
Differential Factors for Predicting Outcomes in Left Main versus Non-Left Main Coronary Bifurcation Stenting

 ,
,  , , , , ,
, , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Percutaneous Coronary Bifurcation Intervention
2.3. Data Collection and Quantitative Coronary Angiography Analysis
2.4. Primary and Secondary Outcomes
2.5. Statistical Analysis
3. Results
3.1. Baseline Clinical Characteristics
3.2. Lesion and Procedural Characteristics
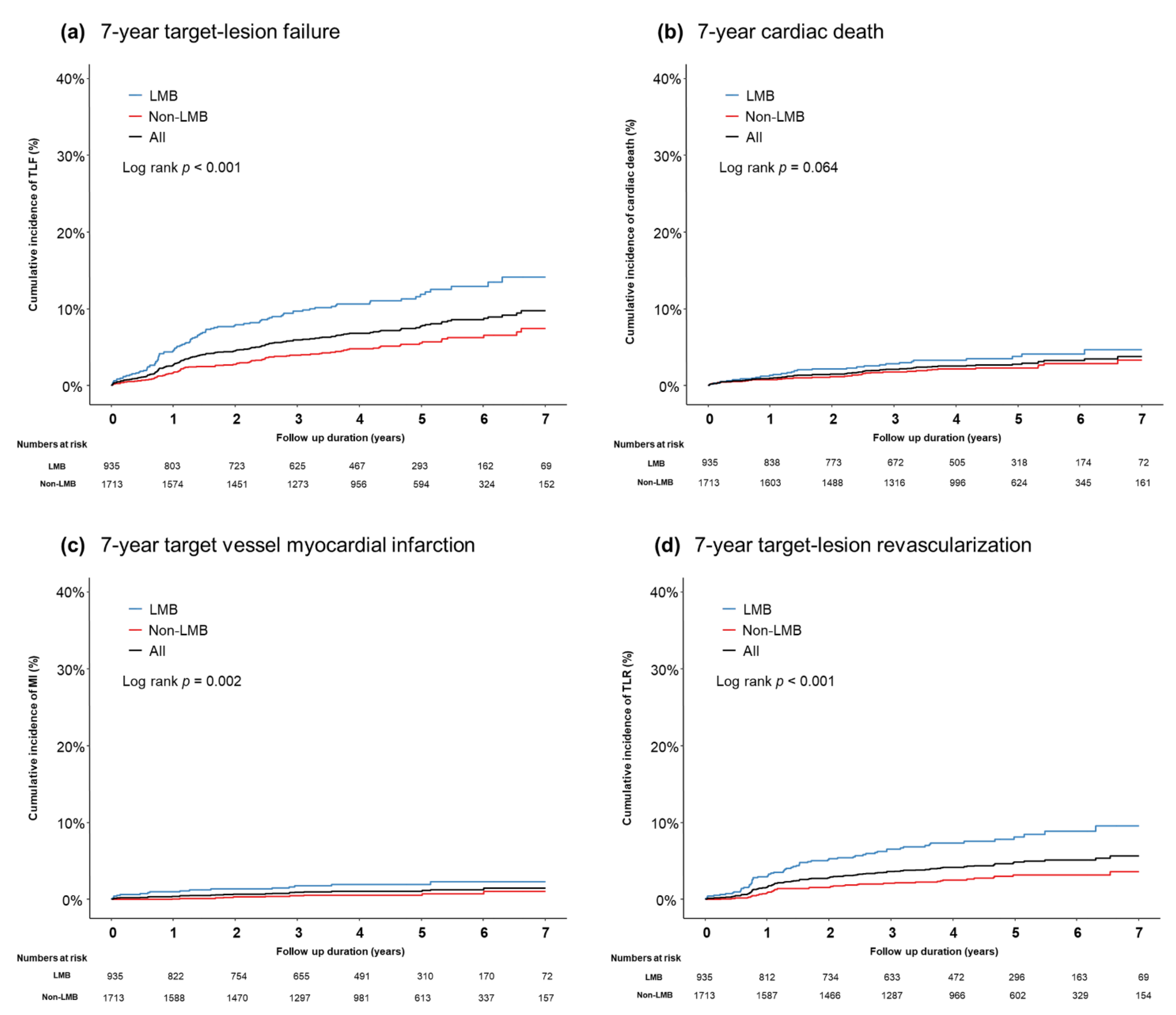
3.3. Clinical Outcomes
3.4. Independent Predictors for TLF
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stone, G.W.; Midei, M.; Newman, W.; Sanz, M.; Hermiller, J.B.; Williams, J.; Farhat, N.; Caputo, R.; Xenopoulos, N.; Applegate, R.; et al. Randomized comparison of everolimus-eluting and paclitaxel-eluting stents: Two-year clinical follow-up from the Clinical Evaluation of the Xience V Everolimus Eluting Coronary Stent System in the Treatment of Patients with de novo Native Coronary Artery Lesions (SPIRIT) III trial. Circulation 2009, 119, 680–686. [Google Scholar] [CrossRef]
- Kaiser, C.; Galatius, S.; Erne, P.; Eberli, F.; Alber, H.; Rickli, H.; Pedrazzini, G.; Hornig, B.; Bertel, O.; Bonetti, P.; et al. Drug-eluting versus bare-metal stents in large coronary arteries. N. Engl. J. Med. 2010, 363, 2310–2319. [Google Scholar] [CrossRef] [PubMed]
- Palmerini, T.; Biondi-Zoccai, G.; Della Riva, D.; Mariani, A.; Sabaté, M.; Smits, P.C.; Kaiser, C.; D’Ascenzo, F.; Frati, G.; Mancone, M.; et al. Clinical outcomes with bioabsorbable polymer- versus durable polymer-based drug-eluting and bare-metal stents: Evidence from a comprehensive network meta-analysis. J. Am. Coll. Cardiol. 2014, 63, 299–307. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.M.; Hahn, J.-Y.; Kang, J.; Park, K.W.; Chun, W.J.; Rha, S.W.; Yu, C.W.; Jeong, J.O.; Jeong, M.H.; Yoon, J.H.; et al. Differential Prognostic Effect Between First- and Second-Generation Drug-Eluting Stents in Coronary Bifurcation Lesions: Patient-Level Analysis of the Korean Bifurcation Pooled Cohorts. JACC Cardiovasc. Interv. 2015, 8, 1318–1331. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.H.; Song, Y.B.; Lee, J.M.; Park, T.K.; Yang, J.H.; Hahn, J.-Y.; Choi, J.-H.; Choi, S.-H.; Kim, H.-S.; Chun, W.J.; et al. Prognostic Effects of Treatment Strategies for Left Main Versus Non-Left Main Bifurcation Percutaneous Coronary Intervention With Current-Generation Drug-Eluting Stent. Circ. Cardiovasc. Interv. 2020, 13, e008543. [Google Scholar] [CrossRef]
