
Prevalence Trend and Disparities in Rheumatoid Arthritis among US Adults, 2005–2018


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source and Study Population
2.2. Variables
2.3. Statistical Analyses
3. Results
3.1. Analytic Sample
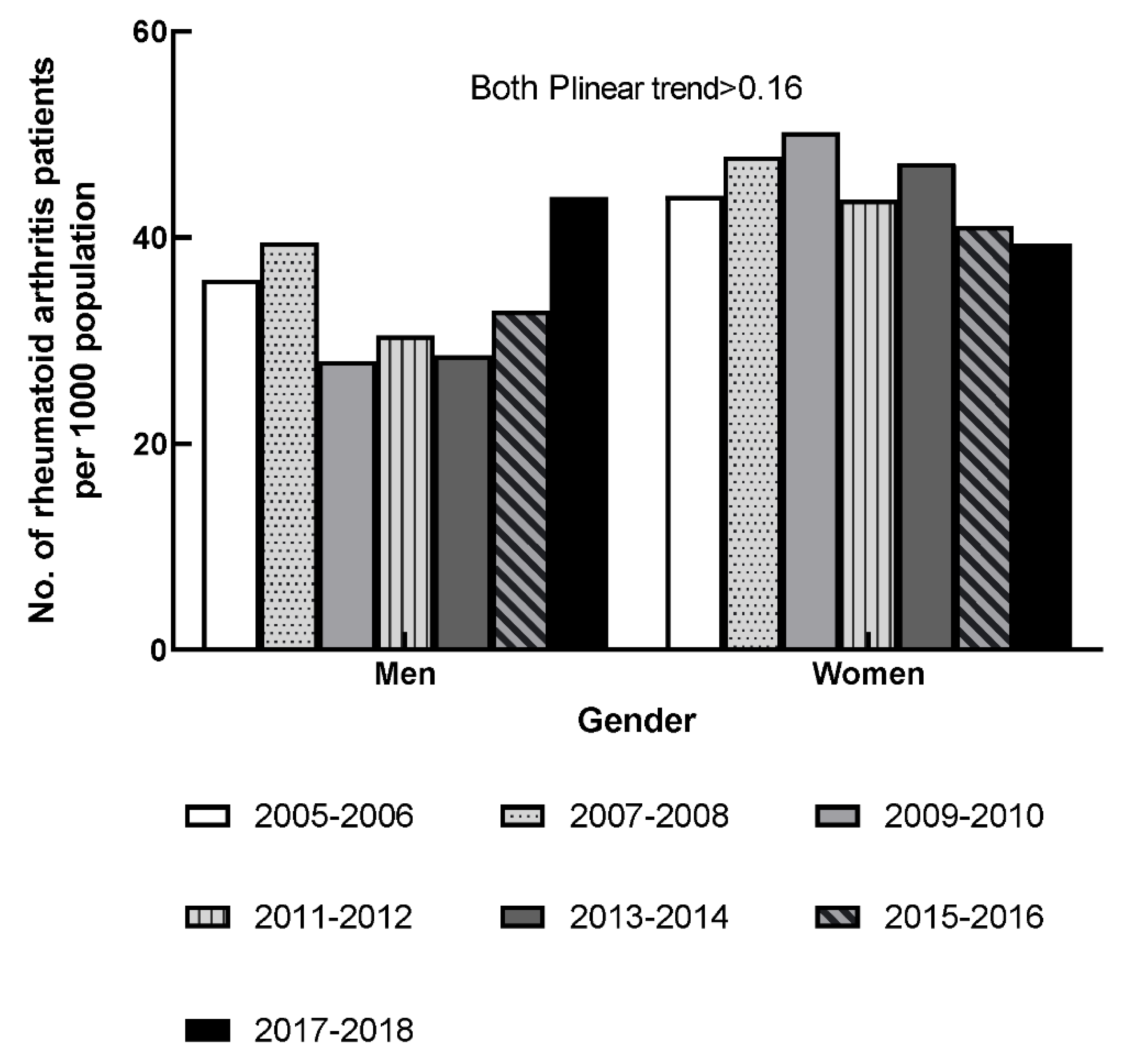
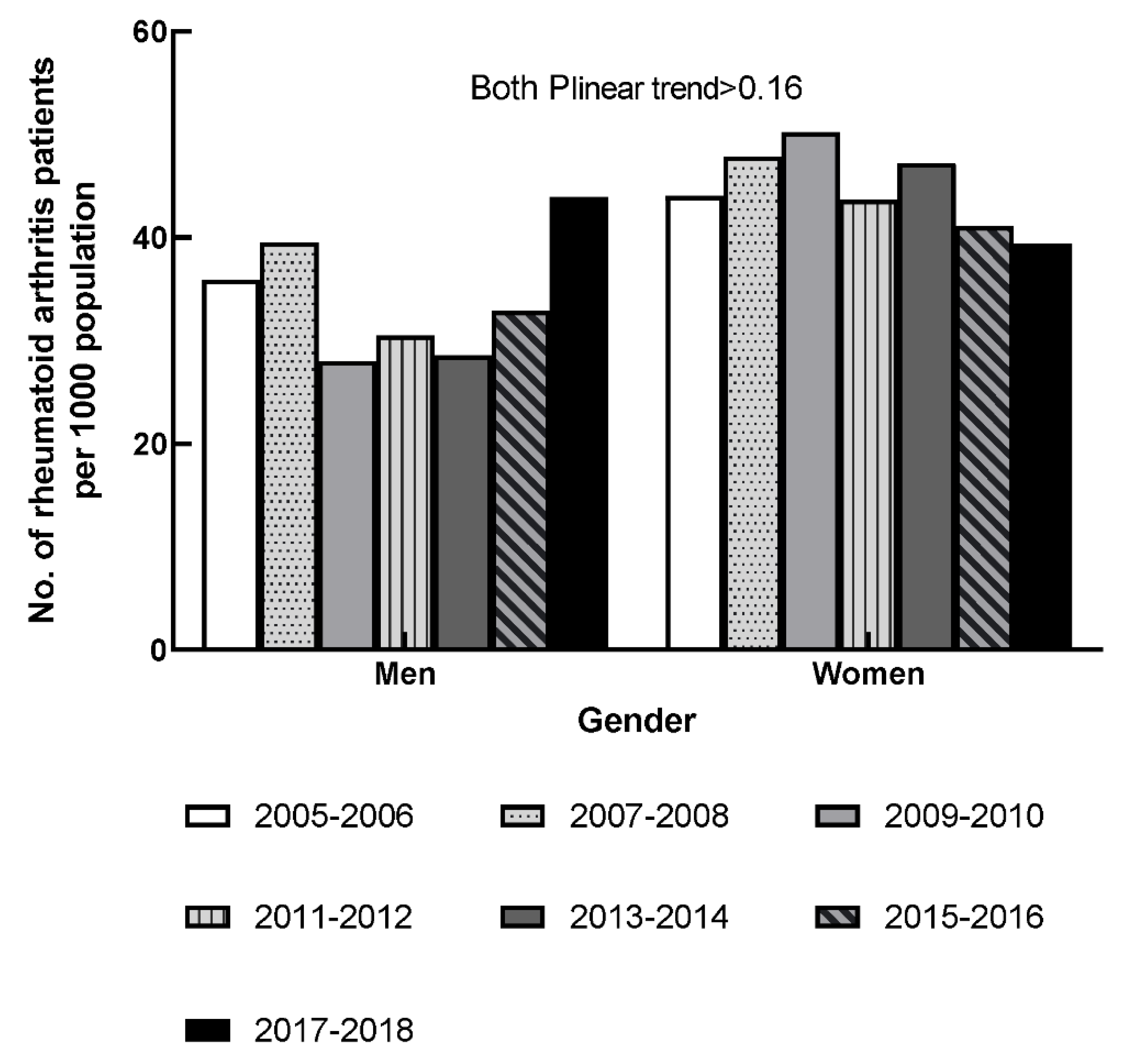
3.2. RA Prevalence in Both Genders
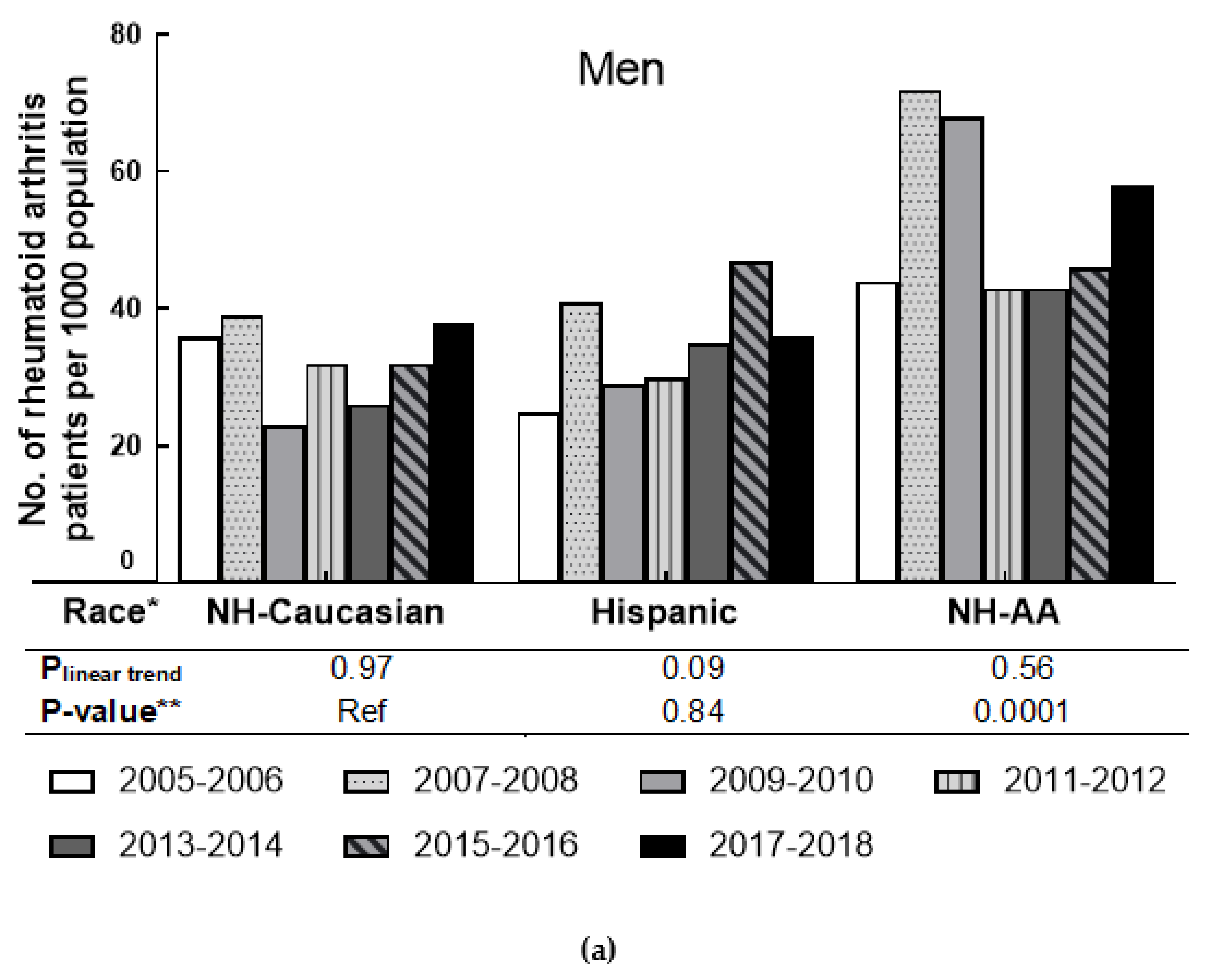
3.3. RA Prevalence by Race in Men and Women
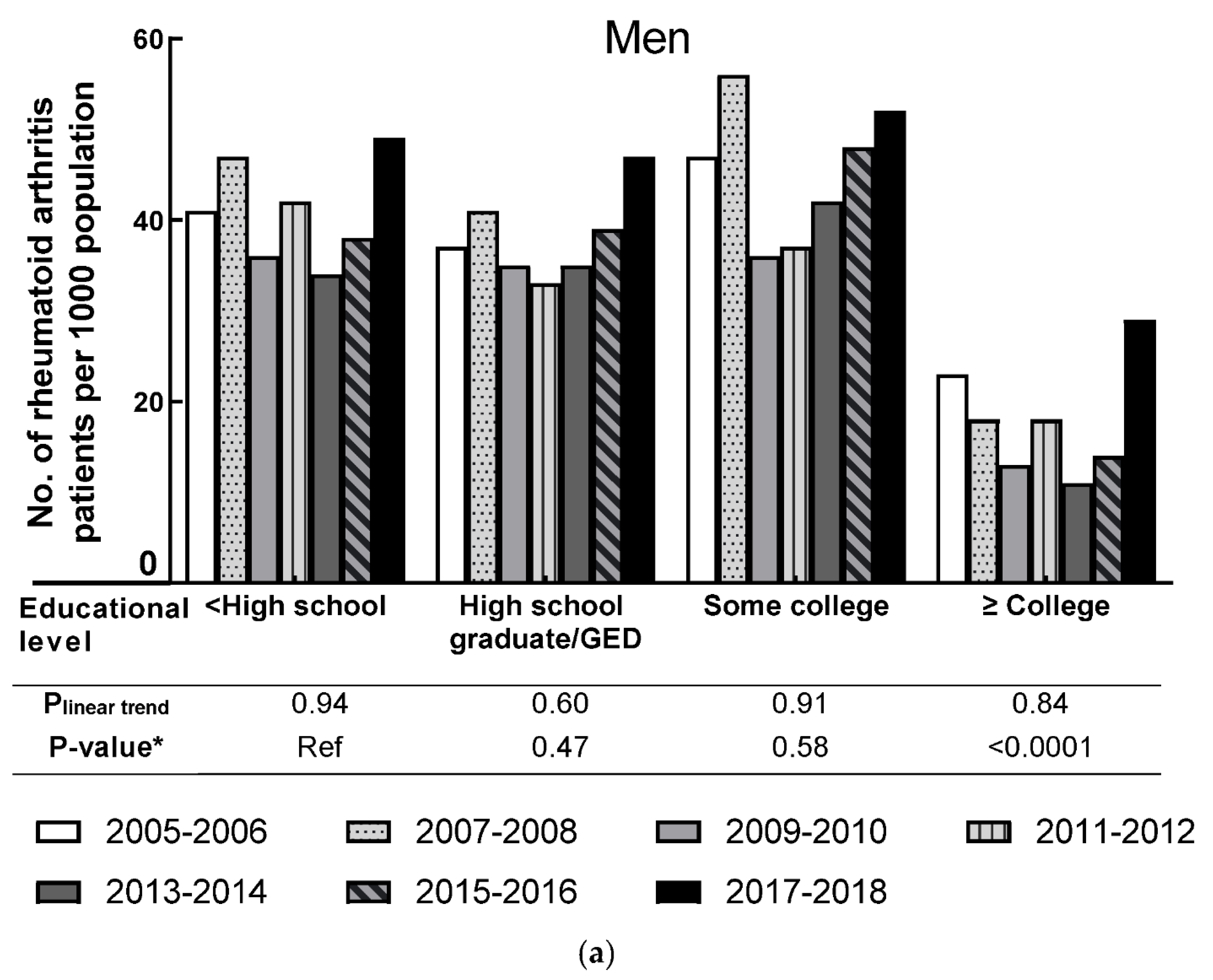
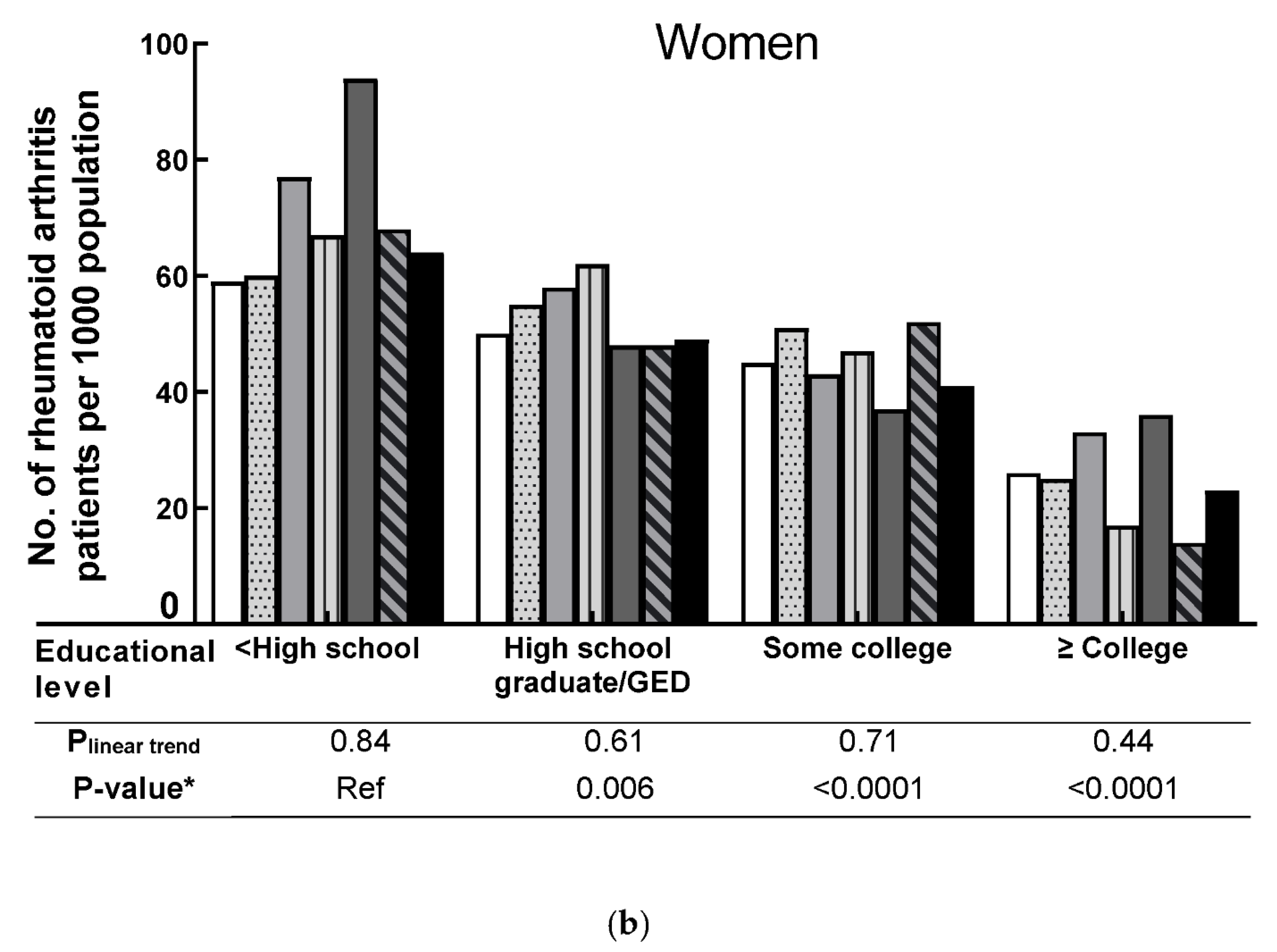
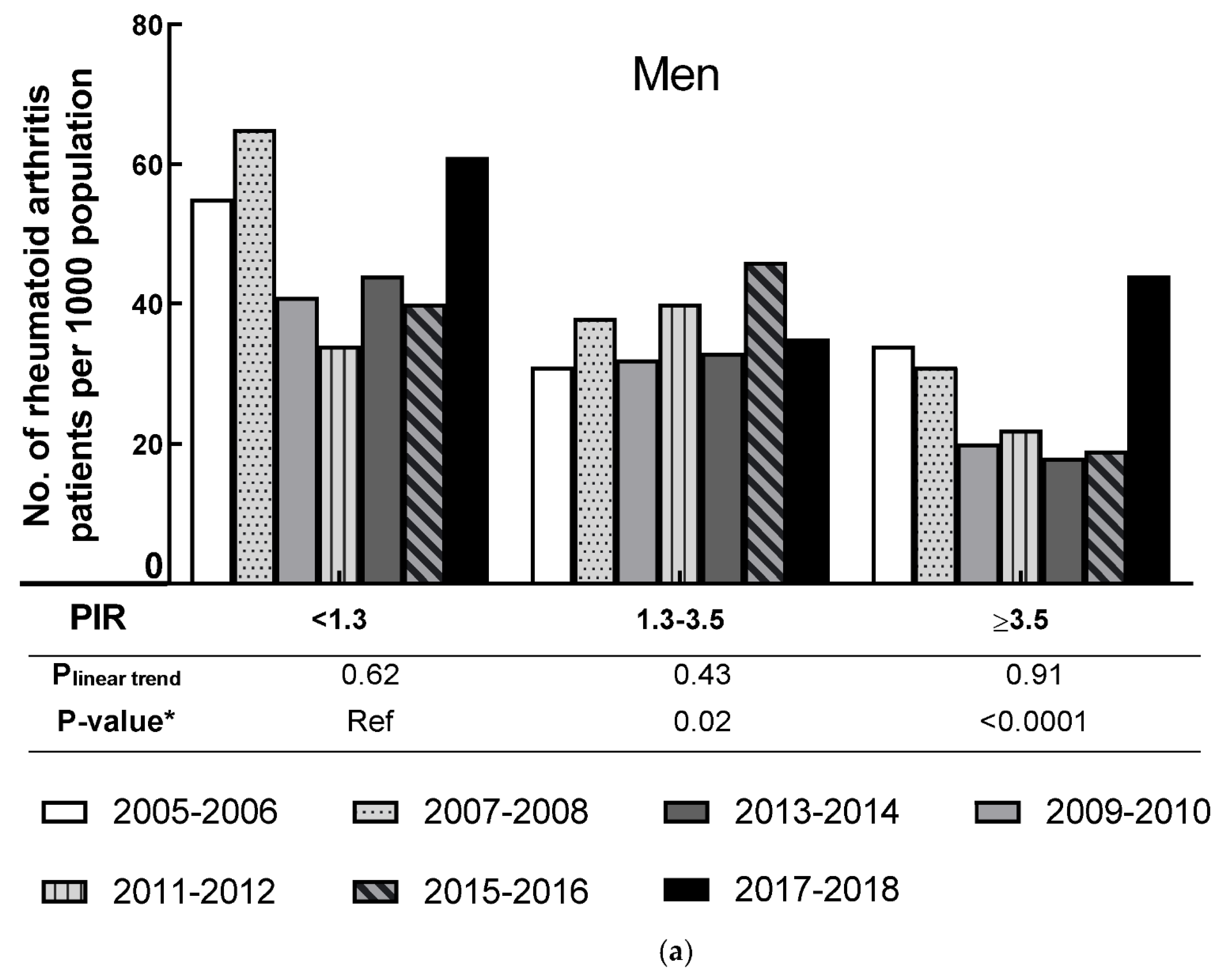
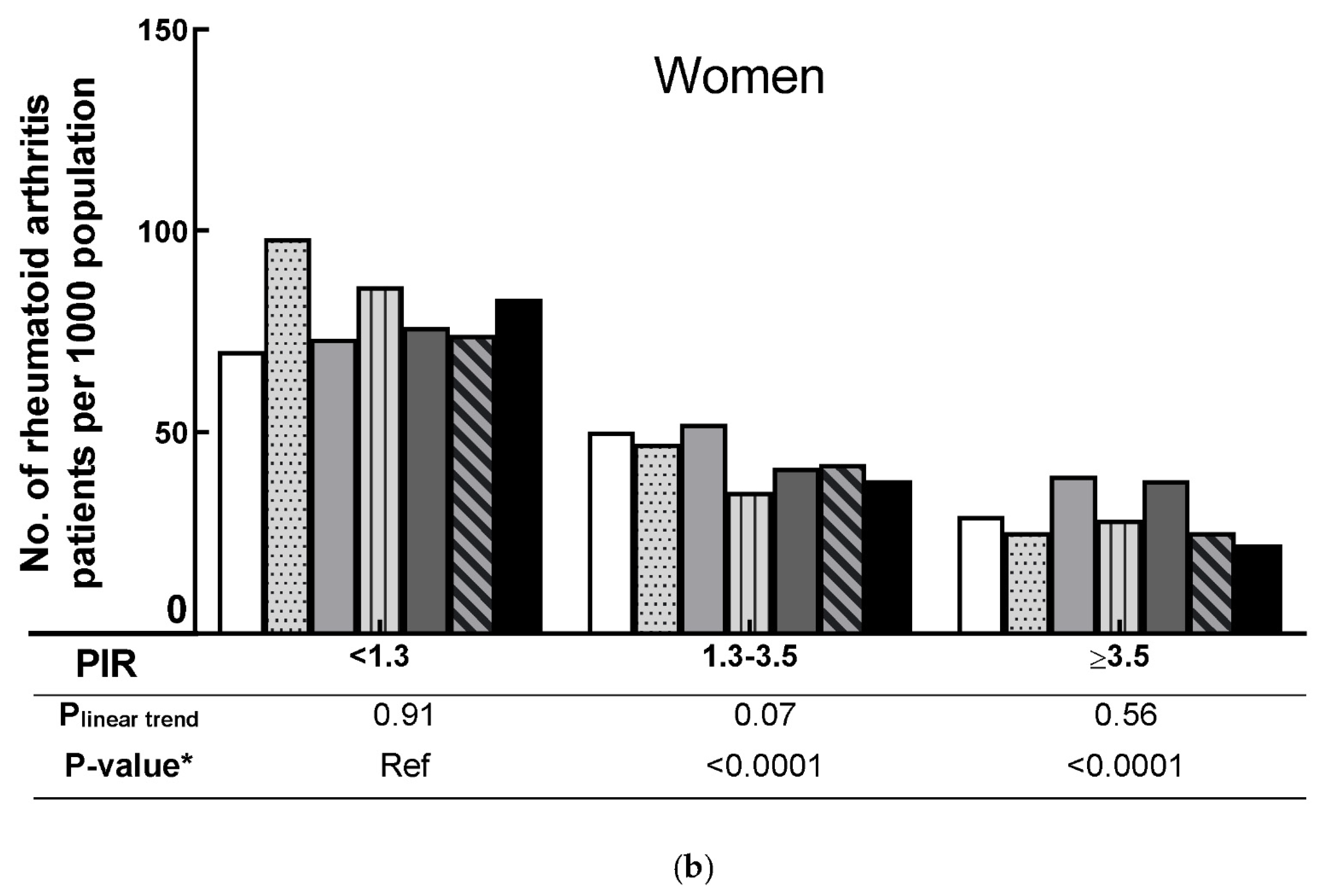
3.4. RA Prevalence by SES in Men and Women
3.5. RA Prevalence by Weight Status in Different Racial Groups, and the Association between Race, SES, and RA
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aletaha, D.; Smolen, J.S. Diagnosis and Management of Rheumatoid Arthritis: A Review. JAMA 2018, 320, 1360–1372. [Google Scholar] [CrossRef]
- Chopra, A.; Abdel-Nasser, A. Epidemiology of rheumatic musculoskeletal disorders in the developing world. Best Pr. Res. Clin. Rheumatol. 2008, 22, 583–604. [Google Scholar] [CrossRef]
- Cross, M.; Smith, E.; Hoy, D.; Carmona, L.; Wolfe, F.; Vos, T.; Williams, B.; Gabriel, S.; Lassere, M.; Johns, N.; et al. The global burden of rheumatoid arthritis: Estimates from the Global Burden of Disease 2010 study. Ann. Rheum. Dis. 2014, 73, 1316–1322. [Google Scholar] [CrossRef]
- Agarwal, S.K. Core Management Principles in Rheumatoid Arthritis to Help Guide Managed Care Professionals. J. Manag. Care Pharm. 2011, 17, S03–S08. [Google Scholar] [CrossRef] [Green Version]
