
Tracheostomy Timing and Outcome in Severe COVID-19: The WeanTrach Multicenter Study

 ,
,  ,
,  , , , , , , ,
, , , , , , ,  , , ,
, , ,  ,
,  , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patient Selection, Inclusion, and Exclusion Criteria
2.3. Data Collection
2.4. Definitions
- ○
- Early tracheostomy was defined as a tracheostomy performed within the first 15 days after endotracheal intubation, while late tracheostomy was defined as a tracheostomy performed ≥ 15 days after endotracheal intubation. The reason for selecting 15 days as the cut-off for early and late tracheostomy was based on the median time to tracheostomy performance in our cohort.
- ○
- Time to tracheostomy was defined as the time elapsed from endotracheal intubation to tracheostomy.
- ○
- Time to weaning was defined as the time from endotracheal intubation to the first spontaneous breathing trial (SBT).
- ○
- SBT was defined as the first attempt to reduce respiratory support before extubation (removal of endotracheal tube and respiratory support). The execution of a SBT did not automatically lead to extubation.
- ○
- Time to extubation was defined as the time between the insertion and the removal of an artificial airway such as an endotracheal tube or tracheostomy tube.
- ○
- Extubation was defined as the removal of an artificial airway. This term was used either for the removal of an endotracheal tube or tracheostomy tube.
- ○
- Time to ICU admission was defined as the time from hospital admission to ICU admission.
- ○
- Time to endotracheal intubation in ICU was defined as the time from ICU admission to endotracheal intubation.
- ○
- ICU discharge was defined as the last day of ICU stay, irrespective of death or discharge to another non-ICU ward.
- ○
- Length of ICU stay was defined as the time between ICU admission and ICU discharge, irrespective of death or discharge to another non-ICU ward.
- ○
- Post-tracheostomy ICU length of stay was considered as the time between tracheostomy and ICU discharge.
- ○
- Reasons for tracheostomy were categorized as follows: prolonged weaning expected, neurological impairment (inability to maintain patient airways because of neurological condition), extubation failure (failure of SBT and/or extubation needing re-intubation), and airway failure (inability to maintain patient airways because of upper airway causes).
2.5. Statistical Analysis
3. Results
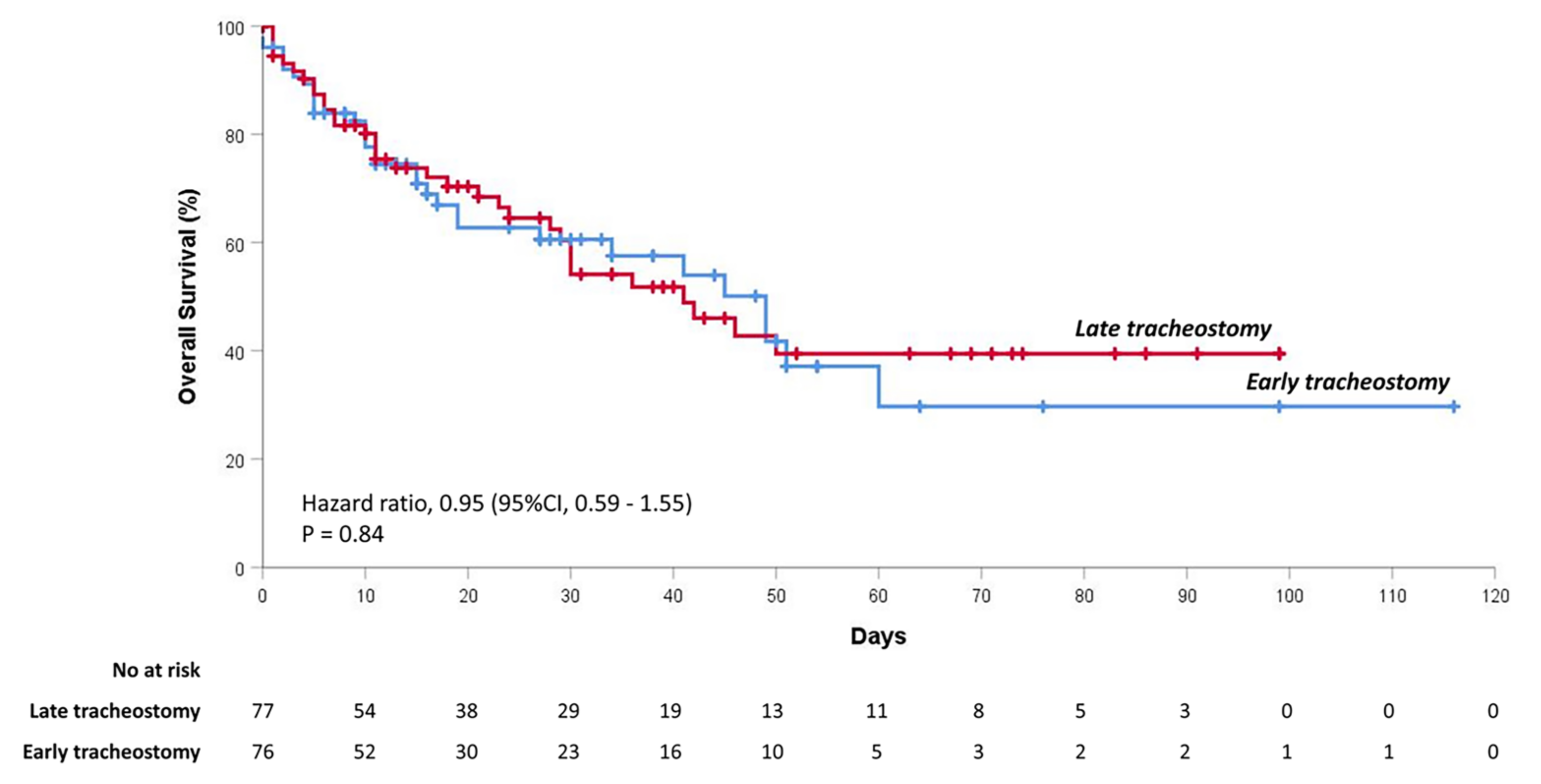
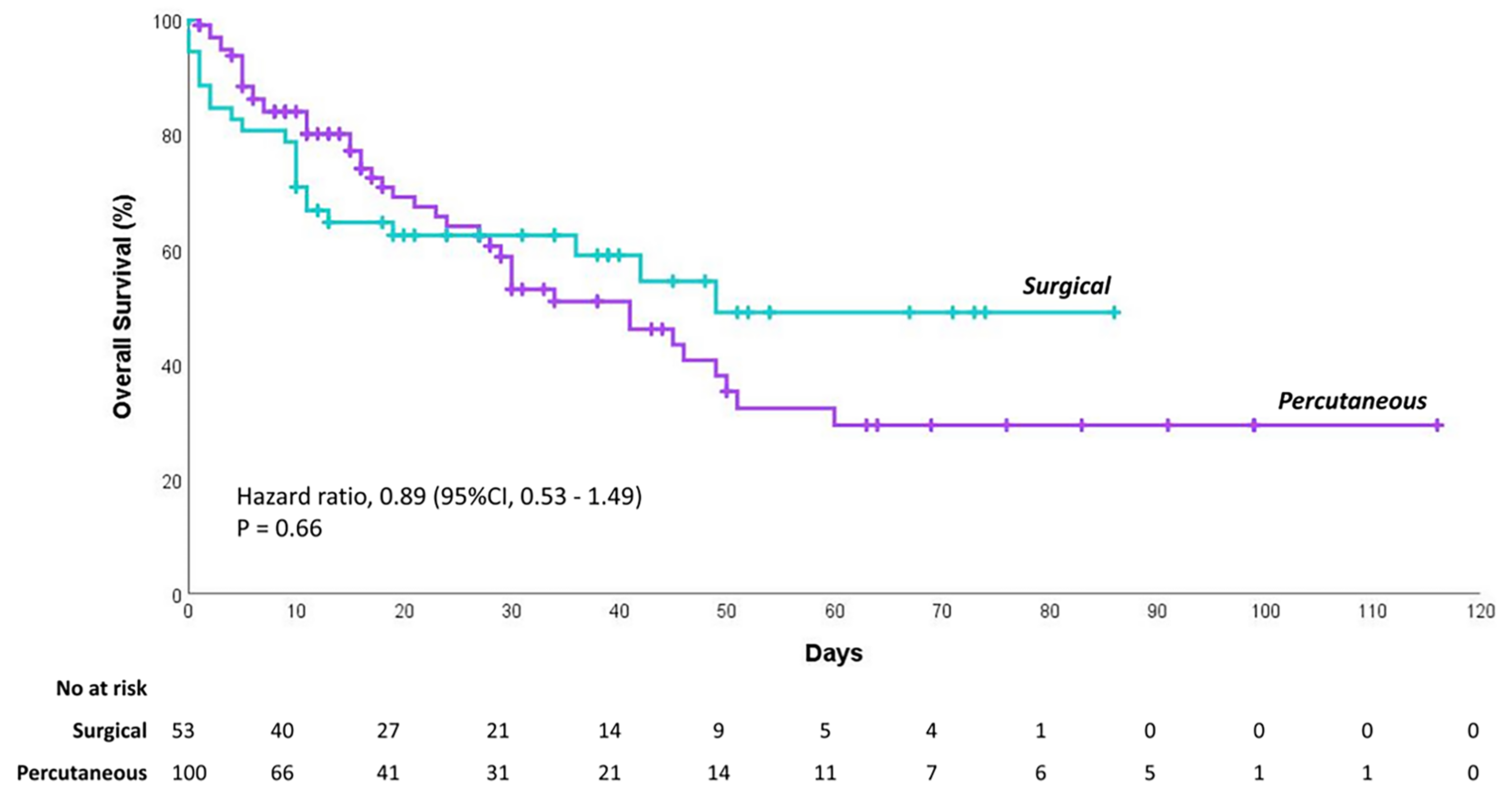
3.1. Cumulative Probability of Survival
3.2. ICU Length of Stay
