
Early Bronchoscopy Improves Extubation Rates after Out-of-Hospital Cardiac Arrest: A Retrospective Cohort Analysis

 , , , ,
, , , ,
Abstract
:1. Introduction:
2. Materials and Methods
2.1. Study Population and Endpoints
2.2. Data Collection
2.3. Bronchoscopy
2.4. Statistical Analysis
3. Results
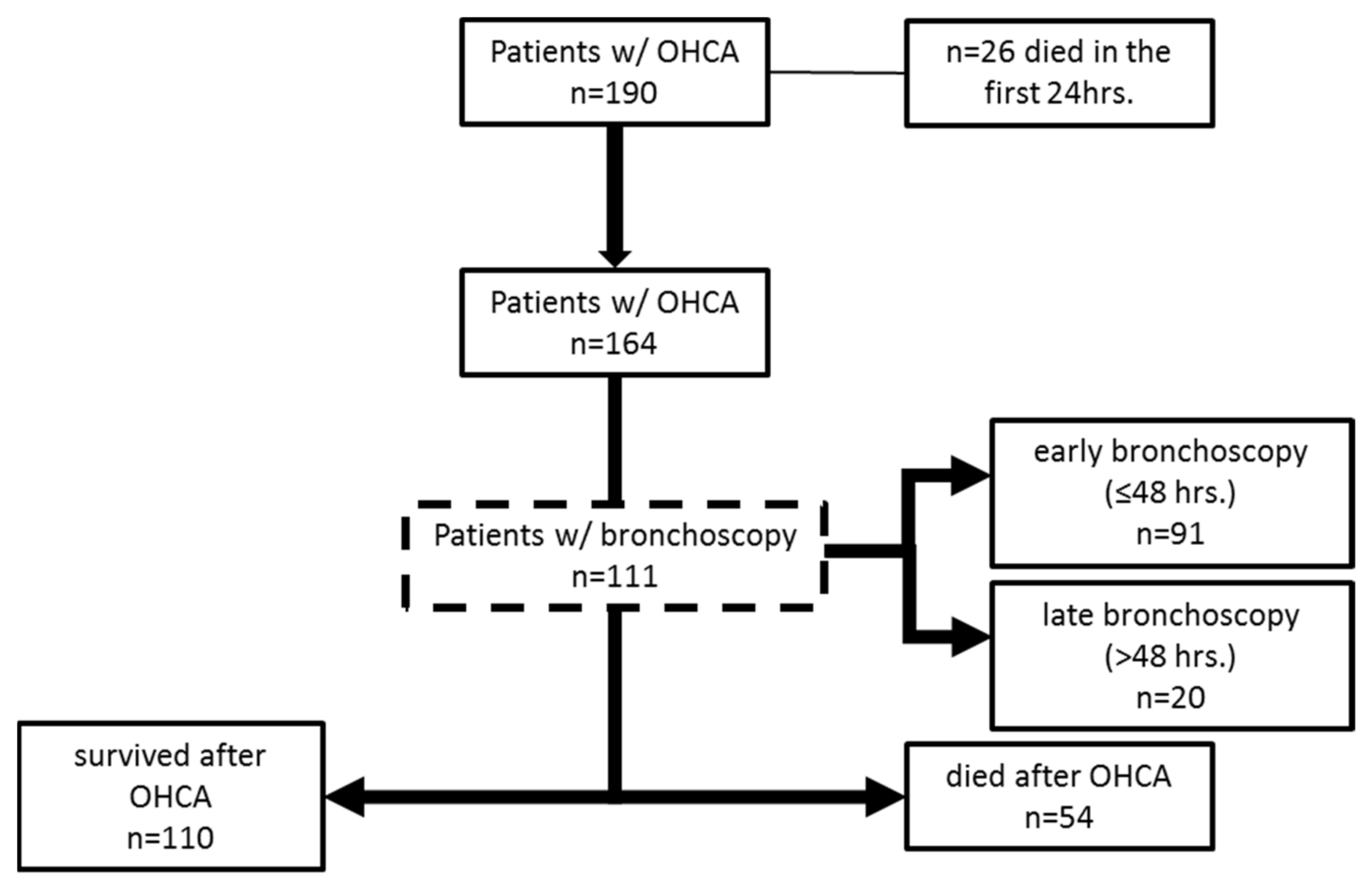
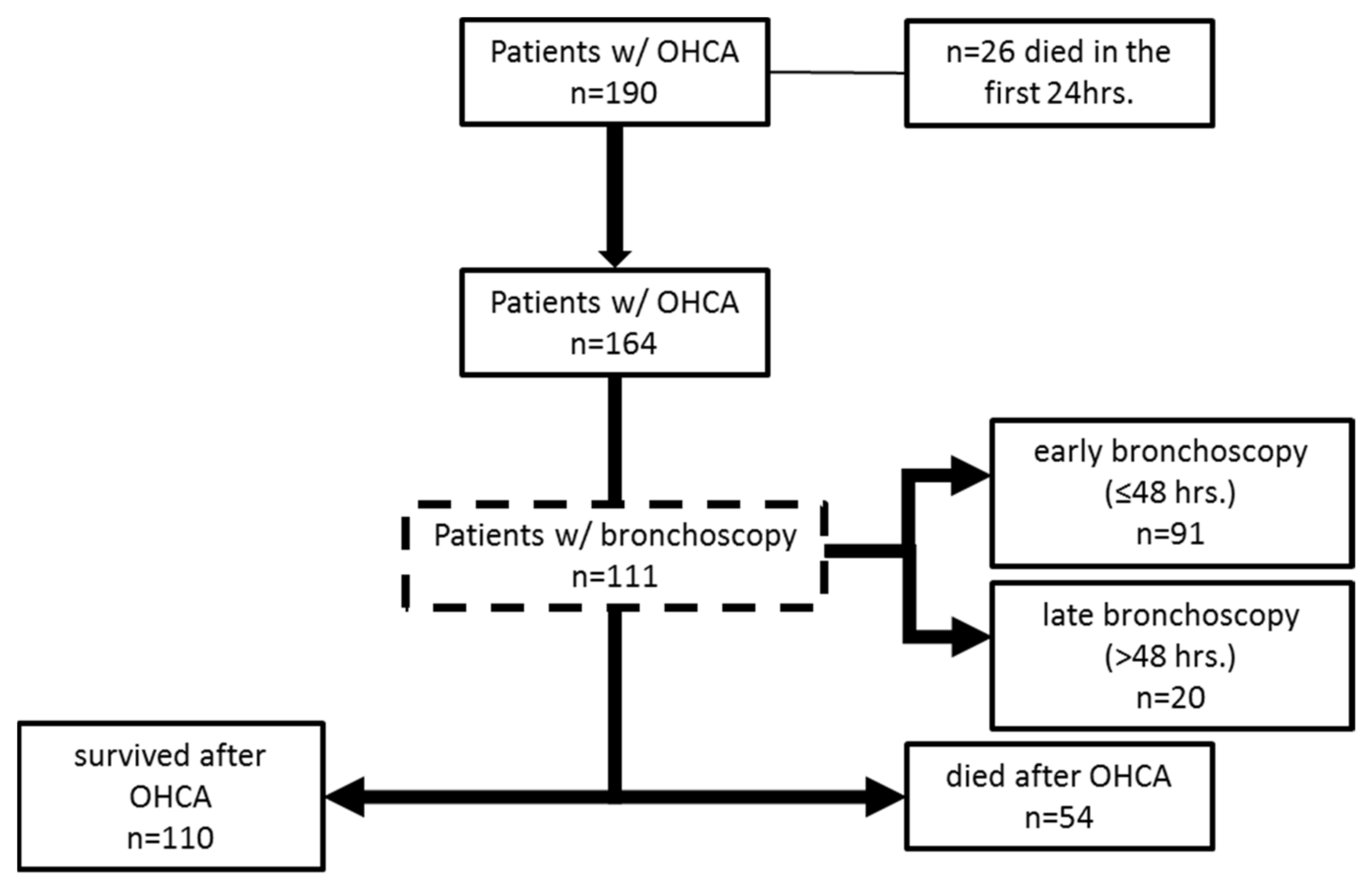
3.1. Patient Population
3.2. Outcome
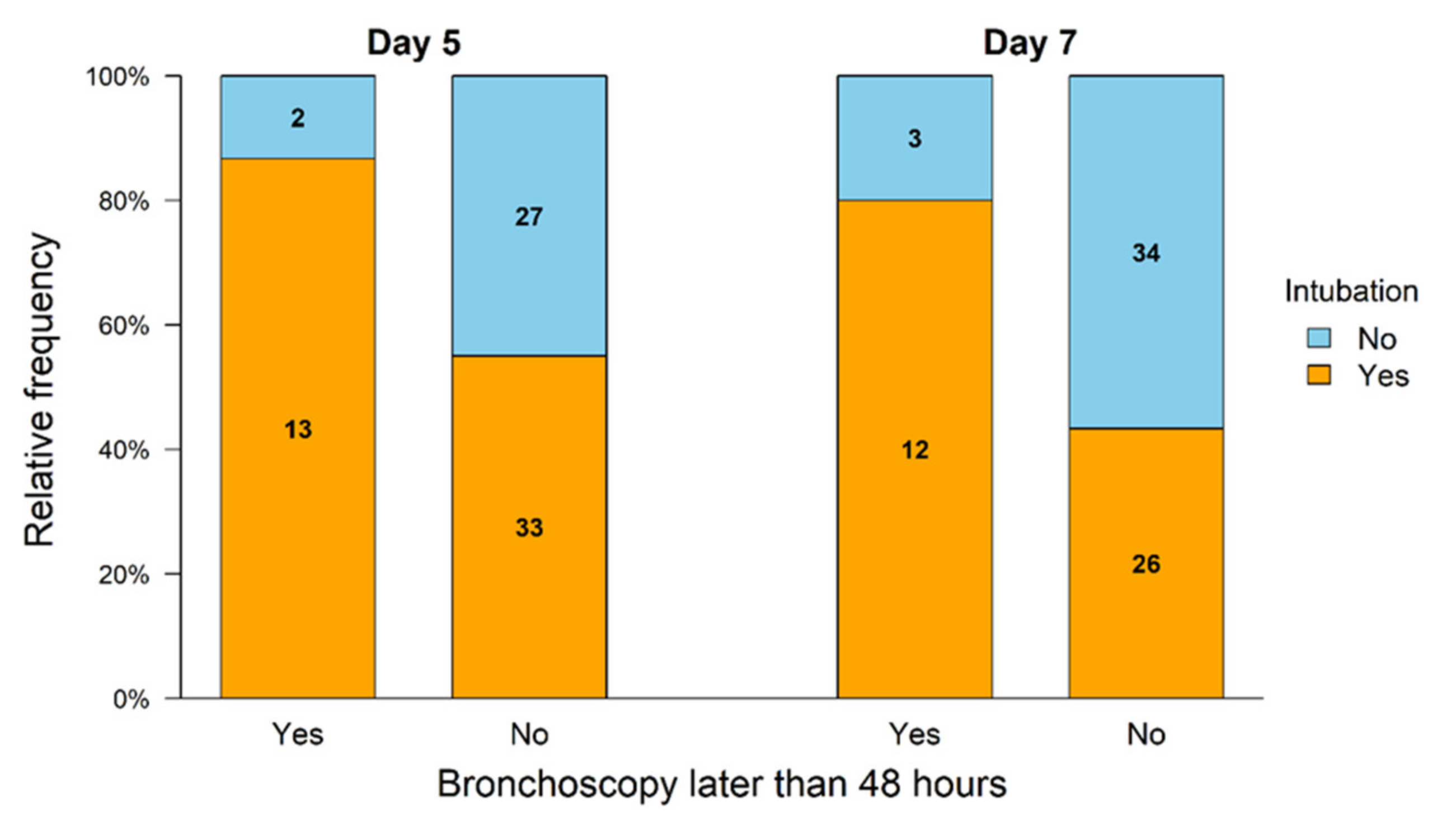
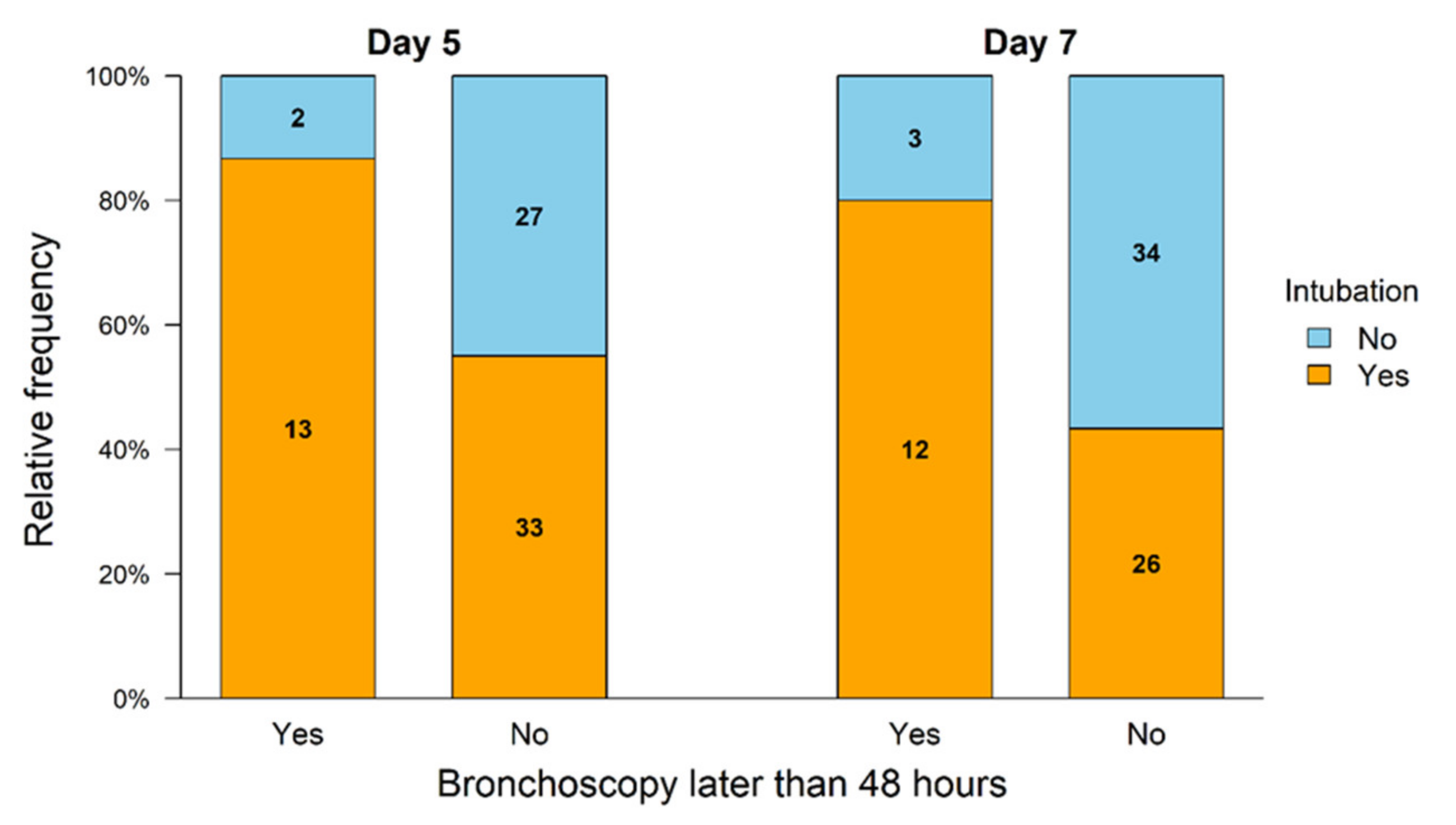
3.3. Bronchoscopy
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BAL | bronchoalveolar lavage |
| CPC | cerebral performance category scale |
| CPR | cardiopulmonary resuscitation |
| CRP | c-reactive protein |
| ER | emergency room |
| IL | interleukin |
| OHCA | out of hospital cardiac arrest |
| PCAS | post cardiac arrest syndrome |
| ROSC | return of spontaneous circulation |
References
- Peberdy, M.A.; Callaway, C.W.; Neumar, R.W.; Geocadin, R.G.; Zimmerman, J.L.; Donnino, M.; Gabrielli, A.; Silvers, S.M.; Zaritsky, A.L.; Merchant, R.; et al. Part 9: Post-cardiac arrest care: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2010, 122 (Suppl. S3), S768–S786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tagami, T.; Matsui, H.; Kuno, M.; Moroe, Y.; Kaneko, J.; Unemoto, K.; Fushimi, K.; Yasunaga, H. Early antibiotics administration during targeted temperature management after out-of-hospital cardiac arrest: A nationwide database study. BMC Anesthesiol. 