- McCaffrey, D.F.; Griffin, B.A.; Almirall, D.; Slaughter, M.E.; Ramchand, R.; Burgette, L.F. A tutorial on propensity score estimation for multiple treatments using generalized boosted models. Stat. Med. 2013, 32, 3388–3414. [Google Scholar] [CrossRef]
- Park, T.K.; Park, Y.H.; Song, Y.B.; Oh, J.H.; Chun, W.J.; Kang, G.H.; Jang, W.J.; Hahn, J.Y.; Yang, J.H.; Choi, S.H.; et al. Long-Term Clinical Outcomes of True and Non-True Bifurcation Lesions According to Medina Classification- Results From the COBIS (COronary BIfurcation Stent) II Registry. Circ. J. 2015, 79, 1954–1962. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.B.; Hahn, J.Y.; Yang, J.H.; Choi, S.-H.; Choi, J.-H.; Lee, S.H.; Jeong, M.-H.; Kim, H.-S.; Lee, J.-H.; Yu, C.W.; et al. Differential prognostic impact of treatment strategy among patients with left main versus non-left main bifurcation lesions undergoing percutaneous coronary intervention: Results from the COBIS (Coronary Bifurcation Stenting) Registry II. JACC Cardiovasc. Interv. 2014, 7, 255–263. [Google Scholar] [CrossRef]
- Diletti, R.; Garcia-Garcia, H.M.; Bourantas, C.V.; van Geuns, R.J.; Van Mieghem, N.M.; Vranckx, P.; Zhang, Y.-J.; Farooq, V.; Iqbal, J.; Wykrzykowska, J.J.; et al. Clinical outcomes after zotarolimus and everolimus drug eluting stent implantation in coronary artery bifurcation lesions: Insights from the RESOLUTE All Comers Trial. Heart 2013, 99, 1267–1274. [Google Scholar] [CrossRef][Green Version]
- Chen, S.-L.; Santoso, T.; Zhang, J.-J.; Ye, F.; Xu, Y.-W.; Fu, Q.; Kan, J.; Paiboon, C.; Zhou, Y.; Ding, S.-Q.; et al. A randomized clinical study comparing double kissing crush with provisional stenting for treatment of coronary bifurcation lesions: Results from the DKCRUSH-II (Double Kissing Crush versus Provisional Stenting Technique for Treatment of Coronary Bifurcation Lesions) trial. J. Am. Coll. Cardiol. 2011, 57, 914–920. [Google Scholar] [CrossRef] [PubMed]
- Moussa, I.D. Coronary artery bifurcation interventions: The disconnect between randomized clinical trials and patient centered decision-making. Catheter. Cardiovasc. Interv. 2011, 77, 537–545. [Google Scholar] [CrossRef]
- Sgueglia, G.A.; Chevalier, B. Kissing balloon inflation in percutaneous coronary interventions. JACC Cardiovasc. Interv. 2012, 5, 803–811. [Google Scholar] [CrossRef]