3.3. Post-Tracheostomy Complications
4. Discussion
4.1. Timing and Type of Tracheostomy
4.2. Cumulative Probability of Survival
4.3. Length of ICU Stay
4.4. Post-Tracheostomy Complications
4.5. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kowalski, L.P.; Sanabria, A.; Ridge, J.A.; Ng, W.T.; Bree, R.; Rinaldo, A.; Takes, R.P.; Mäkitie, A.A.; Carvalho, A.L.; Bradford, C.R.; et al. COVID-19 pandemic: Effects and evidence-based recommendations for otolaryngology and head and neck surgery practice. Head Neck 2020, 42, 1259–1267. [Google Scholar] [CrossRef]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. Baseline Characteristics and Outcomes of 1591 Patients Infected With SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA 2020, 323, 1574. [Google Scholar] [CrossRef]
- Vena, A.; Giacobbe, D.R.; Di Biagio, A.; Mikulska, M.; Taramasso, L.; De Maria, A.; Ball, L.; Brunetti, I.; Loconte, M.; Patroniti, N.A.; et al. Clinical characteristics, management and in-hospital mortality of patients with coronavirus disease 2019 in Genoa, Italy. Clin. Microbiol. Infect. 2020, 26, 1537–1544. [Google Scholar] [CrossRef]
- McGrath, B.A.; Brenner, M.J.; Warrillow, S.J.; Pandian, V.; Arora, A.; Cameron, T.S.; Añon, J.M.; Hernández Martínez, G.; Truog, R.D.; Block, S.D.; et al. Tracheostomy in the COVID-19 era: Global and multidisciplinary guidance. Lancet Respir. Med. 2020, 8, 717–725. [Google Scholar] [CrossRef]
- Young, D.; Harrison, D.A.; Cuthbertson, B.H.; Rowan, K.; TracMan Collaborators. Effect of Early vs Late Tracheostomy Placement on Survival in Patients Receiving Mechanical Ventilation. JAMA 2013, 309, 2121. [Google Scholar] [CrossRef] [PubMed]
- Pan, L.; Guo, Y. Effect of Early Versus Late Tracheotomy in Critically Ill Patients: A Systematic Review and Meta-analysis. Chest 2016, 149, A165. [Google Scholar] [CrossRef]
- Catalino, M.P.; Lin, F.-C.; Davis, N.; Anderson, K.; Olm-Shipman, C.; Dedrick Jordan, J. Early versus late tracheostomy after decompressive craniectomy for stroke. J. Intensive Care 2018, 6, 1. [Google Scholar] [CrossRef] [PubMed]
- Aquino Esperanza, J.; Pelosi, P.; Blanch, L. What’s new in intensive care: Tracheostomy—What is known and what remains to be determined. Intensive Care Med. 2019, 45, 1619–1621. [Google Scholar] [CrossRef] [PubMed]
