
Importance of Lung Ultrasound Follow-Up in Patients Who Had Recovered from Coronavirus Disease 2019: Results from a Prospective Study

 ,
,  , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Epidemiological, Clinical, Laboratory and Radiological Data Assessment
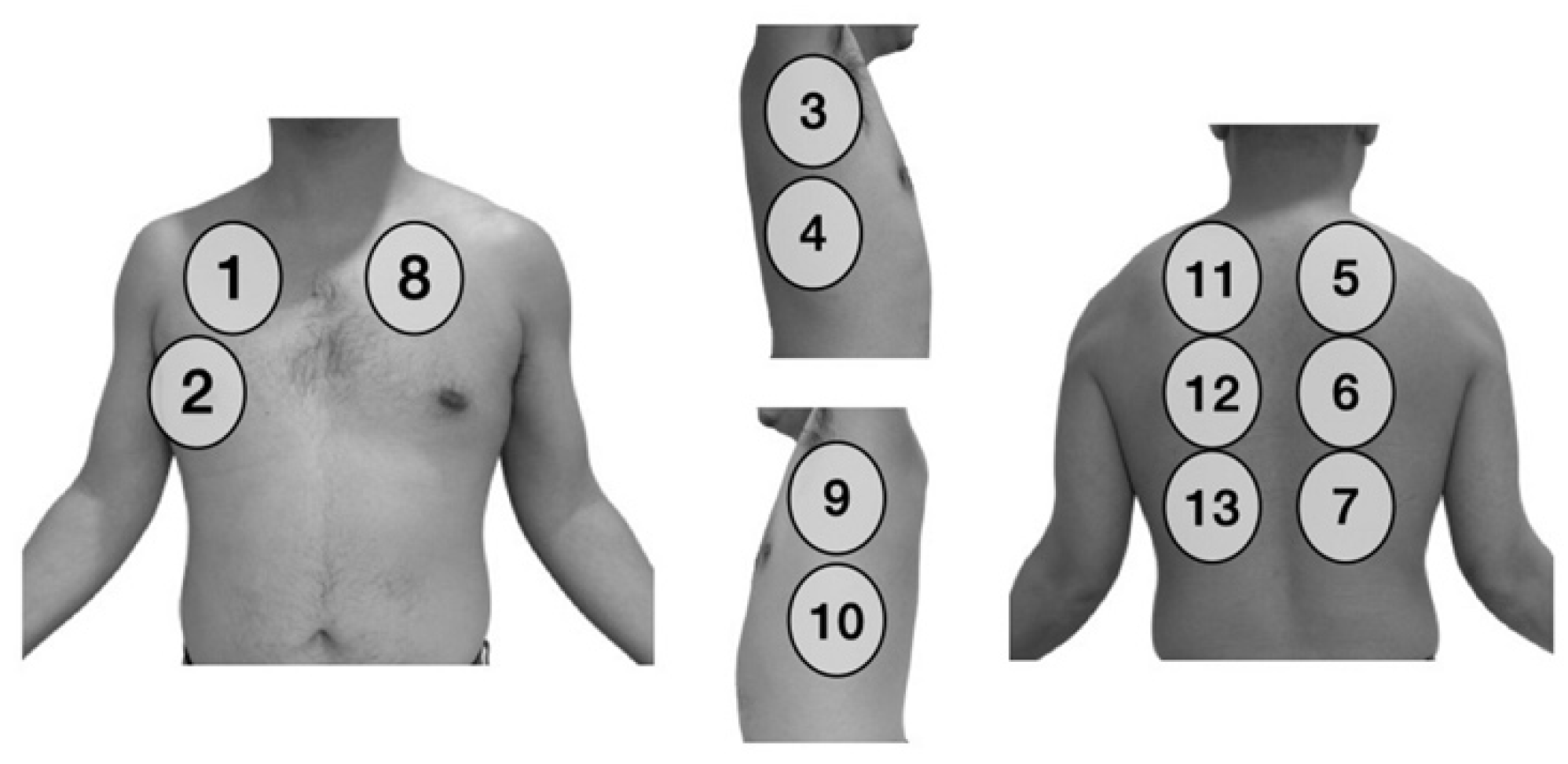
2.3. Ultrasound Data Collection
2.4. PaFi (PaO2/FiO2)
- PaFi ≥ 300 mmHg: no ARDS.
