; Horie, M. Relationship between renal function and serum cardiac troponin T in patients with chronic heart failure. Eur. J. Heart Fail. 2009, 11, 653–658. [Google Scholar] [CrossRef] [PubMed]
- Manjunath, G.; Tighiouart, H.; Ibrahim, H.; MacLeod, B.; Salem, D.N.; Griffith, J.L.; Coresh, J.; Levey, A.S.; Sarnak, M.J. Level of kidney function as a risk factor for atherosclerotic cardiovascular outcomes in the community. J. Am. Coll. Cardiol. 2003, 41, 47–55. [Google Scholar] [CrossRef] [Green Version]
- London, G.M.; Guérin, A.P.; Marchais, S.J.; Métivier, F.; Pannier, B.; Adda, H. Arterial media calcification in end-stage renal disease: Impact on all-cause and cardiovascular mortality. Nephrol. Dial. Transplant. 2003, 18, 1731–1740. [Google Scholar] [CrossRef] [PubMed]
- Fox, C.S.; Matsushita, K.; Woodward, M.; Bilo, H.J.; Chalmers, J.; Heerspink, H.J.; Lee, B.J.; Perkins, R.M.; Rossing, P.; Sairenchi, T.; et al. Associations of kidney disease measures with mortality and end-stage renal disease in individuals with and without diabetes: A meta-analysis. Lancet 2012, 380, 1662–1673. [Google Scholar] [CrossRef] [Green Version]
- Natsuaki, M.; Furukawa, Y.; Morimoto, T.; Sakata, R.; Kimura, T. Renal function and effect of statin therapy on cardiovascular outcomes in patients undergoing coronary revascularization (from the CREDO-Kyoto PCI/CABG Registry Cohort-2). Am. J. Cardiol. 2012, 110, 1568–1577. [Google Scholar] [CrossRef]
- Petronio, A.S.; Amoroso, G.; Limbruno, U.; Papini, B.; De Carlo, M.; Micheli, A.; Ciabatti, N.; Mariani, M. Simvastatin does not inhibit intimal hyperplasia and restenosis but promotes plaque regression in normocholesterolemic patients undergoing coronary stenting: A randomized study with intravascular ultrasound. Am. Heart J. 2005, 149, 520–526. [Google Scholar] [CrossRef]
- Baigent, C.; Blackwell, L.; Emberson, J.; Holland, L.E.; Reith, C.; Bhala, N.; Peto, R.; Barnes, E.H.; Keech, A.; Simes, J.; et al. Efficacy and safety of more intensive lowering of LDL cholesterol: A meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet 2010, 376, 1670–1681. [Google Scholar]
- Walter, D.H.; Schächinger, V.; Elsner, M.; Mach, S.; Auch-Schwelk, W.; Zeiher, A.M. Effect of statin therapy on restenosis after coronary stent implantation. Am. J. Cardiol. 2000, 85, 962–968. [Google Scholar] [CrossRef]
- Crimi, G.; Gritti, V.; Galiffa, V.A.; Scotti, V.; Leonardi, S.; Ferrario, M.; Ferlini, M.; De Ferrari, G.M.; Oltrona Visconti, L.; Klersy, C. Drug eluting stents are superior to bare metal stents to reduce clinical outcome and stent-related complications in CKD patients, a systematic review, meta-analysis and network meta-analysis. J. Interv. Cardiol. 2018, 31, 319–329. [Google Scholar] [CrossRef] [Green Version]
- Volodarskiy, A.; Kumar, S.; Pracon, R.; Sidhu, M.; Kretov, E.; Mazurek, T.; Bockeria, O.; Kaul, U.; Bangalore, S. Drug-Eluting vs. Bare-Metal Stents in Patients with Chronic Kidney Disease and Coronary Artery Disease: Insights From a Systematic Review and Meta-Analysis. J. Invasive Cardiol. 2018, 30, 10–17. [Google Scholar] [PubMed]
- Arbustini, E.; Dal Bello, B.; Morbini, P.; Burke, A.P.; Bocciarelli, M.; Specchia, G.; Virmani, R. Plaque erosion is a major substrate for coronary thrombosis in acute myocardial infarction. Heart 1999, 82, 269–272. [Google Scholar] [CrossRef] [Green Version]
- Ozaki, Y.; Okumura, M.; Ismail, T.F.; Motoyama, S.; Naruse, H.; Hattori, K.; Kawai, H.; Sarai, M.; Takagi, Y.; Ishii, J.; et al. Coronary CT angiographic characteristics of culprit lesions in acute coronary syndromes not related to plaque rupture as defined by optical coherence tomography and angioscopy. Eur. Heart J. 2011, 32, 2814–2823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Özyilmaz, A.; Bakker, S.J.; de Zeeuw, D.; de Jong, P.E.; Gansevoort, R.T. Selection on albuminuria enhances the efficacy of screening for cardiovascular risk factors. Nephrol. Dial. Transplant. 2010, 25, 3560–3568. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| Variables | Total (n = 16,055) | Group A1 eGFR ≥ 90 mL/min/1.73 m2 (n = 6847) | Group A2 eGFR 60–89 mL/min/1.73 m2 (n = 6557) | Group A3 eGFR 30–59 mL/min/1.73 m2 (n = 2144) | Group A4 eGFR < 30 mL/min/1.73 m2 (n = 507) | p Value |
|---|---|---|---|---|---|---|
| Male, n (%) | 12,053 (75.1) | 5536 (80.9) | 4988 (76.1) | 1225 (57.1) | 304 (60.0) | <0.001 |
| Age (years) | 63.0 ± 12.3 | 58.9 ± 11.5 | 64.3 ± 12.1 | 70.8 ± 10.4 | 68.9 ± 10.9 | <0.001 |
| LVEF (%) | 52.8 ± 10.8 | 54.0 ± 10.0 | 52.8 ± 10.7 | 50.0 ± 12.3 | 48.1 ± 11.9 | <0.001 |
| BMI (kg/m2) | 24.2 ± 3.2 | 24.3 ± 3.2 | 24.2 ± 3.2 | 23.9 ± 3.2 | 23.5 ±3.4 | <0.001 |
| SBP (mmHg) | 131.6 ± 27.2 | 133.4 ± 25.0 | 131.4 ± 27.7 | 126.6 ± 30.2 | 132.2 ± 33.3 | <0.001 |
| DBP (mmHg) | 79.9 ± 16.2 | 81.7 ± 15.3 | 79.6 ± 16.4 | 75.7 ± 17.1 | 77.4 ± 18.0 | <0.001 |
| Cardiogenic shock, n (%) | 575 (3.6) | 124 (1.8) | 247 (3.8) | 160 (7.5) | 44 (8.7) | <0.001 |
| CPR on admission, n (%) | 557 (3.5) | 186 (2.7) | 218 (3.3) | 129 (6.0) | 24 (4.7) | <0.001 |
| Killip class III/IV, n (%) | 1454 (9.1) | 322 (4.7) | 578 (8.8) | 416 (19.4) | 138 (27.2) | <0.001 |
| STEMI, n (%) | 8737 (54.4) | 3640 (53.2) | 3764 (57.4) | 1160 (54.1) | 173 (34.1) | <0.001 |
| Primary PCI, n (%) | 8424 (96.4) | 3511 (96.5) | 3633 (96.5) | 1115 (96.1) | 165 (95.4) | 0.809 |
| NSTEMI, n (%) | 7318 (45.6) | 3207 (46.8) | 2793 (42.6) | 984 (45.9) | 334 (65.9) | <0.001 |