- Trouillet, J.-L.; Luyt, C.-E.; Guiguet, M.; Ouattara, A.; Vaissier, E.; Makri, R.; Nieszkowska, A.; Leprince, P.; Pavie, A.; Chastre, J.; et al. Early Percutaneous Tracheotomy Versus Prolonged Intubation of Mechanically Ventilated Patients After Cardiac Surgery. Ann. Intern. Med. 2011, 154, 373. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, J.; Barber, V.S.; Morgan, L.; Young, J.D. Systematic review and meta-analysis of studies of the timing of tracheostomy in adult patients undergoing artificial ventilation. BMJ 2005, 330, 1243. [Google Scholar] [CrossRef]
- Terragni, P.P.; Antonelli, M.; Fumagalli, R.; Faggiano, C.; Berardino, M.; Pallavicini, F.B.; Miletto, A.; Mangione, S.; Sinardi, A.U.; Pastorelli, M.; et al. Early vs. Late Tracheotomy for Prevention of Pneumonia in Mechanically Ventilated Adult ICU Patients. JAMA 2010, 303, 1483. [Google Scholar] [CrossRef]
- Blot, F.; Similowski, T.; Trouillet, J.-L.; Chardon, P.; Korach, J.-M.; Costa, M.-A.; Journois, D.; Thiéry, G.; Fartoukh, M.; Pipien, I.; et al. Early tracheotomy versus prolonged endotracheal intubation in unselected severely ill ICU patients. Intensive Care Med. 2008, 34, 1779–1787. [Google Scholar] [CrossRef]
- Freeman, B.D. Tracheostomy Update. Crit. Care Clin. 2017, 33, 311–322. [Google Scholar] [CrossRef]
- Silvester, W.; Goldsmith, D.; Uchino, S.; Bellomo, R.; Knight, S.; Seevanayagam, S.; Brazzale, D.; McMahon, M.; Buckmaster, J.; Hart, G.K.; et al. Percutaneous versus surgical tracheostomy: A randomized controlled study with long-term follow-up*. Crit. Care Med. 2006, 34, 2145–2152. [Google Scholar] [CrossRef]
- Givi, B.; Schiff, B.A.; Chinn, S.B.; Clayburgh, D.; Iyer, N.G.; Jalisi, S.; Moore, M.G.; Nathan, C.-A.; Orloff, L.A.; O’Neill, J.P.; et al. Safety Recommendations for Evaluation and Surgery of the Head and Neck During the COVID-19 Pandemic. JAMA Otolaryngol. Neck Surg. 2020, 146, 579. [Google Scholar] [CrossRef]
- Pandian, V.; Morris, L.L.; Brodsky, M.B.; Lynch, J.; Walsh, B.; Rushton, C.; Phillips, J.; Rahman, A.; DeRose, T.; Lambe, L.; et al. Critical Care Guidance for Tracheostomy Care During the COVID-19 Pandemic: A Global, Multidisciplinary Approach. Am. J. Crit. Care 2020, 29, e116–e127. [Google Scholar] [CrossRef]
- Putensen, C.; Theuerkauf, N.; Guenther, U.; Vargas, M.; Pelosi, P. Percutaneous and surgical tracheostomy in critically ill adult patients: A meta-analysis. Crit. Care 2014, 18, 544. [Google Scholar] [CrossRef]
- Rosano, A.; Martinelli, E.; Fusina, F.; Albani, F.; Caserta, R.; Morandi, A.; Dell’Agnolo, P.; Dicembrini, A.; Mansouri, L.; Marchini, A.; et al. Early Percutaneous Tracheostomy in Coronavirus Disease 2019: Association with Hospital Mortality and Factors Associated With Removal of Tracheostomy Tube at ICU Discharge. A Cohort Study on 121 Patients*. Crit. Care Med. 2021, 49, 261–270. [Google Scholar] [CrossRef] [PubMed]
