
Spectral-Domain Optical Coherence Tomography Assessment in Treatment-Naïve Patients with Clinically Isolated Syndrome and Different Multiple Sclerosis Types: Findings and Relationship with the Disability Status

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Spectral-Domain Optical Coherence Tomography (SD-OCT) Assessment
2.3. Statistical Analysis
3. Results
3.1. Demographic and Clinical Features
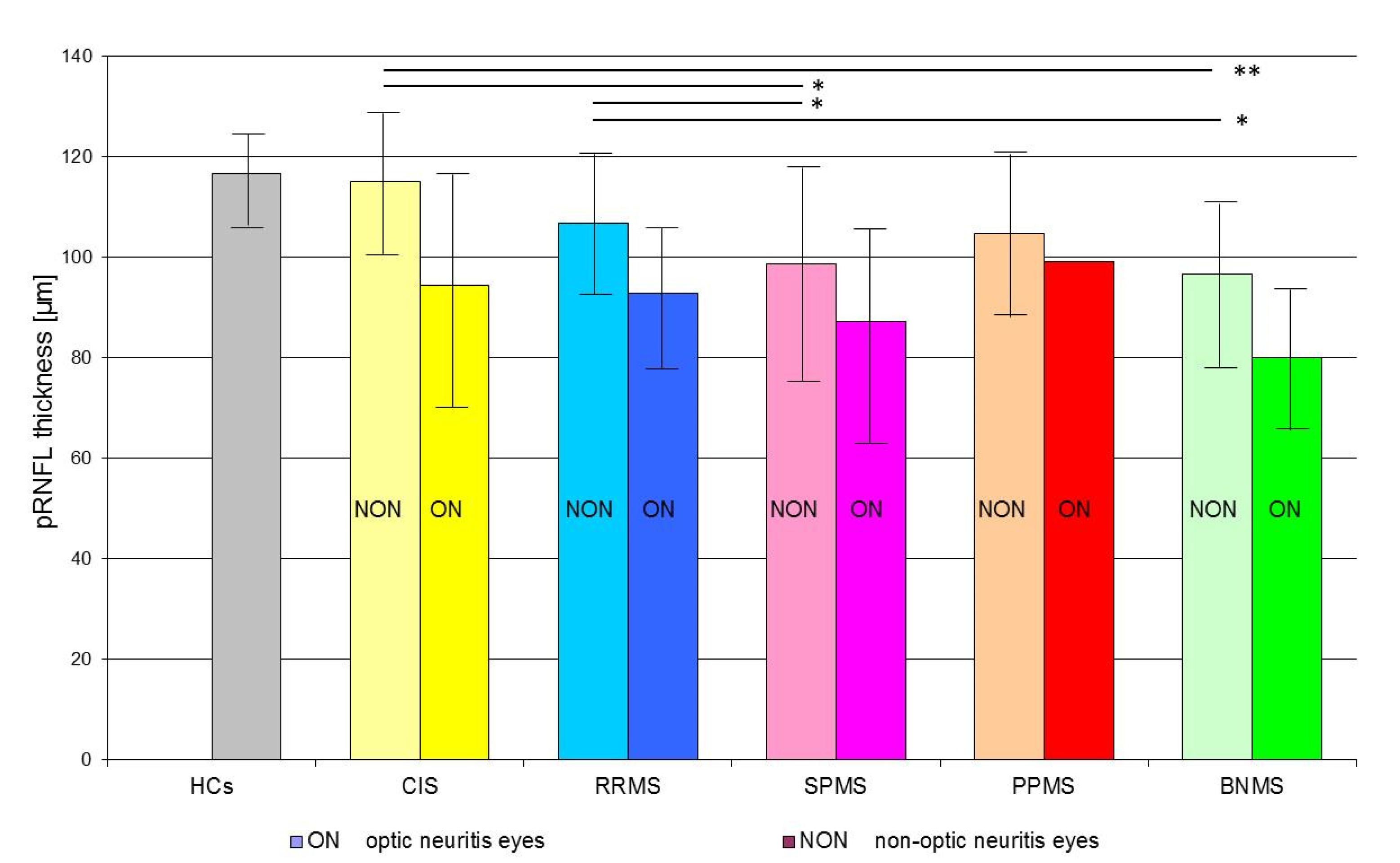
3.2. SD-OCT Peripapillary Retinal Nerve Fiber Layer Data
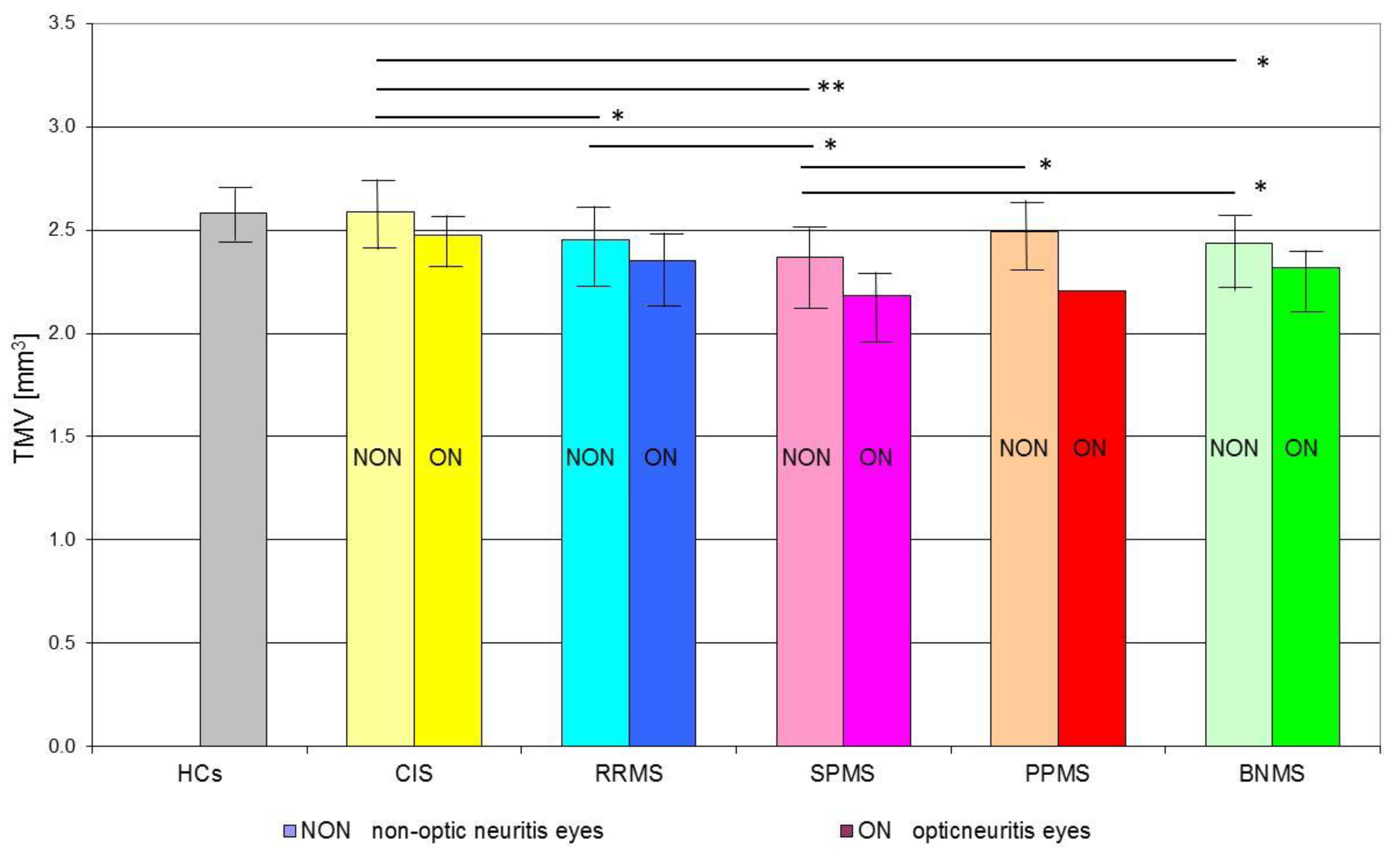
3.3. SD-OCT Total Macular Volume Data
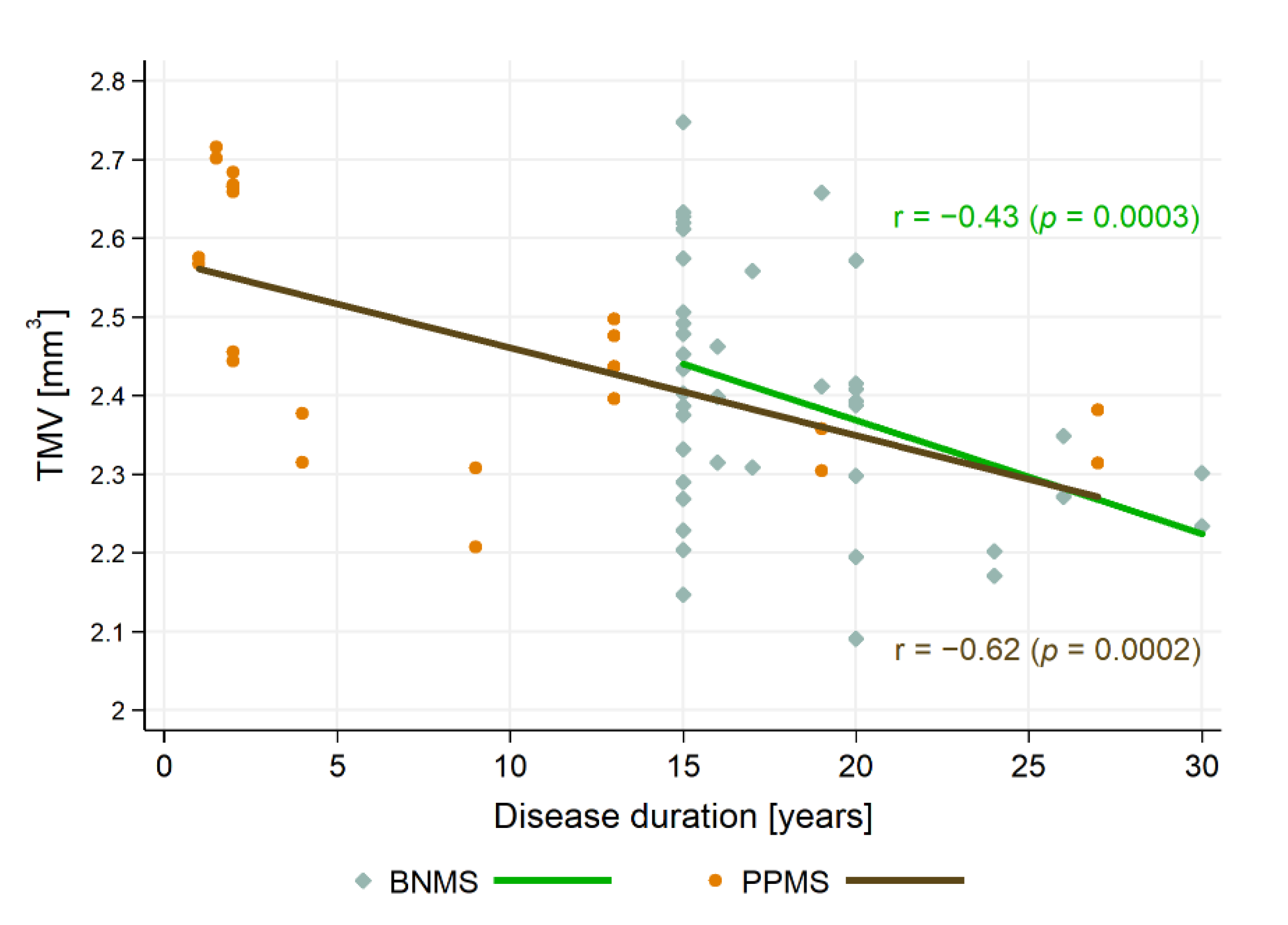
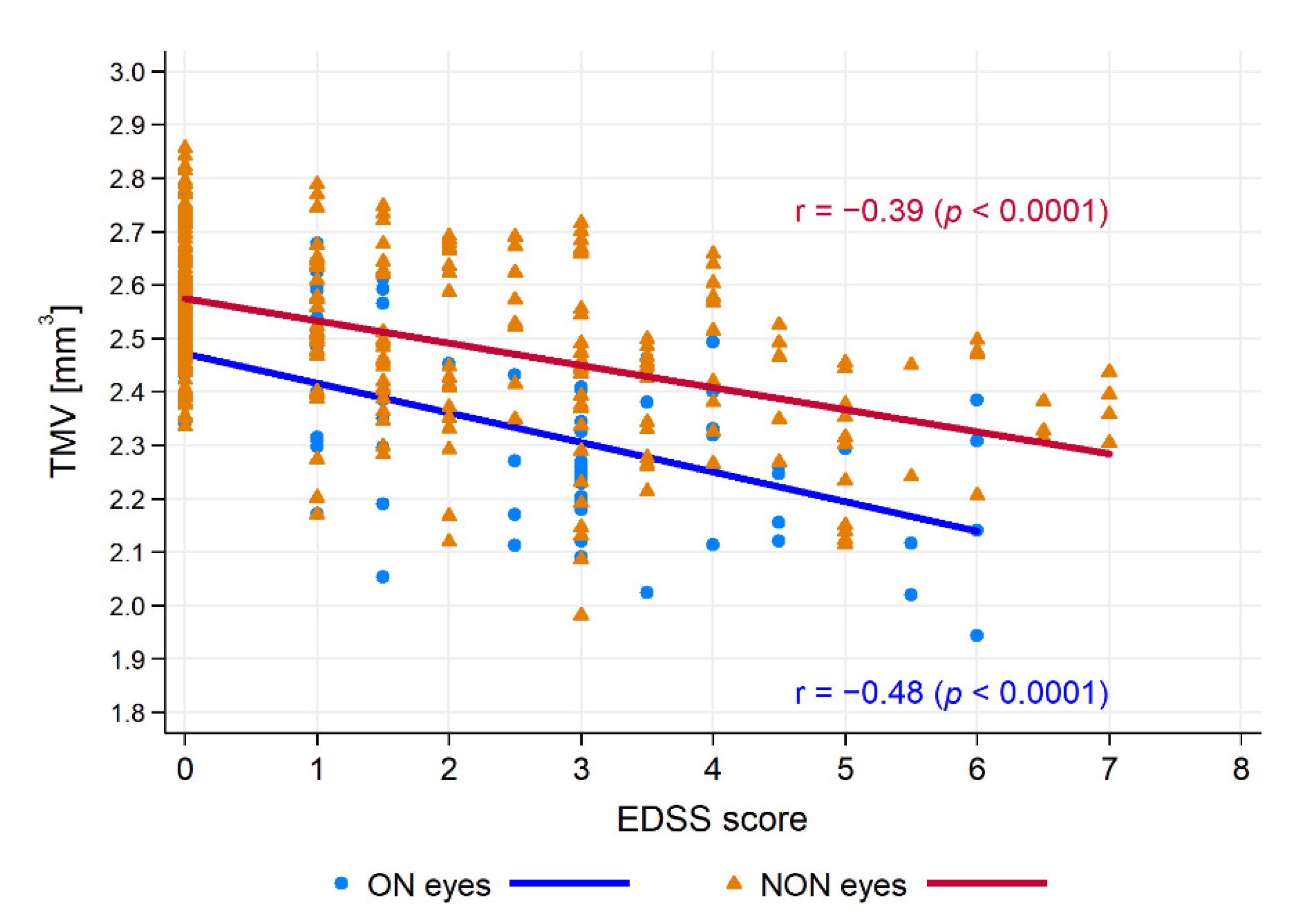
3.4. Relationship between SD-OCT Data and Clinical Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Costello, F.; Burton, J.M. Retinal imaging with optical coherence tomography: A biomarker in multiple sclerosis? Eye Brain 2018, 10, 47–63. [Google Scholar] [CrossRef] [Green Version]
- Montalban, X.; Gold, R.; Thompson, A.J.; Otero-Romero, S.; Amato, M.P.; Chandraratna, D.; Clanet, M.; Comi, G.; Derfuss, T.; Fazekas, F.; et al. ECTRIMS/EAN guideline on the pharmacological treatment of people with multiple sclerosis. Eur. J. Neurol. 2018, 25, 215–237. [Google Scholar] [CrossRef] [Green Version]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef]
- Lublin, F.D.; Reingold, S.C. Defining the clinical course of multiple sclerosis: Results of an international survey. National Multiple Sclerosis Society (USA) Advisory Committee on Clinical Trials of New Agents in Multiple Sclerosis. Neurology 1996, 46, 907–911. [Google Scholar] [CrossRef] [PubMed]
- Confavreux, C.; Vukusic, S. Natural history of multiple sclerosis: A unifying concept. Brain 2006, 129 Pt 3, 606–616. [Google Scholar] [CrossRef] [Green Version]
- Miller, D.; Leary, S. Primary-progressive multiple sclerosis. Lancet Neurol. 2007, 6, 903–912. [Google Scholar] [CrossRef]
- Crielaard, L.; Kavaliunas, A.; Ramanujam, R.; Olsson, T.; Hillert, J.; Stridh, P.; Kockum, I.; Manouchehrinia, A. Factors associated with and long-term outcome of benign multiple sclerosis: A nationwide cohort study. J. Neurol. Neurosurg. Psychiatry 2019, 90, 761–767. [Google Scholar] [CrossRef]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef] [Green Version]