| PCI within 24 h, n (%) | 6303 (86.1) | 2865 (89.3) | 2384 (85.4) | 791 (80.4) | 263 (78.7) | <0.001 |
| Hypertension, n (%) | 7761 (48.3) | 2622 (38.3) | 3238 (49.4) | 1489 (69.4) | 412 (81.3) | <0.001 |
| Diabetes mellitus, n (%) | 4201 (26.2) | 1446 (21.1) | 1534 (23.4) | 903 (42.1) | 318 (62.7) | <0.001 |
| Dyslipidemia, n (%) | 1936 (12.1) | 792 (11.6) | 815 (12.4) | 271 (12.6) | 58 (11.4) | 0.351 |
| Previous MI, n (%) | 661 (4.1) | 214 (3.1) | 261 (4.0) | 140 (6.5) | 46 (9.1) | <0.001 |
| Previous PCI, n (%) | 1008 (6.3) | 327 (4.8) | 394 (6.0) | 215 (10.0) | 72 (14.2) | <0.001 |
| Previous CABG, n (%) | 72 (0.4) | 18 (0.3) | 23 (0.4) | 23 (1.1) | 8 (1.6) | <0.001 |
| Previous HF, n (%) | 150 (0.9) | 24 (0.4) | 52 (0.8) | 54 (2.5) | 20 (3.9) | <0.001 |
| Previous CVA, n (%) | 947 (5.9) | 252 (3.7) | 390 (5.9) | 241 (11.2) | 64 (12.6) | <0.001 |
| Current smokers, n (%) | 6957 (43.3) | 3560 (52.0) | 2721 (41.5) | 566 (26.4) | 110 (21.7) | <0.001 |
| Peak CK-MB (mg/dL) | 121.2 ± 186.0 | 123.9 ± 178.0 | 128.1 ± 206.3 | 103.5 ± 151.0 | 70.8 ± 127.9 | <0.001 |
| Peak troponin-I (ng/mL) | 47.0 ± 128.3 | 41.9 ± 69.5 | 48.6 ± 138.4 | 46.4 ± 94.5 | 97.1 ± 204.6 | <0.001 |
| NT-ProBNP (pg/mL) | 1935.2 ± 4876.9 | 1258.8 ± 1542.6 | 1543.0 ± 2163.7 | 3188.7 ± 5091.2 | 9248.5 ± 8231.4 | <0.001 |
| High-sensitivity CRP (mg/dL) | 7.5 ± 37.5 | 6.1 ± 31.8 | 8.3 ± 42.5 | 8.9 ± 38.6 | 10.1 ± 32.4 | <0.001 |
| Serum creatinine (mg/L) | 1.1 ± 1.1 | 0.7 ± 0.1 | 1.0 ± 0.2 | 1.4 ± 0.3 | 5.1 ± 4.6 | <0.001 |
| eGFR (mL/min/1.73 m2) | 87.5 ± 35.5 | 115.3 ± 33.7 | 76.3 ± 8.5 | 49.2 ± 8.0 | 16.5 ± 8.5 | <0.001 |
| Blood glucose (mg/L) | 165.8 ± 76.7 | 155.2 ± 63.4 | 163.2 ± 70.4 | 197.3 ± 101.1 | 209.0 ± 129.7 | <0.001 |
| Total cholesterol (mg/dL) | 184.3 ± 45.4 | 186.4 ± 43.1 | 186.0 ± 45.6 | 177.1 ± 47.9 | 162.4 ± 52.3 | <0.001 |
| Triglyceride (mg/L) | 137.0 ± 114.0 | 140.0 ± 118.0 | 137.6 ± 114.9 | 128.3 ± 96.9 | 125.7 ± 111.3 | <0.001 |
| HDL cholesterol (mg/L) | 43.3 ± 14.7 | 43.3 ± 13.3 | 43.8 ± 15.5 | 42.7 ± 16.5 | 39.3 ± 12.7 | <0.001 |
| LDL cholesterol (mg/L) | 116.4 ± 40.7 | 119.4 ± 41.2 | 116.9 ± 37.5 | 109.5 ± 46.5 | 95.9 ± 38.8 | <0.001 |
| Discharge medications, n (%) | ||||||
| Aspirin, n (%) | 15,954 (99.4) | 6814 (99.5) | 6515 (99.4) | 2127 (99.2) | 498 (98.2) | 0.003 |
| Clopidogrel, n (%) | 13,600 (84.7) | 5528 (80.7) | 5674 (86.5) | 1941 (90.5) | 457 (90.1) | <0.001 |
| Ticagrelor, n (%) | 1565 (9.7) | 786 (11.5) | 599 (9.1) | 145 (6.8) | 35 (6.9) | <0.001 |
| Prasugrel, n (%) | 890 (5.5) | 533 (7.8) | 284 (4.3) | 58 (2.7) | 15 (3.0) | <0.001 |
| Cilostazole, n (%) | 2903 (18.1) | 1146 (16.7) | 1226 (18.7) | 434 (20.2) | 97 (19.1) | 0.001 |
| ACEIs, n (%) | 8977 (55.9) | 3784 (55.3) | 3893 (59.4) | 1122 (52.3) | 178 (35.1) | <0.001 |
| ARBs, n (%) | 4580 (28.5) | 2023 (29.5) | 1665 (25.4) | 677 (31.6) | 215 (42.4) | <0.001 |
| BBs, n (%) | 13,856 (86.3) | 5984 (87.4) | 5666 (86.4) | 1775 (82.8) | 431 (85.0) | <0.001 |
| CCBs, n (%) | 960 (6.0) | 313 (4.6) | 389 (5.9) | 177 (8.3) | 81 (16.0) | <0.001 |
| Statin, n (%) | ||||||
| Atorvastatin, n (%) | 8636 (53.8) | 3556 (51.9) | 3552 (54.2) | 1202 (56.1) | 326 (64.3) | <0.001 |
| Rosuvastatin, n (%) | 5003 (31.2) | 2254 (32.9) | 2025 (30.9) | 608 (28.4) | 116 (22.9) | <0.001 |
| Simvastatin, n (%) | 949 (5.9) | 378 (5.5) | 412 (6.3) | 133 (6.2) | 26 (5.1) | 0.222 |
| Pitavastatin, n (%) | 1211 (7.5) | 559 (8.1) | 478 (7.3) | 154 (7.2) | 20 (3.9) | 0.003 |
| Pravastatin, n (%) | 214 (1.3) | 86 (1.3) | 76 (1.2) | 40 (1.9) | 12 (2.4) | 0.014 |
| Fluvastatin, n (%) | 42 (0.3) | 14 (0.2) | 14 (0.2) | 7 (0.3) | 7 (1.4) | <0.001 |
| Infarct-related artery | ||||||
| Left main, n (%) | 294 (1.8) | 111 (1.6) | 106 (1.6) | 51 (2.4) | 26 (5.1) | <0.001 |
| LAD, n (%) | 7704 (48.0) | 3440 (50.2) | 3126 (47.7) | 917 (42.8) | 221 (43.6) | <0.001 |
| LCx, n (%) | 2713 (16.9) | 1232 (18.0) | 1085 (16.5) | 324 (15.1) | 72 (14.2) | 0.003 |
| RCA, n (%) | 5344 (33.3) | 2064 (30.1) | 2240 (34.2) | 852 (39.7) | 188 (37.1) | <0.001 |
| Treated vessel | ||||||
| Left main, n (%) | 468 (2.9) | 175 (2.6) | 179 (2.7) | 82 (3.8) | 32 (6.3) | <0.001 |
| LAD, n (%) | 9348 (58.2) | 4105 (60.0) | 3770 (57.5) | 1175 (54.8) | 298 (58.8) | <0.001 |
| LCx, n (%) | 4239 (26.4) | 1875 (27.4) | 1675 (25.5) | 568 (26.5) | 121 (23.9) | 0.056 |
| RCA, n (%) | 6401 (39.9) | 2509 (36.6) | 2672 (40.8) | 997 (46.5) | 223 (44.0) | <0.001 |
| ACC/AHA lesion type | ||||||
| Type B1, n (%) | 2180 (13.6) | 827 (12.1) | 978 (14.9) | 303 (14.1) | 72 (14.2) | <0.001 |
| Type B2, n (%) | 5677 (35.4) | 2643 (38.6) | 2140 (32.6) | 720 (33.6) | 174 (34.3) | <0.001 |
| Type C, n (%) | 7249 (45.2) | 3026 (44.2) | 3002 (45.8) | 983 (45.8) | 238 (46.9) | 0.198 |
| Extent of CAD | ||||||
| Single-vessel, n (%) | 8150 (50.8) | 3827 (55.9) | 3250 (49.6) | 875 (40.8) | 198 (39.1) | <0.001 |
| 2-vessel, n (%) | 4712 (29.3) | 1925 (28.1) | 1968 (30.0) | 671 (31.3) | 148 (29.2) | 0.016 |
| ≥3-vessel, n (%) | 3193 (19.9) | 1095 (16.0) | 1339 (20.4) | 598 (27.9) | 161 (31.8) | <0.001 |
| Pre-PCI TIMI 0/1, n (%) | 9308 (58.0) | 3857 (56.3) | 3966 (60.5) | 1258 (58.7) | 227 (44.8) | <0.001 |
| Type of stent | ||||||
| ZES, n (%) | 5591 (34.8) | 2219 (32.4) | 2404 (36.7) | 801 (37.4) | 167 (32.9) | <0.001 |
| EES, n (%) | 7888 (49.1) | 3335 (48.7) | 3187 (48.6) | 1092 (50.9) | 274 (54.0) | 0.031 |
| BES, n (%) | 2418 (15.1) | 1161 (17.0) | 944 (14.4) | 249 (11.6) | 64 (12.6) | <0.001 |