- PaFi 200–299 mmHg: mild ARDS.
- PaFi 100–199 mmHg: moderate ARDS.
- PaFi < 100 mmHg: severe ARDS.
2.5. Statistical Analysis
3. Results
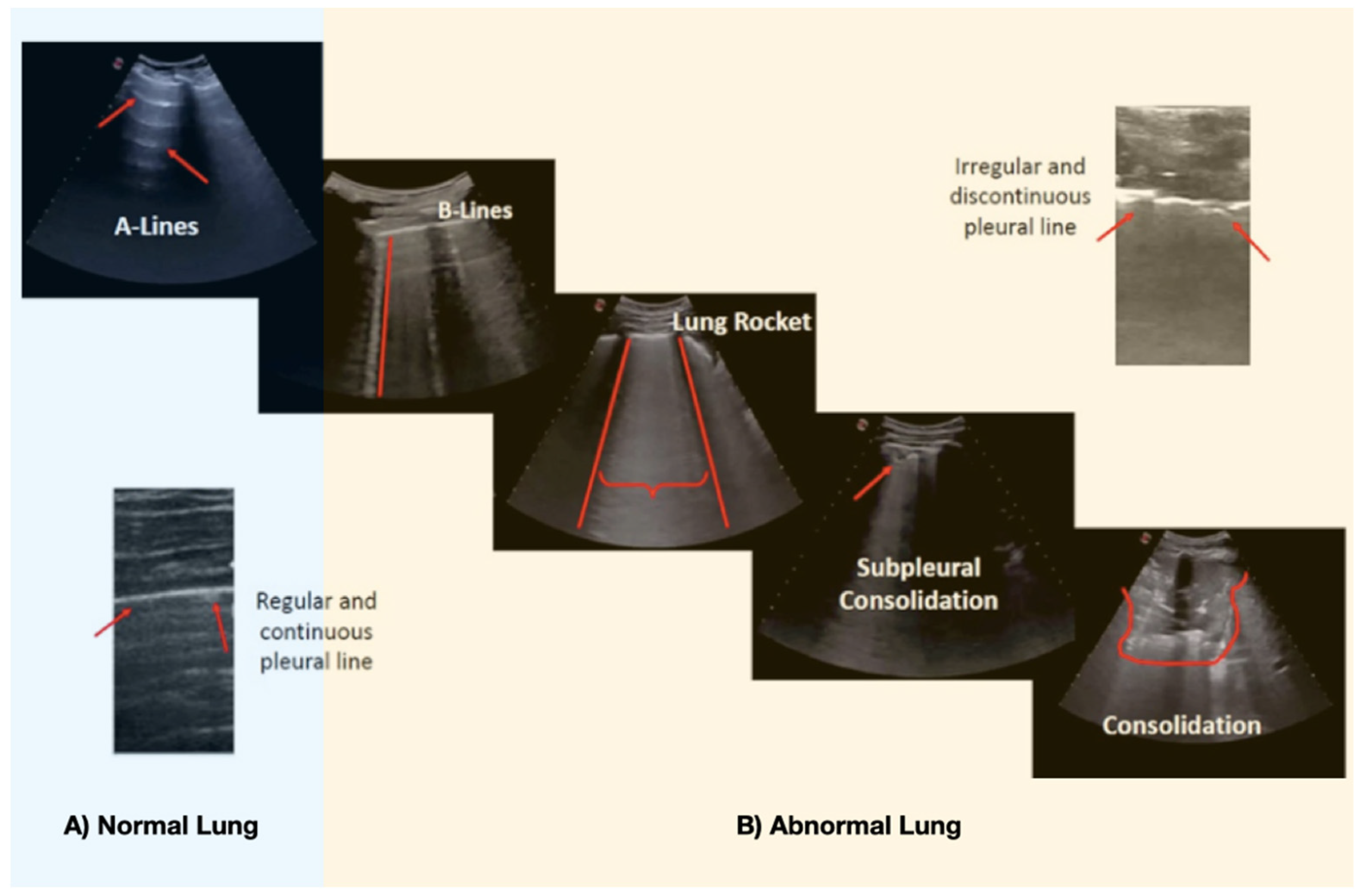
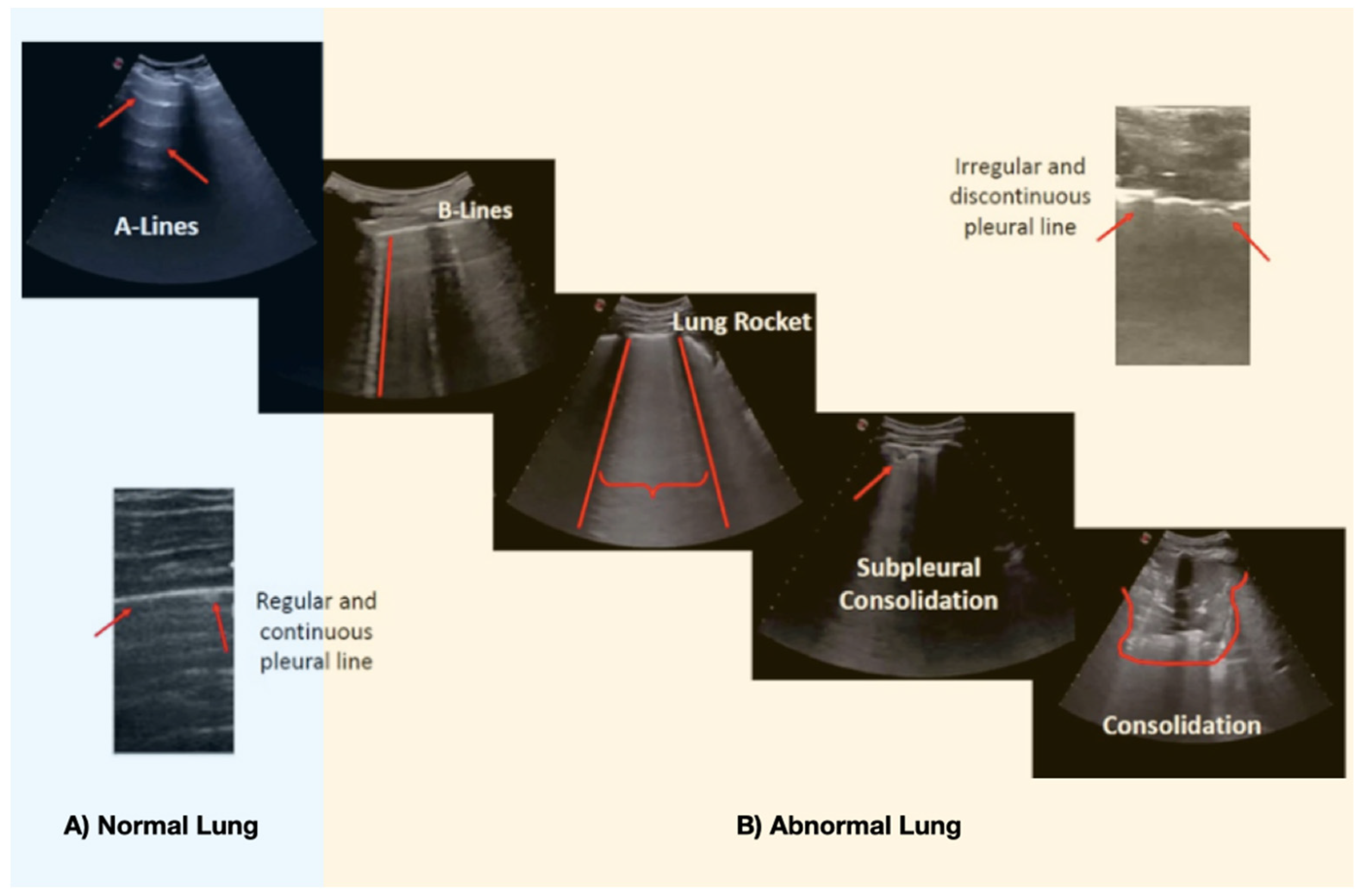
3.1. Findings on Lung Ultrasound
3.1.1. Initial (Baseline) Ultrasound
3.1.2. Lung Ultrasound Follow-Up
3.2. Progression of the Lung Score
- Absence of improvement: decrease in score <25%
- Mild improvement: score decrease of 25–50%
- Moderate improvement: decrease in score from 50% to 75%
- Great improvement: score decrease >75%
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Guan, W.-J.; Ni, Z.-Y.; Hu, Y.; Liang, W.-H.; Ou, C.-Q.; He, J.-X.; Liu, L.; Shan, H.; Lei, C.-L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Weiss, P.; Murdoch, D.R. Clinical course and mortality risk of severe COVID-19. Lancet 2020, 395, 1014–1015. [Google Scholar] [CrossRef]
- Casas-Rojo, J.; Antón-Santos, J.; Millán-Núñez-Cortés, J.; Lumbreras-Bermejo, C.; Ramos-Rincón, J.; Roy-Vallejo, E.; Artero-Mora, A.; Arnalich-Fernández, F.; García-Bruñén, J.; Vargas-Núñez, J.; et al. Clinical characteristics of patients hospitalized with COVID-19 in Spain: Results from the SEMI-COVID-19 Registry. Rev. Clín. Esp. 2020, 220, 480–494. [Google Scholar] [CrossRef]
- Ai, T.; Yang, Z.; Hou, H.; Zhan, C.; Chen, C.; Lv, W.; Tao, Q.; Sun, Z.; Xia, L. Correlation of Chest CT and RT-PCR Testing for Coronavirus Disease 2019 (COVID-19) in China: A Report of 1014 Cases. Radiology 2020, 296, E32–E40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tung-Chen, Y.; Marti de Gracia, M.; Diez Tascon, A.; Agudo-Fernandez, S.; Alonso-Gonzalez, R.; Rodriguez Fuertes, P.; Parra-Gordo, M.L.; Llamas-Fuentes, R. Correlation between chest computed tomography and lung ultrasonography in patients with coronavirus disease 2019 (COVID-19). Ultrasound Med. Biol. 2020, 46, 202–207. [Google Scholar] [CrossRef] [PubMed]
- Orso, D.; Guglielmo, N.; Copetti, R. Lung ultrasound in diagnosing pneumonia in the emergency department: A systematic review and meta-analysis. Eur. J. Emerg. Med. 2018, 25, 312–321. [Google Scholar] [CrossRef] [PubMed]
