
A Novel Method for Adjusting the Taper and Adaption of Automatic Tooth Preparations with a High-Power Femtosecond Laser

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Acquisition
2.2. Tooth Preparation
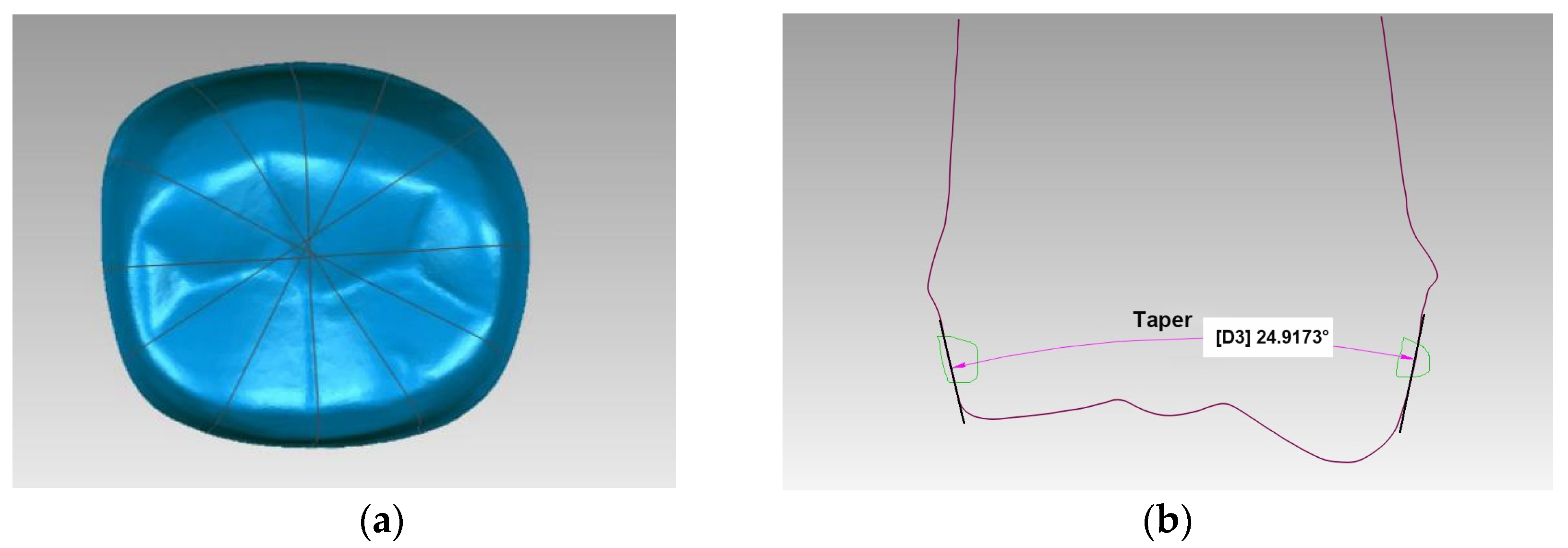
2.3. Software Measurement and Statistical Analysis
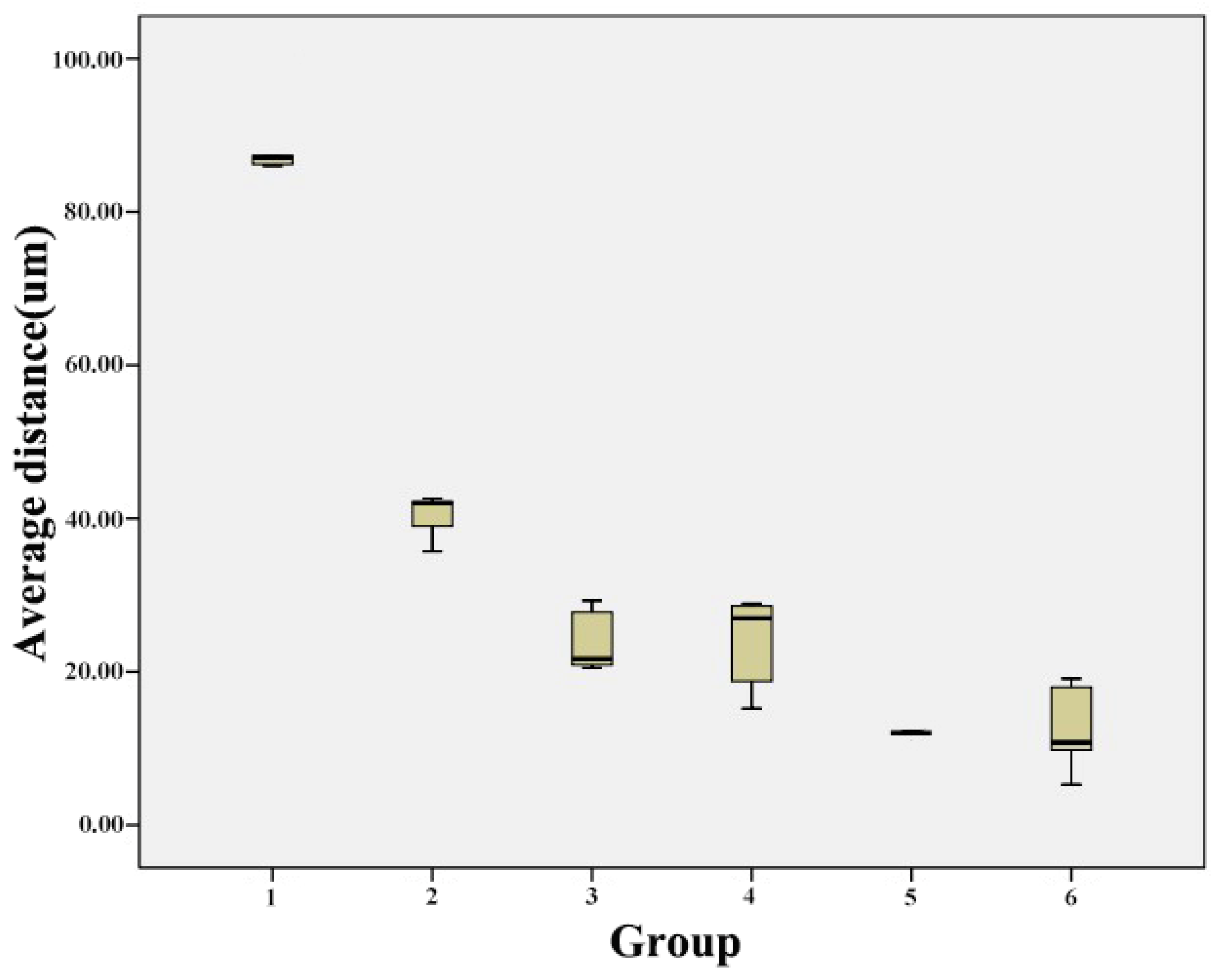
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Theodoroff, S.M.; Folmer, R.L. Hearing loss associated with long-term exposure to high-speed dental handpieces. Gen. Dent. 2015, 63, 71–76. [Google Scholar] [PubMed]
- Yamada, T.; Kuwanom, S.; Ebisu, S.; Hayashi, M. Statistical analysis for subjective and objective evaluations of dental drill sounds. PLoS ONE 2016, 11, e0159926. [Google Scholar] [CrossRef] [PubMed]
- Willershausen, B.; Callaway, A.; Wolf, T.G.; Ehlers, V.; Scholz, L.; Wolf, D.; Letzel, S. Hearing assessment in dental practitioners and other academic professionals from an urban setting. Head Face Med. 2014, 10, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, J.; Xin, X.; Zhang, F. Noise level in prosthetic practice caused by dental handpieces. Chin. J. Prosthodont. 2010, 11, 2–4. [Google Scholar]
- Banga, H.K.; Goel, P.; Kumar, R.; Kumar, V.; Kalra, P.; Singh, S.; Singh, S.; Prakash, C.; Pruncu, C. Vibration exposure and transmissibility on dentist’s anatomy: A study of micro motors and air-turbines. Int. J. Environ. Res. Public Health 2021, 18, 4084. [Google Scholar] [CrossRef]
- Raucci-Neto, W.; Raquel Dos Santos, C.; Augusto de Lima, F.; Pecora, J.D.; Bachmann, L.; Palma-Dibb, R.G. Thermal effects and morphological aspects of varying Er:YAG laser energy on demineralized dentin removal: An in vitro study. Lasers Med. Sci. 2015, 30, 1231–1236. [Google Scholar] [CrossRef]
- Melo, M.A.; Lima, J.P.; Passos, V.F.; Rodrigues, L.K. The influence of dentin demineralization on morphological features of cavities using Er:YAG laser. Photomed. Laser. Surg. 2015, 33, 22–28. [Google Scholar] [CrossRef]
- Helene, C.; Joanne, J.E.C.; Rishi, S.R.; Ritu, G.; John, N.W. The cooling efficiency of different dental high-speed handpiece coolant port designs. Heliyon 2019, 5, e02185. [Google Scholar] [CrossRef] [Green Version]
