
Ultrasound-Guided Near-Nerve Needle Sensory Technique for the Diagnosis of Tarsal Tunnel Syndrome

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Electrodiagnostic Techniques
2.2.1. Tibial Motor Nerve Conduction Velocity (NCV)
2.2.2. Medial and Lateral Plantar Sensory NCV with Surface Electrode
2.2.3. Medial and Lateral Plantar Mixed NCV
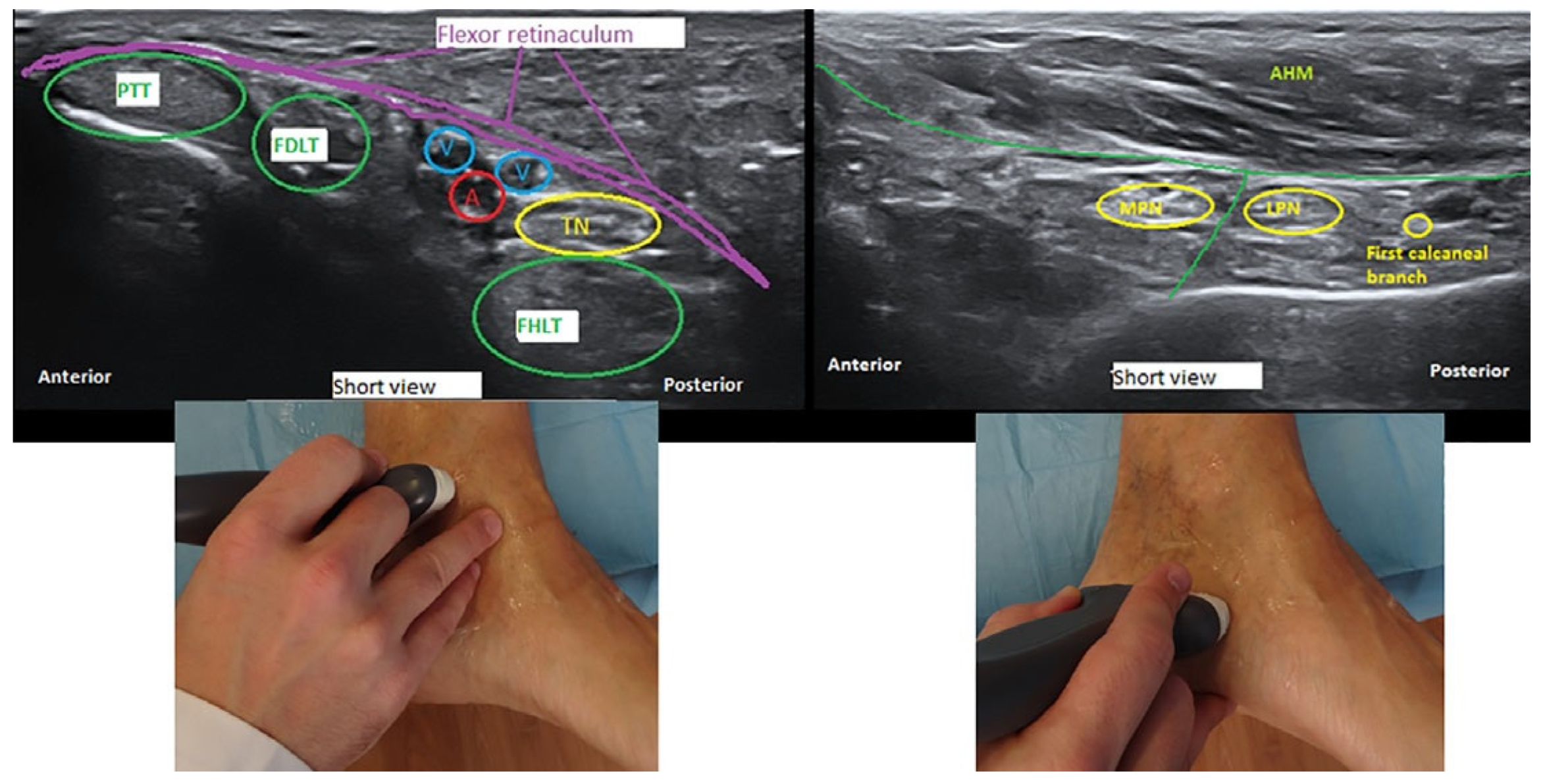
2.2.4. Ultrasound-Guided Near-Nerve Needle Sensory (USG-NNNS) Technique
2.3. Statistical Analysis
3. Results
3.1. Clinical Features
3.2. Electrophysiological Findings
3.2.1. Comparison between the Surface Electrode and USG-NNNS Techniques
3.2.2. Comparison between the Symptomatic Group and the Asymptomatic Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A
References
- Gould, J.S. Tarsal Tunnel Syndrome. Foot Ankle Clin. 2011, 16, 275–286. [Google Scholar] [CrossRef]
- Heimkes, B.; Posel, P.; Stotz, S.; Wolf, K. The proximal and distal tarsal tunnel syndromes. An anatomical study. Int. Orthop. 1987, 11, 193–196. [Google Scholar] [CrossRef] [PubMed]
- Granger, C.J.; Cohen-Levy, W.B. Anatomy, Bony Pelvis and Lower Limb, Posterior Tibial Nerve. 2020 Jul 27. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Delisa, J.A.; Saeed, M.A. The tarsal tunnel syndrome. Muscle Nerve 1983, 6, 664–670. [Google Scholar] [CrossRef] [PubMed]
- Doneddu, P.E.; Coraci, D.; Loreti, C.; Piccinini, G.; Padua, L. Tarsal tunnel syndrome: Still more opinions than evidence. Status of the art. Neurol. Sci. 2017, 38, 1735–1739. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.T.; Gaines, K.; Malamut, R.; Park, T.A.; Toro, D.R.; Holland, N. American Association of Neuromuscular and Electrodiagnostic Medicine. Usefulness of electrodiagnostic techniques in the evaluation of suspected tarsal tunnel syndrome: An evidence-based review. Muscle Nerve 2005, 32, 236–240. [Google Scholar] [CrossRef] [PubMed]
- Erickson, S.J.; Quinn, S.F.; Kneeland, J.B.; Smith, J.W.; Johnson, J.E.; Carrera, G.F.; Shereff, M.J.; Hyde, J.S.; Jesmanowicz, A. MR imaging of the tarsal tunnel and related spaces: Normal and abnormal findings with anatomic correlation. Am. J. Roentgenol. 1990, 155, 323–328. [Google Scholar] [CrossRef] [Green Version]
- Kerr, R.; Frey, C. MR Imaging in Tarsal Tunnel Syndrome. J. Comput. Assist. Tomogr. 1991, 15, 280–286. [Google Scholar] [CrossRef] [PubMed]
