
Incidence and Risk Factors for Acute Kidney Injury during the Treatment of Methicillin-Sensitive Staphylococcus aureus Infections with Cloxacillin Based Antibiotic Regimens: A French Retrospective Study

 ,
,
Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Study Setting
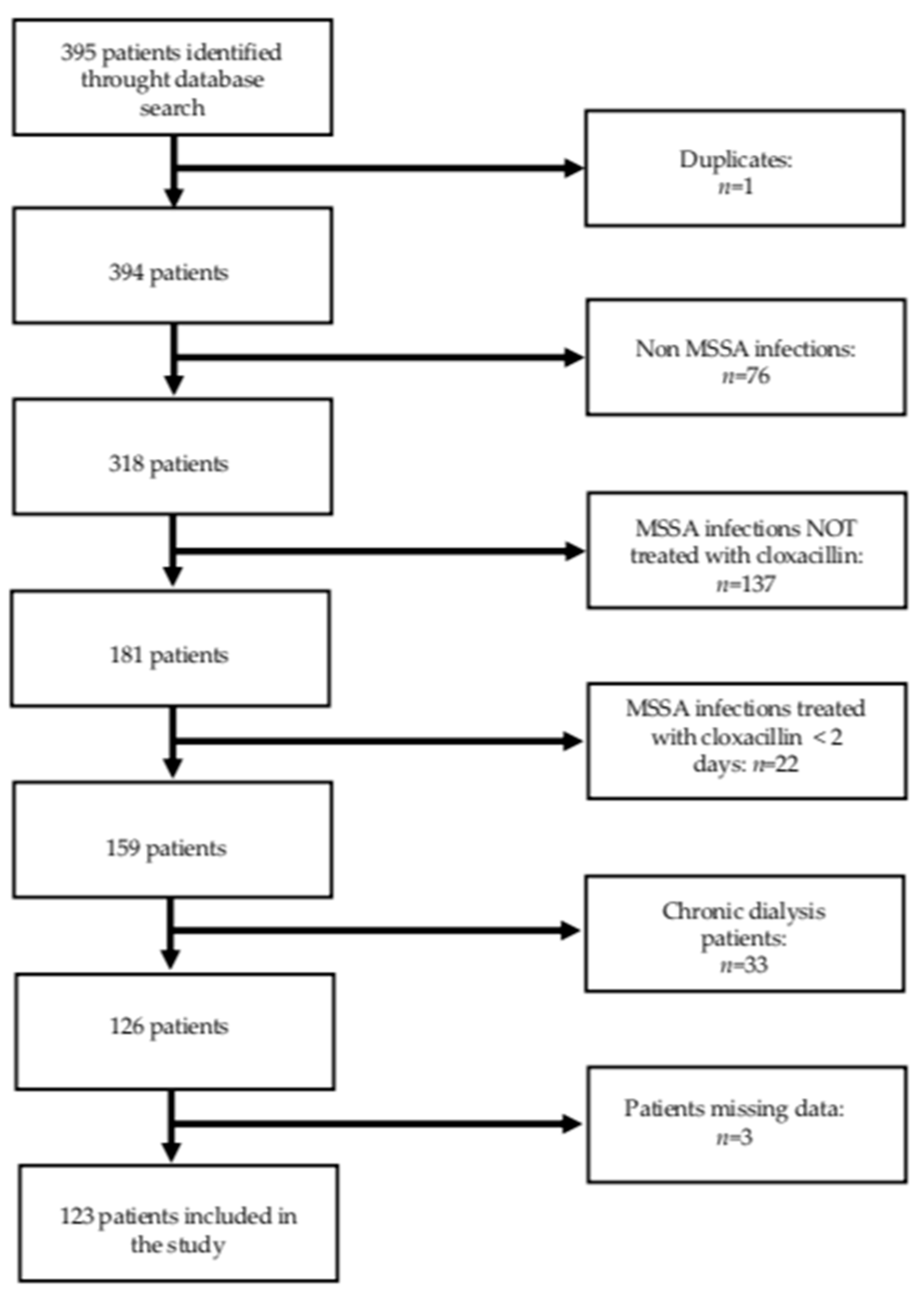
2.3. Participants and Data
2.4. Study Endpoints and Definitions
- -
- Age.
- -
- Body Mass Index (BMI).