- Glad, S.B.; Aarseth, J.H.; Nyland, H.; Riise, T.; Myhr, K.M. Benign multiple sclerosis: A need for a consensus. Acta Neurol. Scand. Suppl. 2010, 190, 44–50. [Google Scholar] [CrossRef]
- Huang-Link, Y.M.; Fredrikson, M.; Link, H. Benign Multiple Sclerosis is Associated with Reduced Thinning of the Retinal Nerve Fiber and Ganglion Cell Layers in Non-Optic-Neuritis Eyes. J. Clin. Neurol. 2015, 11, 241–247. [Google Scholar] [CrossRef] [Green Version]
- Rzepiński, Ł.; Zawadka-Kunikowska, M.; Maciejek, Z.; Newton, J.L.; Zalewski, P. Early Clinical Features, Time to Secondary Progression, and Disability Milestones in Polish Multiple Sclerosis Patients. Medicina 2019, 55, 232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dekker, I.; Eijlers, A.J.C.; Popescu, V.; Balk, L.J.; Vrenken, H.; Wattjes, M.P.; Uitdehaag, B.M.J.; Killestein, J.; Geurts, J.J.G.; Barkhof, F.; et al. Predicting clinical progression in multiple sclerosis after 6 and 12 years. Eur. J. Neurol. 2019, 26, 893–902. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ontaneda, D.; Fox, R.J. Progressive multiple sclerosis. Curr. Opin. Neurol. 2015, 28, 237–243. [Google Scholar] [CrossRef] [Green Version]
- Choi, J.Y.; Jeong, I.H.; Oh, S.H.; Oh, C.H.; Park, N.Y.; Kim, H.J.; Lee, J. Evaluation of Normal-Appearing White Matter in Multiple Sclerosis Using Direct Visualization of Short Transverse Relaxation Time Component (ViSTa) Myelin Water Imaging and Gradient Echo and Spin Echo (GRASE) Myelin Water Imaging. J. Magn. Reson. Imaging 2019, 49, 1091–1098. [Google Scholar] [CrossRef]
- Petzold, A.; Balcer, L.J.; Calabresi, P.A.; Costello, F.; Frohman, T.C.; Frohman, E.M.; Martinez-Lapiscina, E.H.; Green, A.J.; Kardon, R.; Outteryck, O.; et al. Retinal layer segmentation in multiple sclerosis: A systematic review and meta-analysis. Lancet Neurol. 2017, 16, 797–812. [Google Scholar] [CrossRef] [Green Version]
- Kucharczuk, J.; Maciejek, Z.; Sikorski, B.L. Optical coherence tomography in diagnosis and monitoring multiple sclerosis. Neurol. Neurochir. Pol. 2018, 52, 140–149. [Google Scholar] [CrossRef]
