
Subchondral Bone Relative Area and Density in Human Osteoarthritic Femoral Heads Assessed with Micro-CT before and after Mechanical Embedding of the Innovative Multi-Spiked Connecting Scaffold for Resurfacing THA Endoprostheses: A Pilot Study

 ,
, 
 ,
, 
 and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Selection
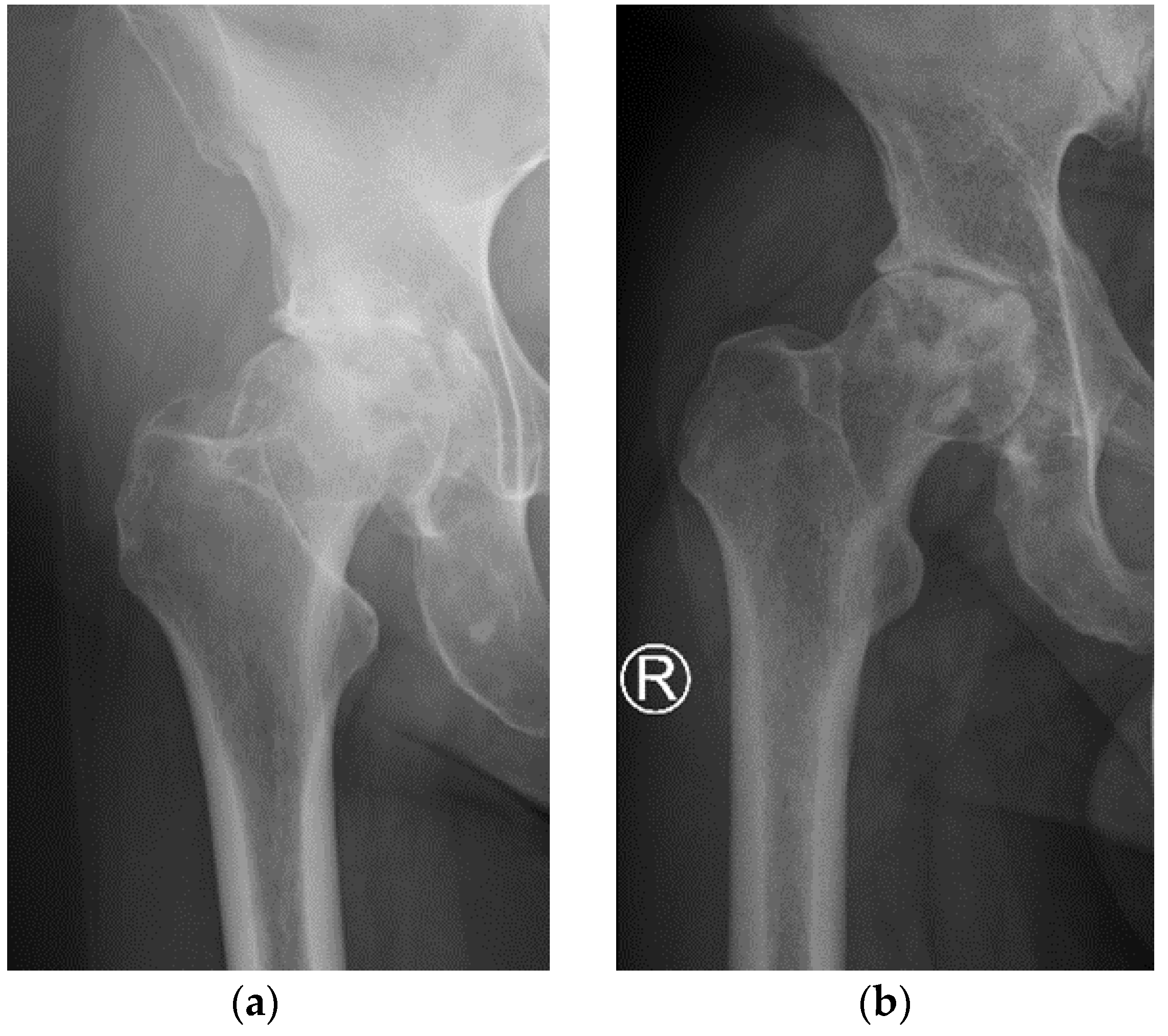
2.2. Radiological and Pain Assessment
2.3. Femoral Heads Sampling
2.4. Femoral Head Specimens Preparation
2.5. MSC-Scaffold Preprototypes
2.6. Micro-CT Examination
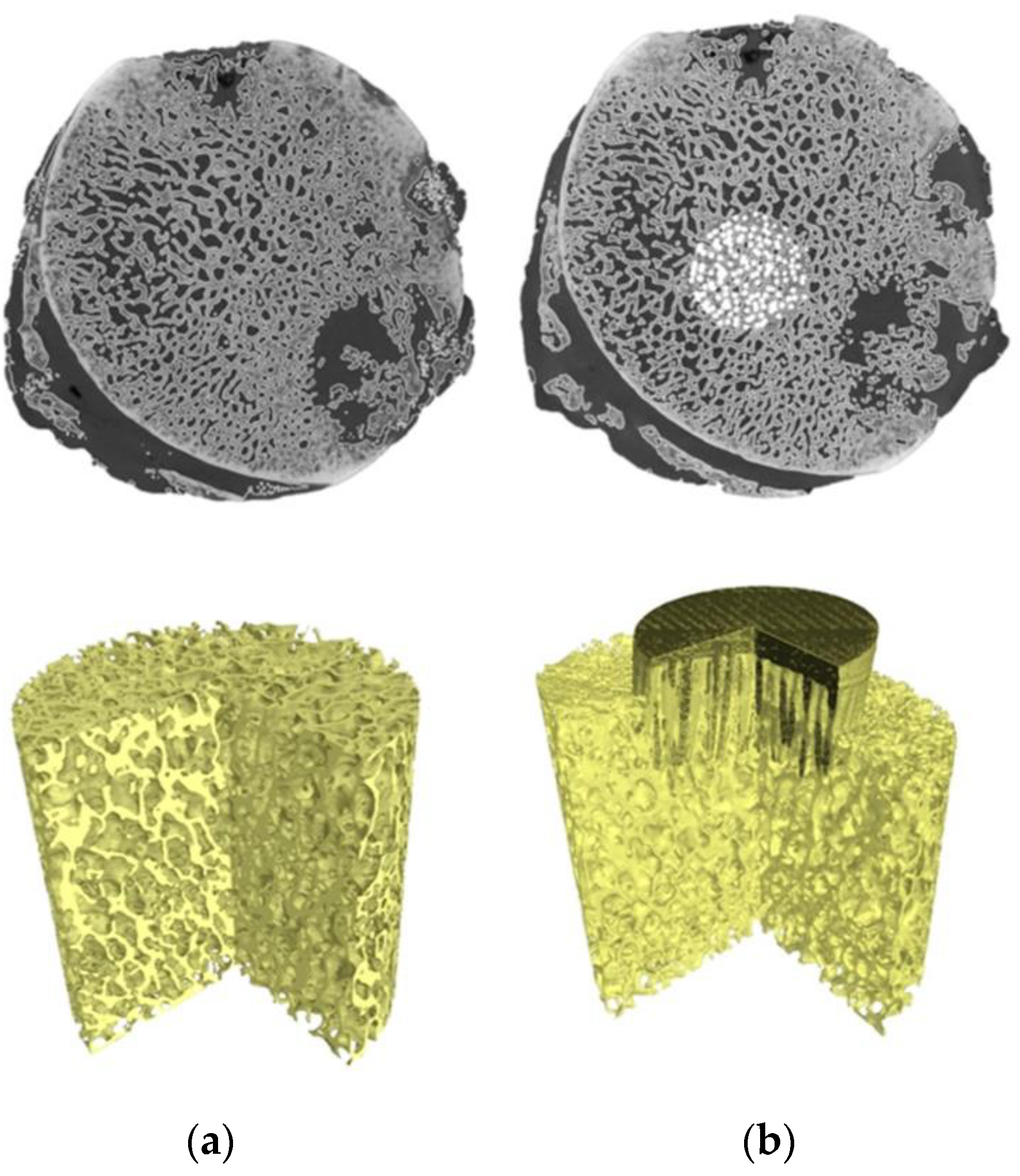
2.7. Micro-CT 3D Reconstruction of Specimens
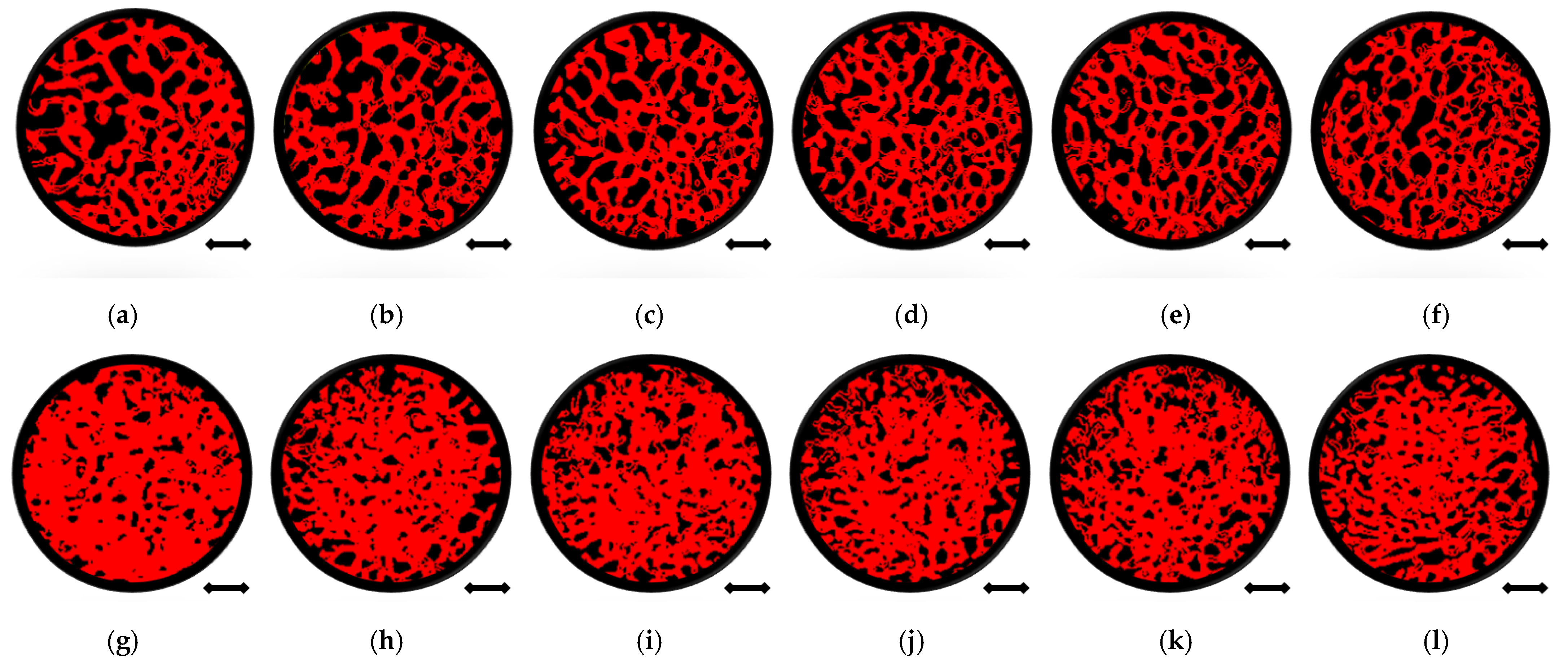
2.8. Determining of Subchondral Trabecular Bone Relative Area, Relative Density, and Compression Strength
3. Results
3.1. Characteristics of the Patients
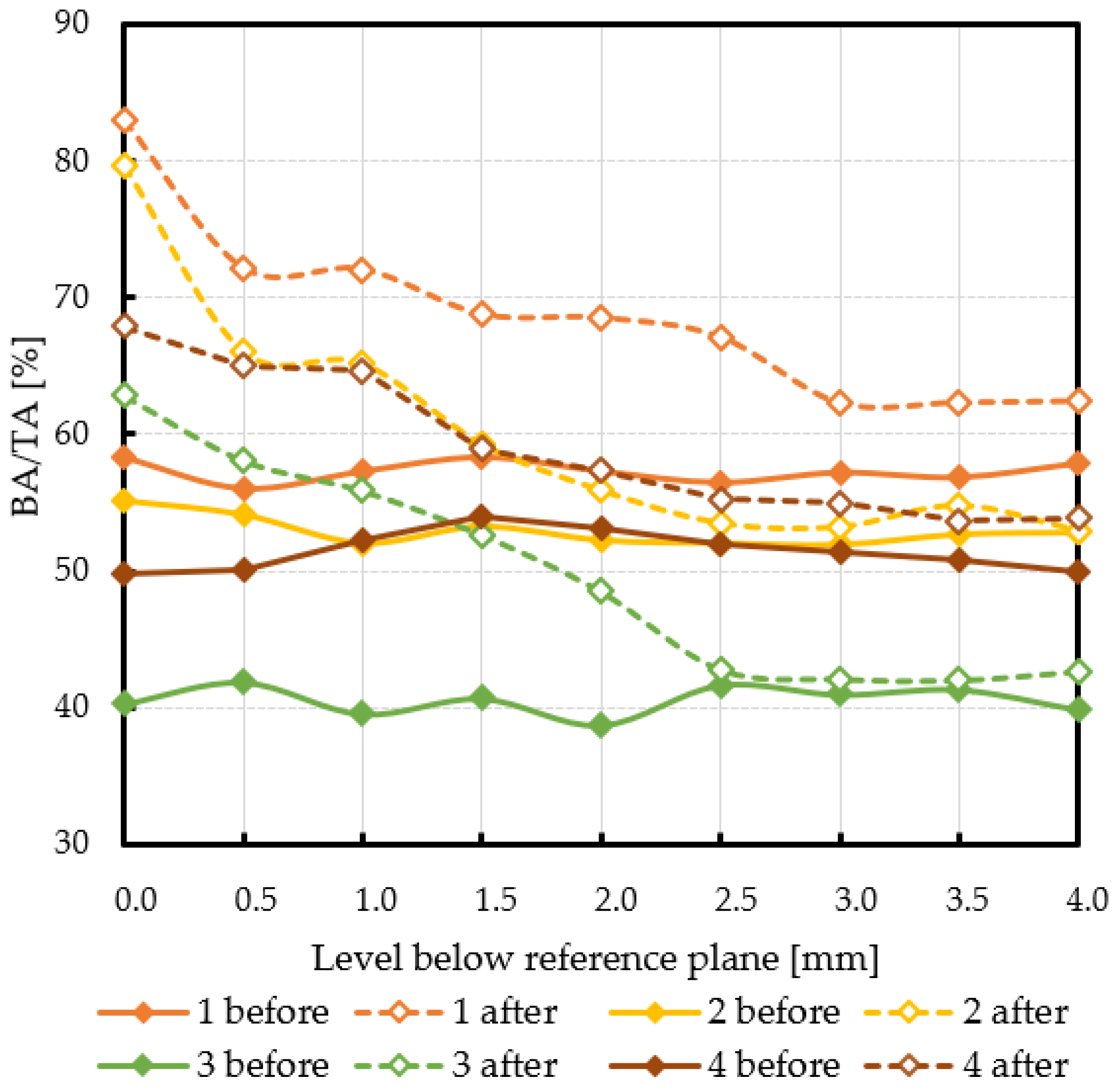
3.2. Subchondral Trabecular Bone Relative Surface before and after MSC-Scaffold Prototype Embedding
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Agarwal, N.; To, K.; Khan, W. Cost-Effectiveness Analyses of Total Hip Arthroplasty for Hip Osteoarthritis: A PRISMA Systematic Review. Int. J. Clin. Pract. 2021, 75, e13806. [Google Scholar] [CrossRef]
- Suárez, J.C.; Forero, A.; Llinás, A.; Bonilla, G.; Rodríguez, H.; Amado, O. Bearing surfaces in primary hip arthroplasty. Is there any difference? Acta Ortop. Mex. 2020, 34, 22–26. [Google Scholar] [CrossRef]
- Daniel, J.; Pradhan, C.; Ziaee, H.; Pynsent, P.B.; McMinn, D.J. Results of Birmingham hip resurfacing at 12 to 15 years: A single-surgeon series. Bone Jt. J. 2014, 96, 1298–1306. [Google Scholar] [CrossRef]
- Ford, M.C.; Hellman, M.D.; Kazarian, G.S.; Clohisy, J.C.; Nunley, R.M.; Barrack, R.L. Five to Ten-Year Results of the Birmingham Hip Resurfacing Implant in the US: A Single Institution’s Experience. J. Bone Jt. Surg. Am. 2018, 100, 1879–1887. [Google Scholar] [CrossRef] [PubMed]
- Hellman, M.D.; Ford, M.C.; Barrack, R.L. Is there evidence to support an indication for surface replacement arthroplasty?: A systematic review. Bone Jt. J. 2019, 101, 32–40. [Google Scholar] [CrossRef]