- Iborra, A.; Villanueva, M.; Sanz-Ruiz, P. Results of ultrasound-guided release of tarsal tunnel syndrome: A review of 81 cases with a minimum follow-up of 18 months. J. Orthop. Surg. Res. 2020, 15, 1–6. [Google Scholar] [CrossRef]
- Iborra, A.; Villanueva, M.; Barrett, S.L.; Rodriguez-Collazo, E.; Sanz, P. Anatomic Delineation of Tarsal Tunnel Innervation via Ultrasonography. J. Ultrasound Med. 2018, 37, 1325–1334. [Google Scholar] [CrossRef]
- Martinoli, C.; Bianchi, S.; Gandolfo, N.; Valle, M.; Simonetti, S.; Derchi, L.E. US of Nerve Entrapments in Osteofibrous Tunnels of the Upper and Lower Limbs. Radiographics 2000, 20, S199–S217. [Google Scholar] [CrossRef] [Green Version]
- Moroni, S.; Zwierzina, M.; Starke, V.; Moriggl, B.; Montesi, F.; Konschake, M. Clinical-anatomic mapping of the tarsal tunnel with regard to Baxter’s neuropathy in recalcitrant heel pain syndrome: Part I. Surg. Radiol. Anat. 2019, 41, 29–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schon, L.C.; Glennon, T.P.; Baxter, D.E. Heel Pain Syndrome: Electrodiagnostic Support for Nerve Entrapment. Foot Ankle 1993, 14, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Buchthal, F.; Rosenfalk, A. Evoked action potentials and conduction velocity in human sensory nerves. Brain Res. 1966, 3, 1–122. [Google Scholar] [CrossRef]
- Oh, S.J.; Kim, H.S.; Ahmad, B.K. The near-nerve sensory nerve conduction in tarsal tunnel syndrome. J. Neurol. Neurosurg. Psychiatry 1985, 48, 999–1003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oh, S.J.; Lee, K.W. Medial plantar neuropathy. Neurology 1987, 37, 1408–1410. [Google Scholar] [CrossRef] [PubMed]
- Oh, S.J. (Ed.) Uncommon Nerve Conduction Studies: Techniques and Normal Values. In Clinical Electromyography: Nerve Conduction Studies, 2nd ed.; Williams & Wilkins: Baltimore, MD, USA, 1993; pp. 149–276. [Google Scholar]
- Oh, S.J.; Kwon, K.H.; Hah, J.S.; Kim, D.E.; Demirci, M. Lateral plantar neuropathy. Muscle Nerve 1999, 22, 1234–1238. [Google Scholar] [CrossRef]
- Uluc, K.; Temucin, C.M.; Ozdamar, S.E.; Demirci, M.; Tan, E. Near-nerve needle sensory and medial plantar nerve conduction studies in patients with small-fiber sensory neuropathy. Eur. J. Neurol. 2008, 15, 928–932. [Google Scholar] [CrossRef]