- Salobrar-Garcia, E.; Hoyas, I.; Leal, M.; de Hoz, R.; Rojas, B.; Ramirez, A.I.; Salazar, J.J.; Yubero, R.; Gil, P.; Triviño, A.; et al. Analysis of Retinal Peripapillary Segmentation in Early Alzheimer’s Disease Patients. BioMed Res. Int. 2015, 2015, 636548. [Google Scholar] [CrossRef] [Green Version]
- Salobrar-García, E.; Ramírez, A.I.; de Hoz, R.; Rojas, P.; Salazar, J.; Rojas, B.; Yubero, R.; Gil, P.; Triviño, A.; Ramírez, J.M. The Impact of the Eye in Dementia: The Eye and its Role in Diagnosis and Follow-Up; Moretti, D., Ed.; Update on Dementia; InTech: London, UK, 2016; pp. 379–426. [Google Scholar]
- Jáñez-Escalada, L.; Jáñez-García, L.; Salobrar-García, E.; Santos-Mayo, A.; de Hoz, R.; Yubero, R.; Gil, P.; Ramírez, J.M. Spatial analysis of thickness changes in ten retinal layers of Alzheimer’s disease patients based on optical coherence tomography. Sci. Rep. 2019, 9, 13000. [Google Scholar] [CrossRef] [PubMed]
- Salobrar-García, E.; de Hoz, R.; Ramírez, A.I.; López-Cuenca, I.; Rojas, P.; Vazirani, R.; Amarante, C.; Yubero, R.; Gil, P.; Pinazo-Durán, M.D.; et al. Changes in visual function and retinal structure in the progression of Alzheimer’s disease. PLoS ONE 2019, 14, e0220535. [Google Scholar] [CrossRef] [Green Version]
- Green, A.J.; McQuaid, S.; Hauser, S.L.; Allen, I.V.; Lyness, R. Ocular pathology in multiple sclerosis: Retinal atrophy and inflammation irrespective of disease duration. Brain 2010, 133, 1591–1601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Britze, J.; Pihl-Jensen, G.; Frederiksen, J.L. Retinal ganglion cell analysis in multiple sclerosis and optic neuritis: A systematic review and meta-analysis. J. Neurol. 2017, 264, 1837–1853. [Google Scholar] [CrossRef] [PubMed]
- Button, J.; Al-Louzi, O.; Lang, A.; Bhargava, P.; Newsome, S.D.; Frohman, T.; Balcer, L.J.; Frohman, E.M.; Prince, J.; Calabresi, P.A.; et al. Disease modifying therapies modulate retinal atrophy in multiple sclerosis. Neurology 2017, 88, 525–532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balk, L.J.; Tewarie, P.; Killestein, J.; Polman, C.H.; Uitdehaag, B.; Petzold, A. Disease course heterogeneity and OCT in multiple sclerosis. Mult. Scler. 2014, 20, 1198–1206. [Google Scholar] [CrossRef]