- Rovira, A.; Tricklebank, S.; Surda, P.; Whebell, S.; Zhang, J.; Takhar, A.; Yeung, E.; Fan, K.; Ahmed, I.; Hopkins, P.; et al. Open versus percutaneous tracheostomy in COVID-19: A multicentre comparison and recommendation for future resource utilisation. Eur. Arch. Oto-Rhino-Laryngol. 2021, 9, 1–8. [Google Scholar] [CrossRef]
- Bellani, G.; Laffey, J.G.; Pham, T.; Fan, E.; Brochard, L.; Esteban, A.; Gattinoni, L.; van Haren, F.; Larsson, A.; McAuley, D.F.; et al. Epidemiology, Patterns of Care, and Mortality for Patients with Acute Respiratory Distress Syndrome in Intensive Care Units in 50 Countries. JAMA 2016, 315, 788. [Google Scholar] [CrossRef]
- Bier-Laning, C.; Cramer, J.D.; Roy, S.; Palmieri, P.A.; Amin, A.; Añon, J.M.; Bonilla-Asalde, C.A.; Bradley, P.J.; Chaturvedi, P.; Cognetti, D.M.; et al. Tracheostomy During the COVID-19 Pandemic: Comparison of International Perioperative Care Protocols and Practices in 26 Countries. Otolaryngol. Neck Surg. 2020, 019459982096198. [Google Scholar] [CrossRef]
- Kwak, P.E.; Connors, J.R.; Benedict, P.A.; Timen, M.R.; Wang, B.; Zhang, Y.; Youlios, S.; Sureau, K.; Persky, M.J.; Rafeq, S.; et al. Early Outcomes from Early Tracheostomy for Patients with COVID-19. JAMA Otolaryngol. Neck Surg. 2020. [Google Scholar] [CrossRef]
- Breik, O.; Nankivell, P.; Sharma, N.; Bangash, M.N.; Dawson, C.; Idle, M.; Isherwood, P.; Jennings, C.; Keene, D.; Manji, M.; et al. Safety and 30-day outcomes of tracheostomy for COVID-19: A prospective observational cohort study. Br. J. Anaesth. 2020, 125, 872–879. [Google Scholar] [CrossRef] [PubMed]
- Angel, L.; Kon, Z.N.; Chang, S.H.; Rafeq, S.; Palasamudram Shekar, S.; Mitzman, B.; Amoroso, N.; Goldenberg, R.; Sureau, K.; Smith, D.E.; et al. Novel Percutaneous Tracheostomy for Critically Ill Patients With COVID-19. Ann. Thorac. Surg. 2020, 110, 1006–1011. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.; Wu, Y.; Zhu, F.; Yang, X.; Huang, C.; Hou, G.; Xu, W.; Hu, M.; Zhang, L.; Cheng, A.; et al. Tracheostomy in 80 COVID-19 Patients: A Multicenter, Retrospective, Observational Study. Front. Med. 2020, 7. [Google Scholar] [CrossRef] [PubMed]
- Chao, T.N.; Harbison, S.P.; Braslow, B.M.; Hutchinson, C.T.; Rajasekaran, K.; Go, B.C.; Paul, E.A.; Lambe, L.D.; Kearney, J.J.; Chalian, A.A.; et al. Outcomes After Tracheostomy in COVID-19 Patients. Ann. Surg. 2020, 272, e181–e186. [Google Scholar] [CrossRef]