2016, 16, 89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nolan, J.P.; Neumar, R.W.; Adrie, C.; Aibiki, M.; Berg, R.A.; Bottiger, B.W.; Callaway, C.; Clark, R.S.; Geocadin, R.G.; Jauch, E.C.; et al. Post-cardiac arrest syndrome: Epidemiology, pathophysiology, treatment, and prognostication. A Scientific Statement from the International Liaison Committee on Resuscitation; the American Heart Association Emergency Cardiovascular Care Committee; the Council on Cardiovascular Surgery and Anesthesia; the Council on Cardiopulmonary, Perioperative, and Critical Care; the Council on Clinical Cardiology; the Council on Stroke. Resuscitation 2008, 79, 350–379. [Google Scholar] [CrossRef]
- Perbet, S.; Mongardon, N.; Dumas, F.; Bruel, C.; Lemiale, V.; Mourvillier, B.; Carli, P.; Varenne, O.; Mira, J.P.; Wolff, M.; et al. Early-onset pneumonia after cardiac arrest: Characteristics, risk factors and influence on prognosis. Am. J. Respir. Crit. Care Med. 2011, 184, 1048–1054. [Google Scholar] [CrossRef] [PubMed]
- Pabst, D.; Romer, S.; Samol, A.; Kumpers, P.; Waltenberger, J.; Lebiedz, P. Predictors and outcome of early-onset pneumonia after out-of-hospital cardiac arrest. Respir. Care 2013, 58, 1514–1520. [Google Scholar] [CrossRef] [Green Version]
- Adrie, C.; Adib-Conquy, M.; Laurent, I.; Monchi, M.; Vinsonneau, C.; Fitting, C.; Fraisse, F.; Dinh-Xuan, A.T.; Carli, P.; Spaulding, C.; et al. Successful cardiopulmonary resuscitation after cardiac arrest as a “sepsis-like” syndrome. Circulation 2002, 106, 562–568. [Google Scholar] [CrossRef]
- Kakavas, S.; Mongardon, N.; Cariou, A.; Gulati, A.; Xanthos, T. Early-onset pneumonia after out-of-hospital cardiac arrest. J. Infect. 2015, 70, 553–562. [Google Scholar] [CrossRef]
