
Transferrin Isoforms, Old but New Biomarkers in Hereditary Fructose Intolerance

 , ,
, ,  , , , , , , , and add
Show full author list
, , , , , , , and add
Show full author list
Abstract
:1. Introduction
2. Experimental Section
2.1. Participants
2.2. Study Visits
2.3. Genotype Analysis
2.4. Biochemical Analyses
2.5. Transferrin Quantification
2.6. Assessment of Diet
2.7. Statistical Analysis
3. Results
3.1. Study Visits
3.2. Biochemical Analyses
3.3. Serum Transferrin Isoforms, Hepatic Parameters and Fructose Consumption in Patients with Fructosemia
3.4. Correlations between Transferrin Isoforms, Hepatic Parameters and Fructose Consumption in Patients with Fructosemia
3.5. Diagnostic Accuracy of Serum Transferrin Isoforms in HFI
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hereditary Fructose Intolerance—StatPearls—NCBI Bookshelf. Available online: https://www.ncbi.nlm.nih.gov/books/NBK559102/ (accessed on 26 December 2020).
- Chambers, R.A.; Pratt, R.T.C. Idiosyncrasy to fructose. Lancet 1956, 268, 340. [Google Scholar] [CrossRef]
- Fagerberg, L.; Hallstrom, B.M.; Oksvold, P.; Kampf, C.; Djureinovic, D.; Odeberg, J.; Habuka, M.; Tahmasebpoor, S.; Danielsson, A.; Edlund, K.; et al. Analysis of the human tissue-specific expression by genome-wide integration of transcriptomics and antibody-based proteomics. Mol. Cell. Proteom. 2014, 13, 397–406. [Google Scholar] [CrossRef] [Green Version]
- Sánchez-Gutiérrez, J.C.; Benlloch, T.; Leal, M.A.; Samper, B.; García-Ripoll, I. Molecular analysis of the aldolase B gene in patients with hereditary fructose intolerance from Spain. J. Med Genet. 2002, 39, e56. [Google Scholar] [CrossRef] [Green Version]
- Santer, R.; Rischewski, J.; von Weihe, M.; Niederhaus, M.; Schneppenheim, S.; Baerlocher, K.; Kohlschütter, A.; Muntau, A.; Posselt, H.G.; Steinmann, B.; et al. The spectrum of aldolase B (ALDOB) mutations and the prevalence of hereditary fructose intolerance in Central Europe. Hum. Mutat. 2005, 25, 594. [Google Scholar] [CrossRef]
- Esposito, G.; Vitagliano, L.; Santamaria, R.; Viola, A.; Zagari, A.; Salvatore, F. Structural and functional analysis of aldolase B mutants related to hereditary fructose intolerance. FEBS Lett. 2002, 531, 152–156. [Google Scholar] [CrossRef] [Green Version]
- Simons, N.; Debray, F.G.; Schaper, N.C.; Kooi, M.E.; Feskens, E.J.M.; Hollak, C.E.M.; Lindeboom, L.; Koek, G.H.; Bons, J.A.P.; Lefeber, D.J.; et al. Patients with Aldolase B Deficiency Are Characterized by Increased Intrahepatic Triglyceride Content. J. Clin. Endocrinol. Metab. 2019, 104, 5056–5064. [Google Scholar] [CrossRef]
- Kim, M.J.M.S.; Moon, J.S.; Kim, M.J.M.S.; Seong, M.-W.W.; Park, S.S.; Ko, J.S. Hereditary Fructose Intolerance Diagnosed in Adulthood. Gut Liver 2020, 15, 22–25. [Google Scholar] [CrossRef] [PubMed]