- Writing Committee Members; Levine, G.N.; Bates, E.R.; Blankenship, J.C.; Bailey, S.R.; Bittl, J.A.; Cercek, B.; Chambers, C.E.; Ellis, S.G.; Guyton, R.A.; et al. ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention: Executive summary: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Circulation 2011, 124, 2574–2609. [Google Scholar] [CrossRef]
- Neumann, F.-J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.-P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef]
- Džavík, V.; Kaul, U.; Guagliumi, G.; Chevalier, B.; Smits, P.C.; Stuteville, M.; Li, D.; Sudhir, K.; Grube, E. Two-year outcomes after deployment of XIENCE V everolimus-eluting stents in patients undergoing percutaneous coronary intervention of bifurcation lesions: A report from the SPIRIT V single arm study. Catheter. Cardiovasc. Interv. 2013, 82, E163–E172. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Salmerón, R.J.; Valenzuela, L.F.; Pérez, I.; Fuentes, M.; Rodríguez-Leiras, S.; Vizcaíno, M.; Carrascosa, C.; Marcos, F. Approach to coronary bifurcation lesions using the everolimus-eluting stent: Comparison between a simple strategy and a complex strategy with T-stenting. Rev. Esp. Cardiol. (Engl. Ed.) 2013, 66, 636–643. [Google Scholar] [CrossRef] [PubMed]
- Kumsars, I.; Holm, N.R.; Niemelä, M.; Erglis, A.; Kervinen, K.; Christiansen, E.H.; Maeng, M.; Dombrovskis, A.; Abraitis, V.; Kibarskis, A.; et al. Randomised comparison of provisional side branch stenting versus a two-stent strategy for treatment of true coronary bifurcation lesions involving a large side branch: The Nordic-Baltic Bifurcation Study IV. Open Heart 2020, 7, e000947. [Google Scholar] [CrossRef] [PubMed]
- Ragosta, M.; Dee, S.; Sarembock, I.J.; Lipson, L.C.; Gimple, L.W.; Powers, E.R. Prevalence of unfavorable angiographic characteristics for percutaneous intervention in patients with unprotected left main coronary artery disease. Catheter. Cardiovasc. Interv. 2006, 68, 357–362. [Google Scholar] [CrossRef]
- McDaniel, M.C.; Eshtehardi, P.; Sawaya, F.J.; Douglas, J.S., Jr.; Samady, H. Contemporary clinical applications of coronary intravascular ultrasound. JACC Cardiovasc. Interv. 2011, 4, 1155–1167. [Google Scholar] [CrossRef]