- Vincent, J.L.; Rello, J.; Marshall, J.; Silva, E.; Anzueto, A.; Martin, C.D.; Moreno, R.; Lipman, J.; Gomersall, C.; Sakr, Y.; et al. International study of the prevalence and outcomes of infection in intensive care units. JAMA 2009, 302, 2323–2329. [Google Scholar] [CrossRef] [Green Version]
- Francois, B.; Cariou, A.; Clere-Jehl, R.; Dequin, P.F.; Renon-Carron, F.; Daix, T.; Guitton, C.; Deye, N.; Legriel, S.; Plantefeve, G.; et al. Prevention of Early Ventilator-Associated Pneumonia after Cardiac Arrest. N. Engl. J. Med. 2019, 381, 1831–1842. [Google Scholar] [CrossRef]
- Ribaric, S.F.; Turel, M.; Knafelj, R.; Gorjup, V.; Stanic, R.; Gradisek, P.; Cerovic, O.; Mirkovic, T.; Noc, M. Prophylactic versus clinically-driven antibiotics in comatose survivors of out-of-hospital cardiac arrest-A randomized pilot study. Resuscitation 2017, 111, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Gagnon, D.J.; Nielsen, N.; Fraser, G.L.; Riker, R.R.; Dziodzio, J.; Sunde, K.; Hovdenes, J.; Stammet, P.; Friberg, H.; Rubertsson, S.; et al. Prophylactic antibiotics are associated with a lower incidence of pneumonia in cardiac arrest survivors treated with targeted temperature management. Resuscitation 2015, 92, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Davies, K.J.; Walters, J.H.; Kerslake, I.M.; Greenwood, R.; Thomas, M.J. Early antibiotics improve survival following out-of hospital cardiac arrest. Resuscitation 2013, 84, 616–619. [Google Scholar] [CrossRef] [PubMed]
- Cummins, R.O.; Chamberlain, D.A.; Abramson, N.S.; Allen, M.; Baskett, P.J.; Becker, L.; Bossaert, L.; Delooz, H.H.; Dick, W.F.; Eisenberg, M.S.; et al. Recommended guidelines for uniform reporting of data from out-of-hospital cardiac arrest: The Utstein Style. A statement for health professionals