
Characterization of a Temporal Profile of Biomarkers as an Index for Ischemic Stroke Onset Definition


 ,
,  ,
,  ,
,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Primary Endpoint
2.2. Study Design
2.3. Population of Study and Clinical Variables
2.4. Analytical Measurements
2.5. Neuroimaging Studies
2.6. Statistical Analysis
3. Results
3.1. Time Dependence of Early Latency Times and Demographic Aspects
3.2. Time Dependency of Clinical Aspects
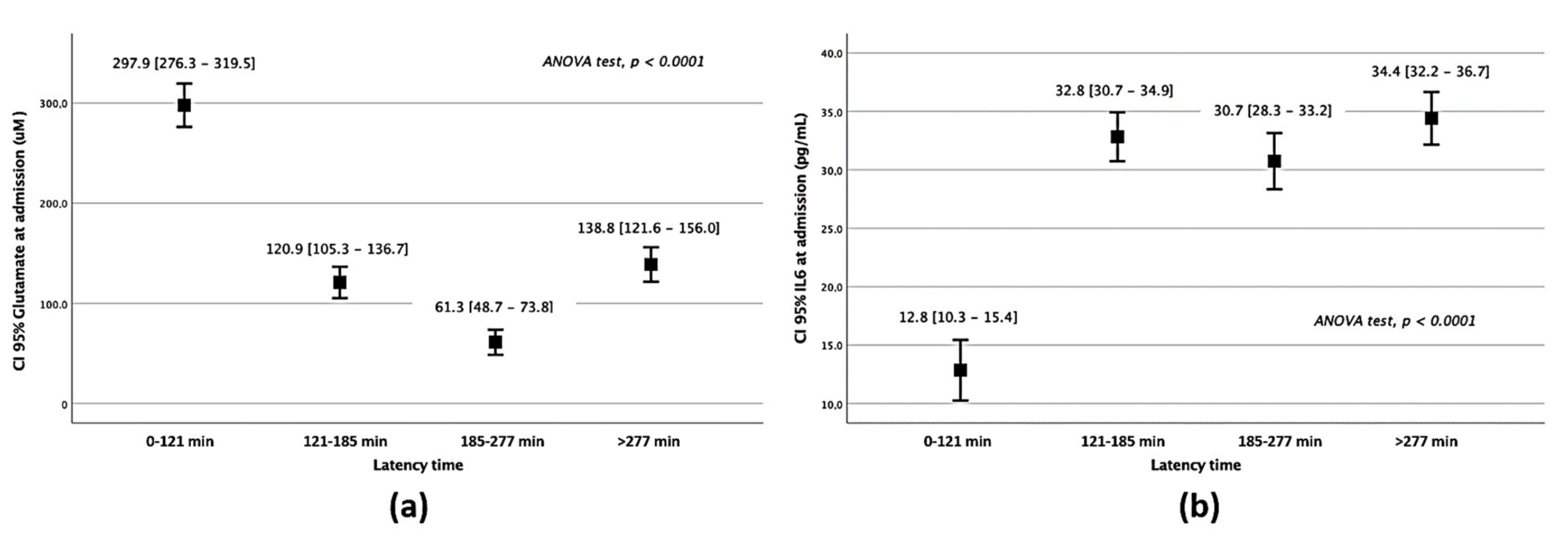
3.3. Time Dependence of Circulating Biomarkers
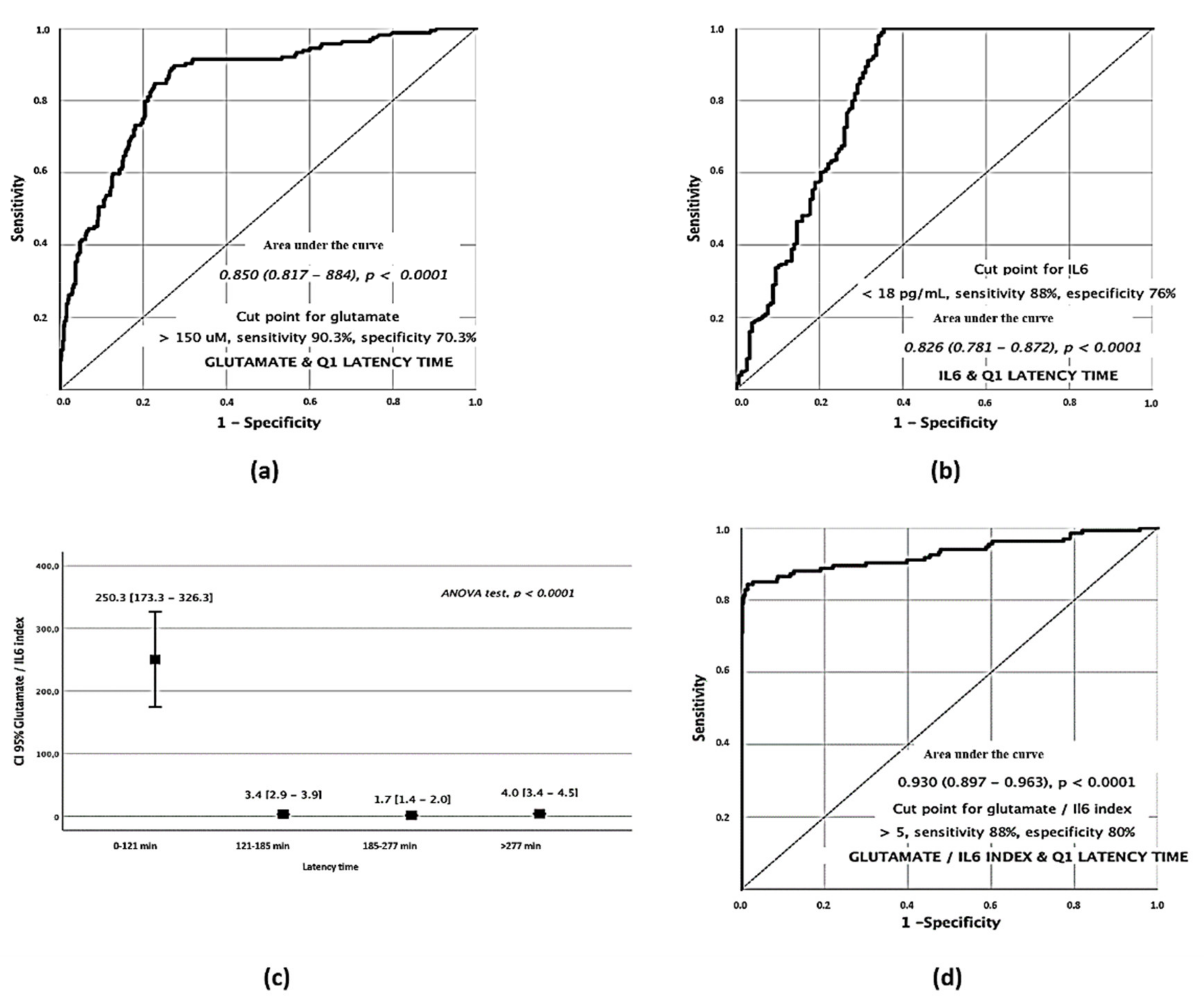
3.4. Excitotoxicity/Inflammation Index as a Time Marker for Early Symptom Onset
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Saver, J.L. Time is brain—Quantified. Stroke 2006, 37, 263–266. [Google Scholar] [CrossRef] [Green Version]
- Yeo, L.L.; Paliwal, P.; Teoh, H.L.; Seet, R.C.; Chan, B.P.; Liang, S.; Venketasubramanian, N.; Rathakrishnan, R.; Ahmad, A.; Ng, K.W.; et al. Timing of recanalization after intravenous thrombolysis and functional outcomes after acute ischemic stroke. JAMA Neurol. 2013, 70, 353–358. [Google Scholar] [CrossRef] [Green Version]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. 2018 Guidelines for the Early Management of Patients With Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2018, 49, e46–e110. [Google Scholar] [CrossRef]
- Campos, F.; Sobrino, T.; Ramos-Cabrer, P.; Argibay, B.; Agulla, J.; Perez-Mato, M.; Rodriguez-Gonzalez, R.; Brea, D.; Castillo, J. Neuroprotection by glutamate oxaloacetate transaminase in ischemic stroke: An experimental study. J. Cereb. Blood Flow Metab. 2011, 31, 1378–1386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Witsch, J.; Bruce, E.; Meyers, E.; Velazquez, A.; Schmidt, J.M.; Suwatcharangkoon, S.; Agarwal, S.; Park, S.; Falo, M.C.; Connolly, E.S.; et al. Intraventricular hemorrhage expansion in patients with spontaneous intracerebral hemorrhage. Neurology 2015, 84, 989–994. [Google Scholar] [CrossRef] [Green Version]
- Aguilar, M.I.; Brott, T.G. Update in intracerebral hemorrhage. Neurohospitalist 2011, 1, 148–159. [Google Scholar] [CrossRef] [Green Version]