- Albatayneh, O.B.; Seow, W.K.; Walsh, L.J. Assessment of Er:YAG laser for cavity preparation in primary and permanent teeth: A scanning electron microscopy and thermographic study. Pediatr. Dent. 2014, 36, 90. [Google Scholar]
- Aminian, A.; Brunton, P.A. A comparison of the depths produced using three different tooth preparation techniques. J. Prosthet. Dent. 2003, 89, 19–22. [Google Scholar] [CrossRef]
- Leempoel, P.J.; Lemmens, P.L.; Snoek, P.A.; van’t Hof, M.A. The convergence angle of tooth preparations for complete crowns. J. Prosthet. Dent. 1987, 58, 414–416. [Google Scholar] [CrossRef]
- Chen, L.; Hua, N.; Zhang, D. Influence of preparation height and taper on the retention of complete crown. Chin. J. Dent. Mater. Dev. 2005, 14, 179–181. [Google Scholar]
- Yuan, F.; Wang, Y.; Zhang, Y.; Sun, Y.; Wang, D.; Lyu, P. An automatic tooth preparation technique: A preliminary study. Sci. Rep. 2016, 6, 25281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braun, A.; Krillke, R.F.; Frentzen, M.; Bourauel, C.; Stark, H.; Schelle, F. Heat generation caused by ablation of dental hard tissues with an ultrashort pulse laser (USPL) system. Lasers Med. Sci. 2015, 30, 475–481. [Google Scholar] [CrossRef]
- Dausinger, F.; Lubatschowski, H.; Lichtner, F. Femtosecond Technology for Technical and Medical Applications; Springer: Berlin/Heidelberg, Germany, 2004. [Google Scholar]
- Serafetinides, A.A.; Khabbaz, M.G.; Makropoulou, M.I.; Kar, A.K. Picosecond laser ablation of dentine in endodontics. Lasers Med. Sci. 1999, 14, 168–174. [Google Scholar] [CrossRef]
- Mauersberger, S.; Schille, J.; Kujawa, K.; Schneider, L.; Million, C.; Hartung, K.; Oehlert, K.; Loeschner, U. High-precision surface profiling using multi-hundred watts ultrashort pulse lasers and ultrafast polygon-mirror based scanner. J. Laser Micro Nanoeng. 2020, 15, 1–9. [Google Scholar] [CrossRef]
- Rode, A.V.; Gamaly, E.G.; Luther-Davies, B.; Taylor, B.T.; Graessel, M.; Dawes, J.M.; Chan, A.; Lowe, R.M.; Hannaford, P. Precision ablation of dental enamel using a subpicosecond pulsed laser. Aust. Dent. J. 2003, 48, 233–239. [Google Scholar] [CrossRef]