- Peng, Q.-Y.; Chinese Critical Care Ultrasound Study Group (CCUSG); Wang, X.-T.; Zhang, L.-N. Findings of lung ultrasonography of novel corona virus pneumonia during the 2019–2020 epidemic. Intensiv. Care Med. 2020, 46, 849–850. [Google Scholar] [CrossRef] [Green Version]
- Gobierno de España MDS. Instituto de Salud Carlos III. Estrategia de Detección Precoz, Vigilancia y Control de COVID-19. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/documentos/COVID19_Estrategia_vigilancia_y_control_e_indicadores.pdf (accessed on 10 December 2020).
- The COVID-19. Treatment Guidelines Panel Regularly Updates the Recommendations in these Guidelines as New Information on the Management of COVID-19 Becomes Available. 2021. The Most Recent Version of the Guidelines can be Found on the COVID-19 Treatment Guidelines Website. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 17 March 2021).
- Soldati, G.; Smargiassi, A.; Inchingolo, R.; Buonsenso, D.; Perrone, T.; Briganti, D.F.; Perlini, S.; Torri, E.; Mariani, A.; Mossolani, E.; et al. Proposal for international standardization of the use of lung ultrasound for COVID-19 patients; a simple, quantitative, reproducible method. J. Ultrasound Med. 2020, 39, 1413–1419. [Google Scholar] [CrossRef] [Green Version]
- ARDS Definition Task Force; Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, S. Acute respiratory distress syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar]
- Brown, S.M.; Grissom, C.K.; Moss, M.; Rice, T.W.; Schoenfeld, D.; Hou, P.C.; Thompson, B.T.; Brower, R. NIH/NHLBI PETAL Network Collaborators. Nonlinear Imputation of Pao2/Fio2 From Spo2/Fio2 Among Patients With Acute Respiratory Distress Syndrome. Chest 2016, 150, 307–313. [Google Scholar] [CrossRef] [Green Version]
- Pare, J.R.; Camelo, I.; Mayo, K.C.; Leo, M.M.; Dugas, J.N.; Nelson, K.P.; Baker, W.; Shareef, F.; Mitchell, P.; Schechter-Perkins, E. Point-of-care Lung Ultrasound Is More Sensitive than Chest Radiograph for Evaluation of COVID-19. West J. Emerg. Med. 2020, 21, 771–778. [Google Scholar] [CrossRef]
- Mateos González, M.; García de Casasola Sánchez, G.; Muñoz, F.J.T.; Proud, K.; Lourdo, D.; Sander, J.-V.; Ortiz Jaimes, E.; Mader, M.; Canora Labrato, J.; Restrepo, M.; et al. Comparison of Lung Ultrasound Versus Chest X-ray for Detection of Pulmonary Infiltrates in COVID-19. Diagnostics 2021, 11, 373. [Google Scholar] [CrossRef] [PubMed]