- Worthmann, H.; Tryc, A.B.; Goldbecker, A.; Ma, Y.T.; Tountopoulou, A.; Hahn, A.; Dengler, R.; Lichtinghagen, R.; Weissenborn, K. The temporal profile of inflammatory markers and mediators in blood after acute ischemic stroke differs depending on stroke outcome. Cerebrovasc. Dis. 2010, 30, 85–92. [Google Scholar] [CrossRef]
- Davalos, A.; Castillo, J.; Serena, J.; Noya, M. Duration of glutamate release after acute ischemic stroke. Stroke 1997, 28, 708–710. [Google Scholar] [CrossRef] [PubMed]
- Campos, F.; Sobrino, T.; Ramos-Cabrer, P.; Castillo, J. Oxaloacetate: A novel neuroprotective for acute ischemic stroke. Int. J. Biochem. Cell Biol. 2012, 44, 262–265. [Google Scholar] [CrossRef]
- Chamorro, Á.; Dirnagl, U.; Urra, X.; Planas, A.M. Neuroprotection in acute stroke: Targeting excitotoxicity, oxidative and nitrosative stress, and inflammation. Lancet Neurol. 2016, 15, 869–881. [Google Scholar] [CrossRef]
- Kellner, C.P.; Connolly, E.S., Jr. Neuroprotective strategies for intracerebral hemorrhage: Trials and translation. Stroke 2010, 41, S99–S102. [Google Scholar] [CrossRef] [Green Version]
- Castillo, J.; Loza, M.I.; Mirelman, D.; Brea, J.; Blanco, M.; Sobrino, T.; Campos, F. A novel mechanism of neuroprotection: Blood glutamate grabber. J. Cereb. Blood Flow Metab. 2015, 36, 292–301. [Google Scholar] [CrossRef] [PubMed]
- Jickling, G.C.; Sharp, F.R. Blood biomarkers of ischemic stroke. Neurotherapeutics 2011, 8, 349–360. [Google Scholar] [CrossRef] [Green Version]
- Dagonnier, M.; Donnan, G.A.; Davis, S.M.; Dewey, H.M.; Howells, D.W. Acute Stroke Biomarkers: Are We There Yet? Front. Neurol. 2021, 12, 73. [Google Scholar] [CrossRef]
- Kamtchum-Tatuene, J.; Jickling, G.C. Blood Biomarkers for Stroke Diagnosis and Management. Neuromol. Med. 2019, 21, 344–368. [Google Scholar] [CrossRef]
- Smith, C.J.; Emsley, H.C.; Gavin, C.M.; Georgiou, R.F.; Vail, A.; Barberan, E.M.; del Zoppo, G.J.; Hallenbeck, J.M.; Rothwell, N.J.; Hopkins, S.J.; et al. Peak plasma interleukin-6 and other peripheral markers of inflammation in the first week of ischaemic stroke correlate with brain infarct volume, stroke severity and long-term outcome. BMC Neurol. 2004, 4, 2. [Google Scholar] [CrossRef]