- Turri-Zanoni, M.; Battaglia, P.; Czaczkes, C.; Pelosi, P.; Castelnuovo, P.; Cabrini, L. Elective Tracheostomy During Mechanical Ventilation in Patients Affected by COVID-19: Preliminary Case Series From Lombardy, Italy. Otolaryngol. Neck Surg. 2020, 163, 135–137. [Google Scholar] [CrossRef]
- Mattioli, F.; Fermi, M.; Ghirelli, M.; Molteni, G.; Sgarbi, N.; Bertellini, E.; Girardis, M.; Presutti, L.; Marudi, A. Tracheostomy in the COVID-19 pandemic. Eur. Arch. Oto-Rhino-Laryngol. 2020, 277, 2133–2135. [Google Scholar] [CrossRef] [PubMed]
- Iftikhar, I.H.; Teng, S.; Schimmel, M.; Duran, C.; Sardi, A.; Islam, S. A Network Comparative Meta-analysis of Percutaneous Dilatational Tracheostomies Using Anatomic Landmarks, Bronchoscopic, and Ultrasound Guidance Versus Open Surgical Tracheostomy. Lung 2019, 197, 267–275. [Google Scholar] [CrossRef]
- Delaney, A.; Bagshaw, S.M.; Nalos, M. Percutaneous dilatational tracheostomy versus surgical tracheostomy in critically ill patients: A systematic review and meta-analysis. Crit Care 2006, 10, R55. [Google Scholar] [CrossRef]
- Mata-Castro, N.; Sanz-López, L.; Pinacho-Martínez, P.; Varillas-Delgado, D.; Miró-Murillo, M.; Martín-Delgado, M.C. Tracheostomy in patients with SARS-CoV-2 reduces time on mechanical ventilation but not intensive care unit stay. Am. J. Otolaryngol. 2021, 42, 102867. [Google Scholar] [CrossRef] [PubMed]
- Schultz, M.J.; Teng, M.S.; Brenner, M.J. Timing of Tracheostomy for Patients with COVID-19 in the ICU—Setting Precedent in Unprecedented Times. JAMA Otolaryngol. Neck Surg. 2020, 146, 887. [Google Scholar] [CrossRef] [PubMed]
- Hosokawa, K.; Nishimura, M.; Egi, M.; Vincent, J.-L. Timing of tracheotomy in ICU patients: A systematic review of randomized controlled trials. Crit. Care 2015, 19, 424. [Google Scholar] [CrossRef] [PubMed]
- Meng, L.; Wang, C.; Li, J.; Zhang, J. Early vs late tracheostomy in critically ill patients: A systematic review and meta-analysis. Clin. Respir. J. 2016, 10, 684–692. [Google Scholar] [CrossRef] [PubMed]
- Siempos, I.I.; Ntaidou, T.K.; Filippidis, F.T.; Choi, A.M.K. Effect of early versus late or no tracheostomy on mortality and pneumonia of critically ill patients receiving mechanical ventilation: A systematic review and meta-analysis. Lancet Respir. Med. 2015, 3, 150–158. [Google Scholar] [CrossRef]
- Massick, D.D.; Yao, S.; Powell, D.M.; Griesen, D.; Hobgood, T.; Allen, J.N.; Schuller, D.E. Bedside Tracheostomy in the Intensive Care Unit: A Prospective Randomized Trial Comparing Open Surgical Tracheostomy with Endoscopically Guided Percutaneous Dilational Tracheotomy. Laryngoscope 2001, 111, 494–500. [Google Scholar] [CrossRef]