- Galetta, K.M.; Graves, J.; Talman, L.S.; Lile, D.J.; Frohman, E.M.; Calabresi, P.A.; Galetta, S.L.; Balcer, L.J. Visual pathway axonal loss in benign multiple sclerosis: A longitudinal study. J. Neuroophthalmol. 2012, 32, 116–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reynders, T.; D’haeseleer, M.; De Keyser, J.; Nagels, G.; D’hooghe, M.B. Definition, prevalence and predictive factors of benign multiple sclerosis. eNeurologicalSci 2017, 7, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Polman, C.H.; Reingold, S.C.; Banwell, B.; Clanet, M.; Cohen, J.A.; Filippi, M.; Fujihara, K.; Havrdova, E.; Hutchinson, M.; Kappos, L.; et al. Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteria. Ann. Neurol. 2011, 69, 292–302. [Google Scholar] [CrossRef] [Green Version]
- Schippling, S.; Balk, L.J.; Costello, F. Quality control for retinal OCT in multiple sclerosis: Validation of the OSCAR-IB criteria. Mult. Scler. 2015, 21, 163–170. [Google Scholar] [CrossRef] [Green Version]
- Cruz-Herranz, A.; Balk, L.J.; Oberwahrenbrock, T.; Saidha, S.; Martinez-Lapiscina, E.H.; Lagreze, W.A.; Schuman, J.S.; Villoslada, P.; Calabresi, P.; Balcer, L.; et al. The APOSTEL recommendations for reporting quantitative optical coherence tomography studies. Neurology 2016, 86, 2303–2309. [Google Scholar] [CrossRef]
- Zhu, W. p < 0.05, < 0.01, < 0.001, < 0.0001, < 0.00001, < 0.000001, or < 0.0000001 …. J. Sport Health Sci. 2016, 5, 77–79. [Google Scholar] [CrossRef] [Green Version]
- Chan, J.K.; Lapiscina, E.H.M.D.; Taylor, C.; Nguyen, A.L.; Alba-Arbalat, S.; Devonshire, V.; Sayao, A.L.; Carruthers, R.; Costello, F.; Traboulsee, A. Long-Term Stability of Neuroaxonal Structure in Alemtuzumab-Treated Relapsing-Remitting Multiple Sclerosis Patients. J. Neuroophthalmol. 2020, 40, 37–43. [Google Scholar] [CrossRef]
- Zivadinov, R.; Tavazzi, E.; Hagemeier, J.; Carl, E.; Hojnacki, D.; Kolb, C.; Weinstock-Guttman, B. The Effect of Glatiramer Acetate on Retinal Nerve Fiber Layer Thickness in Patients with Relapsing-Remitting Multiple Sclerosis: A Longitudinal Optical Coherence Tomography Study. CNS Drugs 2018, 32, 763–770. [Google Scholar] [CrossRef]