- Sotgiu, S.; Zanda, B.; Marchetti, B.; Fois, M.L.; Arru, G.; Pes, G.M.; Salaris, F.S.; Arru, A.; Pirisi, A.; Rosati, G. Inflammatory biomarkers in blood of patients with acute brain ischemia. Eur. J. Neurol. 2006, 13, 505–513. [Google Scholar] [CrossRef]
- Laskowitz, D.T.; Kasner, S.E.; Saver, J.; Remmel, K.S.; Jauch, E.C.; Group, B.S. Clinical usefulness of a biomarker-based diagnostic test for acute stroke: The Biomarker Rapid Assessment in Ischemic Injury (BRAIN) study. Stroke 2009, 40, 77–85. [Google Scholar] [CrossRef] [Green Version]
- Glushakova, O.Y.; Glushakov, A.V.; Miller, E.R.; Valadka, A.B.; Hayes, R.L. Biomarkers for acute diagnosis and management of stroke in neurointensive care units. Brain Circ. 2016, 2, 28–47. [Google Scholar] [CrossRef]
- Montaner, J.; Molina, C.A.; Monasterio, J.; Abilleira, S.; Arenillas, J.F.; Ribo, M.; Quintana, M.; Alvarez-Sabin, J. Matrix metalloproteinase-9 pretreatment level predicts intracranial hemorrhagic complications after thrombolysis in human stroke. Circulation 2003, 107, 598–603. [Google Scholar] [CrossRef] [Green Version]
- Castellanos, M.; Leira, R.; Serena, J.; Pumar, J.M.; Lizasoain, I.; Castillo, J.; Davalos, A. Plasma metalloproteinase-9 concentration predicts hemorrhagic transformation in acute ischemic stroke. Stroke 2003, 34, 40–46. [Google Scholar] [CrossRef] [Green Version]
- Fon, E.A.; Mackey, A.; Cote, R.; Wolfson, C.; McIlraith, D.M.; Leclerc, J.; Bourque, F. Hemostatic markers in acute transient ischemic attacks. Stroke 1994, 25, 282–286. [Google Scholar] [CrossRef] [Green Version]
- Donkel, S.J.; Benaddi, B.; Dippel, D.W.J.; Ten Cate, H.; de Maat, M.P.M. Prognostic Hemostasis Biomarkers in Acute Ischemic Stroke. Arterioscler. Thromb. Vasc. Biol. 2019, 39, 360–372. [Google Scholar] [CrossRef]
- Castillo, J.; Davalos, A.; Noya, M. Progression of ischaemic stroke and excitotoxic aminoacids. Lancet 1997, 349, 79–83. [Google Scholar] [CrossRef]