- Preston, D.C.; Shapiro, B.E. Electromyography and Neuromuscular Disorders. Clinical-Electrophysiologic Correlations, 3rd ed.; Elsevier: London, UK, 2013. [Google Scholar]
- Trojaborg, W. Sensory Nerve Conduction, Near-Nerve Recording. In Methods in Clinical Neurophysiology, 2nd ed.; Buchthal, F., Ed.; Dantec: Danville, CA, USA, 1991; Volume 2, pp. 17–40. [Google Scholar]
- Oh, S.J.; Kim, H.S.; Ahmad, B.K. Electrophysiological diagnosis of interdigital neuropathy of the foot. Muscle Nerve 1984, 7, 218–225. [Google Scholar] [CrossRef]
- Rall, W. Membrane potential transients and membrane time constant of motoneurons. Exp. Neurol. 1960, 2, 503–532. [Google Scholar] [CrossRef]
- Pastor, J. Fundamentos biofísicos de la actividad neuronal. Rev. Neurol. 2000, 30, 741–755. [Google Scholar] [CrossRef]
- Holt, G.R.; Koch, C. Electrical Interactions via the Extracellular Potential Near Cell Bodies. J. Comput. Neurosci. 1999, 6, 169–184. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, M.; Tsang, K.; Mackenney, P.; Adedapo, A. Tarsal tunnel syndrome: A literature review. Foot Ankle Surg. 2012, 18, 149–152. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.N.; Jacobs, B.C.; Ashbaugh, S. Considerations in foot-wear and orthotics. Prim Care 2013, 40, 100. [Google Scholar] [CrossRef] [PubMed]
- Erlanger, J.; Gasser, H.S. Electrical Signs of Nervous Activity; University of Pennsylvania: Philadephia, PA, USA, 1937. [Google Scholar]
- Johnston, D.; Wu, S.M. Functional Properties of Dendrites. En Foundations of Cellular Neurophysiology; MIT Press: Cambridge, MA, USA, 2001. [Google Scholar]
- Shepherd, G.M. Electrotonic Properties of Axons and Dendrites. En: Fundamental Neuroscience; Squire, B., McConnell, R., Spitzer, Z., Eds.; Academic Press: Boston, MA, USA, 2003. [Google Scholar]
- Junge, D. Electrical Recordings from Nerves and Muscles. En: Nerve and Muscle Excitation, 3rd ed.; Sinauer Associates, Inc.: Sunderlands, MA, USA, 1992; pp. 1–17.9. [Google Scholar]
- Pastor, J.; Reina, M.A. Fisiología del Nervio Periférico Normal y Patológico. En: Complicaciones Neurológicas Asociadas con la Anestesia Regional Periférica y Central; Wikinski, J.A., Reina, M.Á., Bollini, C., De Andrés, J.A., Salas, X., Salgueiro, C., Aldrete, J.A., Eds.; Panamericana: Buenos Aires, Argentina, 2011; pp. 87–103. [Google Scholar]