- Antonelli, M.; Michetti, V.; Di Palma, A.; Conti, G.; Pennisi, M.A.; Arcangeli, A.; Montini, L.; Bocci, M.G.; Bello, G.; Almadori, G.; et al. Percutaneous translaryngeal versus surgical tracheostomy: A randomized trial with 1-yr double-blind follow-up*. Crit. Care Med. 2005, 33, 1015–1020. [Google Scholar] [CrossRef]
- Sole, M.L.; Talbert, S.; Penoyer, D.A.; Bennett, M.; Sokol, S.; Wilson, J. Comparison of Respiratory Infections before and after Percutaneous Tracheostomy. Am. J. Crit. Care 2014, 23, e80–e87. [Google Scholar] [CrossRef][Green Version]
- Robba, C.; Battaglini, D.; Ball, L.; Valbusa, A.; Porto, I.; Della Bona, R.; La Malfa, G.; Patroniti, N.; Brunetti, I.; Loconte, M.; et al. Coagulative Disorders in Critically Ill COVID-19 Patients with Acute Distress Respiratory Syndrome: A Critical Review. J. Clin. Med. 2021, 10, 140. [Google Scholar] [CrossRef]
- Lavinio, A.; Ercole, A.; Battaglini, D.; Magnoni, S.; Badenes, R.; Taccone, F.S.; Helbok, R.; Thomas, W.; Pelosi, P.; Robba, C. Safety profile of enhanced thromboprophylaxis strategies for critically ill COVID-19 patients during the first wave of the pandemic: Observational report from 28 European intensive care units. Crit. Care 2021, 25, 155. [Google Scholar] [CrossRef]
- Botti, C.; Lusetti, F.; Neri, T.; Peroni, S.; Castellucci, A.; Salsi, P.; Ghidini, A. Comparison of percutaneous dilatational tracheotomy versus open surgical technique in severe COVID-19: Complication rates, relative risks and benefits. Auris Nasus Larynx 2021, 48, 511–517. [Google Scholar] [CrossRef] [PubMed]
- Yeung, E.; Hopkins, P.; Auzinger, G.; Fan, K. Challenges of tracheostomy in COVID-19 patients in a tertiary centre in inner city London. Int. J. Oral Maxillofac. Surg. 2020, 49, 1385–1391. [Google Scholar] [CrossRef] [PubMed]
- Picetti, E.; Fornaciari, A.; Taccone, F.S.; Malchiodi, L.; Grossi, S.; Di Lella, F.; Falcioni, M.; D’Angelo, G.; Sani, E.; Rossi, S. Safety of bedside surgical tracheostomy during COVID-19 pandemic: A retrospective observational study. PLoS ONE 2020, 15, e0240014. [Google Scholar] [CrossRef] [PubMed]
- Robba, C.; Battaglini, D.; Pelosi, P.; Rocco, R.M.P. Multiple organ dysfunction in SARS-CoV-2: MODS-CoV-2. Expert Rev. Respir. Med. 2020, 14, 865–868. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Baseline Characteristics | Overall | Time to Tracheostomy | Type of Tracheostomy | ||||
|---|---|---|---|---|---|---|---|