- Meng, X.-e.; Li, N.; Guo, D.-Z.; Pan, S.-Y.; Li, H.; Yang, C. High Plasma Glutamate Levels are Associated with Poor Functional Outcome in Acute Ischemic Stroke. Cell. Mol. Neurobiol. 2015, 35, 159–165. [Google Scholar] [CrossRef]
- Emsley, H.C.; Smith, C.J.; Gavin, C.M.; Georgiou, R.F.; Vail, A.; Barberan, E.M.; Hallenbeck, J.M.; del Zoppo, G.J.; Rothwell, N.J.; Tyrrell, P.J.; et al. An early and sustained peripheral inflammatory response in acute ischaemic stroke: Relationships with infection and atherosclerosis. J. Neuroimmunol. 2003, 139, 93–101. [Google Scholar] [CrossRef]
- Perini, F.; Morra, M.; Alecci, M.; Galloni, E.; Marchi, M.; Toso, V. Temporal profile of serum anti-inflammatory and pro-inflammatory interleukins in acute ischemic stroke patients. Neurol. Sci. Off. J. Ital. Neurol. Soc. Ital. Soc. Clin. Neurophysiol. 2001, 22, 289–296. [Google Scholar] [CrossRef]
- Georgakis, M.K.; Malik, R.; Gill, D.; Franceschini, N.; Sudlow, C.L.M.; Dichgans, M.; Lindstrom, S.; Wang, L.; Smith, E.N.; Gordon, W.; et al. Interleukin-6 Signaling Effects on Ischemic Stroke and Other Cardiovascular Outcomes. Circ. Genom. Precis. Med. 2020, 13, e002872. [Google Scholar] [CrossRef]
- Hotter, B.; Hoffmann, S.; Ulm, L.; Meisel, C.; Fiebach, J.B.; Meisel, A. IL-6 Plasma Levels Correlate With Cerebral Perfusion Deficits and Infarct Sizes in Stroke Patients Without Associated Infections. Front. Neurol. 2019, 10, 83. [Google Scholar] [CrossRef]
- Adams, H.P., Jr.; Bendixen, B.H.; Kappelle, L.J.; Biller, J.; Love, B.B.; Gordon, D.L.; Marsh, E.E., 3rd. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke 1993, 24, 35–41. [Google Scholar] [CrossRef] [Green Version]
- White, J.; Hart, R.; Fry, J. An evaluation of the Waters Pico-Tag system for the amino-acid analysis of food materials. J. Anal. Methods Chem. 1986, 8, 170–177. [Google Scholar] [CrossRef] [Green Version]
- Sims, J.R.; Gharai, L.R.; Schaefer, P.W.; Vangel, M.; Rosenthal, E.S.; Lev, M.H.; Schwamm, L.H. ABC/2 for rapid clinical estimate of infarct, perfusion, and mismatch volumes. Neurology 2009, 72, 2104–2110. [Google Scholar] [CrossRef]
