
Impact of Diabetes Mellitus on Cervical Spine Surgery for Ossification of the Posterior Longitudinal Ligament

 , , ,
, , ,  , ,
, ,  ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Surgical Procedures
2.3. Functional Measurements
2.4. Postoperative Complications
2.5. Imaging Studies
2.6. Preoperative Glycemic Control and Treatment Modalities of DM
2.7. Statistical Analysis
3. Results
3.1. Patients’ Characteristics and Baseline Functions
3.2. Postoperative Complications
3.3. Functional Outcomes
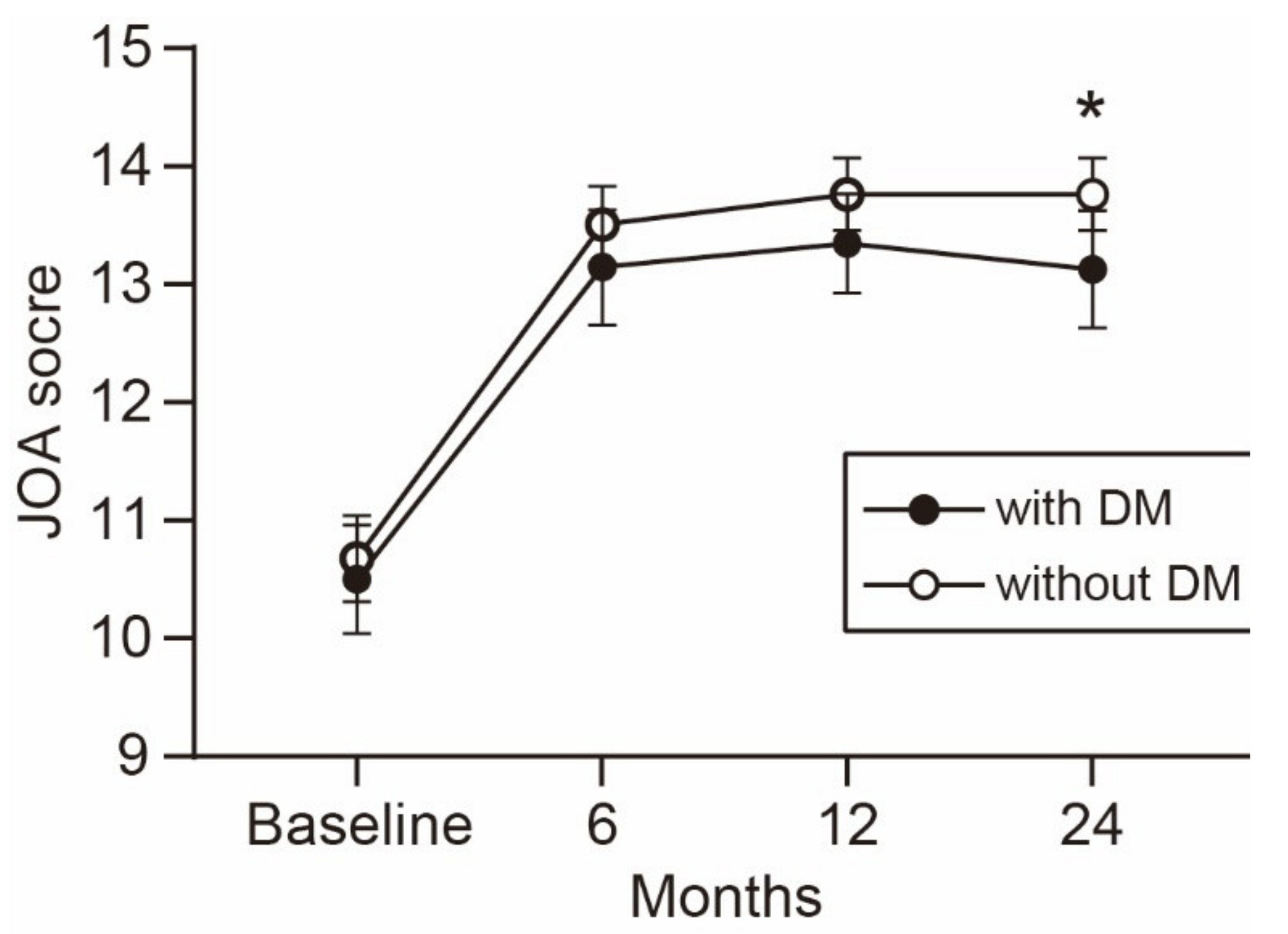
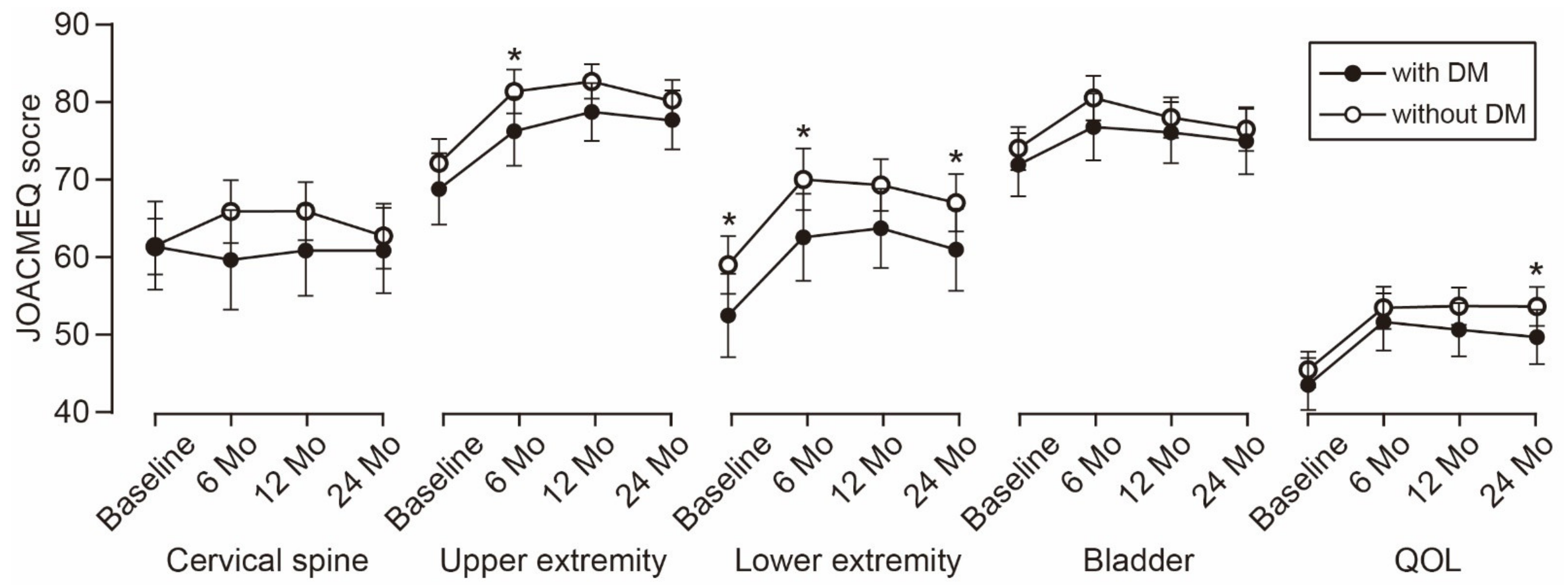
3.4. Time-Dependent Change of Functional Outcomes
3.5. Surgical Outcomes Stratified by Surgical Procedures
3.6. Surgical Outcomes Stratified by Treatment Modalities for DM
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Matsunaga, S.; Sakou, T. Ossification of the posterior longitudinal ligament of the cervical spine: Etiology and natural history. Spine 2012, 37, E309–E314. [Google Scholar] [CrossRef]
- Xiao, B.; Nagoshi, N.; Takeuchi, A.; Mao, J.; Liu, B.; Tian, W.; Tsuji, O.; Okada, E.; Fujita, N.; Yagi, M.; et al. Imaging Comparison Between Chinese and Japanese Patients With Cervical Ossification of the Posterior Longitudinal Ligament. Spine 2018, 43, E1376–E1383. [Google Scholar] [CrossRef]
- Hirai, T.; Yoshii, T.; Ushio, S.; Hashimoto, J.; Mori, K.; Maki, S.; Katsumi, K.; Nagoshi, N.; Takeuchi, K.; Furuya, T.; et al. Associations between Clinical Symptoms and Degree of Ossification in Patients with Cervical Ossification of the Posterior Longitudinal Ligament: A Prospective Multi-Institutional Cross-Sectional Study. J. Clin. Med. 2020, 9, 4055. [Google Scholar] [CrossRef]
- Abiola, R.; Rubery, P.; Mesfin, A. Ossification of the Posterior Longitudinal Ligament: Etiology, Diagnosis, and Outcomes of Nonoperative and Operative Management. Glob. Spine J. 2016, 6, 195–204. [Google Scholar] [CrossRef]
- Bakhsh, W.; Saleh, A.; Yokogawa, N.; Gruber, J.; Rubery, P.T.; Mesfin, A. Cervical Ossification of the Posterior Longitudinal Ligament: A Computed Tomography-Based Epidemiological Study of 2917 Patients. Glob. Spine J. 2019, 9, 820–825. [Google Scholar] [CrossRef] [Green Version]