- Aldámiz-Echevarría, L.; de las Heras, J.; Couce, M.L.; Alcalde, C.; Vitoria, I.; Bueno, M.; Blasco-Alonso, J.; Concepción García, M.; Ruiz, M.; Suárez, R.; et al. Non-alcoholic fatty liver in hereditary fructose intolerance. Clin. Nutr. 2020, 39, 455–459. [Google Scholar] [CrossRef] [PubMed]
- Morris, R.C. An experimental renal acidification defect in patients with hereditary fructose intolerance. I. Its resemblance to renal tubular acidosis. J. Clin. Investig. 1968, 47, 1389–1398. [Google Scholar] [CrossRef] [PubMed]
- Simons, N.; Debray, F.G.; Schaper, N.C.; Feskens, E.J.M.; Hollak, C.E.M.; Bons, J.A.P.; Bierau, J.; Houben, A.J.H.M.; Schalkwijk, C.G.; Stehouwer, C.D.A.; et al. Kidney and vascular function in adult patients with hereditary fructose intolerance. Mol. Genet. Metab. Rep. 2020, 23. [Google Scholar] [CrossRef]
- Adam, B.W.; Flores, S.R.; Hou, Y.; Allen, T.W.; De Jesus, V.R. Galactose-1-phosphate uridyltransferase dried blood spot quality control materials for newborn screening tests. Clin. Biochem. 2015, 48, 437–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaughan, S.; Ayres, L.; Baker, P.R.; Ayres, L.; Gaughan, S.; Weisfeld-Adams, J. Hereditary Fructose Intolerance; University of Washington: Seattle, WA, USA, 1993. [Google Scholar]
- Stibler, H.; Allgulander, C.; Borg, S.; Kjellin, K.G. Abnormal Microheterogeneity of Transferrin in Serum and Cerebrospinal Fluid in Alcoholism. Acta Med. Scand. 1978, 204, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Helander, A.; Wielders, J.; Anton, R.; Arndt, T.; Bianchi, V.; Deenmamode, J.; Jeppsson, J.O.; Whitfield, J.B.; Weykamp, C.; Schellenberg, F. Standardisation and use of the alcohol biomarker carbohydrate-deficient transferrin (CDT). Clin. Chim. Acta 2016, 459, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Stibler, H. Carbohydrate-Deficient Transferrin in Serum: A New Marker of Potentially Harmful Alcohol Consumption Reviewed. Clin. Chem. 1991, 37, 2029–2037. [Google Scholar] [CrossRef]
- Kawahara, H.; Matsuda, Y.; Tsuchishima, M.; Wang, X.E.; Takada, A. Effects of ethanol and acetaldehyde on the maturation of hepatic secretory glycoproteins. Alcohol. Alcoholism. 1993, 28 (Suppl. 1A), 29–35. [Google Scholar] [CrossRef]
- Kingma, H.A.; van der Sluijs, F.H.; Heiner-Fokkema, M.R. Fast screening of N-glycosylation disorders by sialotransferrin profiling with capillary zone electrophoresis. Ann. Clin. Biochem. 2018, 55, 693–701. [Google Scholar] [CrossRef]
- Bergström, J.P.; Helander, A. Influence of alcohol use, ethnicity, age, gender, BMI and smoking on the serum transferrin glycoform pattern: Implications for use of carbohydrate-deficient transferrin (CDT) as alcohol biomarker. Clin. Chim. Acta 2008, 388, 59–67. [Google Scholar] [CrossRef]
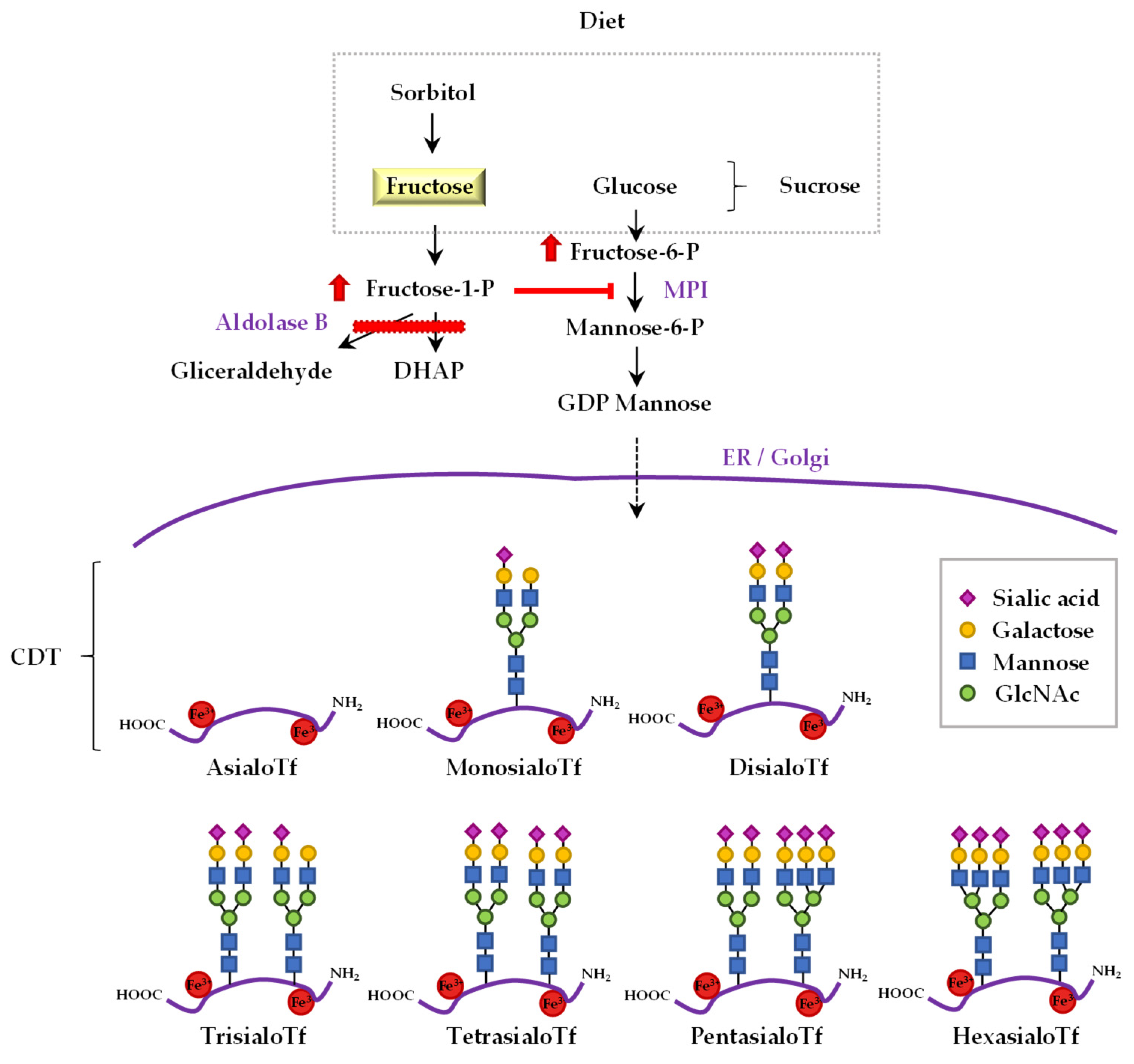
- Jaeken, J.; Pirard, M.; Adamowicz, M.; Pronicka, E.; Van Schaftingen, E. Inhibition of phosphomannose isomerase by fructose 1-phosphate: An explanation for defective N-glycosylation in hereditary fructose intolerance. Pediatr. Res. 1996, 40, 764–766. [Google Scholar] [CrossRef] [Green Version]