- Volpicelli, G.; Gargani, L. Sonographic signs and patterns of COVID-19 pneumonia. Ultrasound J. 2020, 12, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Tung-Chen, Y.; Algora-Martín, A.; Llamas-Fuentes, R.; Rodríguez-Fuertes, P.; Virto, A.M.M.; Sanz-Rodríguez, E.; Alonso-Martinez, B.; Rivera; Nunez, M.A. Point-of-care ultrasonography in the initial characterization of patients with COVID-19. Med. Clínica 2021, in press. [Google Scholar] [CrossRef]
- Vetrugno, L.; Bove, T.; Orso, D.; Barbariol, F.; Bassi, F.; Boero, E.; Ferrari, G.; Kong, R. Our Italian experience using lung ultrasound for identification, grading and serial follow-up of severity of lung involvement for management of patients with COVID-19. Echocardiography 2020, 37, 625–627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubio-Gracia, J.; Giménez-López, I.; Garcés-Horna, V.; López-Delgado, D.; Sierra-Monzón, J.L.; Martínez-Lostao, L.; Josa-Laorden, C.; Ruiz-Laiglesia, F.; Pérez-Calvo, J.I.; Crespo-Aznarez, S.; et al. Point-of-care lung ultrasound assessment for risk stratification and therapy guiding in COVID-19 patients. A prospective non-interventional study. Eur. Respir. J. 2021, 2004283. [Google Scholar] [CrossRef] [PubMed]
- Asukawa, K.; Minami, T.; Boulware, D.R.; Shimada, A.; Fischer, E.A. Point-of-Care Lung Ultrasound for COVID-19: Findings and Prognostic Implications From 105 Consecutive Patients. J. Intensiv. Care Med. 2021, 36, 334–342. [Google Scholar] [CrossRef]
- Han, X.; Fan, Y.; Alwalid, O.; Li, N.; Jia, X.; Yuan, M.; Li, Y.; Cao, Y.; Gu, J.; Wu, H.; et al. Six-month Follow-up Chest CT Findings after Severe COVID-19 Pneumonia. Radiology 2021, 299, E177–E186. [Google Scholar] [CrossRef]
- So, M.; Kabata, H.; Fukunaga, K.; Takagi, H.; Kuno, T. Radiological and functional lung sequelae of COVID-19: A systematic review and meta-analysis. BMC Pulm. Med. 2021, 21, 97. [Google Scholar] [CrossRef]
- Wu, Q.; Zhong, L.; Li, H.; Guo, J.; Li, Y.; Hou, X.; Yang, F.; Xie, Y.; Li, L.; Xing, Z. A Follow-Up Study of Lung Function and Chest Computed Tomography at 6 Months after Discharge in Patients with Coronavirus Disease 2019. Can. Respir. J. 2021, 2021, 1–7. [Google Scholar] [CrossRef]