- Nakashima, H.; Tetreault, L.; Nagoshi, N.; Nouri, A.; Arnold, P.; Yukawa, Y.; Toyone, T.; Tanaka, M.; Zhou, Q.; Fehlings, M.G. Comparison of Outcomes of Surgical Treatment for Ossification of the Posterior Longitudinal Ligament Versus Other Forms of Degenerative Cervical Myelopathy: Results from the Prospective, Multicenter AOSpine CSM-International Study of 479 Patients. J. Bone Jt. Surg. Am. 2016, 98, 370–378. [Google Scholar] [CrossRef]
- Nagoshi, N.; Tetreault, L.A.; Nakashima, H.; Nouri, A.; Arnold, P.; Zileli, M.; Tan, G.; Kopjar, B.; Fehlings, M.G. Do Caucasians and East Asians have Different Outcomes Following Surgery for the Treatment of Degenerative Cervical Myelopathy?: Results From the Prospective Multicenter AOSpine International Study. Spine 2016, 41, 1428–1435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akune, T.; Ogata, N.; Seichi, A.; Ohnishi, I.; Nakamura, K.; Kawaguchi, H. Insulin secretory response is positively associated with the extent of ossification of the posterior longitudinal ligament of the spine. J. Bone Jt. Surg. Am. 2001, 83, 1537–1544. [Google Scholar] [CrossRef] [PubMed]
- Kobashi, G.; Washio, M.; Okamoto, K.; Sasaki, S.; Yokoyama, T.; Miyake, Y.; Sakamoto, N.; Ohta, K.; Inaba, Y.; Tanaka, H.; et al. High body mass index after age 20 and diabetes mellitus are independent risk factors for ossification of the posterior longitudinal ligament of the spine in Japanese subjects: A case-control study in multiple hospitals. Spine 2004, 29, 1006–1010. [Google Scholar] [CrossRef] [PubMed]
- Creager, M.A.; Luscher, T.F.; Cosentino, F.; Beckman, J.A. Diabetes and vascular disease: Pathophysiology, clinical consequences, and medical therapy: Part I. Circulation 2003, 108, 1527–1532. [Google Scholar] [CrossRef] [Green Version]
- Epstein, N.E. Predominantly negative impact of diabetes on spinal surgery: A review and recommendation for better preoperative screening. Surg. Neurol. Int. 2017, 8, 107. [Google Scholar] [CrossRef]
- Machino, M.; Yukawa, Y.; Ito, K.; Inoue, T.; Kobayakawa, A.; Matsumoto, T.; Ouchida, J.; Tomita, K.; Kato, F. Impact of diabetes on the outcomes of cervical laminoplasty: A prospective cohort study of more than 500 patients with cervical spondylotic myelopathy. Spine 2014, 39, 220–227. [Google Scholar] [CrossRef] [PubMed]