- Quintana, E.; Sturiale, L.; Montero, R.; Andrade, F.; Fernandez, C.; Couce, M.L.; Barone, R.; Aldamiz-Echevarria, L.; Ribes, A.; Artuch, R.; et al. Secondary disorders of glycosylation in inborn errors of fructose metabolism. J. Inherit. Metab. Dis. 2009, 32, 273–278. [Google Scholar] [CrossRef]
- Pronicka, E.; Adamowicz, M.; Kowalik, A.; Płoski, R.; Radomyska, B.; Rogaszewska, M.; Rokicki, D.; Sykut-Cegielska, J. Elevated carbohydrate-deficient transferrin (CDT) and its normalization on dietary treatment as a useful biochemical test for hereditary fructose intolerance and galactosemia. Pediatr. Res. 2007, 62, 101–105. [Google Scholar] [CrossRef] [Green Version]
- Adamowicz, M.; Pronicka, E. Carbohydrate deficient glycoprotein syndrome-like transferrin isoelectric focusing pattern in untreated fructosaemia. Eur. J. Pediatr. 1996, 155, 347–348. [Google Scholar] [CrossRef] [PubMed]
- Adamowicz, M.; Płoski, R.; Rokicki, D.; Morava, E.; Gizewska, M.; Mierzewska, H.; Pollak, A.; Lefeber, D.J.; Wevers, R.A.; Pronicka, E.; et al. Transferrin hypoglycosylation in hereditary fructose intolerance: Using the clues and avoiding the pitfalls. J. Inherit. Metab. Dis. 2007, 30, 407. [Google Scholar] [CrossRef] [PubMed]
- Di Dato, F.; Spadarella, S.; Puoti, M.G.; Caprio, M.G.; Pagliardini, S.; Zuppaldi, C.; Vallone, G.; Fecarotta, S.; Esposito, G.; Iorio, R.; et al. Daily fructose traces intake and liver injury in children with hereditary fructose intolerance. Nutrients 2019, 11, 2397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Medical Association. World Medical Association declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA J. Am. Med. Assoc. 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esposito, G.; Imperato, M.R.; Ieno, L.; Sorvillo, R.; Benigno, V.; Parenti, G.; Parini, R.; Vitagliano, L.; Zagari, A.; Salvatore, F. Hereditary fructose intolerance: Functional study of two novel ALDOB natural variants and characterization of a partial gene deletion. Hum. Mutat. 2010, 31, 1294–1303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ALCE INGENIERIA. Available online: https://www.alceingenieria.net/nutricion/descarga.htm (accessed on 3 March 2021).
- Browse Foods. Available online: https://www.foodstandards.gov.au/science/monitoringnutrients/afcd/Pages/foodsearch.aspx (accessed on 3 March 2021).
- Frida—Food Data Published by DTU Food. Available online: https://frida.fooddata.dk/?lang=en (accessed on 3 March 2021).
- Food Composition and Nutrition Tables (Libro, 2000) [WorldCat.org]. Available online: https://www.worldcat.org/title/food-composition-and-nutrition-tables/oclc/44076134 (accessed on 3 March 2021).
- Organizador Dietético Metabólico. Available online: http://www.odimet.es/ (accessed on 3 March 2021).