- Helmick, C.G.; Felson, D.T.; Lawrence, R.C.; Gabriel, S.; Hirsch, R.; Kwoh, C.K.; Liang, M.H.; Kremers, H.M.; Mayes, M.D.; Merkel, P.A.; et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States: Part I. Arthritis Rheum. 2008, 58, 15–25. [Google Scholar] [CrossRef]
- Allaire, S.; Wolfe, F.; Niu, J.; LaValley, M.P. Contemporary prevalence and incidence of work disability associated with rheumatoid arthritis in the US. Arthritis Rheum. 2008, 59, 474–480. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Mendy, A.; Vieira, E.R. Various Types of Arthritis in the United States: Prevalence and Age-Related Trends From 1999 to 2014. Am. J. Public Health 2018, 108, 256–258. [Google Scholar] [CrossRef]
- Hunter, T.M.; Boytsov, N.N.; Zhang, X.; Schroeder, K.; Michaud, K.; Araujo, A.B. Prevalence of rheumatoid arthritis in the United States adult population in healthcare claims databases, 2004–2014. Rheumatol. Int. 2017, 37, 1551–1557. [Google Scholar] [CrossRef]
- Mackie, S.L.; Taylor, J.C.; Twigg, S.; Martin, S.G.; Steer, S.; Worthington, J.; Barton, A.; Wilson, A.G.; Hocking, L.; Young, A.; et al. Relationship between area-level socio-economic deprivation and autoantibody status in patients with rheumatoid arthritis: Multicentre cross-sectional study. Ann. Rheum. Dis. 2012, 71, 1640–1645. [Google Scholar] [CrossRef] [PubMed]
- Verstappen, S.M.M. The impact of socio-economic status in rheumatoid arthritis. Rheumatology 2017, 56, 1051–1052. [Google Scholar] [CrossRef] [Green Version]
- Curtin, L.R.; Mohadjer, L.K.; Dohrmann, S.M.; Montaquila, J.M.; Kruszan-Moran, D.; Mirel, L.B.; Carroll, M.D.; Hirsch, R.; Schober, S.; Johnson, C.L. The National Health and Nutrition Examination Survey: Sample Design, 1999–2006. Vital Health Stat. Ser. 2 Data Eval. Methods Res. 2012, 2, 1–39. [Google Scholar]