- Uklejewski, R.; Rogala, P.; Winiecki, M. and Mielniczuk, J. Prototype of minimally invasive hip resurfacing endoprosthesis—Bioengineering design and manufacturing. Acta Bioeng. Biomech. 2009, 11, 65–70. [Google Scholar] [PubMed]
- Uklejewski, R.; Winiecki, M.; Rogala, P.; Mielniczuk, J. Selective laser melted prototype of original minimally invasive hip endoprosthesis. Rapid Prototyp. J. 2011, 17, 76–85. [Google Scholar] [CrossRef]
- Uklejewski, R.; Rogala, P.; Winiecki, M.; Kędzia, A.; Ruszkowski, P. Preliminary Results of Implantation in Animal Model and Osteoblast Culture Evaluation of Prototypes of Biomimetic Multispiked Connecting Scaffold for Noncemented Stemless Resurfacing Hip Arthroplasty Endoprostheses. BioMed Res. Int. 2013, 2013, 689089. [Google Scholar] [CrossRef]
- Uklejewski, R.; Rogala, P.; Winiecki, M.; Tokłowicz, R.; Ruszkowski, P.; Wołuń-Cholewa, M. Biomimetic Multispiked Connecting Ti-Alloy Scaffold Prototype for Entirely-Cementless Resurfacing Arthroplasty Endoprostheses—Exemplary Results of Implantation of the Ca-P Surface-Modified Scaffold Prototypes in Animal Model and Osteoblast Culture Evaluation. Materials 2016, 9, 532. [Google Scholar] [CrossRef]
- Uklejewski, R.; Winiecki, M.; Rogala, P.; Patalas, A. Structural-Geometric Functionalization of the Additively Manufactured Prototype of Biomimetic Multi-spiked Connecting Ti-Alloy Scaffold for Entirely Noncemented Resurfacing Arthroplasty Endoprostheses. Appl. Bionics Biomech. 2017, 2017, 5638680. [Google Scholar] [CrossRef]
- Uklejewski, R.; Winiecki, M.; Patalas, A.; Rogala, P. Numerical studies of the influence of various geometrical features of a multi-spiked connecting scaffold prototype on mechanical stresses in peri-implant bone. Comput. Methods Biomech. Biomed. Eng. 2018, 21, 541–547. [Google Scholar] [CrossRef]
- Uklejewski, R.; Winiecki, M.; Krawczyk, P.; Tokłowicz, R. Native Osseous CaP Biomineral Coating on a Biomimetic Multi-spiked Connecting Scaffold Prototype for Cementless Resurfacing Arthroplasty Achieved by Combined Electrochemical Deposition. Materials 2019, 12, 3994. [Google Scholar] [CrossRef]