- Sun, Y.; Vorobyev, A.; Liu, J.; Guo, C.; Lyu, P. Femtosecond pulsed laser ablation of dental hard tissues with numerical control: A roughness and morphology study. Chin. J. Stomatol. 2012, 47, 486–489. [Google Scholar] [CrossRef]
- Ji, L.; Li, L.; Devlin, H.; Liu, Z.; Jiao, J.; Whitehead, D. Ti:sapphire femtosecond laser ablation of dental enamel, dentine, and cementum. Lasers. Med. Sci. 2012, 27, 197–204. [Google Scholar] [CrossRef]
- Lizarelli, R.F.Z.; Costa, M.M.; Carvalho, E.; Nunes, F.D.; Bagnato, V.S. Selective ablation of dental enamel and dentin using femtosecond laser pulses. Laser Phys. Lett. 2008, 5, 63–69. [Google Scholar] [CrossRef] [Green Version]
- Daskalova, A.; Bashir, S.; Husinsky, W. Morphology of ablation craters generated by ultra-short laser pulses in dentin surfaces: AFM and ESEM evaluation. Appl. Surf. Sci. 2010, 257, 1119–1124. [Google Scholar] [CrossRef]
- Krüger, J.; Kautek, W.; Newesely, H. Femtosecond-pulse laser ablation of dental hydroxyapatite and single-crystalline fluoroapatite. Appl. Phys. A 1999, 69, S403–S407. [Google Scholar] [CrossRef]
- Sun, Y.; Vorobyev, A.; Chen, H.; Guo, C.; Lyu, P. Study on efficiency of femtosecond laser numerical control ablation of enamel and dentin. Chin. J. Stomatol. 2013, 48, 58–59. [Google Scholar]
- Wei, D.; Cheng, P.; Chen, X.; Wu, B.; Gao, F. Study on femtosecond laser processing of nonmetal vascular stent. Laser Optoelectron. Progr. 2013, 50, 117–122. [Google Scholar]
- Cheng, P.; Wei, D.; Wu, B.; Gao, F.; Chen, X. Femtosecond laser precision machine of biodegradable heart stent. Opt. Eng. 2014, 22, 63–68. [Google Scholar]
- Wang, H.W.; Cheng, C.W.; Li, C.W.; Chang, H.W.; Wu, P.H.; Wang, G.J. Fabrication of pillared PLGA microvessel scaffold using femtosecond laser ablation. Int. J. Nanomed. 2012, 7, 1865–1873. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luengo, M.C.; Portillo, M.; Sanchez, J.M.; Peix, M.; Moreno, P.; Garcia, A.; Montero, J.; Albaladejo, A. Evaluation of micromorphological changes in tooth enamel after mechanical and ultrafast laser preparation of surface cavities. Lasers Med. Sci. 2013, 28, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Sarathkumar, L.; Soundarapandian, S.; Ravi, B.; Muthukumaraswamy, A. Surface Processing: An Elegant Way to Enhance the Femtosecond Laser Ablation Rate and Ablation Efficiency on Human Teeth. Lasers Surg. Med. 2019, 51, 797–807. [Google Scholar] [CrossRef]