- Zipf, G.; Chiappa, M.; Porter, K.S.; Ostchega, Y.; Lewis, B.G.; Dostal, J. National Health and Nutrition Examination Survey: Plan and operations, 1999–2010. Vital Health Stat. 1 2013, 56, 1–37. [Google Scholar]
- Busija, L.; Buchbinder, R.; Osborne, R.H. Quantifying the impact of transient joint symptoms, chronic joint symptoms, and arthritis: A population-based approach. Arthritis Rheum. 2009, 61, 1312–1321. [Google Scholar] [CrossRef]
- Badley, E.M.; Ansari, H. Arthritis and arthritis-attributable activity limitations in the United States and Canada: A cross-border comparison. Arthritis Care Res. 2010, 62, 308–315. [Google Scholar] [CrossRef] [PubMed]
- Dominick, K.L.; Golightly, Y.M.; Jackson, G.L. Arthritis prevalence and symptoms among US non-veterans, veterans, and veterans receiving Department of Veterans Affairs Healthcare. J. Rheumatol. 2006, 33, 348–354. [Google Scholar]
- Borrell, L.N.; Dallo, F.J.; White, K. Education and Diabetes in a Racially and Ethnically Diverse Population. Am. J. Public Health 2006, 96, 1637–1642. [Google Scholar] [CrossRef]
- Sabanayagam, C.; Shankar, A. Income Is a Stronger Predictor of Mortality than Education in a National Sample of US Adults. J. Health Popul. Nutr. 2012, 30, 82–86. [Google Scholar] [CrossRef] [Green Version]
- Ogden, C.L.; Carroll, M.D.; Fakhouri, T.H.; Hales, C.M.; Fryar, C.D.; Li, X.; Freedman, D.S. Prevalence of Obesity Among Youths by Household Income and Education Level of Head of Household—United States 2011–2014. MMWR. Morb. Mortal. Wkly. Rep. 2018, 67, 186–189. [Google Scholar] [CrossRef]