- Tabatabaei, S.M.H.; Rajebi, H.; Moghaddas, F.; Ghasemiadl, M.; Talari, H. Chest CT in COVID-19 pneumonia: What are the findings in mid-term follow-up. Emerg. Radiol. 2020, 27, 711–719. [Google Scholar] [CrossRef]
- Liu, C.; Ye, L.; Xia, R.; Zheng, X.; Yuan, C.; Wang, Z.; Lin, R.; Shi, D.; Gao, Y.; Yao, J.; et al. Chest Computed Tomography and Clinical Follow-Up of Discharged Patients with COVID-19 in Wenzhou City, Zhejiang, China. Ann. Am. Thorac. Soc. 2020, 17, 1231–1237. [Google Scholar] [CrossRef] [PubMed]
- Giovannetti, G.; De Michele, L.; De Ceglie, M.; Pierucci, P.; Mirabile, A.; Vita, M.; Ostilio Palmieri, V.; Carpagnano, F.; Scardapane, A.; D’Agostino, C. Lung ultrasonography for long-term follow-up of COVID-19 survivors compared to chest CT scan. Respir. Med. 2021, 181, 106384. [Google Scholar] [CrossRef] [PubMed]
- Alharthy, A.; Abuhamdah, M.; Balhamar, A.; Faqihi, F.; Nasim, N.; Ahmad, S.; Noor, A.; Tamim, H.; Alwahtani, S.; Al Saud, A. Residual Lung Injury in Patients Recovering From COVID-19 Critical Illness: A Prospective Longitudinal Point-of-Care Lung Ultrasound Study. J. Ultrasound Med. 2020, in press. [Google Scholar] [CrossRef] [PubMed]
- Nazerian, P.; Vanni, S.; Volpicelli, G.; Gigli, C.; Zanobetti, M.; Bartolucci, M.; Ciavatton, A.; Lamorte, A.; Veltri, A.; Fabbri, A.; et al. Accuracy of point-of-care multiorgan ultrasonography for the diagnosis of pulmonary embolism. Chest 2014, 145, 950–957. [Google Scholar] [CrossRef] [Green Version]
- Zotzmann, V.; Lang, C.N.; Bamberg, F.; Bode, C.; Staudacher, D.L. Are subpleural consolidations indicators for segmental pulmonary embolism in COVID-19? Intensiv. Care Med. 2020, 46, 1109–1110. [Google Scholar] [CrossRef] [Green Version]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary Vascular Endothelialitis, Thrombosis, and Angiogenesis in Covid-19. N. Engl. J. Med. 2020, 383, 120–128. [Google Scholar] [CrossRef]
- Mafort, T.T.; Rufino, R.; da Costa, C.H.; da Cal, M.S.; Monnerat, L.B.; Litrento, P.F.; Zuluaga Parra, L.; de Sá Earp de Souza Marinho, A. One-month outcomes of patients with SARS-CoV-2 infection and their relationships with lung ultrasound signs. Ultrasound J. 2021, 13, 19. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Demographics and Clinical Characteristics | Number of Patients (n = 96) |