- Rogala, P.; Uklejewski, R.; Winiecki, M.; Dąbrowski, M.; Gołańczyk, J.; Patalas, A. First biomimetic fixation for resurfacing arthroplasty—Investigation in swine of a prototype partial knee endoprosthesis. BioMed Res. Int. 2019, 2019, 6952649. [Google Scholar] [CrossRef] [PubMed]
- Rogala, P. Endoprosthesis. EU Patent No. EP072418 B1, 22 December 1999. [Google Scholar]
- Rogala, P. Method and Endoprosthesis to Apply This Implantation. Canadian Patent No. 2.200.064, 1 April 2002. [Google Scholar]
- Madry, H.; Niek van Dijk, C.; Mueller-Gerbl, M. The basic science of the subchondral bone. Knee Surg. Sports Traumatol. Arthrosc. 2010, 18, 419–433. [Google Scholar] [CrossRef] [PubMed]
- Khan, I.M.; Gilbert, S.J.; Singhrao, S.K.; Duance, V.C.; Archer, C.W. Cartilage integration: Evaluation of the reasons for failure of integration during cartilage repair. A review. Eur. Cells Mater. 2008, 16, 26–39. [Google Scholar] [CrossRef] [PubMed]
- Beaulé, P.E.; Matar, W.Y.; Poitras, P.; Smit, K.; May, O. Otto Aufranc Award: Component Design and Technique Affect Cement Penetration in Hip Resurfacing. Clin. Orthop. Relat. Res. 2009, 467, 84–93. [Google Scholar] [CrossRef][Green Version]
- Krause, M.; Breer, S.; Hahn, M.; Rüther, W.; Morlock, M.M.; Amling, M.; Zustin, J. Cementation and interface analysis of early failure cases after hip-resurfacing arthroplasty. Int. Orthop. 2012, 36, 1333–1340. [Google Scholar] [CrossRef][Green Version]
- Campbell, P.; De Smet, K. The Birmingham Hip Resurfacing (BHR) prosthesis. In The Hip Resurfacing Handbook. A Practical Guide to the Use and Management of Modern Hip Resurfacings; De Smet, K., Campbell, P., Van Der Straeten, C., Eds.; Woodhead Publishing Series in Biomaterials; Woodhead Publishing: Cambridge, UK, 2013; pp. 25–30. [Google Scholar] [CrossRef]
- Shiraishi, K.; Chiba, K.; Okazaki, N.; Yokota, K.; Nakazoe, Y.; Kidera, K.; Yonekura, A.; Tomita, M.; Osaki, M. In vivo analysis of subchondral trabecular bone in patients with osteoarthritis of the knee using second-generation high-resolution peripheral quantitative computed tomography (HR-pQCT). Bone 2020, 132, 115155. [Google Scholar] [CrossRef] [PubMed]
- Okazaki, N.; Chiba, K.; Motoi, M.; Osaki, M. Analysis of Subchondral Bone Microstructure by HR-PQCT: Relationship with The Severity of Knee Osteoarthritis and Alignments of Lower Extremities. Osteoarthr. Cartil. 2017, 25, S263. [Google Scholar] [CrossRef]