- Deane, K.D.; Demoruelle, M.K.; Kelmenson, L.B.; Kuhn, K.A.; Norris, J.M.; Holers, V.M. Genetic and environmental risk factors for rheumatoid arthritis. Best Pr. Res. Clin. Rheumatol. 2017, 31, 3–18. [Google Scholar] [CrossRef]
- Flegal, K.M.; Kruszon-Moran, D.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Trends in Obesity Among Adults in the United States, 2005 to 2014. JAMA 2016, 315, 2284–2291. [Google Scholar] [CrossRef] [Green Version]
- NHLBI Obesity Education Initiative Expert Panel. Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults: The Evidence Report; National Heart, Lung, and Blood Institute: Bethesda, MD, USA, 1998. [Google Scholar]
- Kahende, J.W.; Adhikari, B.; Maurice, E.; Rock, V.; Malarcher, A. Disparities in Health Care Utilization by Smoking Status—NHANES 1999–2004. Int. J. Environ. Res. Public Health 2009, 6, 1095–1106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klein, R.J.; Schoenborn, C.A. Age Adjustment Using the 2000 Projected US Population; Healthy People 2010 Statistical Notes; Centers for Disease Control and Prevention/National Center for Health Statistics: Hyattsville, MD, USA, 2001. [Google Scholar]
- Kawatkar, A.A.; Portugal, C.; Li, C.; Iyer, R. Racial/Ethnic Trends in Incidence and Prevalence of Rheumatoid Arthritis in a Large Multi-Ethnic Managed Care Population. In Proceedings of the 2012 ACR/ARHP Annual Meeting, Washington, DC, USA, 9–14 November 2012. [Google Scholar]
- Semega, J.; Kollar, M.; Shrider, E.A.; Creamer, J.F. Income and Poverty in the United States: 2019; Census Bureau: Suitland-Silver Hill, MD, USA, 2020; pp. 60–270. [Google Scholar]