- Lacy Clifton, R.; Suh, D.-C.; Bueno, M.; Kostis John, B. Delay in Presentation and Evaluation for Acute Stroke. Stroke 2001, 32, 63–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harper, G.D.; Haigh, R.A.; Potter, J.F.; Castleden, C.M. Factors delaying hospital admission after stroke in Leicestershire. Stroke 1992, 23, 835–838. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, T.W.; Zhang, S.; Wang, Y.T. Excitotoxicity and stroke: Identifying novel targets for neuroprotection. Prog. Neurobiol. 2014, 115, 157–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whiteley, W.; Jackson, C.; Lewis, S.; Lowe, G.; Rumley, A.; Sandercock, P.; Wardlaw, J.; Dennis, M.; Sudlow, C. Inflammatory markers and poor outcome after stroke: A prospective cohort study and systematic review of interleukin-6. PLoS Med. 2009, 6, e1000145. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Not Adjusted | Adjusted | |||||
|---|---|---|---|---|---|---|
| OR | CI 95% | p | OR | CI 95% | p | |
| Year * | 1.12 | 1.09–1.15 | <0.0001 | 1.13 | 1.09–1.16 | <0.0001 |
| Age | 0.99 | 0.98–0.99 | <0.0001 | 0.99 | 0.99–1.01 | 0.683 |
| Woman | 0.30 | 0.24–0.34 | <0.0001 | 0.29 | 0.24–0.35 | <0.0001 |
| Hypertension | 0.82 | 0.71–0.96 | 0.014 | 0.96 | 0.77–1.08 | 0.296 |
| Smoking | 1.45 | 1.19–1.76 | <0.0001 | 1.00 | 0.81–1.26 | 0.944 |
| Enolism | 1.61 | 1.29–2.01 | <0.0001 | 1.10 | 0.87–1.40 | 0.429 |
| Q1 | Q2 | Q3 | Q4 | p | |
|---|---|---|---|---|---|
| Temperature at admission, °C | 36.3 ± 0.6 | 36.3 ± 0.6 | 36.4 ± 0.6 | 36.4 ± 0.7 | 0.054 |
| Glycemia, mg/dL | 137.3 ± 60.1 | 135.9 ± 53.6 | 138.7 ± 56.3 | 138.1 ± 61.3 | 0.793 |
| Leukocytes, ×103/mmc | 8.8 ± 3.1 | 9.1 ± 3.2 | 9.4 ± 3.2 | 9.2 ± 3.1 | <0.0001 |
| Fibrinogen, mg/dL | 434.7 ± 100.4 | 439.7 ± 107.6 | 449.8 ± 108.7 | 453.9 ± 95.4 | 0.002 |
| Microalbuminuria, mg/24 h | 8.0 ± 31.9 | 5.5 ± 23.7 | 6.8 ± 30.6 | 4.9 ± 23.9 | 0.337 |
| C reactive protein, mg/L | 2.7 ± 3.5 | 3.2 ± 3.9 | 4.2 ± 4.7 | 3.3 ± 3.9 | <0.0001 |
| Glycosylated haemoglobin, % | 6.3 ± 4.7 | 6.1 ± 1.1 | 6.2 ± 1.3 | 6.2 ± 1.4 | 0.403 |
| LDL cholesterol, mg/dL | 108.3 ± 38.1 | 110.1 ± 37.3 | 106.2 ± 36.9 | 110.6 ± 37.4 | 0.258 |
| HDL cholesterol, mg/dL | 40.0 ± 14.4 | 45.1 ± 28.3 | 42.0 ± 16.0 | 42.4 ± 18.1 | 0.001 |