|---|---|
| Gender (n (%)) | |
| Male | 53 (55.2%) |
| Female | 43 (44.8%) |
| Age (mean ± SD); (n (%)) | |
| Mean age (years) | 55.79 ± 13.3 |
| 20–35 years | 8 (8.3%) |
| 35–50 years | 21 (21.8%) |
| 50–65 years | 45 (46.8%) |
| 65–80 years | 19 (19.7%) |
| ≥80 years | 3 (3.1%) |
| Medical History (n (%)) | |
| Hypertension | 29 (30.2%) |
| Diabetes mellitus | 10 (10.4%) |
| Overweight or obesity | 54 (56.2%) |
| Chronic heart disease | 8 (8.3%) |
| COPD/asthma | 16 (16.6%) |
| Therapy received during hospitalization (n (%)) | |
| Corticosteroids | 71 (73.9%) |
| Antibiotics | 65 (67.7%) |
| Tocilizumab (anti-interleukin 6) | 34 (35.4%) |
| Anakinra (anti-interleukin 1) | 3 (3.1%) |
| Classification according to Severity (n (%)) | |
| No ARDS (PaFi ≥ 300 mmHg) | 22 (22.9%) |
| Mild ARDS (PaFi 200–299 mmHg) | 11 (11.4%) |
| Moderate ARDS (PaFi 100–199 mmHg) | 37 (38.5%) |
| Severe ARDS (PaFi < 100 mmHg) | 26 (27%) |
| Complications during hospitalization and follow-up | |
| NIMV | 15 (15.6%) |
| PE | 14 (14.6%) |
| Heart failure | 4 (4.1%) |
| IMV | 6 (6.2%) |
| Classification According to Severity | No. with Bilateral Involvement (%) | No. with Affected Lung Areas (Mean ± SD) | No. with Subpleural Consolidation (%) | No. with Consolidation > 1 cm (%) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Basal | 1 Month | 3 Months | Basal | 1 Month | 3 Months | Basal | 1 Month | 3 Months | Basal | 1 Month | 3 Months | |
| All (n = 96) | 90 (93.7%) | 77 (80.2%) | 30 (31.2%) | 10.2 ± 4 | 8 ± 4 | 4.3 ± 3 | 66 (68.7%) | 30 (31%) | 1 (1%) | 24 (25%) | 1 (1%) | 0 |
| No ARDS (n = 22) | 15 (68%) | 5 (22.7%) | 0% | 3.6 ± 2.7 | 3.3 ± 2 | 0 | 8 (36.3%) | 1 (4.5%) | 0 | 0 | 0 | 0 |
| Mild ARDS (n = 11) | 11 (100%) | 10 (91%) | 2 (18%) | 10.8 ± 2 | 7.1 ± 3 | 2.8 ± 2 | 7 (63.6%) | 3 (27%) | 0 | 1 (9%) | 0 | 0 |
| Moderate ARDS (n = 37) | 37 (100%) | 36 (91.3%) | 12 (32.4%) | 12 ± 1.5 | 8 ± 3 | 4 ± 3 | 30 (81%) | 10 (27%) | 0 | 10 (27%) | 0 | 0 |
| Severe ARDS (n = 26) | 26 (100%) | 25 (96.1%) | 16 (61.5%) | 12.7 ± 0.7 | 10 ± 3 | 5 ± 3 | 21 (80.7%) | 16 (61.5%) | 1 (3.8%) | 13 (50%) | 1 (3.8%) | 0 |