| Others, n (%) | 475 (3.0) | 264 (3.9) | 160 (2.4) | 43 (2.0) | 8 (1.6) | <0.001 |
| IVUS, n (%) | 3619 (19.7) | 1358 (19.8) | 1321 (20.1) | 401 (18.7) | 89 (17.6) | 0.295 |
| OCT, n (%) | 113 (0.7) | 61 (0.9) | 47 (0.7) | 4 (0.2) | 1 (0.2) | 0.004 |
| FFR, n (%) | 211 (1.3) | 135 (2.0) | 69 (1.0) | 5 (0.2) | 2 (0.4) | <0.001 |
| Stent diameter (mm) | 3.15 ± 0.42 | 3.16 ± 0.42 | 3.16 ± 0.43 | 3.11 ± 0.42 | 3.09 ± 0.43 | <0.001 |
| Stent length (mm) | 27.1 ± 11.7 | 26.9 ± 11.6 | 26.9 ± 11.5 | 27.8 ± 12.3 | 29.0 ± 13.7 | <0.001 |
| Number of stents | 1.48 ± 0.79 | 1.45 ± 0.77 | 1.48 ± 0.79 | 1.54 ± 0.82 | 1.60 ± 0.87 | <0.001 |
| Variables | Total (n = 2820) | Group B1 eGFR ≥ 90 mL/min/1.73 m2 (n = 889) | Group B2 eGFR 60–89 mL/min/1.73 m2 (n = 1227) | Group B3 eGFR 30–59 mL/min/1.73 m2 (n = 537) | Group B4 eGFR < 30 mL/min/1.73 m2 (n = 167) | p Value |
|---|---|---|---|---|---|---|
| Male, n (%) | 2067 (73.3) | 730 (82.1) | 921 (75.1) | 317 (59.0) | 99 (59.3) | <0.001 |
| Age (years) | 64.1 ± 12.4 | 58.8 ± 11.6 | 64.3 ± 12.2 | 70.8 ± 10.5 | 69.8 ± 10.4 | <0.001 |
| LVEF (%) | 50.9 ± 12.2 | 52.9 ± 11.5 | 51.5 ± 11.7 | 48.4 ± 13.1 | 44.2 ± 12.8 | <0.001 |
| BMI (kg/m2) | 23.8 ± 3.3 | 23.9 ± 3.4 | 23.8 ± 3.2 | 23.7 ± 3.5 | 23.1 ±3.4 | 0.055 |
| SBP (mmHg) | 128.6 ± 29.1 | 132.2 ± 26.7 | 129.7 ± 27.6 | 120.0 ± 32.1 | 128.0 ± 25.8 | <0.001 |
| DBP (mmHg) | 77.9 ± 16.8 | 80.7 ± 15.3 | 78.9 ± 16.4 | 72.0 ± 17.5 | 73.7 ± 19.6 | <0.001 |
| Cardiogenic shock, n (%) | 153 (5.4) | 22 (2.5) | 48 (3.9) | 58 (10.8) | 25 (15.0) | <0.001 |
| CPR on admission, n (%) | 151 (5.4) | 30 (3.4) | 59 (4.8) | 51 (9.5) | 11 (6.6) | <0.001 |
| Killip class III/IV, n (%) | 393 (13.9) | 53 (6.0) | 140 (11.4) | 146 (27.2) | 54 (32.3) | <0.001 |
| STEMI, n (%) | 1630 (57.8) | 512 (57.6) | 744 (60.6) | 309 (57.5) | 65 (38.9) | <0.001 |
| Primary PCI, n (%) | 1551 (95.2) | 485 (94.7) | 705 (94.8) | 297 (96.1) | 64 (98.5) | 0.454 |
| NSTEMI, n (%) | 1190 (42.2) | 377 (42.4) | 483(39.4) | 228 (42.5) | 102 (61.1) | <0.001 |
| PCI within 24 h | 912 (76.6) | 299 (79.3) | 366 (75.8) | 170 (74.6) | 77 (75.5) | 0.507 |
| Hypertension, n (%) | 1391 (49.3) | 318 (35.8) | 598 (48.7) | 340 (63.3) | 135 (80.8) | <0.001 |
| Diabetes mellitus, n (%) | 867 (30.7) | 233 (26.2) | 309 (25.2) | 216 (40.2) | 109 (65.3) | <0.001 |
| Dyslipidemia, n (%) | 249 (8.8) | 75 (8.4) | 108 (8.8) | 48 (8.9) | 18 (10.8) | 0.809 |
| Previous MI, n (%) | 96 (3.4) | 21 (2.4) | 33 (2.7) | 27 (5.0) | 15 (9.0) | <0.001 |
| Previous PCI, n (%) | 186 (6.6) | 44 (4.9) | 73 (8.9) | 52 (9.7) | 17 (10.2) | 0.001 |
| Previous CABG, n (%) | 12 (0.4) | 2 (0.2) | 3 (0.2) | 6 (1.0) | 1 (0.6) | 0.047 |
| Previous HF, n (%) | 58 (2.1) | 9 (1.0) | 19 (1.5) | 19 (3.5) | 11 (6.6) | <0.001 |
| Previous CVA, n (%) | 193 (6.8) | 36 (4.0) | 75 (6.1) | 57 (10.6) | 25 (15.0) | <0.001 |
| Current smokers, n (%) | 1157 (41.0) | 471 (53.0) | 498 (40.6) | 158 (29.4) | 30 (18.0) | <0.001 |
| Peak CK-MB (mg/dL) | 144.5 ± 319.5 | 127.7 ± 154.2 | 168.6 ± 442.3 | 133.8 ± 201.7 | 91.7 ± 144.5 | 0.002 |
| Peak troponin-I (ng/mL) | 46.8 ± 85.9 | 42.4 ± 61.2 | 48.2 ± 87.5 | 48.2 ± 92.3 | 55.3 ± 145.3 | 0.215 |
| NT-ProBNP (pg/mL) | 2487.6 ± 4085.6 | 1499.8 ± 2460.2 | 1599.3 ± 2089.5 | 3802.2 ± 5998.2 | 9948.8 ± 9432.6 | <0.001 |
| High-sensitivity CRP (mg/dL) | 9.8 ± 38.1 | 9.1 ± 34.5 | 8.3 ± 33.9 | 12.7 ± 47.9 | 15.2 ± 48.2 | <0.001 |
| Serum creatinine (mg/L) | 1.2 ± 1.4 | 0.7 ± 0.1 | 1.0 ± 1.2 | 1.4 ± 0.3 | 5.1 ± 3.7 | <0.001 |
| eGFR (mL/min/1.73 m2) | 76.8 ± 38.3 | 114.7 ± 44.3 | 75.6 ± 8.5 | 48.6 ± 8.2 | 15.8 ± 8.2 | <0.001 |
| Blood glucose (mg/L) | 177.7 ± 85.5 | 163.4 ± 65.7 | 169.6 ± 75.1 | 207.9 ± 108.3 | 217.0 ± 124.4 | <0.001 |
| Total cholesterol (mg/dL) | 174.4 ± 43.5 | 180.4 ± 44.1 | 178.1 ± 41.5 | 163.9 ± 41.6 | 148.2 ± 45.6 | <0.001 |
| Triglyceride (mg/L) | 132.4 ± 114.0 | 142.0 ± 122.3 | 135.5 ± 125.1 | 113.2 ± 73.0 | 117.5 ± 68.7 | <0.001 |
| HDL cholesterol (mg/L) | 43.0 ± 15.6 | 43.1 ± 11.7 | 43.8 ± 17.1 | 42.5 ± 17.6 | 37.9 ± 14.8 | <0.001 |
| LDL cholesterol (mg/L) | 108.2 ± 39.2 | 112.5 ± 37.6 | 111.3 ± 38.1 | 100.7 ± 41.8 | 83.9 ± 36.4 | <0.001 |
| Discharge medications, n (%) | ||||||
| Aspirin, n (%) | 2714 (96.2) | 848 (95.5) | 1192 (97.1) | 518 (96.5) | 156 (93.4) | 0.040 |
| Clopidogrel, n (%) | 2726 (96.6) | 843 (94.8) | 1200 (97.8) | 523 (91.1) | 160 (95.8) | <0.001 |
| Ticagrelor, n (%) | 53 (1.9) | 22 (2.5) | 16 (1.3) | 10 (1.9) | 5 (3.0) | 0.169 |
| Prasugrel, n (%) | 41 (1.5) | 24 (2.7) | 11 (0.9) | 4 (0.7) | 2 (1.2) | 0.003 |
| Cilostazole, n (%) | 483 (17.1) | 139 (15.6) | 241 (19.6) | 82 (15.3) | 21 (12.6) | 0.014 |
| ACEIs, n (%) | 1127 (40.0) | 356 (40.0) | 539 (43.9) | 189 (35.2) | 43 (25.7) | <0.001 |
| ARBs, n (%) | 677 (24.0) | 238 (26.8) | 280 (22.8) | 124 (23.1) | 35 (21.0) | 0.123 |
| BBs, n (%) | 1838 (65.2) | 605 (68.1) | 839 (68.4) | 315 (58.7) | 79 (47.3) | <0.001 |
| CCBs, n (%) | 176 (6.2) | 44 (4.9) | 70 (5.7) | 41 (7.6) | 21 (12.6) | 0.001 |
| Infarct-related artery | ||||||
| Left main, n (%) | 58 (2.1) | 20 (2.2) | 14 (1.1) | 16 (3.0) | 8 (4.8) | 0.003 |
| LAD, n (%) | 1324 (47.0) | 434 (48.8) | 593 (48.3) | 228 (42.4) | 69 (41.3) | 0.037 |
| LCx, n (%) | 451 (16.0) | 163 (18.3) | 190 (15.5) | 69 (12.8) | 29 (17.4) | 0.045 |
| RCA, n (%) | 987 (35.0) | 272 (30.6) | 430 (35.0) | 224 (41.7) | 61 (36.5) | <0.001 |
| Treated vessel | ||||||
| Left main, n (%) | 77 (2.7) | 26 (2.9) | 21 (1.7) | 17 (3.2) | 13 (7.8) | <0.001 |