| Triglycerides, mg/dL | 119.9 ± 71.9 | 115.7 ± 53.8 | 122.8 ± 64.1 | 123.0 ± 67.0 | 0.161 |
| Sedimentation rate, mm/hr | 24.2 ± 22.6 | 25.7 ± 23.8 | 26.6 ± 22.9 | 27.5 ± 23.6 | 0.067 |
| ProBNP, pg/mL | 1469.9 ± 1784.1 | 1703.2 ± 1804.5 | 1685.8 ± 1834.7 | 1608.8 ± 1973.1 | 0.128 |
| Vitamin D, ng/mL | 19.9 ± 9.8 | 19.3 ± 9.9 | 18.1 ± 8.3 | 18.8 ± 9.3 | 0.145 |
| Intima-media thickness, mm | 0.8 ± 0.2 | 0.9 ± 0.9 | 0.9 ± 0.7 | 1.0 ± 0.9 | 0.215 |
| Fibrinolytic treatment, % | 27.1 | 39.1 | 31.9 | 2.0 | <0.0001 |
| Thrombectomy, % | 5.9 | 5.1 | 5.3 | 1.5 | <0.0001 |
| NIHSS at admission | 14 (8, 20) | 14 (9, 20) | 14 (9, 19) | 12 (7, 18) | <0.0001 |
| NIHSS at 24 hours | 6 (2, 14) | 8 (3, 15) | 10 (5, 17) | 6 (2, 14) | <0.0001 |
| NIHSS at 48 hours | 5 (1, 12) | 6 (2, 14) | 8 (2, 16) | 6 (2, 14) | <0.0001 |
| NIHSS at discharge | 6 (2,11) | 47 (2, 12) | 8 (2, 13) | 7 (2, 12) | <0.0001 |
| Early neurological improvement, % | 35.1 | 28.8 | 19.2 | 16.9 | <0.0001 |
| Early neurological deterioration, % | 17.2 | 25.0 | 40.7 | 17.2 | <0.0001 |
| TOAST: | 0.102 | ||||
| Atherothrombotic, % | 22.9 | 22.1 | 25.0 | 24.8 | |
| Cardioembolic, % | 35.1 | 40.1 | 38.7 | 36.0 | |
| Lacunar, % | 9.6 | 5.4 | 5.5 | 10.1 | |
| Indeterminate/others, % | 32.4 | 32.6 | 30.9 | 29.5 | |
| Ischemic DWI volume at admission, mL | 64.2 ± 125.2 | 38.7 ± 54.6 | 32.4 ± 39.9 | 39.9 ± 105.8 | 0.148 |
| Clinical-DWI mismatch, % | 18.0 | 16.9 | 9.1 | 8.5 | 0.001 |
| Infarct volume (CT 4th–7th day), mL | 47.8 ± 84.6 | 50.2 ± 80.3 | 66.6 ± 92.7 | 56.4 ± 86.6 | <0.0001 |
| Growth of the infarct, mL | 7.6 ± 19.4 | 1.9 ± 25.1 | 5.9 ± 13.0 | 9.7 ± 21.7 | 0.165 |
| Haemorrhagic transformation, % | 14.0 | 12.6 | 10.3 | 0.048 |
| Not Adjusted | Adjusted | |||||
|---|---|---|---|---|---|---|
| OR | CI 95% | p | OR | CI 95% | p | |
| Leukocytes | 0.95 | 0.93–0.98 | <0.0001 | 0.92 | 0.82–1.04 | 0.176 |
| Fibrinogen | 0.99 | 0.99–1.00 | 0.005 | 0.99 | 0.99–1.01 | 0.527 |
| C reactive protein | 0.94 | 0.91–0.96 | <0.0001 | 0.94 | 0.83–1.06 | 0.344 |
| HDL-cholesterol | 0.99 | 0.98–0.99 | 0.001 | 0.98 | 0.96–1.01 | 0.144 |
