
Biocompatibility Parameters with Standard and Increased Dose of Citrate in Hemodialysis—A Randomized Trial




Abstract
:1. Introduction
2. Patients and Methods
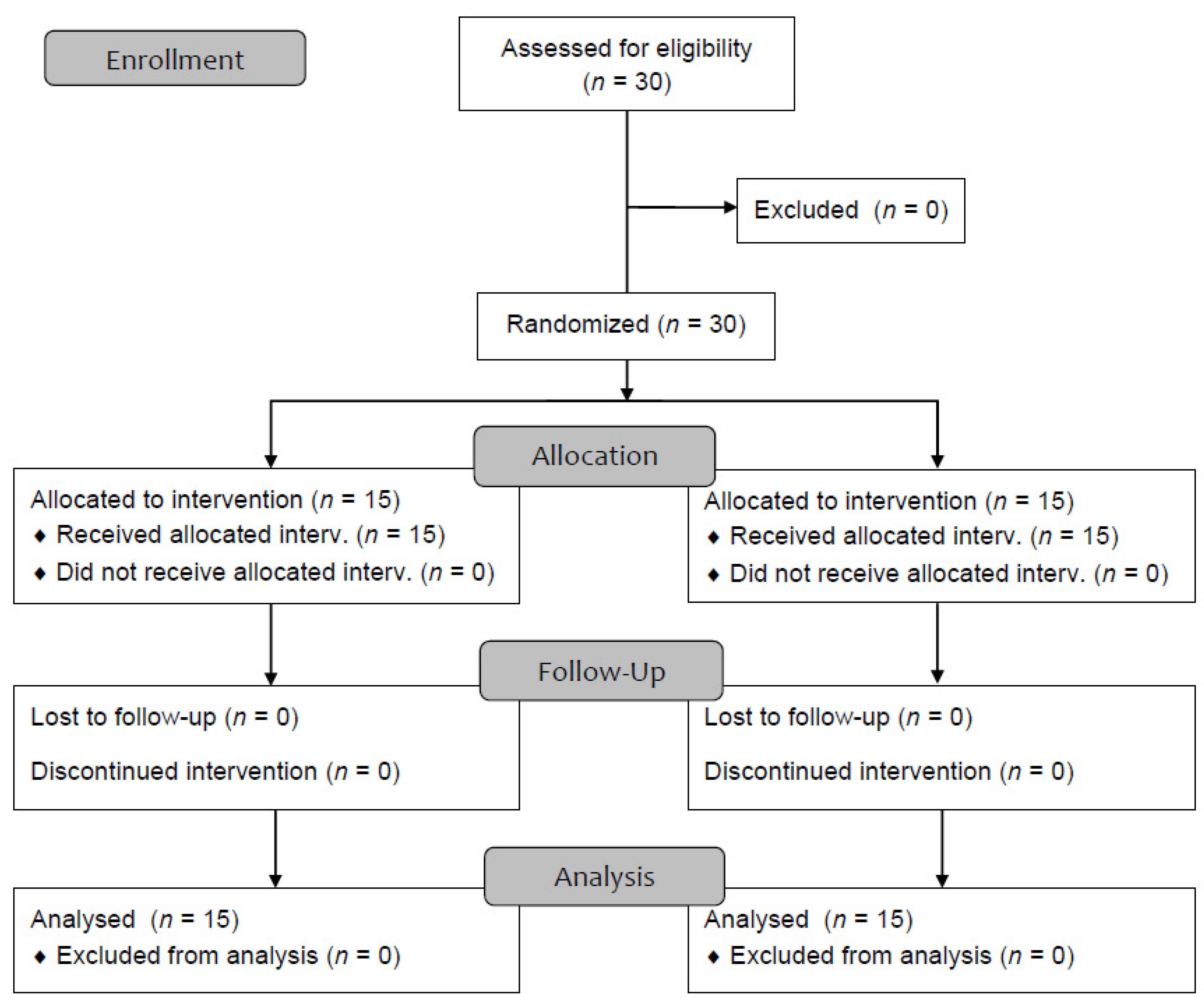
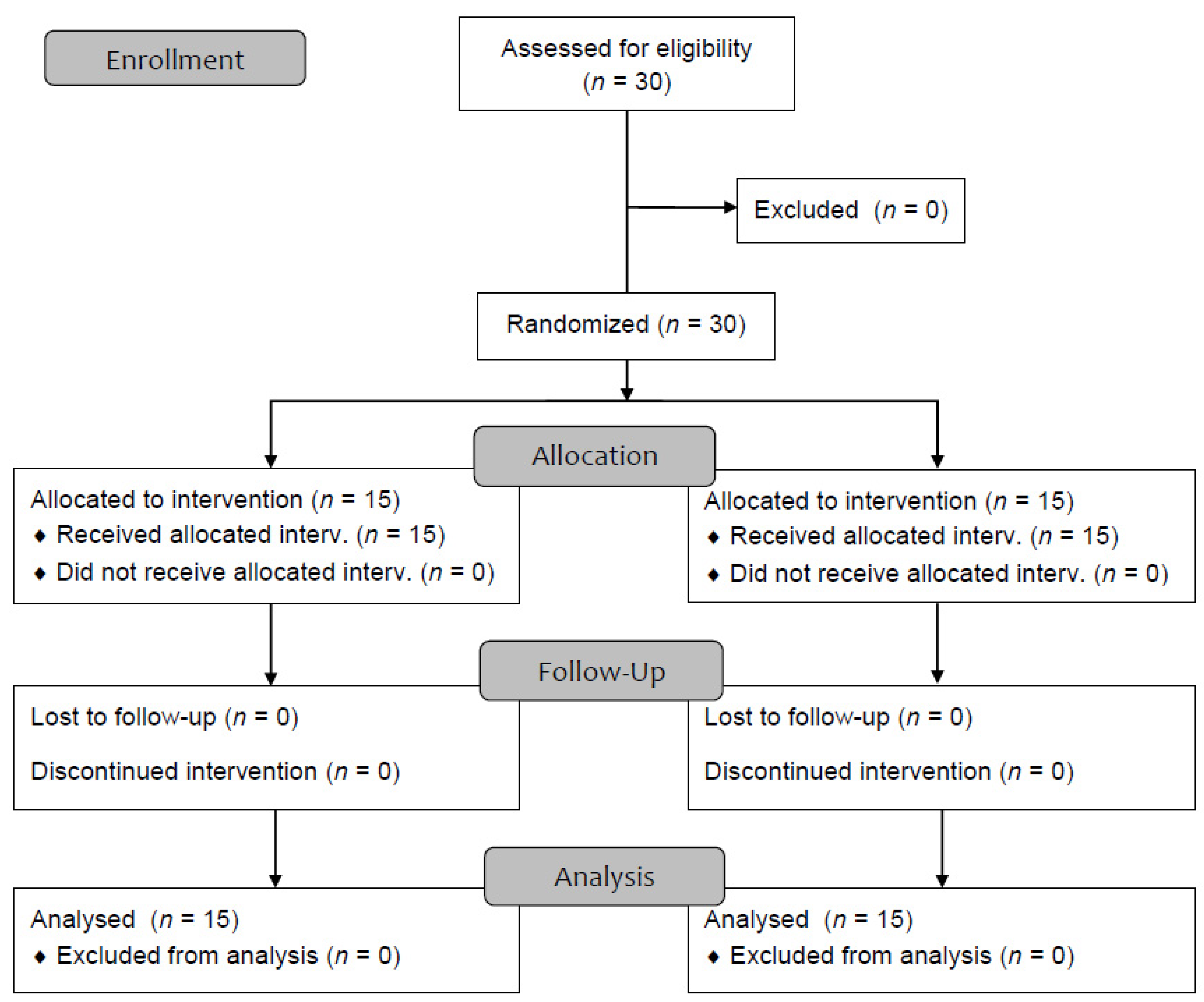
2.1. Study Design and Patients
2.2. Dialysis Procedure and RCA
2.3. Standard Laboratory and Biocompatibility Parameters
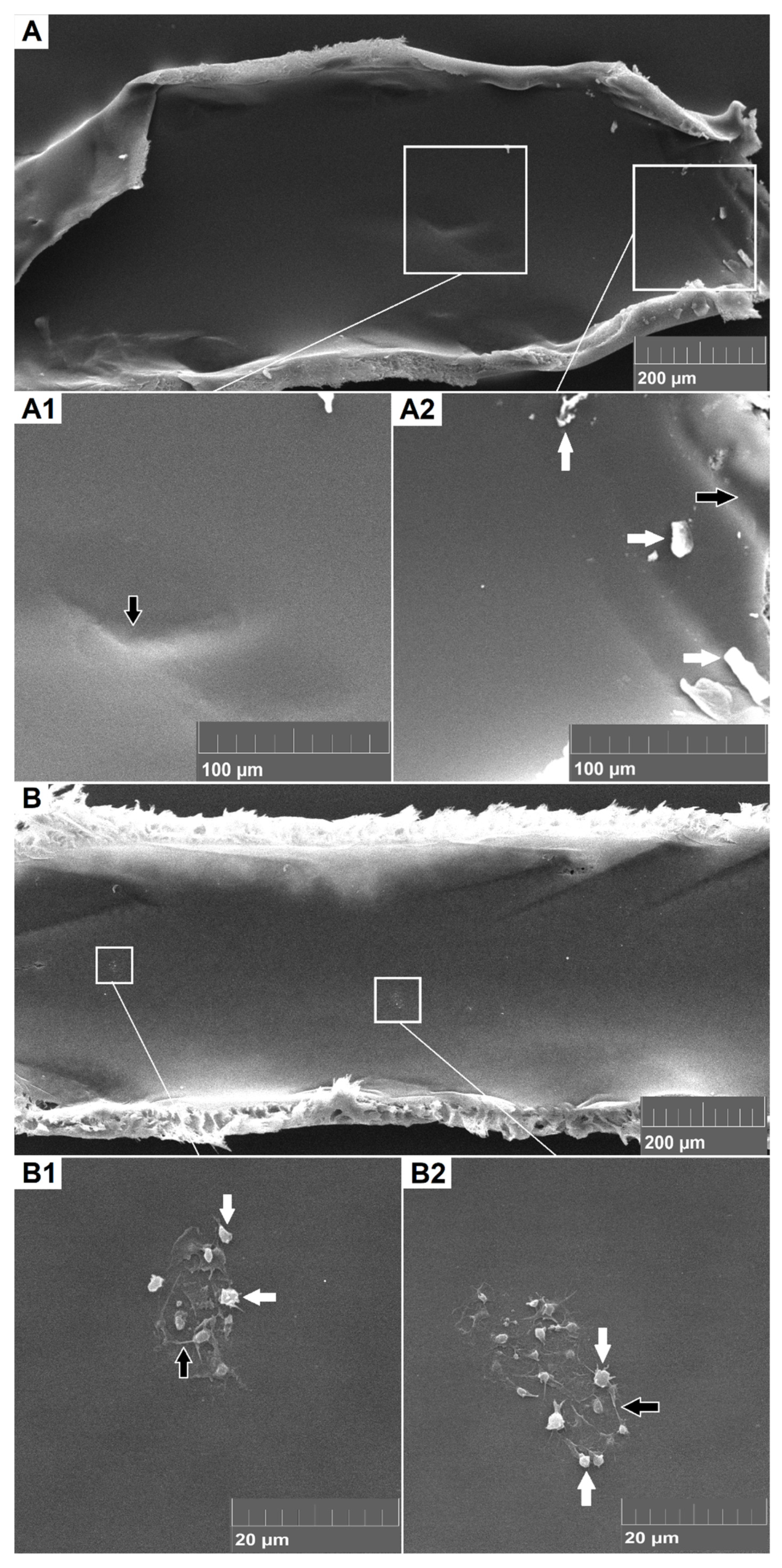
2.4. Scanning Electron Microscopy
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Basic Laboratory Parameters, Anticoagulation Efficiency and Complications
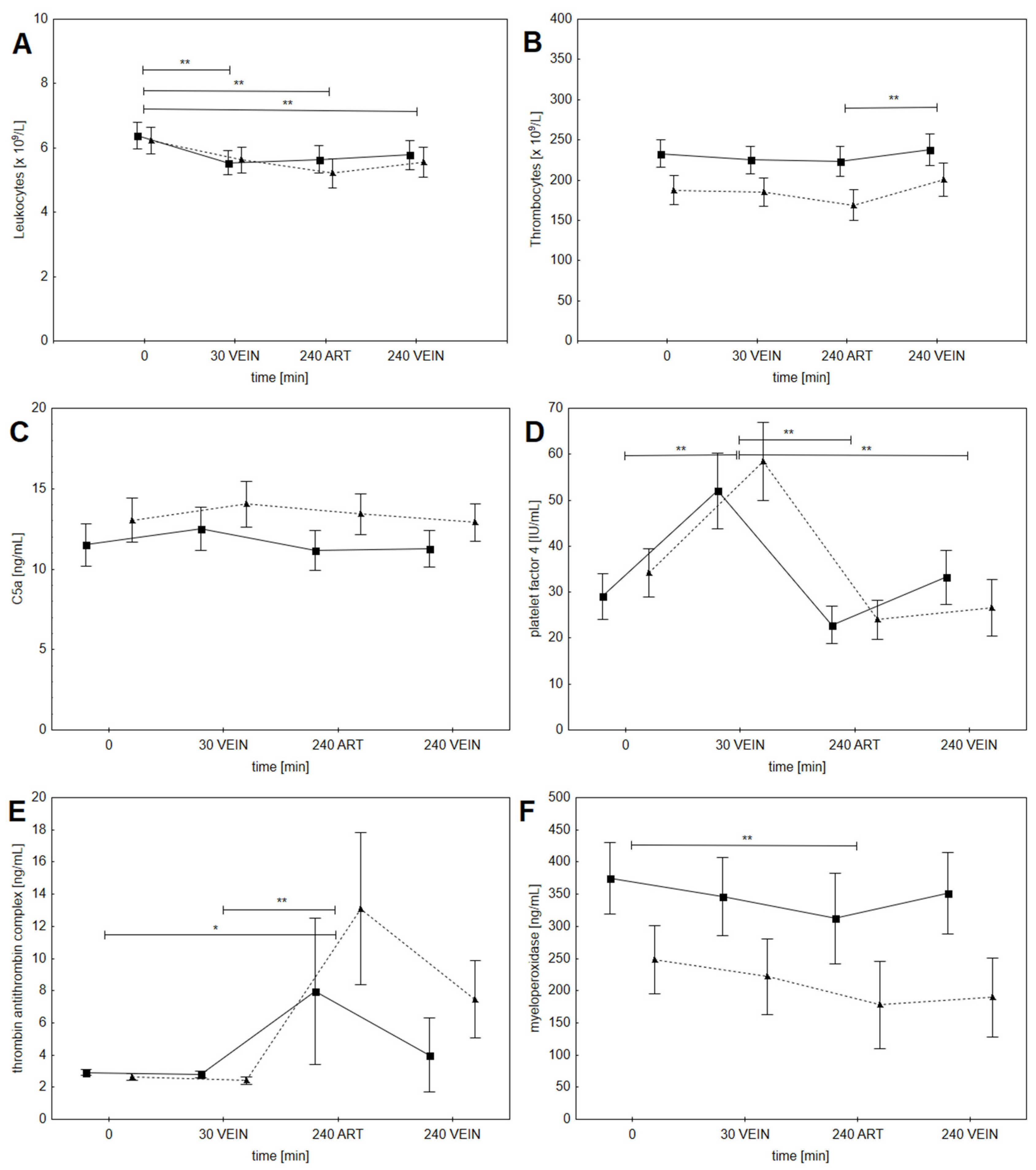
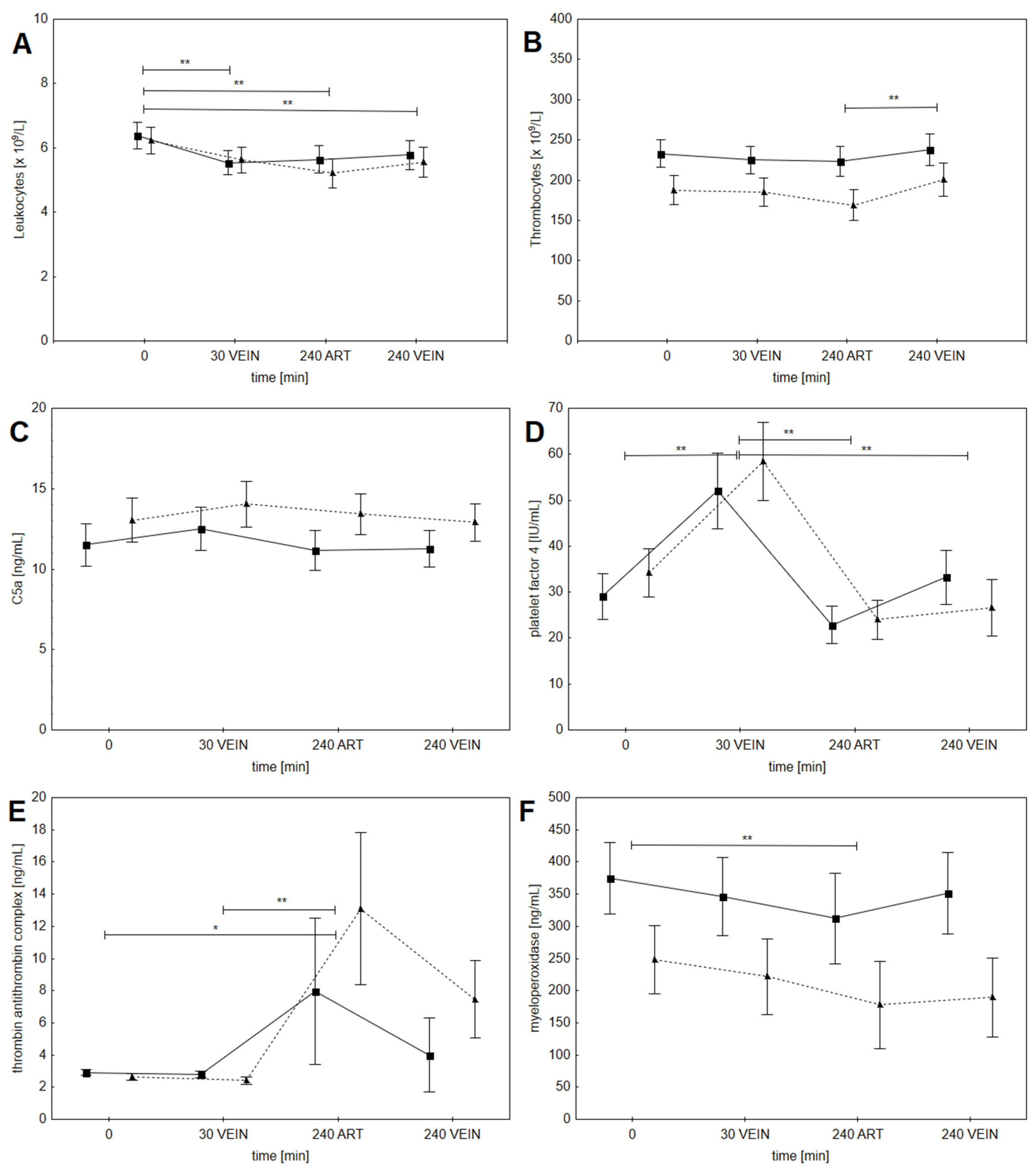
3.3. Biocompatibility Parameters
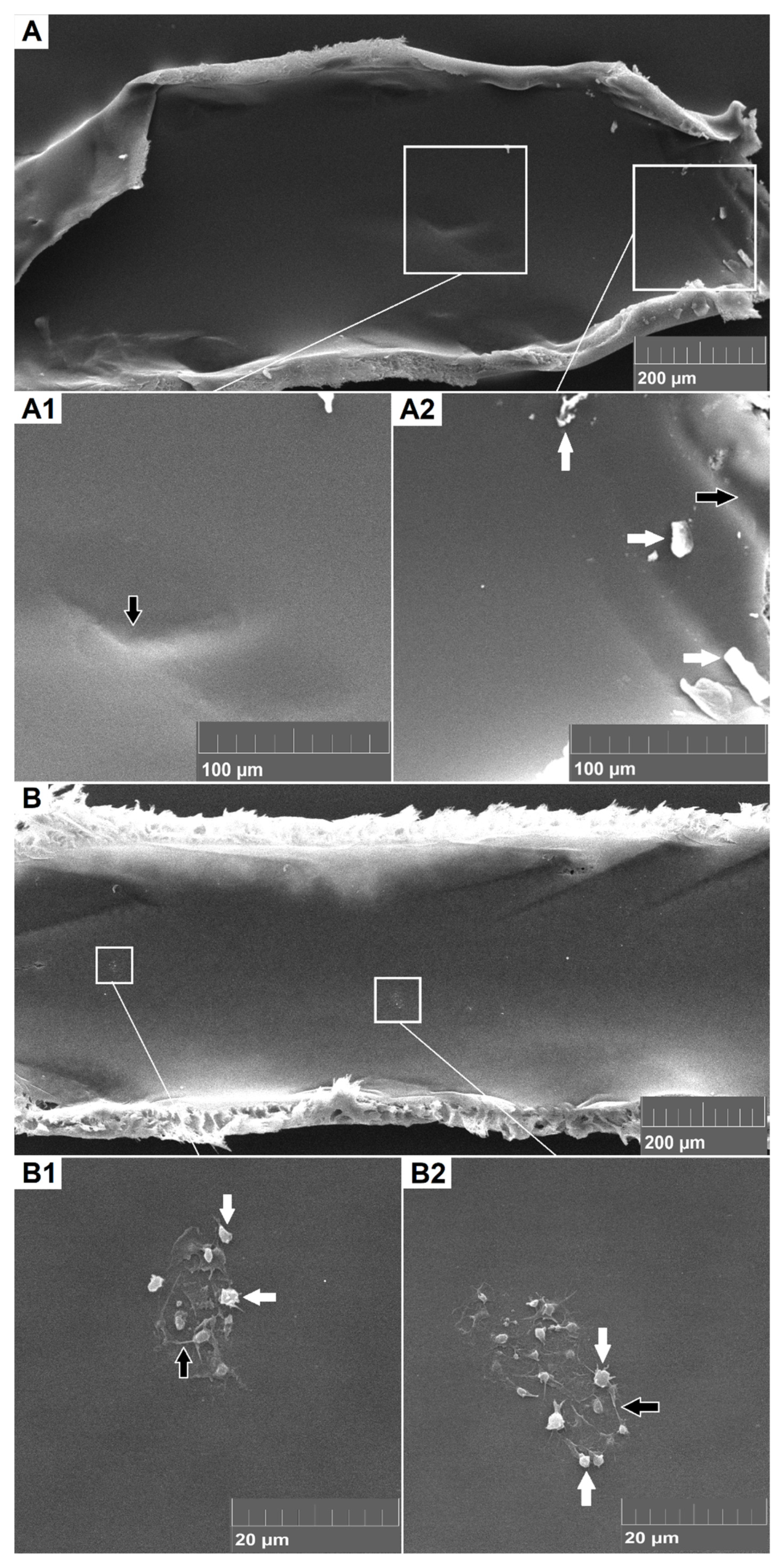
3.4. Electron Microscopy of Dialyzer Fibers
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Uda, S.; Mizobuchi, M.; Akizawa, T. Biocompatible characteristics of high-performance membranes. High-Perform. Membr. Dialyzers 2011, 173, 23–29. [Google Scholar]
- Poppelaars, F.; Faria, B.; Gaya da Costa, M.; Franssen, C.F.; van Son, W.J.; Berger, S.P.; Daha, M.R.; Seelen, M.A. The Complement System in Dialysis: A Forgotten Story? Front. Immunol. 