- Kandzari, D.E.; Gershlick, A.H.; Serruys, P.W.; Leon, M.B.; Morice, M.-C.; Simonton, C.A.; Lembo, N.J.; Banning, A.P.; Merkely, B.; van Boven, A.J.; et al. Outcomes Among Patients Undergoing Distal Left Main Percutaneous Coronary Intervention. Circ. Cardiovasc. Interv. 2018, 11, e007007. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.-L.; Zhang, J.-J.; Han, Y.; Kan, J.; Chen, L.; Qiu, C.; Jiang, T.; Tao, L.; Zeng, H.; Li, L.; et al. Double Kissing Crush Versus Provisional Stenting for Left Main Distal Bifurcation Lesions: DKCRUSH-V Randomized Trial. J. Am. Coll. Cardiol. 2017, 70, 2605–2617. [Google Scholar] [CrossRef] [PubMed]
- Kereiakes, D.J.; Young, J.J. Percutaneous coronary revascularization of diabetic patients in the era of drug-eluting stents. Rev. Cardiovasc. Med. 2005, 6, S48–S58. [Google Scholar] [PubMed]
- Hong, S.J.; Kim, M.H.; Ahn, T.H.; Ahn, Y.K.; Bae, J.H.; Shim, W.J.; Ro, Y.M.; Lim, D.S. Multiple predictors of coronary restenosis after drug-eluting stent implantation in patients with diabetes. Heart 2006, 92, 1119–1124. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Overall | Non-LMB | LMB | p | |
|---|---|---|---|---|
| (n = 2648) | (n = 1713) | (n = 935) | ||
| Age (years) | 63.7 ± 11.0 | 62.8 ± 11.1 | 65.5 ± 10.7 | <0.001 |
| The elderly (≥75 years old), n (%) | 462 (17.4) | 278 (16.2) | 184 (19.7) | 0.029 |
| Male, n (%) | 2013 (76.0) | 1302 (76.0) | 711 (76.0) | >0.999 |
| Hypertension, n (%) | 1504 (56.8) | 947 (55.3) | 557 (59.6) | 0.037 |
| Diabetes mellitus, n (%) | 905 (34.2) | 549 (32.0) | 356 (38.1) | 0.002 |
| Dyslipidemia, n (%) | 1009 (38.1) | 648 (37.8) | 361 (38.6) | 0.724 |
| Chronic Kidney Disease, n (%) | 103 (3.9) | 56 (3.3) | 47 (5.0) | 0.033 |
| Current smoker, n (%) | 798 (30.1) | 572 (33.4) | 226 (24.2) | <0.001 |
| Family Hx of CAD, n (%) | 83 (3.1) | 56 (3.3) | 27 (2.9) | 0.673 |
| Previous MI, n (%) | 113 (4.3) | 65 (3.8) | 48 (5.1) | 0.126 |
| Previous PCI, n (%) | 323 (12.2) | 164 (9.6) | 159 (17.0) | <0.001 |
| Previous stroke, n (%) | 177 (6.7) | 101 (5.9) | 76 (8.1) | 0.034 |
| Clinical presentations | 0.272 | |||
| Stable angina, n (%) | 1029 (38.9) | 652 (38.1) | 377 (40.3) | |
| Acute coronary syndrome, n (%) | 1619 (61.1) | 1061 (61.9) | 558 (59.7) | |
| LV ejection fraction (%) | 58.6 ± 9.9 | 58.8 ± 9.6 | 58.3 ± 10.3 | 0.208 |
| Reduced LV function (LVEF ≤ 40%), n (%) | 117 (4.4) | 66 (3.9) | 51 (5.5) | 0.069 |
| Overall | Non-LMB | LMB | p | |
|---|---|---|---|---|
| (n = 2648) | (n = 1713) | (n = 935) | ||
| Multi-vessel disease, n (%) | 1647 (62.2) | 873 (51.0) | 774 (82.8) | <0.001 |