- Da Lozzo, P.; Magnolato, A.; Del Rizzo, I.; Sirchia, F.; Bruno, I.; Barbi, E. When Long-Lasting Food Selectivity Leads to an Unusual Genetic Diagnosis: A Case Report. J. Adolesc. Health 2019, 64, 137–138. [Google Scholar] [CrossRef]
- Marquardt, T.; Denecke, J. Congenital disorders of glycosylation: Review of their molecular bases, clinical presentations and specific therapies. Eur. J. Pediatr. 2003, 162, 359–379. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Controls | HFI Patients | p-Value | |
|---|---|---|---|
| n | 32 | 37 | |
| Women/men, n/n | 19/13 | 22/15 | 0.594 |
| Age, year | 21.5 ± 15.1 (2.1–61.3) | 19.7 ± 14.8 (3.7–63.4) | 0.629 |
| Weight, kg | 50.5 ± 15.3 (11.9–71.0) | 45.3 ± 16.4 (17–73) | 0.178 |
| Height, cm | 155.5 ± 19.5 (85.5–181.0) | 151.0 ± 21.1(104.2–190.7) | 0.368 |
| BMI, kg/m2 | 20.2 ± 3.2 (14.6–27.1) | 19.0 ± 3.1 (14.0–27.4) | 0.107 |
| Waist circumference, cm | 68.3 ± 9.4 (48–88) | 67.5 ± 9.7 (51–87) | 0.736 |
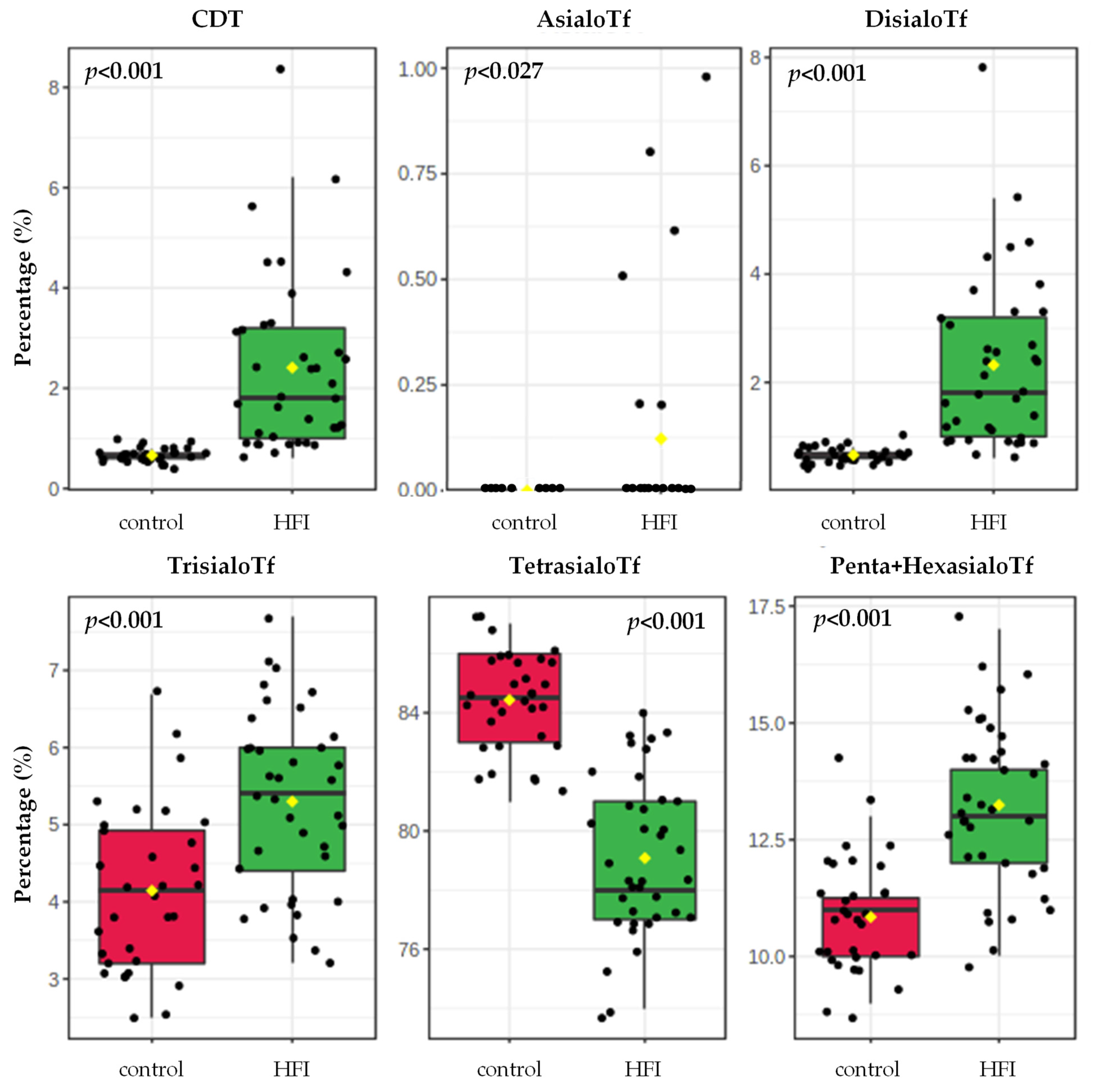
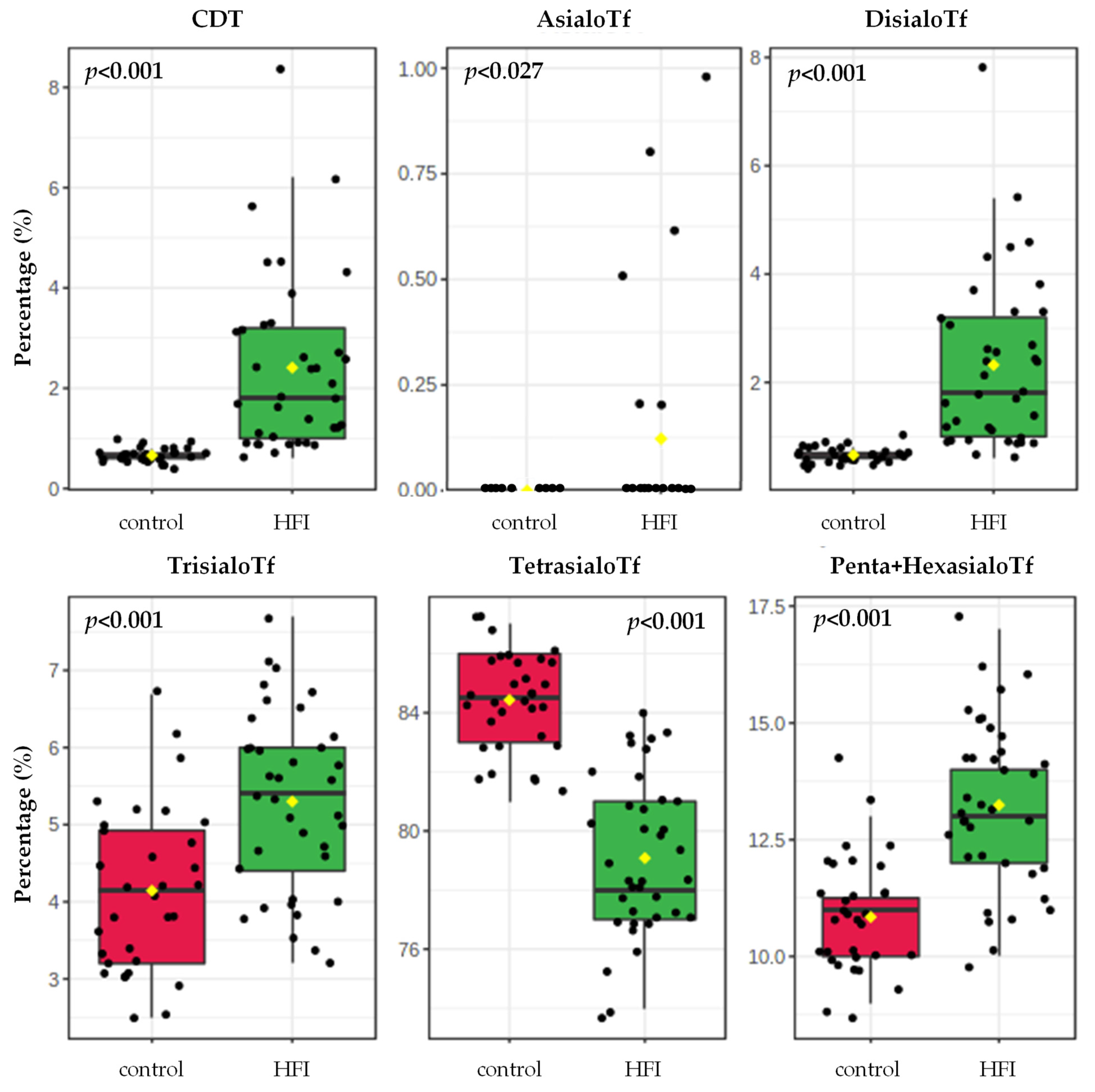
| CDT, % (asialoTf + disialoTf) | 0.7 ± 0.1 (0.4–1.0) | 2.4 ± 1.8 (0.6–8.4) 9 | <0.001 |
| AsialoTf, % | 0.0 ± 0.0 (0.0–0.0) | 0.10 ± 0.3 (0.0–0.1) | 0.027 |
| DisialoTf, % | 0.7 ± 0.1 (0.4–1.0) | 2.3 ± 1.6 (0.6–7.8) | <0.001 |
| TrisialoTf, % | 4.4 ± 1.7 (2.5–6.7) | 5.3 ± 1.2 (3.2–7.7) | <0.001 |
| TetrasialoTf, % | 84.4 ± 1.6 (81–87) | 79.0 ± 2.7 (74–84) | <0.001 |
| Penta- and hexa-sialoTf, % | 10.8 ± 1.1 (9.0–14.1) | 13.3 ± 1.7 (10.3–17.1) | <0.001 |
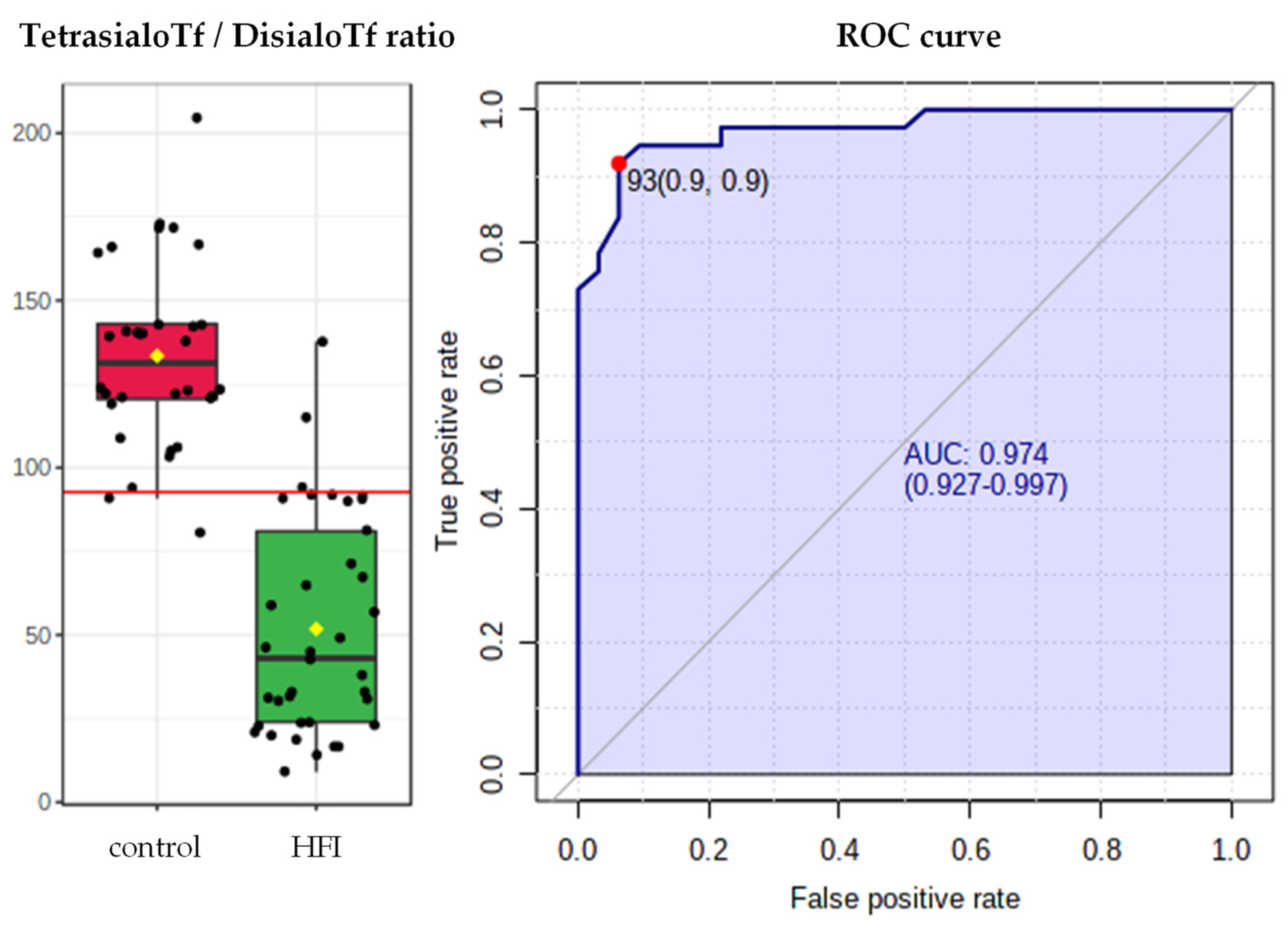