2018, 9, 71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Semple, J.W.; Italiano, J.E.; Freedman, J. Platelets and the immune continuum. Nat. Rev. Immunol. 2011, 11, 264–274. [Google Scholar] [CrossRef] [PubMed]
- Sirolli, V.; Amoroso, L.; Pietropaolo, M.; Grandaliano, G.; Pertosa, G.; Bonomini, M. Platelet-leukocyte interactions in hemodialysis patients: Culprit or bystander? Int. J. Immunopathol. Pharmacol. 2006, 19, 461–470. [Google Scholar] [CrossRef]
- de Borst, H.M. The complement system in hemodialysis patients: Getting to the heart of the matter. Nephron 2016, 132, 1–4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borawski, J. Myeloperoxidase as a marker of hemodialysis biocompatibility and oxidative stress: The underestimated modifying effects of heparin. Am. J. Kidney Dis. 2006, 47, 37–41. [Google Scholar] [CrossRef]
- Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int. Suppl. 2012, 2, 1–138. [Google Scholar]
- Gubenšek, J.; Kovač, J.; Benedik, M.; Marn-Pernat, A.; Knap, B.; Ponikvar, R.; Buturović-Ponikvar, J. Long-term citrate anticoagulation in chronic hemodialysis patients. Ther. Apher. Dial. 2011, 15, 278–282. [Google Scholar] [CrossRef]