- Egawa, N.; Lok, J.; Washida, K.; Arai, K. Mechanisms of Axonal Damage and Repair after Central Nervous System Injury. Transl. Stroke Res. 2017, 8, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Li, H.Y.; Ruan, Y.W.; Ren, C.R.; Cui, Q.; So, K.F. Mechanisms of secondary degeneration after partial optic nerve transection. Neural Regen. Res. 2014, 9, 565–574. [Google Scholar] [CrossRef] [PubMed]
- Nakahara, J. Remyelination in multiple sclerosis: Pathology and treatment strategies. Clin. Exp. Neuroimmunol. 2017, 8, 40–46. [Google Scholar] [CrossRef] [Green Version]
- Rothman, A.; Murphy, O.C.; Fitzgerald, K.C.; Button, J.; Gordon-Lipkin, E.; Ratchford, J.N.; Newsome, S.D.; Mowry, E.M.; Sotirchos, E.S.; Syc-Mazurek, S.B.; et al. Retinal measurements predict 10-year disability in multiple sclerosis. Ann. Clin. Transl. Neurol. 2019, 6, 222–232. [Google Scholar] [CrossRef] [Green Version]
- Thabit, M.N.; Farouk, M.M.; Awni, M.; Al-Amir Bassiouny, M. Early disability in ambulatory patients with multiple sclerosis: Optical coherence tomography versus visual evoked potentials, a comparative study. Egypt. J. Neurol. Psychiatry Neurosurg. 2020, 56, 70. [Google Scholar] [CrossRef]
- Kale, N. Optic neuritis as an early sign of multiple sclerosis. Eye Brain 2016, 8, 195–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balcer, L.J. Optic neuritis. N. Engl. J. Med. 2006, 354, 1273–1280. [Google Scholar] [CrossRef] [PubMed]
- Pulicken, M.; Gordon-Lipkin, E.; Balcer, L.J.; Frohman, E.; Cutter, G.; Calabresi, P.A. Optical coherence tomography and disease subtype in multiple sclerosis. Neurology 2007, 69, 2085–2092. [Google Scholar] [CrossRef] [PubMed]
- Eslami, F.; Ghiasian, M.; Khanlarzade, E.; Moradi, E. Retinal Nerve Fiber Layer Thickness and Total Macular Volume in Multiple Sclerosis Subtypes and Their Relationship with Severity of Disease, a Cross-Sectional Study. Eye Brain 2020, 12, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Oberwahrenbrock, T.; Schippling, S.; Ringelstein, M.; Kaufhold, F.; Zimmermann, H.; Keser, N.; Young, K.L.; Harmel, J.; Hartung, H.P.; Martin, R.; et