| n = 153 | Early n = 76 | Late n = 77 | p-Value | Percutaneous n = 100 | Surgical n = 53 | p-Value | |
| Age, years | 63.4 ± 9.34 64.0 (32.0–89.0) | 63.8 ± 9.24 65.0 (34.0–89.0) | 62.9 ± 9.48 63.0 (32.0–88.0) | 0.36 | 63.9 ± 9.18 64.0 (34.0–88.0) | 62.3 ± 9.64 62.0 (32.0–89.0) | 0.29 |
| Sex, males | 118 (77.1) | 60 (78.9) | 58 (75.3) | 0.59 | 81 (81.0) | 37 (69.8) | 0.12 |
| BMI, kg/m2 | 28.8 ± 5.04 27.8 (16.5–50.8) | 29.0 ± 5.19 27.8 16.5 50.8 | 28.6 ± 4.91 27.8 (19.5–46.4) | 0.62 | 28.7 ± 4.51 27.8 (20.7–46.4) | 29.0 ± 5.96 27.8 (16.5–50.8) | 0.96 |
| Comorbidities | |||||||
| Hypertension | 82 (53.6) | 42 (55.3) | 40 (51.9) | 0.68 | 57 (57.0) | 25 (47.2) | 0.25 |
| Diabetes mellitus | 34 (22.2) | 20 (26.3)) | 14 (18.2) | 0.23 | 22 (22.0) | 12 (22.6) | 0.93 |
| Chronic respiratory disease | 16 (10.5) | 11 (14.7) | 5 (6.5) | 0.10 | 13 (13.1) | 3 (5.7) | 0.15 |
| Chronic cardiac disease | 23 (15.0) | 12 (15.8) | 11 (14.3) | 0.80 | 13 (13.0) | 10 (18.9) | 0.33 |
| Malignancy | 12 (7.8) | 5 (6.6) | 7 (9.1) | 0.56 | 6 (6.0) | 6 (11.3) | 0.24 |
| Chronic liver disease | 6 (3.9) | 3 (3.9) | 3 (3.9) | 0.99 | 6 (6.0) | 0 (0.0) | 0.07 |
| Chronic neurologic disease | 13 (8.5) | 9 (11.8) | 4 (5.2) | 0.14 | 12 (12.0) | 1 (1.9) | 0.033 |
| Chronic kidney disease | 9 (5.9) | 5 (6.6) | 4 (5.2) | 0.72 | 6 (6.0) | 3 (5.7) | 0.93 |
| Smoke | 10 (7.8) | 5 (8.5) | 5 (7.1) | 0.78 | 8 (8.3) | 2 (6.1) | 0.67 |
| Symptoms’ onset to hospital admission, days | 6.3 ± 5.61 5.0 (0.0–36.0) | 6.0 ± 4.85 5.0 (0.0–33.0) | 6.6 ± 6.40 5.0 (0.0–36.0) | 0.96 | 6.9 ± 6.26 6.0 (0.0–36.0) | 5.2 ± 4.02 4.0 (0.0–19.0) | 0.10 |
| Hospital admission to COVID-19 swab, days | 1.5 ± 5.02 0.0 (0.0–31.0) | 1.5 ± 5.74 0.0 (0.0–31.0) | 1.5 ± 4.22 0.0 (0.0–31.0) | 0.03 | 0.8 ± 3.04 0.0 (0.0–26.0) | 3.0 ± 7.56 0.0 (0.0–31.0) | 0.05 |
| Hospital to ICU admission, days | 6.0 ± 9.12 3.0 (0.0–61.0) | 5.8 ± 9.54 3.0 (0.0–61.0) | 6.3 ± 8.75 4.0 (0.0–39.0) | 0.43 | 5.4 ± 7.47 3.0 (0.0–39.0) | 7.3 ± 11.60 3.0 (0.0–61.0) | 0.47 |
| Complications of Tracheostomy | Overall Population | Time to Tracheostomy | Type of Tracheostomy | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Early | Late | Univariate Analysis p-Value OR (95% CI) | Multivariate Analysis p-Value OR (95% CI) | Percutaneous | Surgical | Univariate Analysis p-Value OR (95% CI) | Multivariate Analysis p-Value OR (95% CI) | ||
| Hemorrhage | |||||||||
| No | 128 (90.8) | 68 (95.8) | 60 (85.7) | 0.05 | 0.09 | 83 (87.4) | 45 (97.8) | 0.06 | |
| Yes | 13 (9.2) | 3 (4.2) | 10 (14.3) | 3.78 (0.99–14.37) | 7.98 (0.72–89.11) | 12 (12.6) | 1 (2.2) | 0.15 (0.02–1.22) | |