- Li, G.; Zheng, Q.; Landao-Bassonga, E.; Cheng, T.S.; Pavlos, N.J.; Ma, Y.; Zhang, C.; Zheng, M.H. Influence of age and gender on microarchitecture and bone remodeling in subchondral bone of the osteoarthritic femoral head. Bone 2015, 77, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Chen, L.; Zheng, Q.; Ma, Y.; Zhang, C.; Zheng, M.H. Subchondral bone deterioration in femoral heads in patients with osteoarthritis secondary to hip dysplasia: A case-control study. J. Orthop. Transl. 2019, 24, 190–197. [Google Scholar] [CrossRef]
- Uklejewski, R.; Winiecki, M.; Patalas, A.; Rogala, P. Bone Density Micro-CT Assessment during Embedding of the Innovative Multi-Spiked Connecting Scaffold in Periarticular Bone to Elaborate a Validated Numerical Model for Designing Biomimetic Fixation of Resurfacing Endoprostheses. Materials 2021, 14, 1384. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.M.; Gray, F.; Crawshaw, J.P.; Boek, E.S. Micro-computed tomography pore-scale study of flow in porous media: Effect of voxel resolution. Adv. Water Resour. 2016, 95, 276–287. [Google Scholar] [CrossRef]
- Tuller, M.; Kulkarni, R.; Fink, W. Segmentation of X-ray CT data of porous materials: A review of global and locally adaptive algorithms. In Soil–Water–Root Processes: Advances in Tomography and Imaging; Anderson, S.H., Hopmans, J.W., Eds.; Soil Science Society of America Special Publications: Madison, WI, USA, 2013; Volume 61, pp. 157–182. [Google Scholar] [CrossRef]
- Akhter, M.P.; Recker, R.R. High-resolution imaging in bone tissue research-review. Bone 2021, 143, 115620. [Google Scholar] [CrossRef]
- Buccino, F.; Colombo, C.; Vergani, L.M. A Review on Multiscale Bone Damage: From the Clinical to the Research Perspective. Materials 2021, 14, 1240. [Google Scholar] [CrossRef]
- Gregory, J.; Stewart, A.; Undrill, P.; Reid, D.; Aspden, R. Bone shape, structure, and density as determinants of osteoporotic hip fracture: A pilot study investigating the combination of risk factors. Investig. Radiol. 2005, 40, 591–597. [Google Scholar] [CrossRef]