from a task force of the American Heart Association, the European Resuscitation Council, the Heart and Stroke Foundation of Canada, and the Australian Resuscitation Council. Circulation 1991, 84, 960–975. [Google Scholar] [CrossRef] [Green Version]
- Solidoro, P.; Corbetta, L.; Patrucco, F.; Sorbello, M.; Piccioni, F.; D’Amato, L.; Renda, T.; Petrini, F. Competences in bronchoscopy for Intensive Care Unit, anesthesiology, thoracic surgery and lung transplantation. Panminerva Med. 2019, 61, 367–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perkins, G.D.; Jacobs, I.G.; Nadkarni, V.M.; Berg, R.A.; Bhanji, F.; Biarent, D.; Bossaert, L.L.; Brett, S.J.; Chamberlain, D.; de Caen, A.R.; et al. Cardiac Arrest and Cardiopulmonary Resuscitation Outcome Reports: Update of the Utstein Resuscitation Registry Templates for Out-of-Hospital Cardiac Arrest: A Statement for Healthcare Professionals From a Task Force of the International Liaison Committee on Resuscitation (American Heart Association, European Resuscitation Council, Australian and New Zealand Council on Resuscitation, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Council of Southern Africa, Resuscitation Council of Asia); and the American Heart Association Emergency Cardiovascular Care Committee and the Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation. Resuscitation 2015, 96, 328–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhuang, Y.G.; Chen, Y.Z.; Zhou, S.Q.; Peng, H.; Chen, Y.Q.; Li, D.J. High plasma levels of pro-inflammatory factors interleukin-17 and interleukin-23 are associated with poor outcome of cardiac-arrest patients: A single center experience. BMC Cardiovasc. Disord. 2020, 20, 170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Myat, A.; Song, K.J.; Rea, T. Out-of-hospital cardiac arrest: Current concepts. Lancet 2018, 391, 970–979. [Google Scholar] [CrossRef]