- Nori, S.; Nagoshi, N.; Yoshioka, K.; Nojiri, K.; Takahashi, Y.; Fukuda, K.; Ikegami, T.; Yoshida, H.; Iga, T.; Tsuji, O.; et al. Diabetes Does Not Adversely Affect Neurological Recovery and Reduction of Neck Pain After Posterior Decompression Surgery for Cervical Spondylotic Myelopathy: Results from a Retrospective Multicenter Study of 675 Patients. Spine 2020, 46, 433–439. [Google Scholar] [CrossRef]
- Choi, S.; Lee, S.H.; Lee, J.Y.; Choi, W.G.; Choi, W.C.; Choi, G.; Jung, B.; Lee, S.C. Factors affecting prognosis of patients who underwent corpectomy and fusion for treatment of cervical ossification of the posterior longitudinal ligament: Analysis of 47 patients. J. Spinal Disord. Tech. 2005, 18, 309–314. [Google Scholar] [CrossRef]
- Yoshii, T.; Morishita, S.; Inose, H.; Yuasa, M.; Hirai, T.; Okawa, A.; Fushimi, K.; Fujiwara, T. Comparison of Perioperative Complications in Anterior Decompression With Fusion and Posterior Decompression With Fusion for Cervical Ossification of the Posterior Longitudinal Ligament: Propensity Score Matching Analysis Using a Nation-Wide Inpatient Database. Spine 2020, 45, E1006–E1012. [Google Scholar]
- Yonenobu, K.; Abumi, K.; Nagata, K.; Taketomi, E.; Ueyama, K. Interobserver and intraobserver reliability of the japanese orthopaedic association scoring system for evaluation of cervical compression myelopathy. Spine 2001, 26, 1890–1894, discussion 1895. [Google Scholar] [CrossRef] [PubMed]
- Fukui, M.; Chiba, K.; Kawakami, M.; Kikuchi, S.; Konno, S.; Miyamoto, M.; Seichi, A.; Shimamura, T.; Shirado, O.; Taguchi, T.; et al. An outcome measure for patients with cervical myelopathy: Japanese Orthopaedic Association Cervical Myelopathy Evaluation Questionnaire (JOACMEQ): Part 1. J. Orthop. Sci. 2007, 12, 227–240. [Google Scholar] [CrossRef] [Green Version]
- Cheung, P.W.H.; Wong, C.K.H.; Lau, S.T.; Cheung, J.P.Y. Psychometric Validation of the Adapted Traditional Chinese (Hong Kong) Version of the Japanese Orthopaedic Association Cervical Myelopathy Evaluation Questionnaire (JOACMEQ). Spine 2018, 43, E242–E249. [Google Scholar] [CrossRef] [PubMed]