- San Antonio, T.; Ciaccia, M.; Müller-Karger, C.; Casanova, E. Orientation of orthotropic material properties in a femur FE model: A method based on the principal stresses directions. Med. Eng. Phys. 2012, 34, 914–919. [Google Scholar] [CrossRef]
- Chappard, D.; Retailleau-Gaborit, N.; Legrand, E.; Baslé, M.F.; Audran, M. Comparison insight bone measurements by histomorphometry and microCT. J. Bone Miner. Res. 2005, 20, 1177–1184. [Google Scholar] [CrossRef] [PubMed]
- Vandeweghe, S.; Coelho, P.G.; Vanhove, C.; Wennerberg, A.; Jimbo, R. Utilizing micro-computed tomography to evaluate bone structure surrounding dental implants: A comparison with histomorphometry. J. Biomed. Mater. Res. Part B Appl. Biomater. 2013, 101, 1259–1266. [Google Scholar] [CrossRef]
- Martin, R.B. Porosity and specific surface of bone. Crit. Rev. Biomed. Eng. 1984, 10, 179–222. [Google Scholar]
- Adams, G.J.; Cook, R.B.; Hutchinson, J.R.; Zioupos, P. Bone Apparent and Material Densities Examined by Cone Beam Computed Tomography and the Archimedes Technique: Comparison of the Two Methods and Their Results. Front. Mech. Eng. 2018, 3, 23. [Google Scholar] [CrossRef]
- Zioupos, P.; Cook, R.B.; Hutchinson, J.R. Some basic relationships between density values in cancellous and cortical bone. J. Biomech. 2008, 41, 1961–1968. [Google Scholar] [CrossRef]
- Keenan, M.J.; Hegsted, M.; Jones, K.L.; Delany, J.P.; Kime, J.C.; Melancon, L.E.; Tulley, R.T.; Hong, K.D. Comparison of Bone Density Measurement Techniques: DXA and Archimedes’ Principle. J. Bone Miner. Res. 1997, 12, 1903–1907. [Google Scholar] [CrossRef] [PubMed]
- Lotz, J.C.; Gerhart, T.N.; Hayes, W.C. Mechanical properties of trabecular bone from the proximal femur: A quantitative CT study. J. Comput. Assist. Tomogr. 1990, 14, 107–114. [Google Scholar] [CrossRef]
- Fleps, I.; Bahaloo, H.; Zysset, P.K.; Ferguson, S.J.; Pálsson, H.; Helgason, B. Empirical relationships between bone density and ultimate strength: A literature review. J. Mech. Behav. Biomed. Mater. 2020, 110, 103866. [Google Scholar] [CrossRef]