- Gritters, M.; Grooteman, M.P.; Schoorl, M.; Schoorl, M.; Bartels, P.C.; Scheffer, P.G.; Teerlink, T.; Schalkwijk, C.G.; Spreeuwenberg, M.; Nube, M.J. Citrate anticoagulation abolishes degranulation of polymorphonuclear cells and platelets and reduces oxidative stress during haemodialysis. Nephrol. Dial. Transplant. 2006, 21, 153–159. [Google Scholar] [CrossRef]
- Grooteman, M.P.C.; Van Tellingen, A.; Van Houte, A.J.; Bos, J.C.; Schoorl, M.; Van Limbeek, J.; Nubé, M.J. Hemodialysis-induced degranulation of polymorphonuclear Cells: No correlation between membrane markers and degranulation products. Nephron 2000, 85, 267–274. [Google Scholar] [CrossRef]
- Bos, J.C.; Grooteman, M.P.; Van Houte, A.J.; Schoorl, M.; Van Limbeek, J.; Nubé, M.J. Low polymorphonuclear cell degranulation during citrate anticoagulation: A comparison between citrate and heparin dialysis. Nephrol. Dial. Transplant. 1997, 12, 1387–1393. [Google Scholar] [CrossRef] [Green Version]
- Omokawa, S.; Malchesky, P.S.; Yamashita, M.; Suzuki, T.; Goldcamp, J.G.; Murabayashi, S.; Nose, Y. Effect of anticoagulant on biocompatibility in membrane plasmapheresis. Int. J. Artif. Organs 1990, 13, 768–777. [Google Scholar] [CrossRef]