- Fujiyoshi, T.; Yamazaki, M.; Kawabe, J.; Endo, T.; Furuya, T.; Koda, M.; Okawa, A.; Takahashi, K.; Konishi, H. A new concept for making decisions regarding the surgical approach for cervical ossification of the posterior longitudinal ligament: The K-line. Spine 2008, 33, E990–E993. [Google Scholar] [CrossRef] [PubMed]
- Charvat, H.; Goto, A.; Goto, M.; Inoue, M.; Heianza, Y.; Arase, Y.; Sone, H.; Nakagami, T.; Song, X.; Qiao, Q.; et al. Impact of population aging on trends in diabetes prevalence: A meta-regression analysis of 160,000 Japanese adults. J. Diabetes Investig. 2015, 6, 533–542. [Google Scholar] [CrossRef]
- Zanella, M.T.; Kohlmann, O., Jr.; Ribeiro, A.B. Treatment of obesity hypertension and diabetes syndrome. Hypertension 2001, 38 Pt 2, 705–708. [Google Scholar] [CrossRef] [Green Version]
- Berbudi, A.; Rahmadika, N.; Tjahjadi, A.I.; Ruslami, R. Type 2 Diabetes and its Impact on the Immune System. Curr. Diabetes Rev. 2020, 16, 442–449. [Google Scholar] [CrossRef]
- Armaghani, S.J.; Archer, K.R.; Rolfe, R.; Demaio, D.N.; Devin, C.J. Diabetes Is Related to Worse Patient-Reported Outcomes at Two Years Following Spine Surgery. J. Bone Jt. Surg. Am. 2016, 98, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Arnold, P.M.; Fehlings, M.G.; Kopjar, B.; Yoon, S.T.; Massicotte, E.M.; Vaccaro, A.R.; Brodke, D.S.; Shaffrey, C.I.; Smith, J.S.; Woodard, E.J.; et al. Mild diabetes is not a contraindication for surgical decompression in cervical spondylotic myelopathy: Results of the AOSpine North America multicenter prospective study (CSM). Spine J. 2014, 14, 65–72. [Google Scholar] [CrossRef]
- Sayer, A.A.; Dennison, E.M.; Syddall, H.E.; Gilbody, H.J.; Phillips, D.I.; Cooper, C. Type 2 diabetes, muscle strength, and impaired physical function: The tip of the iceberg? Diabetes Care 2005, 28, 2541–2542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, E.; Backholer, K.; Gearon, E.; Harding, J.; Freak-Poli, R.; Stevenson, C.; Peeters, A. Diabetes and risk of physical disability in adults: A systematic review and meta-analysis. Lancet Diabetes Endocrinol. 2013, 1, 106–114. [Google Scholar] [CrossRef] [Green Version]