- Hellenkamp, K.; Onimischewski, S.; Kruppa, J.; Fasshauer, M.; Becker, A.; Eiffert, H.; Hunlich, M.; Hasenfuss, G.; Wachter, R. Early pneumonia and timing of antibiotic therapy in patients after nontraumatic out-of-hospital cardiac arrest. Crit. Care 2016, 20, 31. [Google Scholar] [CrossRef] [Green Version]
- Kilgannon, J.H.; Jones, A.E.; Parrillo, J.E.; Dellinger, R.P.; Milcarek, B.; Hunter, K.; Shapiro, N.I.; Trzeciak, S.; Emergency Medicine Shock Research Network, I. Relationship between supranormal oxygen tension and outcome after resuscitation from cardiac arrest. Circulation 2011, 123, 2717–2722. [Google Scholar] [CrossRef] [Green Version]
- Roman-Pognuz, E.; Elmer, J.; Guyette, F.X.; Poillucci, G.; Lucangelo, U.; Berlot, G.; Manganotti, P.; Peratoner, A.; Pellis, T.; Taccone, F.; et al. Multimodal Long-Term Predictors of Outcome in Out of Hospital Cardiac Arrest Patients Treated with Targeted Temperature Management at 36 degrees C. J. Clin. Med. 2021, 10, 1331. [Google Scholar] [CrossRef] [PubMed]
- Dumas, F.; Grimaldi, D.; Zuber, B.; Fichet, J.; Charpentier, J.; Pene, F.; Vivien, B.; Varenne, O.; Carli, P.; Jouven, X.; et al. Is hypothermia after cardiac arrest effective in both shockable and nonshockable patients?: Insights from a large registry. Circulation 2011, 123, 877–886. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raman, K.; Nailor, M.D.; Nicolau, D.P.; Aslanzadeh, J.; Nadeau, M.; Kuti, J.L. Early antibiotic discontinuation in patients with clinically suspected ventilator-associated pneumonia and negative quantitative bronchoscopy cultures. Crit. Care Med. 2013, 41, 1656–1663. [Google Scholar] [CrossRef] [PubMed]