- Kimura, J. Anatomy and physiology of peripheral nerve. In Electrodiganosis in Diseases of Nerve and Muscle: Principles and Practice, 4th ed.; Oxford University Press: Oxford, UK, 2013; pp. 63–91. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SE NCV | NNNS NCV | p Value | ||||
|---|---|---|---|---|---|---|
| Variables | Medial | Lateral | Medial | Lateral | Medial SE/NNNS | Lateral SE/NNNS |
| Amplitude (µV) | 0.98 ± 0.15 | 0.65 ± 0.09 | 1.40 ± 0.22 | 1.00 ± 0.11 | p = 0.191 * | p = 0.031 ** |
| SNCV (m/s) | 33.91 ± 0.69 | 36.73 ± 1.29 | 32.51 ± 0.51 | 32.14 ± 0.99 | p = 0.105 * | p = 0.012 ** |
| Duration (ms) | 2.04 ± 0.06 | 1.90 ± 0.09 | 4.3 ± 0.1 | 5.48 ± 0.29 | p = <0.001 ** | p = <0.001 ** |
| No response | 27 | 37 £ | 2 | 4 ¥ | ||
| MNC | Mixed NCV | |||
|---|---|---|---|---|
| Variables | Medial | Lateral | Medial | Lateral |
| Latency (ms) | 4.9 ± 0.1 | 5.3 ± 0.1 | 3.6 ± 0.1 | 3.9 ± 0.1 |
| Amplitude (µV) | 7.6 ±0.4 | 4.9 ± 0.3 | 3.0 ± 0.5 | 2.0 ± 0.1 |
| NCV (m/s) | 47.5 ± 0.8 | 46.6 ± 0.8 | 41.3 ± 0.1 | 41.7 ± 1.3 |
| Duration (ms) | 5.3 ± 0.1 | 5.11 ± 0.2 | 1.6 ± 0.02 | 1.7 ± 0.04 |
| No response (n) | 0 | 0 | 7 | 10 € |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vega-Zelaya, L.; Iborra, Á.; Villanueva, M.; Pastor, J.; Noriega, C. Ultrasound-Guided Near-Nerve Needle Sensory Technique for the Diagnosis of Tarsal Tunnel Syndrome. J. Clin. Med. 2021, 10, 3065. https://doi.org/10.3390/jcm10143065
Vega-Zelaya L, Iborra Á, Villanueva M, Pastor J, Noriega C. Ultrasound-Guided Near-Nerve Needle Sensory Technique for the Diagnosis of Tarsal Tunnel Syndrome. Journal of Clinical Medicine. 2021; 10(14):3065. https://doi.org/10.3390/jcm10143065
Chicago/Turabian StyleVega-Zelaya, Lorena, Álvaro Iborra, Manuel Villanueva, Jesús Pastor, and Concepción Noriega. 2021. "Ultrasound-Guided Near-Nerve Needle Sensory Technique for the Diagnosis of Tarsal Tunnel Syndrome" Journal of Clinical Medicine 10, no. 14: 3065. https://doi.org/10.3390/jcm10143065
APA StyleVega-Zelaya, L., Iborra, Á., Villanueva, M., Pastor, J., & Noriega, C. (2021). Ultrasound-Guided Near-Nerve Needle Sensory Technique for the Diagnosis of Tarsal Tunnel Syndrome. Journal of Clinical Medicine, 10(14), 3065. https://doi.org/10.3390/jcm10143065