al. Retinal damage in multiple sclerosis disease subtypes measured by high-resolution optical coherence tomography. Mult. Scler. Int. 2012, 530305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costello, F.; Hodge, W.; Pan, Y.I.; Eggenberger, E.; Freedman, M.S. Using retinal architecture to help characterize multiple sclerosis patients. Can. J. Ophthalmol. 2010, 45, 520–526. [Google Scholar] [CrossRef]
- Henderson, A.P.D.; Trip, S.A.; Schlottmann, P.G.; Altmann, D.R.; Garway-Heath, D.F.; Plant, G.T.; Miller, D.H. A preliminary longitudinal study of the retinal nerve fiber layer in progressive multiple sclerosis. J. Neurol. 2010, 257, 1083–1091. [Google Scholar] [CrossRef]
- Bsteh, G.; Hegen, H.; Teuchner, B.; Amprosi, M.; Berek, K.; Ladstätter, F.; Wurth, S.; Auer, M.; Di Pauli, F.; Deisenhammer, F.; et al. Peripapillary retinal nerve fibre layer as measured by optical coherence tomography is a prognostic biomarker not only for physical but also for cognitive disability progression in multiple sclerosis. Mult. Scler. 2019, 25, 196–203. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Lapiscina, E.H.; Arnow, S.; Wilson, J.A.; Saidha, S.; Preiningerova, J.L.; Oberwahrenbrock, T.; Brandt, A.U.; Pablo, L.E.; Guerrieri, S.; Gonzalez, I.; et al. Retinal thickness measured with optical coherence tomography and risk of disability worsening in multiple sclerosis: A cohort study. Lancet Neurol. 2016, 15, 574–584. [Google Scholar] [CrossRef] [Green Version]
- Verticchio Vercellin, A.C.; Jassim, F.; Poon, L.Y.; Tsikata, E.; Braaf, B.; Shah, S.; Ben-David, G.; Shieh, E.; Lee, R.; Simavli, H.; et al. Diagnostic Capability of Three-Dimensional Macular Parameters for Glaucoma Using Optical Coherence Tomography Volume Scans. Investig. Ophthalmol. Vis. Sci. 2018, 59, 4998–5010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kapica-Topczewska, K.; Collin, F.; Tarasiuk, J.; Chorąży, M.; Czarnowska, A.; Kwaśniewski, M.; Brola, W.; Bartosik-Psujek, H.; Adamczyk-Sowa, M.; Kochanowicz, J.; et al. Clinical and epidemiological characteristics of multiple sclerosis patients receiving disease-modifying treatment in Poland. Neurol. Neurochir. Pol. 2020, 54, 161–168. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CIS | RRMS | SPMS | PPMS | BNMS | HCs | p-Value | |