- Bonten, M.J.; Bergmans, D.C.; Stobberingh, E.E.; van der Geest, S.; De Leeuw, P.W.; van Tiel, F.H.; Gaillard, C.A. Implementation of bronchoscopic techniques in the diagnosis of ventilator-associated pneumonia to reduce antibiotic use. Am. J. Respir. Crit. Care Med. 1997, 156, 1820–1824. [Google Scholar] [CrossRef]
- Woo, J.H.; Lim, Y.S.; Yang, H.J.; Park, W.B.; Cho, J.S.; Kim, J.J.; Hyun, S.Y.; Lee, G. Factors associated with pneumonia in post-cardiac arrest patients receiving therapeutic hypothermia. Am. J. Emerg. Med. 2014, 32, 150–155. [Google Scholar] [CrossRef]
- Callaway, C.W.; Donnino, M.W.; Fink, E.L.; Geocadin, R.G.; Golan, E.; Kern, K.B.; Leary, M.; Meurer, W.J.; Peberdy, M.A.; Thompson, T.M.; et al. Part 8: Post-Cardiac Arrest Care: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2015, 132 (Suppl. S2), S465–S482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bro-Jeppesen, J.; Kjaergaard, J.; Stammet, P.; Wise, M.P.; Hovdenes, J.; Aneman, A.; Horn, J.; Devaux, Y.; Erlinge, D.; Gasche, Y.; et al. Predictive value of interleukin-6 in post-cardiac arrest patients treated with targeted temperature management at 33 degrees C or 36 degrees C. Resuscitation 2016, 98, 1–8. [Google Scholar] [CrossRef]
- Timmermann, A.; Russo, S.G.; Eich, C.; Roessler, M.; Braun, U.; Rosenblatt, W.H.; Quintel, M. The out-of-hospital esophageal and endobronchial intubations performed by emergency physicians. Anesth. Analg. 2007, 104, 619–623. [Google Scholar] [CrossRef]