| Tetra-/di-sialoTf | 133.4 ± 27.7 (81.3–204.8) | 51.8 ± 32.9 (9.4–137.5) | <0.001 |
| Serum iron (mg/dL) | 98.7 ± 39.7 (34–205) | 85.3 ± 30.6 (53–216) | 0.133 |
| Tf (mg/dL) | 270.9 ± 37.8 (210–397) | 288.1 ± 36.5 (222–378) | 0.064 |
| Ferritin (mg/dL) | 50.4 ± 37.9 (10–176) | 73.2 ± 73.4 (4–284) | 0.124 |
| HFI Patients all Together | FSS-Intake 1st Tertile | FSS-Intake 2nd Tertile | FSS-Intake 3rd Tertile | p | |
|---|---|---|---|---|---|
| n | 34 | 12 | 11 | 11 | |
| Fructose intake (mg/day) | 322 ± 304 (0–1323) | 70 ± 78 (0–220) | 296 ± 161 (98–604) | 621 ± 311 (238–1323) | <0.001 |
| Sucrose intake (mg/day) | 503 ± 651 (15–3747) | 131 ± 99 (15–308) | 378 ± 70 (255–530) | 1032 ± 944 (344–3747) | <0.001 |
| Sorbitol intake (mg/day) | 50 ± 93 (0–443) | 11 ± 20 (0–57) | 32 ± 40 (0–90) | 11 ± 142 (0–443) | 0.049 |
| FSS intake (mg/day) | 1764 ± 938 (15–4366) | 212 ± 157 (15–446) | 707 ± 193 (457–936) | 1764 ± 937 (1020–4366) | <0.001 |
| AsialoTf, % | 0.08 ± 0.25 (0–0.8) | 0.08 ± 0.21 (0.0–0.6) | 0.09 ± 0.22 (0.0–0.8) | 0.14 ± 0.32 (0.00–1.00) | 0.934 |
| DisialoTf, % | 2.3 ± 1.6 (0.6–7.8) | 2.2 ± 2 (0.6–7.8) | 2.4 ± 1.5 (0.9–5.4) | 2.3 ± 1.3 (0.9–4.6) | 0.612 |
| TrisialoTf, % | 5.3 ± 1.2 (3.2–7.7) | 5.1 ± 1.1 (3.4–6.8) | 5.2 ± 1.2 (3.2–7.1) | 5.7 ± 1.1 (4.0–7.7) | 0.395 |
| TetrasialoTf, % | 79.0 ± 2.7 (73.7–84.3) | 78.6 ± 2.9 (73.7–82.5) | 79.6 ± 2.9 (74.4–84.3) | 78.7 ± 2.1 (76.7–82.7) | 0.674 |
| Penta- and hexa-sialoTf, % | 13.3 ± 1.7 (10.3–17.1) | 14.1 ± 1.8 (10.8–17.1) | 12.7 ± 1.6 (10.3–15.9) | 13.1 ± 1.5 (10.37–14.6) | 0.262 |