| LAD, n (%) | 1552 (55.0) | 508 (57.1) | 676 (55.1) | 278 (51.8) | 90 (53.9) | 0.261 |
| LCx, n (%) | 670 (23.8) | 228 (25.6) | 274 (22.3) | 127 (23.6) | 41 (24.6) | 0.363 |
| RCA, n (%) | 1132 (40.1) | 318 (35.8) | 492 (40.1) | 253 (47.1) | 99 (41.3) | <0.001 |
| ACC/AHA lesion type | ||||||
| Type B1, n (%) | 509 (18.0) | 161 (18.1) | 223 (18.2) | 109 (20.3) | 16 (9.6) | 0.019 |
| Type B2, n (%) | 857 (30.4) | 296 (33.3) | 371 (30.2) | 133 (24.8) | 57 (34.1) | 0.005 |
| Type C, n (%) | 1141 (40.5) | 340 (38.2) | 494 (40.3) | 224 (41.7) | 83 (49.7) | 0.044 |
| Extent of CAD | ||||||
| Single-vessel, n (%) | 1369 (48.5) | 481 (54.1) | 614 (50.0) | 211 (39.3) | 63 (37.7) | <0.001 |
| 2-vessel, n (%) | 818 (29.0) | 242 (27.2) | 352 (28.7) | 172 (32.0) | 52 (31.1) | 0.242 |
| ≥3-vessel, n (%) | 633 (22.4) | 166 (18.7) | 261 (21.3) | 154 (28.7) | 52 (31.1) | <0.001 |
| Pre-PCI TIMI 0/1, n (%) | 1745 (61.9) | 544 (61.2) | 788 (64.2) | 330 (61.5) | 83 (49.7) | 0.004 |
| Type of stent | ||||||
| ZES, n (%) | 1171 (41.5) | 347 (39.0) | 526 (42.9) | 233 (43.4) | 65 (38.9) | 0.219 |
| EES, n (%) | 1269 (45.0) | 389 (43.8) | 556 (45.3) | 245 (45.9) | 79 (47.3) | 0.790 |
| BES, n (%) | 315 (11.2) | 123 (13.8) | 122 (9.9) | 52 (9.7) | 18 (10.8) | 0.024 |
| Others, n (%) | 84 (3.0) | 34 (3.8) | 31 (2.5) | 12 (2.2) | 7 (4.2) | 0.176 |
| IVUS, n (%) | 502 (17.8) | 169 (19.0) | 218 (17.8) | 85 (15.8) | 30 (18.0) | 0.509 |
| OCT, n (%) | 17 (0.6) | 7 (0.8) | 7 (0.6) | 3 (0.6) | 0 | 0.669 |
| FFR, n (%) | 7 (0.2) | 3 (0.3) | 0 | 3 (0.6) | 1 (0.6) | 0.100 |
| Stent diameter (mm) | 3.16 ± 0.44 | 3.18 ± 0.43 | 3.17 ± 0.43 | 3.11 ± 0.44 | 3.11 ± 0.44 | 0.019 |
| Stent length (mm) | 25.0 ± 9.4 | 24.1 ± 8.1 | 24.7 ± 8.5 | 26.0 ± 11.1 | 28.1 ± 14.4 | <0.001 |
| Number of stents | 1.43 ± 0.76 | 1.40 ± 0.72 | 1.40 ± 0.75 | 1.53 ± 0.82 | 1.51 ± 0.76 | 0.004 |
| Variables | Group A1 eGFR ≥ 90 mL/min/1.73 m2 (n = 6847) | Group B1 eGFR ≥ 90 mL/min/1.73 m2 (n = 889) | p Value | Group A2 eGFR 60–89 mL/min/1.73 m2 (n = 6557) | Group B2 eGFR 60–89 mL/min/1.73 m2 (n = 1227) | p Value |
|---|---|---|---|---|---|---|
| Male, n (%) | 5536 (80.9) | 730 (82.1) | 0.367 | 4988 (76.1) | 921 (75.1) | 0.448 |
| Age (years) | 58.9 ± 11.5 | 58.8 ± 11.6 | 0.848 | 64.3 ± 12.1 | 64.3 ± 12.2 | 0.915 |
| LVEF (%) | 54.0 ± 10.0 | 52.9 ± 11.5 | 0.007 | 52.8 ± 10.7 | 51.5 ± 11.7 | 0.001 |
| BMI (kg/m2) | 24.2 ± 3.2 | 23.9 ± 3.4 | 0.009 | 24.2 ± 3.2 | 23.8 ± 3.2 | <0.001 |
| SBP (mmHg) | 133.4 ± 25.0 | 132.2 ± 26.7 | 0.221 | 131.4 ± 27.7 | 129.7 ± 27.6 | 0.051 |
| DBP (mmHg) | 81.7 ± 15.3 | 80.7 ± 15.3 | 0.074 | 79.6 ± 16.4 | 78.9 ± 16.4 | 0.220 |
| Cardiogenic shock, n (%) | 124 (1.8) | 22 (2.5) | 0.171 | 247 (3.8) | 48 (3.9) | 0.807 |
| CPR on admission, n (%) | 186 (2.7) | 30 (3.4) | 0.263 | 218 (3.3) | 59 (4.8) | 0.010 |
| Killip class III/IV, n (%) | 322 (4.7) | 53 (6.0) | 0.100 | 578 (8.8) | 140 (11.4) | 0.004 |
| STEMI, n (%) | 3640 (53.2) | 512 (57.6) | 0.013 | 3764 (57.4) | 744 (60.6) | 0.035 |
| Primary PCI, n (%) | 3511 (96.5) | 485 (94.7) | 0.054 | 3633 (96.5) | 705 (94.8) | 0.021 |
| NSTEMI, n (%) | 3207 (46.8) | 377 (42.4) | 0.013 | 2793 (42.6) | 483(39.4) | 0.035 |
| PCI within 24 h | 2865 (89.3) | 299 (79.3) | <0.001 | 2384 (85.4) | 366 (75.8) | <0.001 |
| Hypertension, n (%) | 2622 (38.3) | 318 (35.8) | 0.145 | 3238 (49.4) | 598 (48.7) | 0.678 |
| Diabetes mellitus, n (%) | 1446 (21.1) | 233 (26.2) | 0.001 | 1534 (23.4) | 309 (25.2) | 0.176 |
| Dyslipidemia, n (%) | 792 (11.6) | 75 (8.4) | 0.005 | 815 (12.4) | 108 (8.8) | <0.001 |
| Previous MI, n (%) | 214 (3.1) | 21 (2.4) | 0.212 | 261 (4.0) | 33 (2.7) | 0.029 |
| Previous PCI, n (%) | 327 (4.8) | 44 (4.9) | 0.820 | 394 (6.0) | 73 (8.9) | 0.936 |
| Previous CABG, n (%) | 18 (0.3) | 2 (0.2) | 0.834 | 23 (0.4) | 3 (0.2) | 0.788 |
| Previous HF, n (%) | 24 (0.4) | 9 (1.0) | 0.004 | 52 (0.8) | 19 (1.5) | 0.011 |
| Previous CVA, n (%) | 252 (3.7) | 36 (4.0) | 0.585 | 390 (5.9) | 75 (6.1) | 0.823 |
| Current smokers, n (%) | 3560 (52.0) | 471 (53.0) | 0.579 | 2721 (41.5) | 498 (40.6) | 0.552 |
| Peak CK-MB (mg/dL) | 123.9 ± 178.0 | 127.7 ± 154.2 | 0.538 | 128.1 ± 206.3 | 168.6 ± 442.3 | 0.002 |
| Peak troponin-I (ng/mL) | 41.9 ± 69.5 | 42.4 ± 61.2 | 0.823 | 48.6 ± 138.4 | 48.2 ± 87.5 | 0.905 |
| NT-ProBNP (pg/mL) | 1258.8 ± 1542.6 | 1499.8 ± 2460.2 | 0.004 | 1543.0 ± 2163.7 | 1599.3 ± 2089.5 | 0.389 |
| High-sensitivity CRP (mg/dL) | 6.1 ± 31.8 | 9.1 ± 34.5 | 0.012 | 8.3 ± 42.5 | 8.3 ± 33.9 | 0.972 |
| Serum creatinine (mg/L) | 0.7 ± 0.1 | 0.7 ± 0.1 | 0.062 | 1.0 ± 0.2 | 1.0 ± 1.2 | 0.245 |
| eGFR (mL/min/1.73 m2) | 115.3 ± 33.7 | 114.7 ± 44.3 | 0.725 | 76.3 ± 8.5 | 75.6 ± 8.5 | 0.060 |
| Blood glucose (mg/L) | 155.2 ± 63.4 | 163.4 ± 65.7 | 0.001 | 163.2 ± 70.4 | 169.6 ± 75.1 | 0.007 |
| Total cholesterol (mg/dL) | 186.4 ± 43.1 | 180.4 ± 44.1 | <0.001 | 186.0 ± 45.6 | 178.1 ± 41.5 | <0.001 |
| Triglyceride (mg/L) | 140.0 ± 118.0 | 142.0 ± 122.3 | 0.639 | 137.6 ± 114.9 | 135.5 ± 125.1 | 0.592 |
| HDL cholesterol (mg/L) | 43.3 ± 13.3 | 43.1 ± 11.7 | 0.676 | 43.8 ± 15.5 | 43.8 ± 17.1 | 0.943 |
| LDL cholesterol (mg/L) | 119.4 ± 41.2 | 112.5 ± 37.6 | <0.001 | 116.9 ± 37.5 | 111.3 ± 38.1 | <0.001 |
| Discharge medications, n (%) | ||||||
| Aspirin, n (%) | 6814 (99.5) | 848 (95.5) | <0.001 | 6515 (99.4) | 1192 (97.1) | <0.001 |
| Clopidogrel, n (%) | 5528 (80.7) | 843 (94.8) | <0.001 | 5674 (86.5) | 1200 (97.8) | <0.001 |