|---|---|---|---|---|---|---|---|
| No. of patients/eyes | 15/30 | 65/130 | 14/28 | 11/22 | 21/42 | 63/126 | |
| Sex (female/male) | 10/5 | 45/20 | 12/2 | 8/3 | 15/6 | 31/32 | 0.0614 |
| Mean age (range) [years] | 35.3 ± 11.0 (20–55) | 34.7 ± 8.8 (18–53) | 39.1 ± 10.5 (24–59) | 42.9 ± 10.7 (26–54) | 45.5 ± 8.7 (31–66) | 35.8 ± 12.8 (18–69) | 0.001 |
| Median disease duration(range) [years] | 1 (0.3–4) | 3 (0.5–23) | 9.5 (4–22) | 4 (1–27) | 16 (15–30) | <0.0001 | |
| Median EDSS score (range) | 0 (0–2) | 2.0 (0–5) | 4.3 (3–6.5) | 5.0 (3–7) | 2.0 (1–3) | <0.0001 | |
| ON/NON eyes (%ON) | 3/27 (10%) | 35/95 (26.93%) | 12/16 (42.86%) | 1/21 (4.55%) | 14/28 (33.33%) | 0.0146 | |
| Median time elapsed from ON(range) [months] | 12 (6–24) | 30 (12–90) | 110 (60–150) | 40 | 195 (180–240) | <0.0001 |
| Total Eyes | NON Eyes | ON Eyes | p-Value | ||||
|---|---|---|---|---|---|---|---|
| HCs vs. Total | HCs vs. NON | HCs vs. ON | NON vs. ON | ||||
| pRNFL (µm) | |||||||
| HCs | 116.5 ± 9.0 | ||||||
| CIS | 113.0 ± 15.6 | 115.0 ± 13.7 | 94.3 ± 22.8 | 0.3341 | 0.6868 | 0.0001 | 0.0905 |
| RRMS | 102.9 ± 15.9 | 106.6 ± 14.9 # | 92.8 ± 14.3 * | <0.0001 | <0.0001 | <0.0001 | 0.0001 |
| SPMS | 93.8 ± 21.7 | 98.7 ± 21.0 # | 87.3 ± 21.8 * | <0.0001 | 0.0094 | <0.0001 | 0.3135 |
| PPMS | 104.6 ± 16.8 | 105.2 ± 16.6 # | 99.0 * | 0.0193 | 0.0188 | <0.0001 | 0.0018 |
| BNMS | 91.0 ± 17.4 | 96.6 ± 16.7 # | 79.9 ± 13.3 * | <0.0001 | <0.0001 | <0.0001 | <0.0001 |
| TMV (mm3) | |||||||
| HCs | 2.580 ± 0.104 | ||||||
| CIS | 2.575 ± 0.147 | 2.586 ± 0.149 | 2.476 ± 0.105 | 0.8943 | 0.8813 | 0.0911 | 0.0617 |
| RRMS | 2.426 ± 0.179 | 2.453 ± 0.165 § | 2.352 ± 0.170 | <0.0001 | <0.0001 | <0.0001 | 0.0267 |
| SPMS | 2.289 ± 0.180 | 2.367 ± 0.163 § | 2.185 ± 0.149 | <0.0001 | 0.0001 | <0.0001 | 0.0090 |
| PPMS | 2.478 ± 0.154 | 2.490 ± 0.146 § | 2.207 | 0.0288 | 0.0396 | <0.0001 | <0.0001 |
| BNMS | 2.397 ± 0.159 | 2.437 ± 0.154 § | 2.317 ± 0.129 | <0.0001 | 0.0001 | <0.0001 | 0.0006 |