- Noonan, A.S.; Velasco-Mondragon, H.E.; Wagner, F.A. Improving the health of African Americans in the USA: An overdue opportunity for social justice. Public Health Rev. 2016, 37, 1–20. [Google Scholar] [CrossRef] [Green Version]
- American Psychological Association Working Group on Stress and Health Disparities. Stress and Health Disparities: Contexts, Mechanisms, and Interventions among Racial/Ethnic Minority and Low-Socioeconomic Status Populations; American Psychological Association (APA): Washington, DC, USA, 2017. [Google Scholar]
- Cutolo, M.; Straub, R.H. Stress as a Risk Factor in the Pathogenesis of Rheumatoid Arthritis. Neuroimmunomodulation 2006, 13, 277–282. [Google Scholar] [CrossRef]
- MacGregor, A.J.; Snieder, H.; Rigby, A.S.; Koskenvuo, M.; Kaprio, J.; Aho, K.; Silman, A.J. Characterizing the quantitative genetic contribution to rheumatoid arthritis using data from twins. Arthritis Rheum. 2000, 43, 30–37. [Google Scholar] [CrossRef]
- Raychaudhuri, S.; Sandor, C.; Stahl, E.A.; Freudenberg, J.; Lee, H.S.; Jia, X.; Alfredsson, L.; Padyukov, L.; Klareskog, L.; Worthington, J.; et al. Five amino acids in three HLA proteins explain most of the association between MHC and seropositive rheumatoid arthritis. Nat. Genet. 2012, 44, 291–296. [Google Scholar] [CrossRef]
- Viatte, S.; Plant, D.; Han, B.; Fu, B.; Yarwood, A.; Thomson, W.; Symmons, D.P.; Worthington, J.; Young, A.; Hyrich, K.L.; et al. Association of HLA-DRB1 Haplotypes With Rheumatoid Arthritis Severity, Mortality, and Treatment Response. JAMA 2015, 313, 1645–1656. [Google Scholar] [CrossRef]