| Ticagrelor, n (%) | 786 (11.5) | 22 (2.5) | <0.001 | 599 (9.1) | 16 (1.3) | <0.001 |
| Prasugrel, n (%) | 533 (7.8) | 24 (2.7) | <0.001 | 284 (4.3) | 11 (0.9) | <0.001 |
| Cilostazole, n (%) | 1146 (16.7) | 139 (15.6) | 0.406 | 1226 (18.7) | 241 (19.6) | 0.438 |
| ACEIs, n (%) | 3784 (55.3) | 356 (40.0) | <0.001 | 3893 (59.4) | 539 (43.9) | <0.001 |
| ARBs, n (%) | 2023 (29.5) | 238 (26.8) | 0.087 | 1665 (25.4) | 280 (22.8) | 0.057 |
| BBs, n (%) | 5984 (87.4) | 605 (68.1) | <0.001 | 5666 (86.4) | 839 (68.4) | <0.001 |
| CCBs, n (%) | 313 (4.6) | 44 (4.9) | 0.613 | 389 (5.9) | 70 (5.7) | 0.792 |
| Statin, n (%) | ||||||
| Atorvastatin, n (%) | 3556 (51.9) | 3552 (54.2) | ||||
| Rosuvastatin, n (%) | 2254 (32.9) | 2025 (30.9) | ||||
| Simvastatin, n (%) | 378 (5.5) | 412 (6.3) | ||||
| Pitavastatin, n (%) | 559 (8.1) | 478 (7.3) | ||||
| Pravastatin, n (%) | 86 (1.3) | 76 (1.2) | ||||
| Fluvastatin, n (%) | 14 (0.2) | 14 (0.2) | ||||
| Infarct-related artery | ||||||
| Left main, n (%) | 111 (1.6) | 20 (2.2) | 0.172 | 106 (1.6) | 14 (1.1) | 0.256 |
| LAD, n (%) | 3440 (50.2) | 434 (48.8) | 0.347 | 3126 (47.7) | 593 (48.3) | 0.747 |
| LCx, n (%) | 1232 (18.0) | 163 (18.3) | 0.803 | 1085 (16.5) | 190 (15.5) | 0.356 |
| RCA, n (%) | 2064 (30.1) | 272 (30.6) | 0.783 | 2240 (34.2) | 430 (35.0) | 0.550 |
| Treated vessel | ||||||
| Left main, n (%) | 175 (2.6) | 26 (2.9) | 0.516 | 179 (2.7) | 21 (1.7) | 0.039 |
| LAD, n (%) | 4105 (60.0) | 508 (57.1) | 0.108 | 3770 (57.5) | 676 (55.1) | 0.119 |
| LCx, n (%) | 1875 (27.4) | 228 (25.6) | 0.273 | 1675 (25.5) | 274 (22.3) | 0.018 |
| RCA, n (%) | 2509 (36.6) | 318 (35.8) | 0.611 | 2672 (40.8) | 492 (40.1) | 0.669 |
| ACC/AHA lesion type | ||||||
| Type B1, n (%) | 827 (12.1) | 161 (18.1) | <0.001 | 978 (14.9) | 223 (18.2) | 0.004 |
| Type B2, n (%) | 2643 (38.6) | 296 (33.3) | 0.002 | 2140 (32.6) | 371 (30.2) | 0.103 |
| Type C, n (%) | 3026 (44.2) | 340 (38.2) | 0.001 | 3002 (45.8) | 494 (40.3) | <0.001 |
| Extent of CAD | ||||||
| Single-vessel, n (%) | 3827 (55.9) | 481 (54.1) | 0.313 | 3250 (49.6) | 614 (50.0) | 0.760 |
| 2-vessel, n (%) | 1925 (28.1) | 242 (27.2) | 0.606 | 1968 (30.0) | 352 (28.7) | 0.351 |
| ≥3-vessel, n (%) | 1095 (16.0) | 166 (18.7) | 0.042 | 1339 (20.4) | 261 (21.3) | 0.499 |
| Pre-PCI TIMI 0/1, n (%) | 3857 (56.3) | 544 (61.2) | 0.006 | 3966 (60.5) | 788 (64.2) | 0.014 |
| Type of stent | ||||||
| ZES, n (%) | 2219 (32.4) | 347 (39.0) | <0.001 | 2404 (36.7) | 526 (42.9) | <0.001 |
| EES, n (%) | 3335 (48.7) | 389 (43.8) | 0.005 | 3187 (48.6) | 556 (45.3) | 0.034 |
| BES, n (%) | 1161 (17.0) | 123 (13.8) | 0.019 | 944 (14.4) | 122 (9.9) | <0.001 |
| Others, n (%) | 264 (3.9) | 34 (3.8) | 0.964 | 160 (2.4) | 31 (2.5) | 0.841 |
| IVUS, n (%) | 1358 (19.8) | 169 (19.0) | 0.591 | 1321 (20.1) | 218 (17.8) | 0.056 |
| OCT, n (%) | 61 (0.9) | 7 (0.8) | 0.756 | 47 (0.7) | 7 (0.6) | 0.709 |
| FFR, n (%) | 135 (2.0) | 3 (0.3) | 0.001 | 69 (1.0) | 0 | <0.001 |
| Stent diameter (mm) | 3.16 ± 0.42 | 3.18 ± 0.43 | 0.344 | 3.16 ± 0.43 | 3.17 ± 0.43 | 0.274 |
| Stent length (mm) | 26.9 ± 11.6 | 24.1 ± 8.1 | <0.001 | 26.9 ± 11.5 | 24.7 ± 8.5 | <0.001 |
| Number of stents | 1.45 ± 0.77 | 1.40 ± 0.72 | 0.039 | 1.48 ± 0.79 | 1.40 ± 0.75 | 0.002 |
| Variables | Group A3 eGFR 30–59 mL/min/1.73 m2 (n = 2144) | Group B3 eGFR 30–59 mL/min/1.73 m2 (n = 537) | p Value | Group A4 eGFR < 30 mL/min/1.73 m2 (n = 507) | Group B4 eGFR < 30 mL/min/1.73 m2 (n = 167) | p Value |
|---|---|---|---|---|---|---|
| Male, n (%) | 1225 (57.1) | 317 (59.0) | 0.427 | 304 (60.0) | 99 (59.3) | 0.877 |
| Age (years) | 70.8 ± 10.4 | 70.8 ± 10.5 | 0.884 | 68.9 ± 10.9 | 69.8 ± 10.4 | 0.376 |
| LVEF (%) | 50.0 ± 12.3 | 48.4 ± 13.1 | 0.020 | 48.1 ± 11.9 | 44.2 ± 12.8 | 0.001 |
| BMI (kg/m2) | 23.9 ± 3.2 | 23.7 ± 3.5 | 0.414 | 23.5 ±3.4 | 23.1 ±3.4 | 0.276 |
| SBP (mmHg) | 126.6 ± 30.2 | 120.0 ± 32.1 | <0.001 | 132.2 ± 33.3 | 128.0 ± 25.8 | 0.183 |
| DBP (mmHg) | 75.7 ± 17.1 | 72.0 ± 17.5 | <0.001 | 77.4 ± 18.0 | 73.7 ± 19.6 | 0.035 |
| Cardiogenic shock, n (%) | 160 (7.5) | 58 (10.8) | 0.011 | 44 (8.7) | 25 (15.0) | 0.020 |
| CPR on admission, n (%) | 129 (6.0) | 51 (9.5) | 0.004 | 24 (4.7) | 11 (6.6) | 0.349 |
| Killip class III/IV, n (%) | 416 (19.4) | 146 (27.2) | <0.001 | 138 (27.2) | 54 (32.3) | 0.204 |
| STEMI, n (%) | 1160 (54.1) | 309 (57.5) | 0.152 | 173 (34.1) | 65 (38.9) | 0.260 |
| Primary PCI, n (%) | 1115 (96.1) | 297 (96.1) | 0.997 | 165 (95.4) | 64 (98.5) | 0.266 |
| NSTEMI, n (%) | 984 (45.9) | 228 (42.5) | 0.152 | 334 (65.9) | 102 (61.1) | 0.260 |
| PCI within 24 h | 791 (80.4) | 170 (74.6) | 0.051 | 263 (78.7) | 77 (75.5) | 0.488 |
| Hypertension, n (%) | 1489 (69.4) | 340 (63.3) | 0.006 | 412 (81.3) | 135 (80.8) | 0.903 |
| Diabetes mellitus, n (%) | 903 (42.1) | 216 (40.2) | 0.434 | 318 (62.7) | 109 (65.3) | 0.553 |
| Dyslipidemia, n (%) | 271 (12.6) | 48 (8.9) | 0.017 | 58 (11.4) | 18 (10.8) | 0.815 |
| Previous MI, n (%) | 140 (6.5) | 27 (5.0) | 0.231 | 46 (9.1) | 15 (9.0) | 0.972 |
| Previous PCI, n (%) | 215 (10.0) | 52 (9.7) | 0.872 | 72 (14.2) | 17 (10.2) | 0.235 |
| Previous CABG, n (%) | 23 (1.1) | 6 (1.0) | 0.929 | 8 (1.6) | 1 (0.6) | 0.464 |
| Previous HF, n (%) | 54 (2.5) | 19 (3.5) | 0.194 | 20 (3.9) | 11 (6.6) | 0.157 |
| Previous CVA, n (%) | 241 (11.2) | 57 (10.6) | 0.759 | 64 (12.6) | 25 (15.0) | 0.437 |
| Current smokers, n (%) | 566 (26.4) | 158 (29.4) | 0.159 | 110 (21.7) | 30 (18.0) | 0.302 |