| Location of bifurcated vessel, n (%) | <0.001 | |||
| LAD | 1208 (45.6) | 1208 (70.5) | 0 (0.0) | |
| LCX | 350 (13.2) | 350 (20.4) | 0 (0.0) | |
| LM | 935 (35.3) | 0 (0.0) | 935 (100.0) | |
| RCA | 155 (5.9) | 155 (9.0) | 0 (0.0) | |
| Medina classification, n (%) | <0.001 | |||
| 0.0.1 | 95 (3.6) | 39 (2.3) | 56 (6.0) | |
| 0.1.0 | 575 (21.7) | 291 (17.0) | 284 (30.4) | |
| 0.1.1 | 248 (9.4) | 175 (10.2) | 73 (7.8) | |
| 1.0.0 | 296 (11.2) | 212 (12.4) | 84 (9.0) | |
| 1.0.1 | 168 (6.3) | 130 (7.6) | 38 (4.1) | |
| 1.1.0 | 427 (16.1) | 248 (14.5) | 179 (19.1) | |
| 1.1.1 | 839 (31.7) | 618 (36.1) | 221 (23.6) | |
| True bifurcation, n (%) | 1255 (47.4) | 923 (53.9) | 332 (35.5) | <0.001 |
| Stent Technique, n (%) | <0.001 | |||
| Simple Crossover | 1685 (63.6) | 1196 (69.8) | 489 (52.3) | |
| 1 stent with SB Balloon | 475 (17.9) | 300 (17.5) | 175 (18.7) | |
| Classic Crush | 99 (3.7) | 32 (1.9) | 67 (7.2) | |
| Balloon Crush | 65 (2.5) | 37 (2.2) | 28 (3.0) | |
| Mini Crush | 80 (3.0) | 33 (1.9) | 47 (5.0) | |
| Culotte | 31 (1.2) | 15 (0.9) | 16 (1.7) | |
| TAP | 74 (2.8) | 30 (1.8) | 44 (4.7) | |
| Classic T | 51 (1.9) | 35 (2.0) | 16 (1.7) | |
| Kissing Stent | 41 (1.5) | 15 (0.9) | 26 (2.8) | |
| Others | 47 (1.8) | 20 (1.2) | 27 (2.9) | |
| 2-stenting strategy, n (%) | 454 (17.1) | 201 (11.7) | 253 (27.1) | <0.001 |
| No. of stents | 1.79 ± 0.97 | 1.72 ± 0.95 | 1.93 ± 1.00 | <0.001 |
| Transradial approach, n (%) | 1507 (56.9) | 1035 (60.4) | 472 (50.5) | <0.001 |
| IVUS-guidance PCI, n (%) | 1054 (39.8) | 460 (26.9) | 594 (63.5) | <0.001 |
| Rotablator, n (%) | 16 (0.6) | 5 (0.3) | 11 (1.2) | 0.011 |
| Cutting balloon, n (%) | 50 (1.9) | 6 (0.4) | 44 (4.7) | <0.001 |
| NC balloon, n (%) | 534 (20.2) | 285 (16.6) | 249 (26.6) | <0.001 |
| FKB, n (%) | 789 (29.8) | 393 (22.9) | 396 (42.4) | <0.001 |
| POT, n (%) | 739 (27.9) | 446 (26.0) | 293 (31.3) | 0.004 |
| Re-POT, n (%) | 123 (4.6) | 50 (2.9) | 73 (7.8) | <0.001 |
| Maximal diameter of MV stents (mm) | 3.13 ± 0.65 | 2.99 ± 0.62 | 3.39 ± 0.62 | <0.001 |
| Minimal diameter of MV stents (mm) | 3.05 ± 0.63 | 2.93 ± 0.61 | 3.26 ± 0.62 | <0.001 |
| Cumulative length of MV stents (mm) | 28.89 ± 13.66 | 28.55 ± 12.63 | 29.51 ± 15.35 | 0.101 |
| Crude HR | Adjusted HR | 95% CI | p Value | |
|---|---|---|---|---|
| All patients (n = 2648) | ||||
| The elderly (≥75 years old) | 1.60 | 1.47 | 1.02–2.10 | 0.038 |