- Opatrný, K.; Richtrová, P.; Polanská, K.; Wirth, J.; Šefrna, F.; Brandl, M.; Falkenhagen, D. Citrate anticoagulation control by ionized calcium levels does not prevent hemostasis and complement activation during hemodialysis. Artif. Organs 2007, 31, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Richtrova, P.; Rulcova, K.; Mares, J.; Reischig, T. Evaluation of Three Different Methods to Prevent Dialyzer Clotting Without Causing Systemic Anticoagulation Effect. Artif. Organs 2011, 35, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Buturovic-Ponikvar, J.; Cerne, S.; Gubensek, J.; Ponikvar, R. Regional citrate anticoagulation for hemodialysis: Calcium-free vs. calcium containing dialysate-A randomized trial. Int. J. Artif. Organs 2008, 31, 418–424. [Google Scholar] [CrossRef] [PubMed]
- Evenepoel, P.; Maes, B.; Vanwalleghem, J.; Kuypers, D.; Messiaen, T.; Vanrenterghem, Y. Regional citrate anticoagulation for hemodialysis using a conventional calcium-containing dialysate. Am. J. Kidney Dis. 2002, 39, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Gubensek, J.; Strobl, K.; Harm, S.; Weiss, R.; Eichhorn, T.; Buturovic-Ponikvar, J.; Weber, V.; Hartmann, J. Influence