- Nagoshi, N.; Watanabe, K.; Nakamura, M.; Matsumoto, M.; Li, N.; Ma, S.; He, D.; Tian, W.; Jeon, H.; Lee, J.J.; et al. Does Diabetes Affect the Surgical Outcomes in Cases With Cervical Ossification of the Posterior Longitudinal Ligament? A Multicenter Study from Asia Pacific Spine Study Group. Glob. Spine J. 2021. [Google Scholar] [CrossRef] [PubMed]
- Yoshii, T.; Sakai, K.; Hirai, T.; Yamada, T.; Inose, H.; Kato, T.; Enomoto, M.; Tomizawa, S.; Kawabata, S.; Arai, Y.; et al. Anterior decompression with fusion versus posterior decompression with fusion for massive cervical ossification of the posterior longitudinal ligament with a >/=50% canal occupying ratio: A multicenter retrospective study. Spine J. 2016, 16, 1351–1357. [Google Scholar] [CrossRef]
- Mullins, J.; Pojskic, M.; Boop, F.A.; Arnautovic, K.I. Retrospective single-surgeon study of 1123 consecutive cases of anterior cervical discectomy and fusion: A comparison of clinical outcome parameters, complication rates, and costs between outpatient and inpatient surgery groups, with a literature review. J. Neurosurg. Spine 2018, 28, 630–641. [Google Scholar] [CrossRef] [Green Version]
- Guzman, J.Z.; Skovrlj, B.; Shin, J.; Hecht, A.C.; Qureshi, S.A.; Iatridis, J.C.; Cho, S.K. The impact of diabetes mellitus on patients undergoing degenerative cervical spine surgery. Spine 2014, 39, 1656–1665. [Google Scholar] [CrossRef] [Green Version]
- Shin, J.I.; Phan, K.; Kothari, P.; Kim, J.S.; Guzman, J.Z.; Cho, S.K. Impact of Glycemic Control on Morbidity and Mortality in Adult Idiopathic Scoliosis Patients Undergoing Spinal Fusion. Clin. Spine Surg. 2017, 30, E974–E980. [Google Scholar] [CrossRef] [PubMed]
- Spina, N.T.; Aleem, I.S.; Nassr, A.; Lawrence, B.D. Surgical Site Infections in Spine Surgery: Preoperative Prevention Strategies to Minimize Risk. Glob. Spine J. 2018, 8, 31S–36S. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Characteristics | With DM (N = 127) | Without DM (N = 275) | p Value * |
|---|---|---|---|
| Age | 64.2 ± 11.0 | 64.0 ± 11.9 | 0.743 |
| Gender (Male/Female) | 90/37 | 208/67 | 0.328 |
| BMI | 26.5 ± 4.5 | 25.3 ± 4.3 | 0.006 |
| Medical comorbidities | |||
| Hypertension | 59 (46) | 94 (34) | 0.021 |
| Cerebral infarction | 11 (9) | 10 (4) | 0.051 |
| Myocardial infarction | 8 (6) | 6 (2) | 0.044 |