- Hernandez Padilla, A.C.; Trampont, T.; Lafon, T.; Daix, T.; Cailloce, D.; Barraud, O.; Dalmay, F.; Vignon, P.; Francois, B. Is prehospital endobronchial intubation a risk factor for subsequent ventilator associated pneumonia? A retrospective analysis. PLoS ONE 2019, 14, e0217466. [Google Scholar] [CrossRef]
- Fordyce, C.B.; Katz, J.N.; Alviar, C.L.; Arslanian-Engoren, C.; Bohula, E.A.; Geller, B.J.; Hollenberg, S.M.; Jentzer, J.C.; Sims, D.B.; Washam, J.B.; et al. Prevention of Complications in the Cardiac Intensive Care Unit: A Scientific Statement From the American Heart Association. Circulation 2020, 142, e379–e406. [Google Scholar] [CrossRef]
- Geurts, M.; Macleod, M.R.; Kollmar, R.; Kremer, P.H.; van der Worp, H.B. Therapeutic hypothermia and the risk of infection: A systematic review and meta-analysis. Crit. Care Med. 2014, 42, 231–242. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| All Patients n (%) | Survivors n (%) | Non-Survivor n (%) | p-Value | |
|---|---|---|---|---|
| Patients | 164 | 110 | 54 | |
| Female | 41 (25.0) | 22 (20.0) | 19 (35.2) | 0.035 |
| Age (years) | 64.9 ± 15.0 | 62.1 ± 14.6 | 70.8 ± 14.2 | <0.000 |
| Ongoing CPR on admission | 14 (8.5) | 7 (6.4) | 7 (13.0) | 0.155 |
| Shockable rhythm | 107 (65.2) | 81 (73.6) | 36 (66.6) | 0.001 |
| Cause of OHCA | ||||
| Myocardial ischemia | 91 (55.5) | 66 (60.0) | 25 (46.3) | 0.097 |
| Pulmonary embolism | 7 (4.3) | 3 (2.7) | 4 (7.4) | 0.163 |
| Rhythm event | 18 (11.0) | 13 (11.8) | 5 (9.3) | 0.622 |
| Unknown/other | 48 (29.3) | 28 (25.5) | 20 (37.0) | 0.162 |
| Time to ROSC (min) | 17.6 ± 15.8 | 15.0 ± 14.1 | 23.7 ± 17.8 | 0.012 |