- Ito, M.; Nakamura, T.; Matsumoto, T.; Tsurusaki, K.; Hayashi, K. Analysis of trabecular microarchitecture of human iliac bone using microcomputed tomography in patients with hip arthrosis with or without vertebral fracture. Bone 1998, 23, 163–169. [Google Scholar] [CrossRef]
- Ryan, M.; Barnet, L.; Rochester, J.; Wilkinson, J.M.; Dall’Ara, E. A new approach to comprehensively evaluate the morphological properties of the human femoral head: Example of application to osteoarthritic joint. Sci. Rep. 2020, 10, 5538. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient No. | Age | Sex | BMI | Side | Opposite Side OA | Duration of Pain [years] | Orthopedic Supports | KL | VAS |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 72 | M | 27.5 | R | yes | 5 | orthopedic walker | 3 | 6 |
| 2 | 54 | F | 24.0 | R | yes | 1 | without orthopedic supports | 4 | 7 |
| 3 | 68 | F | 28.8 | R | yes | 2 | elbow crutches | 3 | 7 |
| 4 | 51 | M | 33.2 | R | no | 2 | elbow crutches | 4 | 8 |
| Patient No. | Levels Below Reference Plane [mm] | Mean ± SD | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 0.0 | 0.5 | 1.0 | 1.5 | 2.0 | 2.5 | 3.0 | 3.5 | 4.0 | |||
| 1 | BA/TA before MSCS embedding [%] | 58.4 | 56.1 | 57.3 | 58.4 | 57.3 | 56.5 | 57.2 | 56.9 | 57.9 | 57.3 ± 0.8 |
| BA/TA after MSCS embedding [%] | 83.0 | 72.2 | 72.1 | 68.8 | 68.5 | 67.1 | 62.3 | 62.3 | 62.4 | ||
| Change in BA/TA [%] | 24.7 | 16.1 | 14.8 | 10.4 | 11.2 | 10.6 | 5.0 * | 5.4 | 4.5 | ||
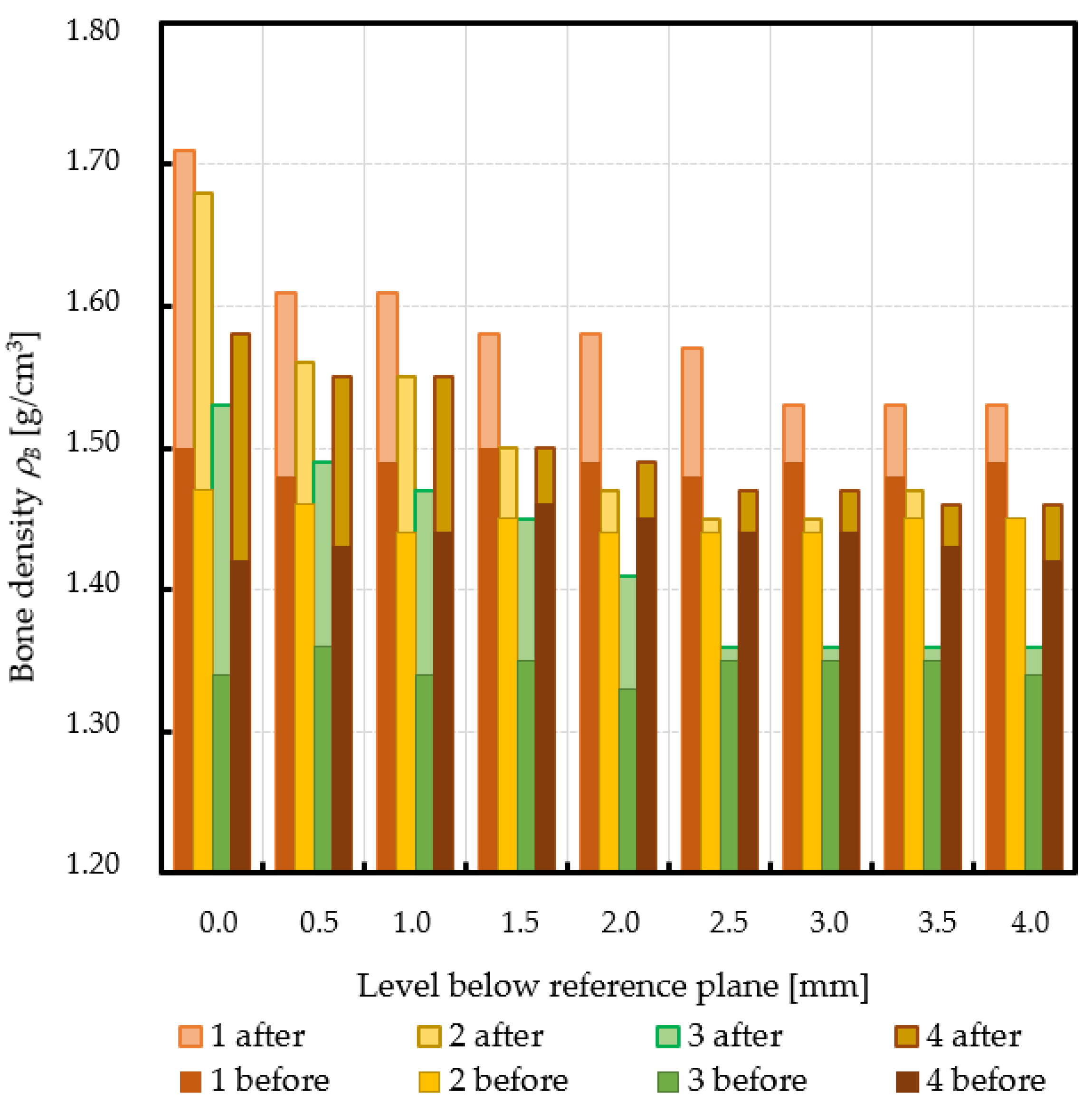
| ρB before MSCS embedding [g/cm3] | 1.50 | 1.48 | 1.49 | 1.50 | 1.49 | 1.48 | 1.49 | 1.48 | 1.49 | 1.49 ± 0.01 | |
| ρB after MSCS embedding [g/cm3] | 1.71 | 1.61 | 1.61 | 1.58 | 1.58 | 1.57 | 1.53 | 1.53 | 1.53 | ||
| ρB relative change [%] | 14.3 | 9.0 | 8.3 | 5.6 | 6.3 | 6.1 | 2.9 | 3.1 | 2.5 | ||
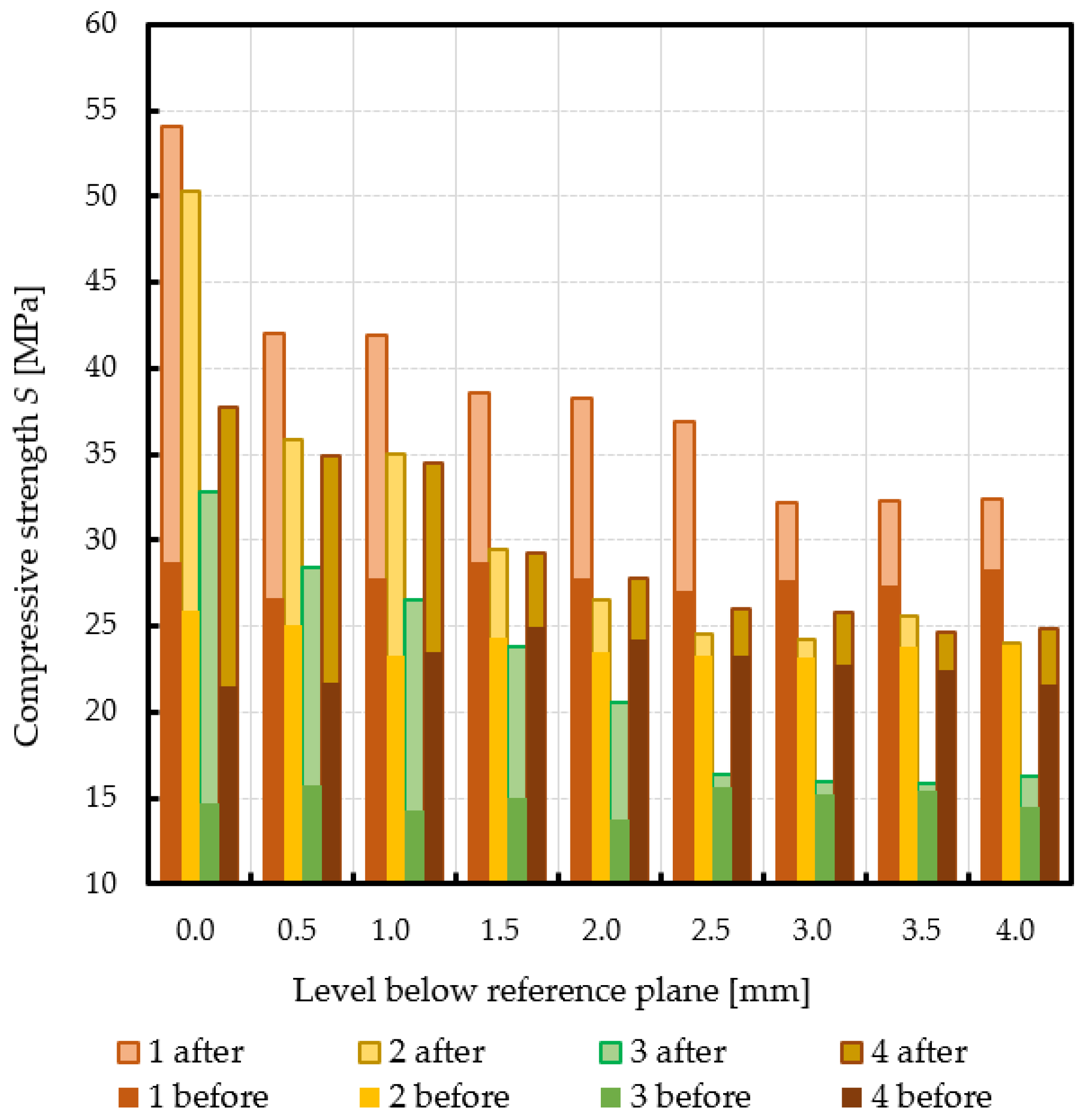
| S before MSCS embedding [MPa] | 28.7 | 26.7 | 27.8 | 28.7 | 27.8 | 27.1 | 27.7 | 27.4 | 28.3 | 27.8 ± 0.7 | |
| S after MSCS embedding [MPa] | 54.1 | 42.0 | 41.9 | 38.5 | 38.3 | 36.9 | 32.2 | 32.3 | 32.4 | ||
| S relative change [%] | 88.6 | 57.5 | 51.0 | 34.3 | 37.7 | 36.3 | 16.3 | 17.8 | 14.3 | ||
| 2 | BA/TA before MSCS embedding [%] | 55.1 | 54.1 | 52.0 | 53.2 | 52.2 | 52.0 | 51.9 | 52.7 | 52.8 | 52.9 ± 1.1 |