of citrate concentration on the activation of blood cells in an in vitro dialysis setup. PLoS ONE 2018, 13, e0199204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strobl, K.; Harm, S.; Weber, V.; Hartmann, J. The role of ionized calcium and magnesium in regional citrate anticoagulation and its impact on inflammatory parameters. Int. J. Artif. Organs 2017, 40, 15–21. [Google Scholar] [CrossRef]
- Schneditz, D.; Putz-Bankuti, C.; Ribitsch, W.; Schilcher, G. Correction of plasma concentrations for effects of hemoconcentration or hemodilution. ASAIO J. 2012, 58, 160–162. [Google Scholar] [CrossRef]
- Hofbauer, R.; Moser, D.; Frass, M.; Oberbauer, R.; Kaye, A.D.; Wagner, O.; Kapiotis, S.; Druml, W. Effect of anticoagulation on blood membrane interactions during hemodialysis. Kidney Int. 1999, 56, 1578–1583. [Google Scholar] [CrossRef] [Green Version]
- Böhler, J.; Schollmeyer, P.; Dressel, B.; Dobos, G.; Hörl, W.H. Reduction of granulocyte activation during hemodialysis with regional citrate anticoagulation: Dissociation of complement activation and neutropenia from neutrophil degranulation. J. Am. Soc. Nephrol. 1996, 7, 234–241. [Google Scholar] [CrossRef]