| Musculoskeletal disease | 18(14) | 31 (11) | 0.416 |
| Connective tissue disease | 1 (0.8) | 3 (1.1) | 1.000 |
| Anticoagulant/antiplatelet medication | 26 (20) | 34 (12) | 0.049 |
| Duration of symptoms (month) | 46.7 ± 62.3 | 41.4 ± 66.0 | 0.189 |
| JOA score | 10.5 ± 2.6 | 10.7 ± 3.0 | 0.341 |
| JOACMEQ | |||
| Cervical spine | 60.8 ± 31.2 | 61.5 ± 28.7 | 0.944 |
| Upper extremity | 68.8 ± 25.2 | 72.6± 24.3 | 0.126 |
| Lower extremity | 52.4 ± 29.4 | 59.4 ± 29.4 | 0.019 |
| Bladder | 71.5 ± 23.6 | 72.9 ± 22.2 | 0.430 |
| QOL | 42.5 ± 19.8 | 44.4 ± 18.3 | 0.179 |
| Neck pain VAS | 47.6 ± 32.3 | 39.8 ± 30.7 | 0.035 |
| Imaging finding | |||
| C2-C7 Cobb angle (degree) | 8.6 ± 12.9 | 10.1 ± 10.5 | 0.258 |
| Range of motion (degree) | 24.7 ± 12.4 | 28.1 ± 14.4 | 0.051 |
| Occupancy ratio of OPLL (%) | 45.7 ± 15.6 | 43.3 ± 15.3 | 0.173 |
| K-line (−) | 42 (33) | 93 (34) | 0.883 |
| Surgical method | |||
| ADF | 21 (17) | 68 (25) | 0.071 |
| 39 (31) | 52 (19) | 0.010 | |
| LP | 63 (50) | 148 (54) | 0.453 |
| APF | 4 (3) | 7 (3) | 0.748 |
| No. of surgical levels | 4 (3–5) | 4 (3–4) | 0.029 |
| Complication | With DM (N = 127) | Without DM (N = 275) | p Value * |
|---|---|---|---|
| Early (≤30 days from surgery) | |||
| Neurological deterioration | 12 (9) | 30 (11) | 0.727 |
| CSF leakage | 6 (5) | 14 (5) | 1.000 |
| Dysphasia | 3 (2) | 8 (3) | 1.000 |
| Graft bone failure | 3 (2) | 5 (2) | 0.712 |
| Instrument failure | 2 (1.6) | 5 (2) | 1.000 |
| Wound infection | 2 (1.6) | 4 (1.5) | 1.000 |
| Wound dehiscence | 2 (1.6) | 2 (0.7) | 0.594 |
| Epidural hematoma | 1 (0.8) | 1 (0.4) | 0.533 |
| Upper air way obstruction | 1 (0.8) | 1 (0.4) | 0.533 |
| Urinary tract infection | 6 (5) | 3 (1) | 0.031 |
| Delirium | 4 (3) | 5 (2) | 0.472 |
| Deep vein thrombosis | 1 (0.8) | 2 (0.7) | 1.000 |
| Gastrointestinal bleeding | 0 (0) | 3 (1) | 0.555 |
| Heart failure | 1 (0.8) | 1 (0.4) | 0.533 |
| Liver dysfunction | 1 (0.8) | 1 (0.4) | 0.533 |
| Brain infarction | 0 (0) | 1 (0.4) | 1.000 |
| Pneumonia | 0 (0) | 1 (0.4) | 1.000 |
| Cholecystitis | 1 (0.8) | 0 (0) | 0.316 |
| Any early complications | 43 (34) | 66 (24) | 0.041 |
| Late (>30 days from surgery) | |||
| Instrument failure | 6 (5) | 5 (2) | 0.109 |