| Classification According to Severity | PaFi (Mean ± SD mmHg) | Score (Mean ± SD) | ||||
|---|---|---|---|---|---|---|
| Basal | 1 Month | 3 Months | Basal | 1 Month | 3 Months | |
| All (n = 96) | 201 ± 125 | 388 ± 50 | 424 ± 39 | 39 ± 20 | 22 ± 17 | 5 ± 7 |
| No ARDS (n = 22) | 405 ± 56 | 430 ± 36 | 444 ± 32 | 9.8 ± 8 | 3.2 ± 5 | 0 |
| Mild ARDS (n = 11) | 249 ± 21 | 393 ± 44 | 415 ± 46 | 32.8 ± 7 | 17.8 ± 10 | 2.7 ± 5 |
| Moderate ARDS (n = 37) | 148 ± 33 | 379 ± 37 | 423 ± 36 | 42 ± 6 | 24.2 ± 16 | 4.5 ± 7 |
| Severe ARDS (n = 26) | 88 ± 7 | 364 ± 56 | 415 ± 43 | 61.5 | 34.5 | 9 ± 10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hernández-Píriz, A.; Tung-Chen, Y.; Jiménez-Virumbrales, D.; Ayala-Larrañaga, I.; Barba-Martín, R.; Canora-Lebrato, J.; Zapatero-Gaviria, A.; Casasola-Sánchez, G.G.D. Importance of Lung Ultrasound Follow-Up in Patients Who Had Recovered from Coronavirus Disease 2019: Results from a Prospective Study. J. Clin. Med. 2021, 10, 3196. https://doi.org/10.3390/jcm10143196
Hernández-Píriz A, Tung-Chen Y, Jiménez-Virumbrales D, Ayala-Larrañaga I, Barba-Martín R, Canora-Lebrato J, Zapatero-Gaviria A, Casasola-Sánchez GGD. Importance of Lung Ultrasound Follow-Up in Patients Who Had Recovered from Coronavirus Disease 2019: Results from a Prospective Study. Journal of Clinical Medicine. 2021; 10(14):3196. https://doi.org/10.3390/jcm10143196
Chicago/Turabian StyleHernández-Píriz, Alba, Yale Tung-Chen, David Jiménez-Virumbrales, Ibone Ayala-Larrañaga, Raquel Barba-Martín, Jesús Canora-Lebrato, Antonio Zapatero-Gaviria, and Gonzalo García De Casasola-Sánchez. 2021. "Importance of Lung Ultrasound Follow-Up in Patients Who Had Recovered from Coronavirus Disease 2019: Results from a Prospective Study" Journal of Clinical Medicine 10, no. 14: 3196. https://doi.org/10.3390/jcm10143196
APA StyleHernández-Píriz, A., Tung-Chen, Y., Jiménez-Virumbrales, D., Ayala-Larrañaga, I., Barba-Martín, R., Canora-Lebrato, J., Zapatero-Gaviria, A., & Casasola-Sánchez, G. G. D. (2021). Importance of Lung Ultrasound Follow-Up in Patients Who Had Recovered from Coronavirus Disease 2019: Results from a Prospective Study. Journal of Clinical Medicine, 10(14), 3196. https://doi.org/10.3390/jcm10143196