- Daugirdas, J.T.; Bernardo, A.A. Hemodialysis effect on platelet count and function and hemodialysis-associated thrombocytopenia. Int. Soc. Nephrol. 2012, 82, 147–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polanská, K.; Opatrný, K.; Rokyta, R.; Kroužecký, A.; Vit, L.; Kasal, E. Effect of regional citrate anticoagulation on thrombogenicity and biocompatibility during CVVHDF. Ren. Fail. 2006, 28, 107–118. [Google Scholar] [CrossRef] [PubMed]
- Lehner, G.F.; Harler, U.; Feistritzer, C.; Haller, V.M.; Hasslacher, J.; Bellmann, R.; Joannidis, M. Hemofiltration induces generation of leukocyte-derived CD31+/CD41-microvesicles in sepsis. Ann. Intensive Care 2017, 7, 89. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Standard Dose Group | Increased Dose Group | |
|---|---|---|
| Blood flow [mL/min] | 250 | 250 |
| 8% Na citrate flow [mL/min] | 150 | 220 |
| Citrate concentration in blood * [mmol/L] | 2.7 | 4.0 |
| Dose of citrate [mmol/h] | 40 | 60 |
| Infusion of 1M CaCl2 ** [mL/h] | 14 | 16 |
| Standard Dose Group | Increased Dose Group | p Value | |
|---|---|---|---|