| Peak CK-MB (mg/dL) | 103.5 ± 151.0 | 133.8 ± 201.7 | <0.001 | 70.8 ± 127.9 | 91.7 ± 144.5 | 0.076 |
| Peak troponin-I (ng/mL) | 46.4 ± 94.5 | 48.2 ± 92.3 | 0.700 | 97.1 ± 204.6 | 55.3 ± 145.3 | 0.445 |
| NT-ProBNP (pg/mL) | 3188.7 ± 5091.2 | 3802.2 ± 5998.2 | 0.016 | 9248.5 ± 8231.4 | 9948.8 ± 9432.6 | 0.589 |
| High-sensitivity CRP (mg/dL) | 8.9 ± 38.6 | 12.7 ± 47.9 | 0.093 | 10.1 ± 32.4 | 15.2 ± 48.2 | 0.209 |
| Serum creatinine (mg/L) | 1.4 ± 0.3 | 1.4 ± 0.3 | 0.074 | 5.1 ± 4.6 | 5.1 ± 3.7 | 0.965 |
| eGFR (mL/min/1.73 m2) | 49.2 ± 8.0 | 48.6 ± 8.2 | 0.130 | 16.5 ± 8.5 | 15.8 ± 8.2 | 0.305 |
| Blood glucose (mg/L) | 197.3 ± 101.1 | 207.9 ± 108.3 | 0.044 | 209.0 ± 129.7 | 217.0 ± 124.4 | 0.479 |
| Total cholesterol (mg/dL) | 177.1 ± 47.9 | 163.9 ± 41.6 | <0.001 | 162.4 ± 52.3 | 148.2 ± 45.6 | 0.001 |
| Triglyceride (mg/L) | 128.3 ± 96.9 | 113.2 ± 73.0 | <0.001 | 125.7 ± 111.3 | 117.5 ± 68.7 | 0.282 |
| HDL cholesterol (mg/L) | 42.7 ± 16.5 | 42.5 ± 17.6 | 0.828 | 39.3 ± 12.7 | 37.9 ± 14.8 | 0.302 |
| LDL cholesterol (mg/L) | 109.5 ± 46.5 | 100.7 ± 41.8 | <0.001 | 95.9 ± 38.8 | 83.9 ± 36.4 | 0.001 |
| Discharge medications, n (%) | ||||||
| Aspirin, n (%) | 2127 (99.2) | 518 (96.5) | <0.001 | 498 (98.2) | 156 (93.4) | 0.001 |
| Clopidogrel, n (%) | 1941 (90.5) | 523 (91.1) | 0.798 | 457 (90.1) | 160 (95.8) | 0.606 |
| Ticagrelor, n (%) | 145 (6.8) | 10 (1.9) | <0.001 | 35 (6.9) | 5 (3.0) | 0.087 |
| Prasugrel, n (%) | 58 (2.7) | 4 (0.7) | 0.006 | 15 (3.0) | 2 (1.2) | 0.266 |
| Cilostazole, n (%) | 434 (20.2) | 82 (15.3) | 0.008 | 97 (19.1) | 21 (12.6) | 0.060 |
| ACEIs, n (%) | 1122 (52.3) | 189 (35.2) | <0.001 | 178 (35.1) | 43 (25.7) | 0.029 |
| ARBs, n (%) | 677 (31.6) | 124 (23.1) | <0.001 | 215 (42.4) | 35 (21.0) | <0.001 |
| BBs, n (%) | 1775 (82.8) | 315 (58.7) | <0.001 | 431 (85.0) | 79 (47.3) | <0.001 |
| CCBs, n (%) | 177 (8.3) | 41 (7.6) | 0.724 | 81 (16.0) | 21 (12.6) | 0.321 |
| Statin, n (%) | ||||||
| Atorvastatin, n (%) | 1202 (56.1) | 326 (64.3) | ||||
| Rosuvastatin, n (%) | 608 (28.4) | 116 (22.9) | ||||
| Simvastatin, n (%) | 133 (6.2) | 26 (5.1) | ||||
| Pitavastatin, n (%) | 154 (7.2) | 20 (3.9) | ||||
| Pravastatin, n (%) | 40 (1.9) | 12 (2.4) | ||||
| Fluvastatin, n (%) | 7 (0.3) | 7 (1.4) | ||||
| Infarct-related artery | ||||||
| Left main, n (%) | 51 (2.4) | 16 (3.0) | 0.425 | 26 (5.1) | 8 (4.8) | 0.863 |
| LAD, n (%) | 917 (42.8) | 228 (42.4) | 0.963 | 221 (43.6) | 69 (41.3) | 0.472 |
| LCx, n (%) | 324 (15.1) | 69 (12.8) | 0.195 | 72 (14.2) | 29 (17.4) | 0.320 |
| RCA, n (%) | 852 (39.7) | 224 (41.7) | 0.404 | 188 (37.1) | 61 (36.5) | 0.927 |
| Treated vessel | ||||||
| Left main, n (%) | 82 (3.8) | 17 (3.2) | 0.524 | 32 (6.3) | 13 (7.8) | 0.508 |
| LAD, n (%) | 1175 (54.8) | 278 (51.8) | 0.207 | 298 (58.8) | 90 (53.9) | 0.268 |
| LCx, n (%) | 568 (26.5) | 127 (23.6) | 0.179 | 121 (23.9) | 41 (24.6) | 0.857 |
| RCA, n (%) | 997 (46.5) | 253 (47.1) | 0.799 | 223 (44.0) | 99 (41.3) | 0.589 |
| ACC/AHA lesion type | ||||||
| Type B1, n (%) | 303 (14.1) | 109 (20.3) | <0.001 | 72 (14.2) | 16 (9.6) | 0.145 |
| Type B2, n (%) | 720 (33.6) | 133 (24.8) | <0.001 | 174 (34.3) | 57 (34.1) | 0.965 |
| Type C, n (%) | 983 (45.8) | 224 (41.7) | 0.090 | 238 (46.9) | 83 (49.7) | 0.536 |
| Extent of CAD | ||||||
| Single-vessel, n (%) | 875 (40.8) | 211 (39.3) | 0.521 | 198 (39.1) | 63 (37.7) | 0.760 |
| 2-vessel, n (%) | 671 (31.3) | 172 (32.0) | 0.743 | 148 (29.2) | 52 (31.1) | 0.633 |
| ≥3-vessel, n (%) | 598 (27.9) | 154 (28.7) | 0.717 | 161 (31.8) | 52 (31.1) | 0.924 |
| Pre-PCI TIMI 0/1, n (%) | 1258 (58.7) | 330 (61.5) | 0.242 | 227 (44.8) | 83 (49.7) | 0.268 |
| Type of stent | ||||||
| ZES, n (%) | 801 (37.4) | 233 (43.4) | 0.010 | 167 (32.9) | 65 (38.9) | 0.158 |
| EES, n (%) | 1092 (50.9) | 245 (45.9) | 0.030 | 274 (54.0) | 79 (47.3) | 0.153 |
| BES, n (%) | 249 (11.6) | 52 (9.7) | 0.222 | 64 (12.6) | 18 (10.8) | 0.587 |
| Others, n (%) | 43 (2.0) | 12 (2.2) | 0.738 | 8 (1.6) | 7 (4.2) | 0.065 |
| IVUS, n (%) | 401 (18.7) | 85 (15.8) | 0.133 | 89 (17.6) | 30 (18.0) | 0.907 |
| OCT, n (%) | 4 (0.2) | 3 (0.6) | 0.131 | 1 (0.2) | 0 | 0.566 |
| FFR, n (%) | 5 (0.2) | 3 (0.6) | 0.216 | 2 (0.4) | 1 (0.6) | 0.575 |
| Stent diameter (mm) | 3.11 ± 0.42 | 3.11 ± 0.44 | 0.887 | 3.09 ± 0.43 | 3.11 ± 0.44 | 0.555 |
| Stent length (mm) | 27.8 ± 12.3 | 26.0 ± 11.1 | 0.002 | 29.0 ± 13.7 | 28.1 ± 14.4 | 0.497 |
| Number of stents | 1.54 ± 0.82 | 1.53 ± 0.82 | 0.648 | 1.60 ± 0.87 | 1.51 ± 0.76 | 0.196 |
| Hazard Ratio (95% CI) Unadjusted | p Value | Event Rates at 2 Years a | Hazard Ratio (95% CI) Adjusted b | p Value | |
|---|---|---|---|---|---|
| MACE | |||||
| Group A1 vs. | - | 5.2 % | - | - | |
| Group A2 | 1.228 (1.059–1.425) | 0.017 | 6.4 % | 1.139 (0.969–1.339) | 0.114 |
| Group A3 | 2.015 (1.689–2.404) | <0.001 | 10.1 % | 1.465 (1.183–1.813) | <0.001 |
| Group A4 | 3.804 (2.991–4.837) | <0.001 | 18.5 % | 2.082 (1.514–2.863) | <0.001 |
| Group A2 vs. Group A3 | 1.641 (1.383–1.946) | <0.001 | 1.249 (1.027–1.520) | 0.026 | |
| Group A2 vs. Group A4 | 3.096 (2.445–3.922) | <0.001 | 1.701 (1.263–2.290) | <0.001 | |
| Group A3 vs. Group A4 | 1.881 (1.458–2.427) | <0.001 | 1.439 (1.059–1.954) | 0.020 | |
| All-cause death | |||||
| Group A1 vs. | 0.9 % | - | |||
| Group A2 | 2.076 (1.494–2.886) | <0.001 | 1.8 % | 1.937 (1.348–2.784) | <0.001 |
| Group A3 | 5.454 (3.887–7.652) | <0.001 | 4.6 % | 3.691 (2.452–5.554) | <0.001 |
| Group A4 | 15.55 (10.71–22.56) | <0.001 | 12.9 % | 5.068 (3.037–8.459) | <0.001 |