- Hughes, L.B.; Morrison, D.; Kelley, J.M.; Padilla, M.A.; Vaughan, L.K.; Westfall, A.O.; Dwivedi, H.; Mikuls, T.R.; Holers, V.M.; Parrish, L.A.; et al. The HLA–DRB1 shared epitope is associated with susceptibility to rheumatoid arthritis in African Americans through European genetic admixture. Arthritis Rheum. 2008, 58, 349–358. [Google Scholar] [CrossRef] [Green Version]
- Reynolds, R.J.; Ahmed, A.F.; Danila, M.I.; Hughes, L.B.; Gregersen, P.K.; Raychaudhuri, S.; Plenge, R.M.; Bridges, S.L., Jr. HLA-DRB1-Associated Rheumatoid Arthritis Risk at Multiple Levels in African Americans: Hierarchical Classification Systems, Amino Acid Positions, and Residues. Arthritis Rheumatol. 2014, 66, 3274–3282. [Google Scholar] [CrossRef] [Green Version]
- Siahpush, M.; Singh, G.K.; Jones, P.R.; Timsina, L.R. Racial/ethnic and socioeconomic variations in duration of smoking: Results from 2003, 2006 and 2007 Tobacco Use Supplement of the Current Population Survey. J. Public Health 2010, 32, 210–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ward, Z.J.; Bleich, S.N.; Cradock, A.L.; Barrett, J.L.; Giles, C.M.; Flax, C.; Long, M.W.; Gortmaker, S.L. Projected U.S. State-Level Prevalence of Adult Obesity and Severe Obesity. N. Engl. J. Med. 2019, 381, 2440–2450. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.; Yang, S.M.; Kim, S.H.; Han, K.H.; Park, S.J.; Shin, J.I. Smoking and Rheumatoid Arthritis. Int. J. Mol. Sci. 2014, 15, 22279–22295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalpakcioglu, B.; Senel, K. The interrelation of glutathione reductase, catalase, glutathione peroxidase, superoxide dismutase, and glucose-6-phosphate in the pathogenesis of rheumatoid arthritis. Clin. Rheumatol. 2008, 27, 141–145. [Google Scholar] [CrossRef] [PubMed]