| N | 15 | 15 | / |
| Female | 6 (40%) | 5 (33%) | p = 0.75 |
| Age | 62 ± 14 years | 71 ± 13 years | p = 0.07 |
| Renal replacement therapy | 6 ± 2.5 years | 11 ± 10 years | p = 0.04 |
| PF4 before hemodialysis | 28 ± 16 | 31 ± 17 | p = 0.33 |
| TAT before hemodialysis (ug/L) | 4 ± 4 | 3 ± 2 | p = 0.28 |
| MPO before hemodialysis (ng/mL) | 342 ± 260 | 239 ± 70 | p = 0.09 |
| C5a-desArg before hemodialysis (ng/mL) | 11 ± 3 | 11 ± 6 | p = 0.43 |
| Standard Dose Group | Increased Dose Group | p Value | |
|---|---|---|---|
| corrected Ca before [mmol/L] | 2.22 ± 0.23 | 2.21 ± 0.14 | p = 0.45 |
| corrected Ca after [mmol/L] | 2.08 ± 0.13 | 2.25 ± 0.17 | p < 0.01 |
| total/ionized calcium ratio | 2.06 ± 0.11 | 2.07 ± 0.11 | p = 0.42 |
| N of patients with total/ionized calcium > 2.5 | 0/15 | 0/15 | / |
| post-filter ionized calcium after 30 min [mmol/L] | 0.32 ± 0.05 | 0.23 ± 0.05 | p < 0.01 |
| post-filter ionized calcium after 2 h [mmol/L] | 0.30 ± 0.04 | 0.20 ± 0.05 | p < 0.01 |
| Mg before [mmol/L] | 1.02 ± 0.15 | 1.04 ± 0.14 | p = 0.33 |
| Mg after [mmol/L] | 0.81 ± 0.06 | 0.80 ± 0.10 | p = 0.47 |
| pH before | 7.44 ± 0.05 | 7.41± 0.04 | p = 0.05 |