- -
- Chronic Kidney Disease (CKD). CKD was defined by an eGFR < 60 mL/min/1.73 m2 [19] at baseline according to the MDRD equation (without race adjustment, since race was not recorded in medical charts).
- -
- Comorbidities (diabetes, hypertension, Charlson comorbidity index).
- -
- Smoking.
- -
- High alcohol consumption. It was defined as any alcohol use described as excessive or pathological in clinical charts.
- -
- Serum albumin (g/L).
- -
- Hypotension during hospitalization: defined by at least one episode of acute hypotension (mean arterial pressure of <65 mmHg or a systolic arterial pressure of <100 mmHg) recorded in the patient’s medical file.
- -
- Nephrotoxic drugs: Proton Pump Inhibitors (PPI), Nonsteroidal Anti-Inflammatory Drugs (NSAID), Renin Angiotensin Aldosteron System (RAAS) inhibitors, loop diuretics, non-loop diuretics, statins.
- -
- Other antibiotics.
- -
- Iodinated contrast media.
- -
- Type of Infection (endocarditis vs. other infections: bacteremia, catheter blood stream infection, bones infection, and urinary tract infection).
- -
- Regarding cloxacillin use:
- Dose (g per day).
- Mode of administration (IV, versus oral).
- Infusion type (continuous versus intermittent).
- Treatment duration.
2.5. Statistical Analysis
2.6. Ethical Issues
3. Results
3.1. Baseline Data and Data at Diagnosis of AKI
3.2. Clinical Data at AKI Presentation
3.3. Risk Factors for AKI
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Habib, G.; Lancellotti, P.; Antunes, M.J.; Bongiorni, M.G.; Casalta, J.-P.; Del Zotti, F.; Dulgheru, R.; El Khoury, G.; Erba, P.A.; Iung, B.; et al. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur. Heart J. 2015, 36, 3075–3128. [Google Scholar] [PubMed]
- Prothèse de Hanche ou de Genou: Diagnostic et Prise en Charge de L’infection Dans Le Mois Suivant L’implantation. Haute Autorité de Santé. Available online: https://www.has-sante.fr/jcms/c_1228574/fr/prothese-de-hanche-ou-de-genou-diagnostic-et-prise-en-charge-de-l-infection-dans-le-mois-suivant-l-implantation (accessed on 25 September 2020).
- Réévaluation des Pénicillines du Groupe M: Oxacilline et Cloxacilline—Lettre Aux Professionnels de Santé—ANSM: Agence nationale de Sécurité du Médicament et Des Produits de Santé. Available online: https://www.ansm.sante.fr/S-informer/Informations-de-securite-Lettres-aux-professionnels-de-sante/Reevaluation-des-penicillines-du-groupe-M-oxacilline-et-cloxacilline-Lettre-aux-professionnels-de-sante (accessed on 21 October 2018).
- Longuet, P.; LeCapitaine, A.; Cassard, B.; Batista, R.; Gauzit, R.; Lesprit, P.; Haddad, R.; Vanjak, D.; Diamantis, S.; Bastita, R. Preparing and administering injectable antibiotics: How to avoid playing God. Med. Mal. Infect. 2016, 46, 242–268. [Google Scholar] [CrossRef]
- Verdier, M.C.; Tribut, O.; Tattevin, P.; Michelet, C.; Bentué-Ferrer, D. Assessment of interindividual variability of plasma concentrations after administrazion of high doses of intravenous amoxicillin or cloxacillin in critically ill patients. J. Chemother. 2011, 23, 277–281. [Google Scholar] [CrossRef]
- Neuville, M.; El-Helali, N.; Magalhaes, E.; Radjou, A.; Smonig, R.; Soubirou, J.-F.; Voiriot, G.; Le Monnier, A.; Ruckly, S.; Bouadma, L.; et al. Systematic overdosing of oxa- and cloxacillin in severe infections treated in ICU: Risk factors and side effects. Ann. Intensive Care 2017, 7, 1–9. [Google Scholar] [CrossRef]