| Chronic kidney disease | 4.35 | 3.06 | 1.88–4.96 | <0.001 |
| Reduced LVEF (EF ≤ 40%) | 3.51 | 3.07 | 1.91–4.93 | <0.001 |
| Left main bifurcation PCI | 2.24 | 2.06 | 1.42–2.99 | <0.001 |
| Two-stenting strategy (vs. provisional) | 1.92 | 1.54 | 0.97–2.45 | 0.068 |
| Left main bifurcation group (n = 935) | ||||
| Chronic kidney disease | 4.41 | 4.06 | 2.15–7.66 | <0.001 |
| Reduced LVEF (EF ≤ 40%) | 2.98 | 3.05 | 1.55–5.99 | <0.001 |
| Two-stenting strategy (vs provisional) | 1.88 | 2.01 | 1.11–3.64 | 0.021 |
| Non-left main bifurcation group (n = 1713) | ||||
| The elderly (≥75 years old) | 2.30 | 2.21 | 1.33–3.67 | 0.002 |
| Diabetes mellitus | 1.97 | 1.71 | 1.09–2.69 | 0.020 |
| Chronic kidney disease | 3.71 | 2.49 | 1.13–5.48 | 0.024 |
| Reduced LVEF (EF ≤ 40%) | 3.87 | 3.67 | 1.83–7.34 | <0.001 |
| Two-stenting strategy (vs provisional) | 1.17 | 1.15 | 0.50–2.63 | 0.738 |
| Maximal diameter of MV stents (mm) | 0.73 | 0.72 | 0.54–0.96 | 0.024 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cha, J.-J.; Hong, S.J.; Joo, H.J.; Park, J.H.; Yu, C.W.; Ahn, T.H.; Kim, H.-S.; Chun, W.J.; Hur, S.-H.; Han, S.H.; et al. Differential Factors for Predicting Outcomes in Left Main versus Non-Left Main Coronary Bifurcation Stenting. J. Clin. Med. 2021, 10, 3024. https://doi.org/10.3390/jcm10143024
Cha J-J, Hong SJ, Joo HJ, Park JH, Yu CW, Ahn TH, Kim H-S, Chun WJ, Hur S-H, Han SH, et al. Differential Factors for Predicting Outcomes in Left Main versus Non-Left Main Coronary Bifurcation Stenting. Journal of Clinical Medicine. 2021; 10(14):3024. https://doi.org/10.3390/jcm10143024
Chicago/Turabian StyleCha, Jung-Joon, Soon Jun Hong, Hyung Joon Joo, Jae Hyoung Park, Cheol Woong Yu, Tae Hoon Ahn, Hyo-Soo Kim, Woo Jung Chun, Seung-Ho Hur, Seung Hwan Han, and et al. 2021. "Differential Factors for Predicting Outcomes in Left Main versus Non-Left Main Coronary Bifurcation Stenting" Journal of Clinical Medicine 10, no. 14: 3024. https://doi.org/10.3390/jcm10143024
APA StyleCha, J.-J., Hong, S. J., Joo, H. J., Park, J. H., Yu, C. W., Ahn, T. H., Kim, H.-S., Chun, W. J., Hur, S.-H., Han, S. H., Rha, S.-W., Chae, I.-H., Jeong, J.-O., Heo, J. H., Yoon, J., Choi, K. H., Song, Y. B., Gwon, H.-C., Park, J.-S., ... Lim, D.-S. (2021). Differential Factors for Predicting Outcomes in Left Main versus Non-Left Main Coronary Bifurcation Stenting. Journal of Clinical Medicine, 10(14), 3024. https://doi.org/10.3390/jcm10143024