- Reinhard, E.F.; Maria, Q.; Nate, J.; Peter, K.; Michael, A.; Felix, K.K.; Jozef, Z.; Martin, G.; Hartmut, S. Ablation Precision and Thermal Effects of a Picosecond Infrared Laser (PIRL) on Roots of Human Teeth: A Pilot Study Ex Vivo. In Vivo 2020, 34, 2325–2336. [Google Scholar] [CrossRef]
- Straßl, M.; Kopecek, H.; Weinrotter, M.; Bäcker, A.; Al-Janabi, A.H.; Wieger, V.; Wintner, E. Novel applications of short and ultra-short pulses. Appl. Surf. Sci. 2005, 247, 561–570. [Google Scholar] [CrossRef]
- Yuan, F.; Lv, P.; Wang, D.; Wang, L.; Sun, Y.; Wang, Y. Controlling dental enamel-cavity ablation depth with optimized stepping parameters along the focal plane normal using a three axis, numerically controlled picosecond laser. Photomed. Laser Surg. 2015, 33, 92–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stern, D.; Schoenlein, R.W.; Puliafito, C.A.; Dobi, E.T.; Birngruber, R.; Fujimoto, J.G. Corneal ablation by nanosecond, picosecond, and femtosecond lasers at 532 and 625 nm. Arch. Ophthalmol. 1989, 107, 587–592. [Google Scholar] [CrossRef]
- Elizabeth, J.K.; Jeremy, Y.; Bruce, E.B.; Mark, C.P.; Sivanandan, S.H. The role of ambient gas confinement, plasma chemistry, and focusing conditions on emission features of femtosecond laser-produced plasmas. J. Anal. At. Spectrom. 2020, 35, 1574–1586. [Google Scholar] [CrossRef]
- Lenzner, M.; Krüger, J.; Sartania, S.; Cheng, Z.; Spielmann, C.H.; Mourou, G.; Kautek, W.; Krausz, F. Femtosecond Optical Breakdown in Dielectrics. Phys. Rev. Lett. 1998, 80, 4076–4079. [Google Scholar] [CrossRef] [Green Version]
- Sallé, B.; Gobert, O.; Meynadier, P.; Perdrix, M.; Petite, G.; Semerok, A. Femtosecond and picosecond laser microablation: Ablation efficiency and laser microplasma expansion. Appl. Phys. A 1999, 69, S381–S383. [Google Scholar] [CrossRef]