| Group A2 vs. Group A3 | 2.625 (1.985–3.471) | <0.001 | 1.843 (1.342–2.531) | <0.001 | |
| Group A2 vs. Group A4 | 7.512 (5.457–10.34) | <0.001 | 3.160 (2.104–4.745) | <0.001 | |
| Group A3 vs. Group A4 | 2.853 (2.052–3.966) | <0.001 | 2.060 (1.396–3.039) | <0.001 | |
| Cardiac death | |||||
| Group A1 vs. | 0.4 % | - | |||
| Group A2 | 2.364 (1.504–3.714) | <0.001 | 1.0 % | 1.964 (1.215–3.177) | 0.006 |
| Group A3 | 6.001 (3.764–9.568) | <0.001 | 2.6 % | 3.429 (1.993–5.898) | <0.001 |
| Group A4 | 15.28 (9.047–25.81) | <0.001 | 6.8 % | 4.512 (2.318–8.783) | <0.001 |
| Group A2 vs. Group A3 | 2.537 (1.752–3.675) | <0.001 | 1.647 (1.087–2.495) | 0.019 | |
| Group A2 vs. Group A4 | 6.476 (4.166–10.07) | <0.001 | 2.829 (1.674–4.781) | <0.001 | |
| Group A3 vs. Group A4 | 2.540 (1.610–4.008) | <0.001 | 2.040 (1.218–3.418) | 0.007 | |
| Recurrent MI | |||||
| Group A1 vs. | 1.6 % | - | |||
| Group A2 | 1.040 (0.785–1.377) | 0.786 | 1.6 % | 1.060 (0.778–1.444) | 0.712 |
| Group A3 | 1.738 (1.244–2.429) | 0.001 | 2.8 % | 1.070 (0.708–1.616) | 0.750 |
| Group A4 | 2.658 (1.607–4.395) | <0.001 | 4.3 % | 1.486 (0.786–2.806) | 0.223 |
| Group A2 vs. Group A3 | 1.675 (1.675–2.340) | 0.002 | 1.218 (0.821–1.807) | 0.327 | |
| Group A2 vs. Group A4 | 2.556 (1.546–4.225) | <0.001 | 1.430 (0.762–2.682) | 0.265 | |
| Group A3 vs. Group A4 | 1.531 (0.897–2.614) | 0.118 | 1.192 (0.627–2.265) | 0.593 | |
| Any repeat revascularization | |||||
| Group A1 vs. | 3.4 % | ||||
| Group A2 | 1.092 (0.902–1.323) | 0.367 | 3.6 % | 1.036 (0.843–1.274) | 0.735 |
| Group A3 | 1.308 (1.013–1.689) | 0.039 | 4.3 % | 1.010 (0.743–1.372) | 0.950 |
| Group A4 | 1.582 (1.019–2.456) | 0.041 | 5.2 % | 1.161 (0.680–1.981) | 0.585 |
| Group A2 vs. Group A3 | 1.197 (0.929–1.542) | 0.164 | 1.057 (0.791–1.413) | 0.706 | |
| Group A2 vs. Group A4 | 1.442 (0.930–2.236) | 0.102 | 1.053 (0.629–1.762) | 0.845 | |
| Group A3 vs. Group A4 | 1.202 (0.751–1.924) | 0.442 | 1.019 (0.587–1.771) | 0.945 | |
| Statin Users | Statin Nonusers | ||||||
|---|---|---|---|---|---|---|---|
| Outcomes | Group A1 (n = 6847) | Group B1 (n = 889) | Log-Rank | Unadjusted | Adjusted a | ||
| HR (95% CI) | p Value | HR (95% CI) | p Value | ||||
| MACE | 320 (5.2) | 78 (9.0) | <0.001 | 1.821 (1.421–2.332) | <0.001 | 1.573 (1.181–2.096) | 0.002 |
| All-cause death | 53 (0.9) | 30 (3.4) | <0.001 | 4.235 (2.705–6.629) | <0.001 | 2.242 (1.261–3.984) | 0.006 |
| Cardiac death | 27 (0.4) | 20 (2.3) | <0.001 | 5.567 (3.121–9.929) | <0.001 | 2.956 (1.412–6.189) | 0.004 |
| Re-MI | 97 (1.6) | 19 (2.2) | 0.138 | 1.448 (0.886–2.369) | 0.140 | 1.578 (0.918–2.711) | 0.099 |
| Any revascularization | 203 (3.4) | 33 (4.0) | 0.353 | 1.190 (0.824–1.720) | 0.354 | 1.191 (0.796–1.783) | 0.395 |
| Outcomes | Group A2 (n = 6557) | Group B2 (n = 1227) | Log-Rank | Unadjusted | Adjusted b | ||
| HR (95% CI) | p Value | HR (95% CI) | p Value | ||||
| MACE | 381 (6.4) | 117 (9.7) | <0.001 | 1.573 (1.279–1.935) | <0.001 | 1.381 (1.092–1.747) | 0.007 |
| All-cause death | 107 (1.8) | 63 (5.2) | <0.001 | 3.031 (2.220–4.138) | <0.001 | 2.139 (1.471–3.110) | <0.001 |
| Cardiac death | 62 (1.0) | 48 (4.0) | <0.001 | 4.023 (2.759–5.864) | <0.001 | 2.422 (1.536–3.819) | <0.001 |
| Re-MI | 98 (1.6) | 19 (1.6) | 0.980 | 1.006 (0.616–1.645) | 0.980 | 1.199 (0.719–2.001) | 0.487 |
| Any revascularization | 215 (3.6) | 49 (4.2) | 0.345 | 1.161 (0.851–1.584) | 0.345 | 1.196 (0.856–1.671) | 0.294 |
| Outcomes | Group A3 (n = 2144) | Group B3 (n = 537) | Log-Rank | Unadjusted | Adjusted c | ||
| HR (95% CI) | p Value | HR (95% CI) | p Value | ||||
| MACE | 201 (10.1) | 90 (17.0) | <0.001 | 1.817 (1.417–2.330) | <0.001 | 1.732 (1.329–2.266) | <0.001 |
| All-cause death | 91 (4.6) | 66 (12.4) | <0.001 | 2.978 (2.169–4.088) | <0.001 | 2.510 (1.780–3.541) | <0.001 |
| Cardiac death | 51 (2.6) | 50 (9.5) | <0.001 | 4.034 (2.731–5.958) | <0.001 | 3.150 (2.069–4.795) | <0.001 |
| Re-MI | 53(2.8) | 15 (3.1) | 0.661 | 1.137 (0.641–2.017) | 0.661 | 1.311 (0.735–2.409) | 0.346 |
| Any revascularization | 83 (4.3) | 29 (6.1) | 0.111 | 1.407 (0.922–2.148) | 0.113 | 1.532 (1.018–2.428) | 0.086 |
| Outcomes | Group A4 (n = 507) | Group B4 (n = 167) | Log-Rank | Unadjusted | Adjusted d | ||
| HR (95% CI) | p Value | HR (95% CI) | p Value | ||||
| MACE | 84 (18.5) | 52 (32.2) | <0.001 | 2.009 (1.422–2.840) | <0.001 | 1.949 (1.347–2.822) | <0.001 |
| All-cause death | 58 (12.9) | 44 (27.3) | <0.001 | 2.493 (1.685–3.690) | <0.001 | 2.476 (1.629–3.755) | <0.001 |
| Cardiac death | 29 (6.8) | 30 (19.0) | <0.001 | 3.378 (2.027–5.628) | <0.001 | 3.341 (1.975–5.706) | <0.001 |
| Re-MI | 18 (4.3) | 6 (4.4) | 0.901 | 1.060 (0.421–2.672) | 0.901 | 1.065 (0.410–2.764) | 0.898 |
| Any revascularization | 22 (5.2) | 10 (7.9) | 0.293 | 1.490 (0.705–3.146) | 0.296 | 1.412 (0.639–3.118) | 0.394 |
| Variables | MACE | All-Cause Death | ||||||
|---|---|---|---|---|---|---|---|---|
| Unadjusted | Adjusted | Unadjusted | Adjusted | |||||
| HR (95% CI) | p Value | HR (95% CI) | p Value | HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Group A1 vs. Group A2 | 1.228 (1.059–1.425) | 0.017 | 1.106 (0.940–1.301) | 0.226 | 2.076 (1.494–2.886) | <0.001 | 1.146 (1.007–1.345) | 0.040 |
| Group A1 vs. Group A3 | 2.015 (1.689–2.404) | <0.001 | 1.314 (1.066–1.687) | 0.012 | 5.454 (3.887–7.652) | <0.001 | 2.365 (1.544–3.625) | <0.001 |