| Tetra-/di-sialoTf | 51.8 ± 32.9 (9.4–137.5) | 62.2 ± 40.8 (9.4–137.5) | 47.3 ± 29.1 (13.8–93.7) | 46.1 ± 27.9 (16.7–91.9) | 0.758 |
| GGT (U/L) | 15.3 ± 5.9 (9–36) | 17.4 ± 8.2 (9–36) | 14.4 ± 4.9 (9–27) | 14.2 ± 3.5 (10–21) | 0.221 |
| GOT, AST (U/L) | 26.5 ± 9.5 (16–66) | 45.8 ± 30.4 (19–45) | 28.5 ± 4.8 (19–33) | 27.9 ± 4.7 (16–66) | 0.322 |
| GPT, ALT (U/L) | 30.4 ± 31.4 (9–198) | 44.3 ± 50.7 (16–198) | 22.8 ± 9.5 (10–47) | 24.7 ± 15.7 (9–68) | 0.234 |
| INR | 1.00 ± 0.08 (0.9–1.1) | 0.96 ± 0.08 (0.9–1.1) | 1.00 ± 0.67 (0.9–1.1) | 1.00 ± 0.77 (0.9–1.1) | 0.151 |
| No AsialoTf Expression | AsialoTf Expression | p-Value | |
|---|---|---|---|
| Fructose intake (mg/day) | 354 ± 321 (0–1323) | 434 ± 327 (220–620) | 0.254 |
| Sucrose intake (mg/day) | 434 ± 327 (15–1334) | 1096 ± 1496 (117–3747) | 0.232 |
| Sorbitol intake (mg/day) | 64 ± 104 (0–443) | 19 ± 41 (0–93) | 0.192 |
| FSS intake (mg/day) | 868 ± 596 (15–2119) | 1535 ± 1618 (337–4366) | 0.487 |
| GGT (U/L) | 15.5 ± 6.1 (9–36) | 14.7 ± 5.2 (9–21) | 1 |
| GOT, AST (U/L) | 27.2 ± 10.3 (13–66) | 23 ± 2.8 (19–27) | 0.606 |
| GPT, ALT (U/L) | 31.5 ± 34.2 (9–198) | 24.7 ± 6.2 (19–35) | 0.223 |
| INR | 1.0 ± 0.1 (0.9–1.1) | 1.0 ± 0.1 (1.0–1.1) | 0.295 |
| CDT, % (asialoTf+disialoTf) | 1.8 ± 1.0 (0.6–4.5) | 5.5 ± 1.7 (3.9–8.4) | <0.001 |
| AsialoTf, % | 0 | 0.6 ± 0.3 (0.2–1.0) | <0.001 |
| DisialoTf, % | 1.8 ± 1.0 (0.6–4.5) | 4.9 ± 1.5 (3.7–7.8) | <0.001 |
| TrisialoTf, % | 5.3 ± 1.2 (3.2–7.7) | 5.6 ± 1.2 (4.0–7.1) | 0.575 |
| TetrasialoTf, % | 79.5 ± 2.5 (76.5–84.3) | 76.5 ± 2.2 (73.5–79.8) | 0.005 |