| pH after | 7.49 ± 0.05 | 7.46 ± 0.04 | p = 0.06 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orsag, A.; Bozic-Mijovski, M.; Hudoklin, S.; Simcic, S.; Gubensek, J. Biocompatibility Parameters with Standard and Increased Dose of Citrate in Hemodialysis—A Randomized Trial. J. Clin. Med. 2021, 10, 2987. https://doi.org/10.3390/jcm10132987
Orsag A, Bozic-Mijovski M, Hudoklin S, Simcic S, Gubensek J. Biocompatibility Parameters with Standard and Increased Dose of Citrate in Hemodialysis—A Randomized Trial. Journal of Clinical Medicine. 2021; 10(13):2987. https://doi.org/10.3390/jcm10132987
Chicago/Turabian StyleOrsag, Alesa, Mojca Bozic-Mijovski, Samo Hudoklin, Sasa Simcic, and Jakob Gubensek. 2021. "Biocompatibility Parameters with Standard and Increased Dose of Citrate in Hemodialysis—A Randomized Trial" Journal of Clinical Medicine 10, no. 13: 2987. https://doi.org/10.3390/jcm10132987
APA StyleOrsag, A., Bozic-Mijovski, M., Hudoklin, S., Simcic, S., & Gubensek, J. (2021). Biocompatibility Parameters with Standard and Increased Dose of Citrate in Hemodialysis—A Randomized Trial. Journal of Clinical Medicine, 10(13), 2987. https://doi.org/10.3390/jcm10132987