| Coagulation | |||||||||
| No | 138 (97.9) | 69 (97.2) | 69 (98.6) | 0.99 | 92 (96.8) | 46 (100.0) | 0.55 | ||
| Yes | 3 (2.1) | 2 (2.8) | 1 (1.4) | 3 (3.2) | 0 (0.0) | ||||
| Tracheal stenosis | |||||||||
| No | 139 (100.0) | 71 (100.0) | 68 (100.0) | / | 93 (100.0) | 46 (100.0) | / | ||
| Yes | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | ||||
| Infection of stoma | |||||||||
| No | 128 (90.8) | 64 (90.1) | 64 (91.4) | 0.79 | 84 (87.5) | 44 (97.8) | 0.06 | ||
| Yes | 13 (9.2) | 7 (9.9) | 6 (8.6) | 12 (12.5) | 1 (2.2) | 0.16 (0.02–1.26) | |||
| Pneumothorax | |||||||||
| No | 137 (100.0) | 66 (95.7) | 66 (94.3) | 0.71 | 86 (92.5) | 46 (100.0) | 0.10 | ||
| Yes | 7 (5.0) | 3 (4.3) | 4 (5.7) | 7 (7.5) | 0 (0.0) | ||||
| LRTI * | |||||||||
| Negative | 30 (34.5) | 7 (22.6) | 23 (41.1) | 0.09 | 0.07 | 24 (46.2) | 6 (17.1) | 0.06 | 0.007 |
| Positive | 57 (65.5) | 24 (77.4) | 33 (58.9) | 0.42 (0.16–1.13) | 0.27 (0.07–1.11) | 28 (53.8) | 29 (82.9) | 4.14 (1.47–11.66) | 10.06 (1.89–53.54) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Battaglini, D.; Missale, F.; Schiavetti, I.; Filauro, M.; Iannuzzi, F.; Ascoli, A.; Bertazzoli, A.; Pascucci, F.; Grasso, S.; Murgolo, F.; et al. Tracheostomy Timing and Outcome in Severe COVID-19: The WeanTrach Multicenter Study. J. Clin. Med. 2021, 10, 2651. https://doi.org/10.3390/jcm10122651
Battaglini D, Missale F, Schiavetti I, Filauro M, Iannuzzi F, Ascoli A, Bertazzoli A, Pascucci F, Grasso S, Murgolo F, et al. Tracheostomy Timing and Outcome in Severe COVID-19: The WeanTrach Multicenter Study. Journal of Clinical Medicine. 2021; 10(12):2651. https://doi.org/10.3390/jcm10122651
Chicago/Turabian StyleBattaglini, Denise, Francesco Missale, Irene Schiavetti, Marta Filauro, Francesca Iannuzzi, Alessandro Ascoli, Alberto Bertazzoli, Federico Pascucci, Salvatore Grasso, Francesco Murgolo, and et al. 2021. "Tracheostomy Timing and Outcome in Severe COVID-19: The WeanTrach Multicenter Study" Journal of Clinical Medicine 10, no. 12: 2651. https://doi.org/10.3390/jcm10122651
APA StyleBattaglini, D., Missale, F., Schiavetti, I., Filauro, M., Iannuzzi, F., Ascoli, A., Bertazzoli, A., Pascucci, F., Grasso, S., Murgolo, F., Binda, S., Maraggia, D., Montrucchio, G., Sales, G., Pascarella, G., Agrò, F. E., Faccio, G., Ferraris, S., Spadaro, S., ... Pelosi, P. (2021). Tracheostomy Timing and Outcome in Severe COVID-19: The WeanTrach Multicenter Study. Journal of Clinical Medicine, 10(12), 2651. https://doi.org/10.3390/jcm10122651