| BA/TA after MSCS embedding [%] | 79.7 | 66.1 | 65.2 | 59.3 | 55.9 | 53.5 | 53.2 | 54.8 | 52.9 | ||
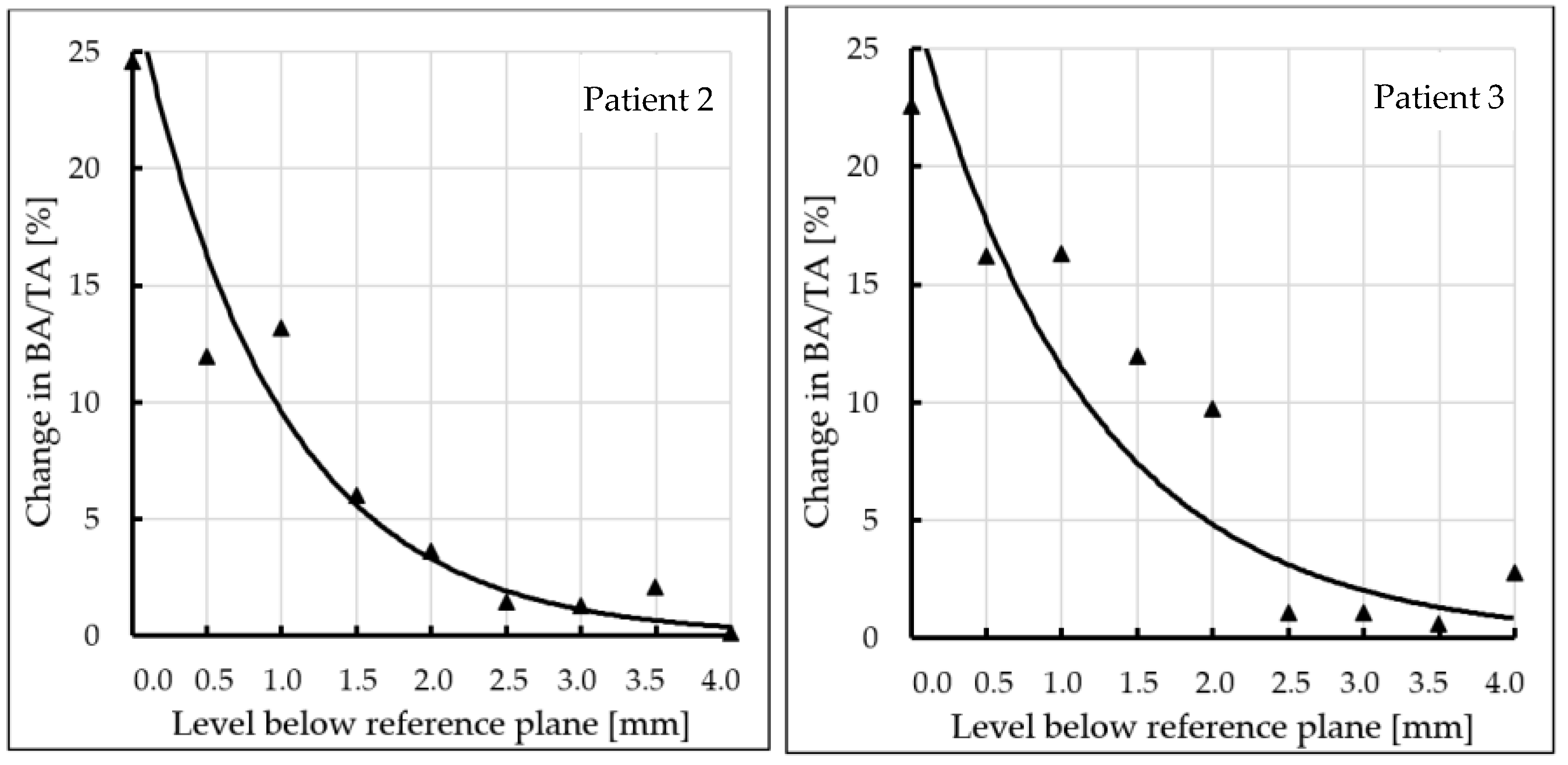
| Change in BA/TA [%] | 24.6 | 12.0 | 13.2 | 6.0 | 3.7 * | 1.4 | 1.3 | 2.1 | 0.1 | ||
| ρB before MSCS embedding [g/cm3] | 1.47 | 1.46 | 1.44 | 1.45 | 1.44 | 1.44 | 1.44 | 1.45 | 1.45 | 1.45 ± 0.01 | |
| ρB after MSCS embedding [g/cm3] | 1.68 | 1.56 | 1.55 | 1.50 | 1.47 | 1.45 | 1.45 | 1.47 | 1.45 | ||
| ρB relative change [%] | 14.4 | 6.9 | 7.5 | 3.3 | 1.8 | 0.6 | 0.6 | 1.5 | 0.1 | ||
| S before MSCS embedding [MPa] | 25.9 | 25.0 | 23.3 | 24.3 | 23.5 | 23.3 | 23.2 | 23.8 | 23.9 | 24.0 ± 0.9 | |
| S after MSCS embedding [MPa] | 50.3 | 35.9 | 35.0 | 29.5 | 26.5 | 24.5 | 24.3 | 25.6 | 24.1 | ||
| S relative change [%] | 94.3 | 43.2 | 50.1 | 21.3 | 12.9 | 5.0 | 4.5 | 7.3 | 0.5 | ||
| 3 | BA/TA before MSCS embedding [%] | 40.3 | 41.9 | 39.6 | 40.7 | 38.7 | 41.7 | 41.0 | 41.4 | 39.9 | 40.6 ± 1.0 |
| BA/TA after MSCS embedding [%] | 62.9 | 58.1 | 55.9 | 52.6 | 48.5 | 42.8 | 42.1 | 42.0 | 42.6 | ||
| Change in BA/TA [%] | 22.6 | 16.2 | 16.3 | 11.9 | 9.8 * | 1.1 | 1.1 | 0.6 | 2.8 | ||
| ρB before MSCS embedding [g/cm3] | 1.34 | 1.36 | 1.34 | 1.35 | 1.33 | 1.35 | 1.35 | 1.35 | 1.34 | 1.34 ± 0.01 | |
| ρB after MSCS embedding [g/cm3] | 1.53 | 1.49 | 1.47 | 1.45 | 1.41 | 1.36 | 1.36 | 1.36 | 1.36 | ||
| ρB relative change [%] | 14.0 | 9.9 | 10.0 | 7.7 | 6.1 | 0.4 | 0.9 | 0.6 | 1.6 | ||
| S before MSCS embedding [MPa] | 14.7 | 15.8 | 14.2 | 15.0 | 13.7 | 15.7 | 15.2 | 15.4 | 14.5 | 14.9 ± 0.7 | |
| S after MSCS embedding [MPa] | 32.8 | 28.5 | 26.5 | 23.8 | 20.6 | 16.4 | 15.9 | 15.9 | 16.3 | ||
| S relative change [%] | 122.7 | 80.2 | 86.2 | 58.9 | 49.9 | 4.8 | 4.8 | 4.8 | 12.8 | ||
| 4 | BA/TA before MSCS embedding [%] | 49.7 | 50.0 | 52.2 | 54.0 | 53.1 | 51.9 | 51.4 | 50.9 | 49.9 | 51.4 ± 1.5 |
| BA/TA after MSCS embedding [%] | 67.9 | 65.0 | 64.7 | 59.0 | 57.4 | 55.3 | 55.0 | 53.7 | 53.9 | ||
| Change in BA/TA [%] | 18.2 | 15.0 | 12.5 | 4.9 * | 4.3 | 3.4 | 3.6 | 2.8 | 4.0 | ||
| ρB before MSCS embedding [g/cm3] | 1.42 | 1.43 | 1.44 | 1.46 | 1.45 | 1.44 | 1.44 | 1.43 | 1.42 | 1.44 ± 0.01 | |