- Bracke, K.; Cataldo, D.; Maes, T.; Gueders, M.; Noël, A.; Foidart, J.M.; Brusselle, G.; Pauwels, R.A. Matrix Metalloproteinase-12 and Cathepsin D Expression in Pulmonary Macrophages and Dendritic Cells of Cigarette Smoke-Exposed Mice. Int. Arch. Allergy Immunol. 2005, 138, 169–179. [Google Scholar] [CrossRef]
- Liu, Y.; Aryee, M.J.; Padyukov, L.; Fallin, M.D.; Hesselberg, E.; Runarsson, A.; Reinius, L.; Acevedo, N.; Taub, M.; Ronninger, M.; et al. Epigenome-wide association data implicate DNA methylation as an intermediary of genetic risk in rheumatoid arthritis. Nat. Biotechnol. 2013, 31, 142–147. [Google Scholar] [CrossRef]
- Zeilinger, S.; Kühnel, B.; Klopp, N.; Baurecht, H.; Kleinschmidt, A.; Gieger, C.; Weidinger, S.; Lattka, E.; Adamski, J.; Peters, A.; et al. Tobacco Smoking Leads to Extensive Genome-Wide Changes in DNA Methylation. PLoS ONE 2013, 8, e63812. [Google Scholar] [CrossRef] [PubMed]
- Viatte, S.; Plant, D.; Raychaudhuri, S. Genetics and epigenetics of rheumatoid arthritis. Nat. Rev. Rheumatol. 2013, 9, 141–153. [Google Scholar] [CrossRef]
- Trayhurn, P.; Wood, I.S. Signalling role of adipose tissue: Adipokines and inflammation in obesity. Biochem. Soc. Trans. 2005, 33, 1078–1081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soriano-Guillén, L.; Hernández-García, B.; Pita, J.; Domínguez-Garrido, N.; Del Río-Camacho, G.; Rovira, A. High-sensitivity C-reactive protein is a good marker of cardiovascular risk in obese children and adolescents. Eur. J. Endocrinol. 2008, 159, R1–R4. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. FAQs-Self-Reported Case Definitions. Available online: https://www.cdc.gov/arthritis/data_statistics/faqs.htm (accessed on 19 July 2020).