| Lumbar spinal stenosis | 3 (2) | 8 (3) | 1.000 |
| Adjacent segment disease | 2 (1.6) | 1 (0.4) | 0.236 |
| Thoracic OPLL | 1 (0.8) | 1 (0.4) | 0.533 |
| C5 palsy | 1 (0.8) | 1 (0.4) | 0.528 |
| Non-union | 0 (0) | 2 (0.7) | 1.000 |
| Wound infection | 0 (0) | 2 (0.7) | 1.000 |
| Dysphasia | 2 (1.6) | 0 (0) | 0.099 |
| Stroke | 2 (1.6) | 0 (0) | 0.099 |
| Urinary tract infection | 2 (1.6) | 1 (0.4) | 0.236 |
| Pneumonia | 2 (1.6) | 0 (0) | 0.099 |
| Parkinson’s disease | 0 (0) | 2 (0.7) | 1.000 |
| Multiple sclerosis | 0 (0) | 1 (0.4) | 1.000 |
| Any late complications | 19 (15) | 21 (8) | 0.031 |
| Outcome | With DM (N = 127) | Without DM (N = 275) | p Value * |
|---|---|---|---|
| JOA score | 13.1 ± 2.8 | 13.8 ± 2.5 | 0.024 |
| JOACMEQ | |||
| Cervical spine | 60.7 ± 20.1 | 62.8 ± 32.1 | 0.389 |
| Upper extremity | 77.9 ± 20.0 | 81.1 ± 19.5 | 0.105 |
| Lower extremity | 61.0 ± 28.1 | 67.7 ± 28.1 | 0.026 |
| Bladder | 75.1 ± 22.4 | 77.1 ± 21.3 | 0.369 |
| QOL | 49.6 ± 18.7 | 54.1 ± 19.2 | 0.036 |
| Neck pain VAS | 40.6 ± 31.1 | 36.0 ± 30.0 | 0.197 |
| Outcome | With DM (N = 127) | Without DM (N = 275) | p Value * |
|---|---|---|---|
| Recovery rate of JOA score | 40.8 ± 33.6 | 48.7 ± 32.5 | 0.051 |
| Postoperative gain in JOA score | 2.6 ± 2.4 | 3.1 ± 2.5 | 0.151 |
| Postoperative gain in JOACMEQ | |||
| Cervical spine | −3.1 ± 29.2 | 1.6 ± 34.1 | 0.230 |
| Upper extremity | 6.4 ± 23.1 | 8.4 ± 22.1 | 0.251 |
| Lower extremity | 6.2 ± 24.5 | 7.6 ± 24.2 | 0.826 |
| Bladder | 0.9 ± 20.7 | 3.0 ± 19.8 | 0.639 |
| QOL | 4.9 ± 16.7 | 9.3 ± 18.9 | 0.094 |
| Postoperative change in neck pain VAS | −5.8 ± 32.6 | −3.2 ± 33.7 | 0.625 |
| Surgical Procedure | p Value | ||||
|---|---|---|---|---|---|
| ADF (N = 89) | LP (N = 211) | PDF (N = 91) | APF (N = 11) | ||
| No. of levels decompressed | 3 | 4 | 5 | 4 | <0.001 * |
| No. of levels fused | 3 | N/A | 5 | 4 | <0.001 * |
| Preoperative JOA score | 10.9 ± 2.6 | 10.9 ± 2.7 | 9.7 ± 3.3 | 9.5 ± 3.2 | 0.002 * |
| Postoperative JOA score | 14.1 ± 2.4 | 13.7 ± 2.4 | 12.9 ± 3.1 | 12.7 ± 2.7 | 0.010 * |
| Recovery rate of JOA score | 53.1 ± 31.1 | 44.3 ± 33.7 | 44.9 ± 33.1 | 38.7 ± 30.4 | 0.157 * |
| Early complication | 34 (38) | 38 (18) | 34 (37) | 3 (27) | <0.001 † |