| Penta- and hexa-sialoTf, % | 58.6 ± 31.7 (10.3–17.1) | 16.6 ± 4.3 (10.3–14.4) | 0.427 |
| Tetra-/di-sialoTf | 13.4 ± 1.7 (17.0–137.5) | 12.5 ± 1.6 (9.4–20.9) | <0.001 |
| Dietary Intake | CDT, % | A-Tf, % | Di-Tf, % | Tri-Tf, % | Tetra-Tf, % | Penta- and Hexa-Tf, % | Tetra-/di-Tf Ratio | |
|---|---|---|---|---|---|---|---|---|
| Fructose | R | 0.063 | 0.107 | 0.046 | 0.244 | 0.092 | −0.386 | −0.085 |
| p | 0.725 | 0.573 | 0.794 | 0.169 | 0.606 | 0.024 | 0.631 | |
| Sucrose | R | 0.242 | 0.575 | 0.18 | 0.238 | −0.073 | −0.303 | −0.187 |
| p | 0.168 | <0.001 | 0.309 | 0.175 | 0.68 | 0.08 | 0.29 | |
| Sorbitol | R | −0.197 | −0.175 | −0.197 | −0.181 | 0.361 | −0.253 | 0.209 |
| p | 0.264 | 0.354 | 0.264 | 0.305 | 0.036 | 0.15 | 0.236 | |
| FSS | R | 0.187 | 0.475 | 0.133 | 0.25 | 0.016 | −0.4 | −0.151 |
| p | 0.29 | 0.008 | 0.453 | 0.154 | 0.929 | 0.019 | 0.392 | |
| Liver Parameters | ||||||||
| GGT | R | 0.061 | 0.006 | 0.077 | 0.049 | −0.12 | 0.091 | −0.107 |
| p | 0.719 | 0.974 | 0.653 | 0.774 | 0.48 | 0.592 | 0.528 | |
| GOT (AST) | R | −0.213 | −0.135 | −0.212 | −0.004 | 0.184 | −0.059 | 0.184 |
| p | 0.212 | 0.453 | 0.214 | 0.982 | 0.282 | 0.733 | 0.281 | |
| GPT (ALT) | R | 0.044 | −0.01 | 0.061 | 0.076 | −0.185 | 0.193 | −0.092 |
| p | 0.795 | 0.955 | 0.72 | 0.656 | 0.272 | 0.253 | 0.587 | |
| INR | R | −0.026 | 0.082 | −0.033 | −0.064 | −0.055 | 0.162 | 0.103 |