| ρB after MSCS embedding [g/cm3] | 1.58 | 1.55 | 1.55 | 1.50 | 1.49 | 1.47 | 1.47 | 1.46 | 1.46 | ||
| ρB relative change [%] | 11.1 | 8.8 | 7.4 | 2.8 | 2.7 | 2.0 | 2.3 | 1.9 | 2.5 | ||
| S before MSCS embedding [MPa] | 21.5 | 21.8 | 23.5 | 25.0 | 24.2 | 23.2 | 22.8 | 22.4 | 21.6 | 22.9 ± 1.2 | |
| S after MSCS embedding [MPa] | 37.7 | 34.9 | 34.5 | 29.2 | 27.8 | 26.0 | 25.8 | 24.7 | 24.8 | ||
| S relative change [%] | 75.3 | 60.3 | 47.1 | 17.1 | 15.1 | 12.0 | 13.0 | 10.2 | 14.9 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dąbrowski, M.; Rogala, P.; Uklejewski, R.; Patalas, A.; Winiecki, M.; Gapiński, B. Subchondral Bone Relative Area and Density in Human Osteoarthritic Femoral Heads Assessed with Micro-CT before and after Mechanical Embedding of the Innovative Multi-Spiked Connecting Scaffold for Resurfacing THA Endoprostheses: A Pilot Study. J. Clin. Med. 2021, 10, 2937. https://doi.org/10.3390/jcm10132937
Dąbrowski M, Rogala P, Uklejewski R, Patalas A, Winiecki M, Gapiński B. Subchondral Bone Relative Area and Density in Human Osteoarthritic Femoral Heads Assessed with Micro-CT before and after Mechanical Embedding of the Innovative Multi-Spiked Connecting Scaffold for Resurfacing THA Endoprostheses: A Pilot Study. Journal of Clinical Medicine. 2021; 10(13):2937. https://doi.org/10.3390/jcm10132937
Chicago/Turabian StyleDąbrowski, Mikołaj, Piotr Rogala, Ryszard Uklejewski, Adam Patalas, Mariusz Winiecki, and Bartosz Gapiński. 2021. "Subchondral Bone Relative Area and Density in Human Osteoarthritic Femoral Heads Assessed with Micro-CT before and after Mechanical Embedding of the Innovative Multi-Spiked Connecting Scaffold for Resurfacing THA Endoprostheses: A Pilot Study" Journal of Clinical Medicine 10, no. 13: 2937. https://doi.org/10.3390/jcm10132937
APA StyleDąbrowski, M., Rogala, P., Uklejewski, R., Patalas, A., Winiecki, M., & Gapiński, B. (2021). Subchondral Bone Relative Area and Density in Human Osteoarthritic Femoral Heads Assessed with Micro-CT before and after Mechanical Embedding of the Innovative Multi-Spiked Connecting Scaffold for Resurfacing THA Endoprostheses: A Pilot Study. Journal of Clinical Medicine, 10(13), 2937. https://doi.org/10.3390/jcm10132937