| Late complication | 12 (13) | 15 (7) | 13 (14) | 0 (0) | 0.067 † |
| Treatment Modality | p Value | |||
|---|---|---|---|---|
| Dietary Control (N = 32) | Oral Antidiabetics (N = 78) | Insulin Therapy (N = 17) | ||
| Preoperative HbA1c | 6.7 ± 1.3 | 6.7 ± 0.8 | 7.7 ± 1.1 | <0.001 * |
| Preoperative JOA score | 10.7 ± 3.3 | 10.5 ± 2.2 | 10.2 ± 3.1 | 0.788 * |
| Postoperative JOA score | 13.3 ± 3.5 | 13.1 ± 2.6 | 13.2 ± 2.7 | 0.917 * |
| Recovery rate of JOA score | 42.6 ± 29.0 | 38.6 ± 36.9 | 47.6 ± 25.3 | 0.576 * |
| Early (≤30 days from surgery) complications | 10 (31) | 29 (38) | 5 (24) | 0.518 † |
| Late (>30 days from surgery) complication | 2 (6) | 16 (21) | 1 (6) | 0.086 † |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kimura, A.; Takeshita, K.; Yoshii, T.; Egawa, S.; Hirai, T.; Sakai, K.; Kusano, K.; Nakagawa, Y.; Wada, K.; Katsumi, K.; et al. Impact of Diabetes Mellitus on Cervical Spine Surgery for Ossification of the Posterior Longitudinal Ligament. J. Clin. Med. 2021, 10, 3375. https://doi.org/10.3390/jcm10153375
Kimura A, Takeshita K, Yoshii T, Egawa S, Hirai T, Sakai K, Kusano K, Nakagawa Y, Wada K, Katsumi K, et al. Impact of Diabetes Mellitus on Cervical Spine Surgery for Ossification of the Posterior Longitudinal Ligament. Journal of Clinical Medicine. 2021; 10(15):3375. https://doi.org/10.3390/jcm10153375
Chicago/Turabian StyleKimura, Atsushi, Katsushi Takeshita, Toshitaka Yoshii, Satoru Egawa, Takashi Hirai, Kenichiro Sakai, Kazuo Kusano, Yukihiro Nakagawa, Kanichiro Wada, Keiichi Katsumi, and et al. 2021. "Impact of Diabetes Mellitus on Cervical Spine Surgery for Ossification of the Posterior Longitudinal Ligament" Journal of Clinical Medicine 10, no. 15: 3375. https://doi.org/10.3390/jcm10153375
APA StyleKimura, A., Takeshita, K., Yoshii, T., Egawa, S., Hirai, T., Sakai, K., Kusano, K., Nakagawa, Y., Wada, K., Katsumi, K., Fujii, K., Furuya, T., Nagoshi, N., Kanchiku, T., Nagamoto, Y., Oshima, Y., Nakashima, H., Ando, K., Takahata, M., ... Okawa, A. (2021). Impact of Diabetes Mellitus on Cervical Spine Surgery for Ossification of the Posterior Longitudinal Ligament. Journal of Clinical Medicine, 10(15), 3375. https://doi.org/10.3390/jcm10153375