| pRNFL Thickness | TMV | |||
|---|---|---|---|---|
| Correlation Coefficient | p | Correlation Coefficient | p | |
| CIS duration | r = −0.01 | 0.9490 | r = −0.14 | 0.4570 |
| BNMS duration | r = −0.32 | 0.0104 | r = −0.43 | 0.0003 |
| RRMS duration | r = −0.10 | 0.1217 | r = −0.19 | 0.0290 |
| SPMS duration | r = −0.16 | 0.2661 | r = −0.19 | 0.2319 |
| PPMS duration | r = −0.55 | 0.0016 | r = −0.61 | 0.0002 |
| EDSS score | R = −0.22 | 0.0004 | R = −0.39 | <0.0001 |
| (a) ON eyes | R = −0.01 | 0.9364 | R = −0.48 | <0.0001 |
| (b) NON eyes | R = −0.29 | 0.0003 | R = −0.39 | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rzepiński, Ł.; Kucharczuk, J.; Maciejek, Z.; Grzybowski, A.; Parisi, V. Spectral-Domain Optical Coherence Tomography Assessment in Treatment-Naïve Patients with Clinically Isolated Syndrome and Different Multiple Sclerosis Types: Findings and Relationship with the Disability Status. J. Clin. Med. 2021, 10, 2892. https://doi.org/10.3390/jcm10132892
Rzepiński Ł, Kucharczuk J, Maciejek Z, Grzybowski A, Parisi V. Spectral-Domain Optical Coherence Tomography Assessment in Treatment-Naïve Patients with Clinically Isolated Syndrome and Different Multiple Sclerosis Types: Findings and Relationship with the Disability Status. Journal of Clinical Medicine. 2021; 10(13):2892. https://doi.org/10.3390/jcm10132892
Chicago/Turabian StyleRzepiński, Łukasz, Jan Kucharczuk, Zdzisław Maciejek, Andrzej Grzybowski, and Vincenzo Parisi. 2021. "Spectral-Domain Optical Coherence Tomography Assessment in Treatment-Naïve Patients with Clinically Isolated Syndrome and Different Multiple Sclerosis Types: Findings and Relationship with the Disability Status" Journal of Clinical Medicine 10, no. 13: 2892. https://doi.org/10.3390/jcm10132892
APA StyleRzepiński, Ł., Kucharczuk, J., Maciejek, Z., Grzybowski, A., & Parisi, V. (2021). Spectral-Domain Optical Coherence Tomography Assessment in Treatment-Naïve Patients with Clinically Isolated Syndrome and Different Multiple Sclerosis Types: Findings and Relationship with the Disability Status. Journal of Clinical Medicine, 10(13), 2892. https://doi.org/10.3390/jcm10132892