- Xia, X.; Tan, F.; Wang, L.; Wu, S. Effects of different tooth preparations on three-dimensional adaption of crowns based on the reverse engineering. West China J. Stomatol. 2015, 33, 470–473. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Light-Off Delay (ms) | Mean (°) | SD (°) |
|---|---|---|---|
| 1 | 180 | 39.268 | 4.530 |
| 2 | 240 | 38.806 | 2.888 |
| 3 | 300 | 33.652 | 2.257 |
| 4 | 360 | 32.476 | 1.553 |
| 5 | 420 | 31.159 | 2.078 |
| 6 | 480 | 25.393 | 5.496 |
| Group | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|
| 1 | 0.749 | 0.000 | 0.000 | 0.000 | 0.000 |
| 2 | - | 0.001 | 0.000 | 0.000 | 0.000 |
| 3 | - | - | 0.416 | 0.087 | 0.000 |
| 4 | - | - | - | 0.363 | 0.000 |
| 5 | - | - | - | - | 0.000 |
| Group | Light-off Delay (ms) | Mean (μm) | SD (μm) |
|---|---|---|---|
| 1 | 180 | 0.089 | 0.005 |
| 2 | 240 | 0.040 | 0.003 |
| 3 | 300 | 0.024 | 0.042 |
| 4 | 360 | 0.024 | 0.006 |
| 5 | 420 | 0.013 | 0.025 |
| 6 | 480 | 0.013 | 0.030 |
| Group | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|
| 1 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 |
| 2 | - | 0.000 | 0.000 | 0.000 | 0.000 |
| 3 | - | - | 0.911 | 0.001 | 0.001 |
| 4 | - | - | - | 0.001 | 0.001 |
| 5 | - | - | - | - | 0.932 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yuan, F.; Liang, S.; Lyu, P. A Novel Method for Adjusting the Taper and Adaption of Automatic Tooth Preparations with a High-Power Femtosecond Laser. J. Clin. Med. 2021, 10, 3389. https://doi.org/10.3390/jcm10153389
Yuan F, Liang S, Lyu P. A Novel Method for Adjusting the Taper and Adaption of Automatic Tooth Preparations with a High-Power Femtosecond Laser. Journal of Clinical Medicine. 2021; 10(15):3389. https://doi.org/10.3390/jcm10153389
Chicago/Turabian StyleYuan, Fusong, Shanshan Liang, and Peijun Lyu. 2021. "A Novel Method for Adjusting the Taper and Adaption of Automatic Tooth Preparations with a High-Power Femtosecond Laser" Journal of Clinical Medicine 10, no. 15: 3389. https://doi.org/10.3390/jcm10153389
APA StyleYuan, F., Liang, S., & Lyu, P. (2021). A Novel Method for Adjusting the Taper and Adaption of Automatic Tooth Preparations with a High-Power Femtosecond Laser. Journal of Clinical Medicine, 10(15), 3389. https://doi.org/10.3390/jcm10153389