| CPC Score at Discharge | n | % | Age (Years) |
|---|---|---|---|
| CPC 1 | 56 | 52.8 | 60.0 ± 13.0 |
| CPC 2 | 14 | 13.2 | 63.8 ± 16.4 |
| CPC 3 | 28 | 26.4 | 67.7 ± 15.5 |
| CPC 4 | 8 | 7.5 | 58.5 ± 15.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zimmermann, G.S.; Palm, J.; Lahmann, A.L.; Peltz, F.; Okrojek, R.; Weis, F.; Müller, A.; Ziegler, T.; Steger, A.; Haller, B.; et al. Early Bronchoscopy Improves Extubation Rates after Out-of-Hospital Cardiac Arrest: A Retrospective Cohort Analysis. J. Clin. Med. 2021, 10, 3055. https://doi.org/10.3390/jcm10143055
Zimmermann GS, Palm J, Lahmann AL, Peltz F, Okrojek R, Weis F, Müller A, Ziegler T, Steger A, Haller B, et al. Early Bronchoscopy Improves Extubation Rates after Out-of-Hospital Cardiac Arrest: A Retrospective Cohort Analysis. Journal of Clinical Medicine. 2021; 10(14):3055. https://doi.org/10.3390/jcm10143055
Chicago/Turabian StyleZimmermann, Gregor S., Jana Palm, Anna Lena Lahmann, Friedhelm Peltz, Rainer Okrojek, Florian Weis, Arne Müller, Tilman Ziegler, Alexander Steger, Bernhard Haller, and et al. 2021. "Early Bronchoscopy Improves Extubation Rates after Out-of-Hospital Cardiac Arrest: A Retrospective Cohort Analysis" Journal of Clinical Medicine 10, no. 14: 3055. https://doi.org/10.3390/jcm10143055
APA StyleZimmermann, G. S., Palm, J., Lahmann, A. L., Peltz, F., Okrojek, R., Weis, F., Müller, A., Ziegler, T., Steger, A., Haller, B., Hoppmann, P., Laugwitz, K.-L., & Hautmann, H. (2021). Early Bronchoscopy Improves Extubation Rates after Out-of-Hospital Cardiac Arrest: A Retrospective Cohort Analysis. Journal of Clinical Medicine, 10(14), 3055. https://doi.org/10.3390/jcm10143055