| Group A1 vs. Group A4 | 3.804 (2.991–4.837) | <0.001 | 1.779 (1.239–2.554) | 0.002 | 15.55 (10.71–22.56) | <0.001 | 3.807 (2.151–6.736) | <0.001 |
| Group A2 vs. Group A3 | 1.641 (1.383–1.946) | <0.001 | 1.342 (1.028–1.483) | 0.040 | 2.625 (1.985–3.471) | <0.001 | 1.510 (1.085–2.100) | 0.015 |
| Group A2 vs. Group A4 | 3.096 (2.445–3.922) | <0.001 | 1.946 (1.522–2.415) | 0.017 | 7.512 (5.457–10.34) | <0.001 | 2.175 (1.345–3.518) | 0.002 |
| Group A3 vs. Group A4 | 1.881 (1.458–2.427) | <0.001 | 1.521 (1.189–2.027) | 0.034 | 2.853 (2.052–3.966) | <0.001 | 1.797 (1.162–2.779) | 0.008 |
| Male | 1.325 (1.157–1.518) | <0.001 | 1.047 (0.888–1.235) | 0.584 | 1.587 (1.255–2.006) | <0.001 | 1.146 (1.007–1.345) | 0.040 |
| Age, ≥65 years | 1.577 (1.391–1.788) | <0.001 | 1.276 (1.094–1.488) | 0.002 | 4.502 (3.430–5.910) | <0.001 | 3.985 (2.860–5.534) | <0.001 |
| STEMI | 1.300 (1.148–1.473) | <0.001 | 1.180 (1.028–1.355) | 0.019 | 1.727 (1.377–2.166) | <0.001 | 1.425 (1.102–1.842) | 0.007 |
| LVEF, <40% | 2.031 (1.724–2.393) | <0.001 | 1.491 (1.236–1.797) | <0.001 | 3.671 (2.865–4.703) | <0.001 | 2.088 (1.557–2.800) | <0.001 |
| Cardiogenic shock | 1.431 (1.074–1.907) | <0.001 | 1.369 (1.037–1.897) | 0.005 | 2.304 (1.519–3.495) | <0.001 | 1.987 (1.269–3.231) | 0.024 |
| CPR on admission | 2.680 (2.132–3.368) | <0.001 | 2.308 (1.787–2.982) | <0.001 | 3.979 (2.822–5.610) | <0.001 | 2.842 (1.900–4.252) | <0.001 |
| Hypertension | 1.498 (1.320–1.700) | <0.001 | 1.164 (1.007–1.345) | 0.040 | 2.123 (1.676–2.678) | <0.001 | 1.390 (1.056–1.829) | 0.019 |
| Diabetes mellitus | 1.791 (1.575–2.036) | <0.001 | 1.428 (1.234–1.653) | <0.001 | 2.391 (1.911–2.991) | <0.001 | 1.524 (1.172–1.980) | 0.002 |
| Previous heart failure | 1.250 (0.690–2.266) | <0.001 | 1.613 (0.799–3.253) | 0.182 | 2.590 (1.224–5.479) | 0.013 | 1.058 (0.466–2.405) | 0.892 |
| Current smoker | 1.309 (1.150–1.489) | <0.001 | 1.022 (0.873–1.197) | 0.786 | 1.731 (1.360–2.202) | <0.001 | 1.214 (0.904–1.629) | 0.197 |
| NT-ProBNP | 1.002 (0.999–1.004) | <0.001 | 1.003 (1.000–1.005) | <0.001 | 1.001 (0.998–1.002) | <0.001 | 1.002 (0.999–1.003) | <0.001 |
| Total cholesterol | 0.997 (0.995–0.998) | <0.001 | 1.001 (0.998–1.003) | 0.637 | 0.994 (0.991–0.997) | <0.001 | 1.002 (0.998–1.007) | 0.372 |
| Triglyceride | 0.999 (0.998–1.000) | <0.001 | 0.998 (0.997–0.999) | 0.121 | 0.998 (0.996–0.999) | 0.003 | 0.999 (0.997–1.001) | 0.370 |
| HDL cholesterol | 0.990 (0.984–0.995) | <0.001 | 0.993 (0.988–1.001) | 0.245 | 0.981 (0.976–0.997) | 0.011 | 0.987 (0.975–0.999) | 0.425 |
| LDL cholesterol | 0.998 (0.996–0.999) | <0.001 | 0.999 (0.997–1.000) | 0.009 | 0.995 (0.992–0.999) | 0.005 | 0.997 (0.992–1.001) | 0.029 |
| Aspirin | 2.527 (1.491–4.283) | 0.001 | 1.083 (0.553–2.121) | 0.817 | 1.784 (1.356–2.351) | 0.010 | 1.481 (0.661–3.318) | 0.340 |
| Ticagrelor | 1.134 (0.874–1.471) | 0.344 | 1.297 (0.972–1.730) | 0.077 | 1.477 (0.877–2.486) | 0.143 | 1.826 (0.993–3.360) | 0.053 |
| Prasugrel | 1.344 (0.972–1.859) | 0.074 | 1.256 (0.890–1.771) | 0.194 | 3.224 (1.332–7.803) | 0.009 | 2.356 (0.953–5.826) | 0.063 |
| ACEI | 1.542 (1.360–1.747) | <0.001 | 1.369 (1.194–1.570) | <0.001 | 1.922 (1.532–2.411) | <0.001 | 1.613 (1.245–2.089) | <0.001 |
| BB | 1.360 (1.153–1.560) | <0.001 | 1.033 (0.856–1.245) | 0.738 | 1.547 (1.167–2.051) | 0.002 | 1.230 (0.902–1.679) | 0.191 |
| ≥3-vessel disease | 1.893 (1.656–2.164) | <0.001 | 1.572 (1.355–1.823) | <0.001 | 2.112 (1.671–2.668) | <0.001 | 1.374 (1.052–1.794) | 0.020 |
| Stent diameter <3.0 mm | 1.189 (1.039–1.361) | 0.012 | 1.038 (0.897–1.202) | 0.614 | 1.075 (0.834–1.386) | 0.575 | 1.333 (1.011–1.758) | 0.041 |
| Stent length ≥30 mm | 1.250 (1.095–1.427) | 0.001 | 1.096 (0.951–1.264) | 0.206 | 1.499 (1.190–1.889) | 0.001 | 1.263 (0.981–1.625) | 0.070 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.H.; Her, A.-Y.; Jeong, M.H.; Kim, B.-K.; Hong, S.-J.; Kim, S.; Ahn, C.-M.; Kim, J.-S.; Ko, Y.-G.; Choi, D.; et al. Efficacy of Statin Treatment According to Baseline Renal Function in Korean Patients with Acute Myocardial Infarction Not Requiring Dialysis Undergoing Newer-Generation Drug-Eluting Stent Implantation. J. Clin. Med. 2021, 10, 3504. https://doi.org/10.3390/jcm10163504
Kim YH, Her A-Y, Jeong MH, Kim B-K, Hong S-J, Kim S, Ahn C-M, Kim J-S, Ko Y-G, Choi D, et al. Efficacy of Statin Treatment According to Baseline Renal Function in Korean Patients with Acute Myocardial Infarction Not Requiring Dialysis Undergoing Newer-Generation Drug-Eluting Stent Implantation. Journal of Clinical Medicine. 2021; 10(16):3504. https://doi.org/10.3390/jcm10163504
Chicago/Turabian StyleKim, Yong Hoon, Ae-Young Her, Myung Ho Jeong, Byeong-Keuk Kim, Sung-Jin Hong, Seunghwan Kim, Chul-Min Ahn, Jung-Sun Kim, Young-Guk Ko, Donghoon Choi, and et al. 2021. "Efficacy of Statin Treatment According to Baseline Renal Function in Korean Patients with Acute Myocardial Infarction Not Requiring Dialysis Undergoing Newer-Generation Drug-Eluting Stent Implantation" Journal of Clinical Medicine 10, no. 16: 3504. https://doi.org/10.3390/jcm10163504
APA StyleKim, Y. H., Her, A.-Y., Jeong, M. H., Kim, B.-K., Hong, S.-J., Kim, S., Ahn, C.-M., Kim, J.-S., Ko, Y.-G., Choi, D., Hong, M.-K., & Jang, Y. (2021). Efficacy of Statin Treatment According to Baseline Renal Function in Korean Patients with Acute Myocardial Infarction Not Requiring Dialysis Undergoing Newer-Generation Drug-Eluting Stent Implantation. Journal of Clinical Medicine, 10(16), 3504. https://doi.org/10.3390/jcm10163504