| p | 0.882 | 0.662 | 0.849 | 0.717 | 0.752 | 0.351 | 0.555 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cano, A.; Alcalde, C.; Belanger-Quintana, A.; Cañedo-Villarroya, E.; Ceberio, L.; Chumillas-Calzada, S.; Correcher, P.; Couce, M.L.; García-Arenas, D.; Gómez, I.; et al. Transferrin Isoforms, Old but New Biomarkers in Hereditary Fructose Intolerance. J. Clin. Med. 2021, 10, 2932. https://doi.org/10.3390/jcm10132932
Cano A, Alcalde C, Belanger-Quintana A, Cañedo-Villarroya E, Ceberio L, Chumillas-Calzada S, Correcher P, Couce ML, García-Arenas D, Gómez I, et al. Transferrin Isoforms, Old but New Biomarkers in Hereditary Fructose Intolerance. Journal of Clinical Medicine. 2021; 10(13):2932. https://doi.org/10.3390/jcm10132932
Chicago/Turabian StyleCano, Ainara, Carlos Alcalde, Amaya Belanger-Quintana, Elvira Cañedo-Villarroya, Leticia Ceberio, Silvia Chumillas-Calzada, Patricia Correcher, María Luz Couce, Dolores García-Arenas, Igor Gómez, and et al. 2021. "Transferrin Isoforms, Old but New Biomarkers in Hereditary Fructose Intolerance" Journal of Clinical Medicine 10, no. 13: 2932. https://doi.org/10.3390/jcm10132932
APA StyleCano, A., Alcalde, C., Belanger-Quintana, A., Cañedo-Villarroya, E., Ceberio, L., Chumillas-Calzada, S., Correcher, P., Couce, M. L., García-Arenas, D., Gómez, I., Hernández, T., Izquierdo-García, E., Martínez Chicano, D., Morales, M., Pedrón-Giner, C., Petrina Jáuregui, E., Peña-Quintana, L., Sánchez-Pintos, P., Serrano-Nieto, J., ... de las Heras, J. (2021). Transferrin Isoforms, Old but New Biomarkers in Hereditary Fructose Intolerance. Journal of Clinical Medicine, 10(13), 2932. https://doi.org/10.3390/jcm10132932