| Fibrinolytic treatment | 1.16 | 0.97–1.37 | 0.009 | 1.74 | 0.59–5.17 | 0.316 |
| Thrombectomy | 1.15 | 1.08–2.12 | 0.016 | 0.16 | 0.02–1.12 | 0.065 |
| Early neurological improvement | 1.98 | 1.67–2.36 | <0.0001 | 0.53 | 0.09–2.93 | 0.046 |
| Early neurological deterioration | 0.60 | 0.41–0.87 | 0.007 | 1.62 | 0.27–9.81 | 0.599 |
| Clinical-DWI mismatch | 1.73 | 1.18–2.52 | 0.005 | 4.23 | 0.93–19.13 | 0.061 |
| NIHSS at admission | 0.98 | 0.97–0.99 | 0.016 | 1.02 | 0.95–1.10 | 0.537 |
| Infarct volume | 0.99 | 0.99–1.00 | 0.011 | 0.99 | 0.97–1.01 | 0.420 |
| Hemorrhagic transformation | 1.24 | 1.00–1.28 | 0.035 | 1.37 | 0.33–5.74 | 0.667 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Da Silva-Candal, A.; Dopico-López, A.; Pérez-Mato, M.; Rodríguez-Yáñez, M.; Pumar, J.M.; Ávila-Gómez, P.; Castillo, J.; Sobrino, T.; Campos, F.; Hervella, P.; et al. Characterization of a Temporal Profile of Biomarkers as an Index for Ischemic Stroke Onset Definition. J. Clin. Med. 2021, 10, 3136. https://doi.org/10.3390/jcm10143136
Da Silva-Candal A, Dopico-López A, Pérez-Mato M, Rodríguez-Yáñez M, Pumar JM, Ávila-Gómez P, Castillo J, Sobrino T, Campos F, Hervella P, et al. Characterization of a Temporal Profile of Biomarkers as an Index for Ischemic Stroke Onset Definition. Journal of Clinical Medicine. 2021; 10(14):3136. https://doi.org/10.3390/jcm10143136
Chicago/Turabian StyleDa Silva-Candal, Andrés, Antonio Dopico-López, Maria Pérez-Mato, Manuel Rodríguez-Yáñez, José M. Pumar, Paulo Ávila-Gómez, José Castillo, Tomás Sobrino, Francisco Campos, Pablo Hervella, and et al. 2021. "Characterization of a Temporal Profile of Biomarkers as an Index for Ischemic Stroke Onset Definition" Journal of Clinical Medicine 10, no. 14: 3136. https://doi.org/10.3390/jcm10143136
APA StyleDa Silva-Candal, A., Dopico-López, A., Pérez-Mato, M., Rodríguez-Yáñez, M., Pumar, J. M., Ávila-Gómez, P., Castillo, J., Sobrino, T., Campos, F., Hervella, P., & Iglesias-Rey, R. (2021). Characterization of a Temporal Profile of Biomarkers as an Index for Ischemic Stroke Onset Definition. Journal of Clinical Medicine, 10(14), 3136. https://doi.org/10.3390/jcm10143136