- Centers for Disease Control and Prevention. Arthritis. Available online: https://www.cdc.gov/arthritis/basics/osteoarthritis.htm (accessed on 28 July 2020).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 2005–2006 (n = 4459) | 2007–2008 (n = 5084) | 2009–2010 (n = 5399) | 2011–2012 (n = 4801) | 2013–2014 (n = 5094) | 2015–2016 (n = 4846) | 2017–2018 (n = 4488) | |
|---|---|---|---|---|---|---|---|
| Age, mean (SD) | 46.20 (0.75) | 46.51 (0.43) | 46.84 (0.51) | 47.04 (0.88) | 47.38 (0.38) | 47.59 (0.57) | 48.10 (0.65) |
| Women, unweighted No. (Weighted %) | 2326 (51.94) | 2585 (51.82) | 2785 (51.96) | 2442 (51.82) | 2661 (51.82) | 2518 (52.17) | 2320 (51.77) |
| Race, unweighted No. (Weighted %) | |||||||
| Hispanic a | 1012 (11.05) | 1388 (12.73) | 1439 (12.72) | 944 (13.90) | 1072 (13.89) | 1447 (14.69) | 954 (14.48) |
| NH-Caucasian | 2240 (72.13) | 2436 (70.23) | 2691 (69.54) | 1822 (67.47) | 2240(66.75) | 1647 (65.16) | 1637 (64.27) |
| NH-African American | 1026 (11.51) | 1052 (11.04) | 975 (11.11) | 1243 (11.08) | 1048 (11.36) | 1010 (11.00) | 1019 (10.83) |
| NH-Other | 181(5.31) | 208 (6.00) | 294 (6.63) | 792 (7.55) | 734 (8.00) | 742 (9.15) | 878 (10.42) |
| Education level, unweighted No. (Weighted %) | |||||||
| <high school | 1205 (17.28) | 1545 (20.16) | 1474 (18.31) | 1082 (15.80) | 1049 (14.66) | 1099 (13.76) | 829 (10.40) |
| High school graduate/GED or equivalent | 1065 (24.92) | 1250 (25.07) | 1242 (22.79) | 1002 (19.87) | 1141 (21.74) | 1058 (20.72) | 1081 (27.25) |
| Some college | 1283 (31.40) | 1318 (29.01) | 1544 (30.52) | 1470 (32.32) | 1601 (33.12) | 1459 (32.60) | 1480 (31.22) |
| ≥college | 906 (26.40) | 971 (25.76) | 1139 (28.38) | 1247 (32.01) | 1303 (30.48) | 1230 (32.92) | 1098 (31.13) |
| PIR, unweighted No. (Weighted %) | |||||||
| <1.3 | 1166 (17.18) | 1551 (20.50) | 1813 (21.68) | 1724 (24.85) | 1759 (24.79) | 1567 (21.00) | 1274 (20.06) |
| 1.3–3.5 | 1757 (37.85) | 1979 (35.01) | 2023 (36.49) | 1629 (34.08) | 1749 (34.34) | 1924 (36.78) | 1855 (35.92) |
| ≥3.5 | 1536 (44.97) | 1554 (44.49) | 1561 (41.82) | 1448 (41.07) | 1586 (40.87) | 1355 (42.21) | 1359 (44.02) |
| Men * | Women * | |
|---|---|---|
| Race | ||
| NH-Caucasian | 1 (ref) | 1 (ref) |
| Hispanic a | 0.99 (0.77, 1.27) | 1.41 (1.16, 1.72) |
| NH-African American | 1.53 (1.17,1.99) | 1.88 (1.58, 2.23) |
| Education level | ||
| <high school | 1 (ref) | 1 (ref) |
| High school graduate/GED | 0.94 (0.70, 1.25) | 0.75 (0.59, 0.94) |
| Some college | 1.14(0.84, 1.55) | 0.68 (0.55, 0.83) |
| ≥college | 0.49 (0.32, 0.77) | 0.40 (0.29, 0.54) |
| PIR | ||
| <1.3 | 1 (ref) | 1 (ref) |
| 1.3–3.5 | 0.75 (0.59, 0.94) | 0.57 (0.46, 0.71) |
| ≥3.5 | 0.58 (0.44, 0.77) | 0.41 (0.31, 0.53) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xu, Y.; Wu, Q. Prevalence Trend and Disparities in Rheumatoid Arthritis among US Adults, 2005–2018. J. Clin. Med. 2021, 10, 3289. https://doi.org/10.3390/jcm10153289
Xu Y, Wu Q. Prevalence Trend and Disparities in Rheumatoid Arthritis among US Adults, 2005–2018. Journal of Clinical Medicine. 2021; 10(15):3289. https://doi.org/10.3390/jcm10153289
Chicago/Turabian StyleXu, Yingke, and Qing Wu. 2021. "Prevalence Trend and Disparities in Rheumatoid Arthritis among US Adults, 2005–2018" Journal of Clinical Medicine 10, no. 15: 3289. https://doi.org/10.3390/jcm10153289
APA StyleXu, Y., & Wu, Q. (2021). Prevalence Trend and Disparities in Rheumatoid Arthritis among US Adults, 2005–2018. Journal of Clinical Medicine, 10(15), 3289. https://doi.org/10.3390/jcm10153289