- Johansson, S.; Christensen, O.M.; Thorsmark, A.H. A retrospective study of acute kidney injury in hip arthroplasty patients receiving gentamicin and dicloxacillin. Acta Orthop. 2016, 87, 589–591. [Google Scholar] [CrossRef]
- Xu, B.; Murray, M. Flucloxacillin induced acute renal failure. Aust. Fam. Physician 2008, 37, 1009–1011. [Google Scholar]
- Isacson, J.; Collert, S. Renal impairment after high doses of dicloxacillin-prophylaxis in joint replacement surgery. Acta Orthop. Scand. 1984, 55, 407–410. [Google Scholar] [CrossRef]
- Lavergne, A.; Vigneau, C.; Polard, E.; Triquet, L.; Rioux-Leclercq, N.; Tattevin, P.; Golbin, L. Acute kidney injury during treatment with high-dose cloxacillin: A report of 23 cases and literature review. Int. J. Antimicrob. Agents 2018, 52, 344–349. [Google Scholar] [CrossRef]
- Hammond, D.A.; Smith, M.N.; Li, C.; Hayes, S.M.; Lusardi, K.; Bookstaver, P.B. Systematic Review and Meta-Analysis of Acute Kidney Injury Associated with Concomitant Vancomycin and Piperacillin/tazobactam. Clin. Infect. Dis. 2016, 64, 666–674. [Google Scholar] [CrossRef] [PubMed]
- Challagundla, S.R.; Knox, D.; Hawkins, A.; Hamilton, D.; Wv Flynn, R.; Robertson, S.; Isles, C. Renal impairment after high-dose flucloxacillin and single-dose gentamicin prophylaxis in patients undergoing elective hip and knee replacement. Nephrol. Dial. Transplant. 2013, 28, 612–619. [Google Scholar] [CrossRef] [PubMed]
- Spanou, Z.; Keller, M.; Britschgi, M.; Yawalkar, N.; Fehr, T.; Neuweiler, J.; Gugger, M.; Mohaupt, M.; Pichler, W.J. Involvement of Drug-Specific T Cells in Acute Drug-Induced Interstitial Nephritis. J. Am. Soc. Nephrol. 2006, 17, 2919–2927. [Google Scholar] [CrossRef]
- Bakker, S.J.L.; Luik, A.J.; Leunissen, K.M.L. Flucloxacillin-induced acute interstitial nephritis. Nephrol. Dial. Transplant. 1995, 10, 579. [Google Scholar] [CrossRef] [PubMed]
- García-Ortiz, R.; Espinoza, R.S.; Silva, G.R.; Alonso, R.K.; Opazo, H.S.; Houghton, D.C. Cloxacillin-Induced Acute Tubulo Interstitial Nephritis. Ann. Pharmacother. 1992, 26, 1241–1242. [Google Scholar] [CrossRef] [PubMed]
- Grimm, P.C.; Ogborn, M.R.; Larson, A.J.; Crocker, J.F. Interstitial Nephritis Induced by Cloxacillin. Nephron 1989, 51, 285–286. [Google Scholar] [CrossRef]
- Khalili, H.; Bairami, S.; Kargar, M. Antibiotics induced acute kidney injury: Incidence, risk factors, onset time and outcome. Acta Med. Iran. 2013, 51, 871–878. [Google Scholar] [PubMed]
- Bellomo, R.; Ronco, C.; Kellum, J.A.; Mehta, R.L.; Palevsky, P. Acute renal failure—Definition, outcome measures, animal models, fluid therapy and information technology needs: The Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit. Care 2004, 8, R204–R212. [Google Scholar] [CrossRef] [PubMed]
- Kidney Disease: Improving GlobalOutcomes (KDIGO) CKD Work Group. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int. Suppl. 2013, 3, 1–150. [Google Scholar]
- Tune, B.M. Nephrotoxicity of beta-lactam antibiotics: Mechanisms and strategies for prevention. Pediatr. Nephrol. 1997, 11, 768–772. [Google Scholar] [CrossRef] [PubMed]
- Bagshaw, S.M.; George, C.; Bellomo, R. The ANZICS Database Management Committe Early acute kidney injury and sepsis: A multicentre evaluation. Crit. Care 2008, 12, R47. [Google Scholar] [CrossRef]
- Duval, X.; Delahaye, F.; Alla, F.; Tattevin, P.; Obadia, J.F.; Le Moing, V.; Doco-Lecompte, T.; Celard, M.; Poyart, C.; Strady, C.; et al. Temporal trends in infective endocarditis in the context of prophylaxis guideline modifications: Three successive population-based surveys. J. Am. Coll. Cardiol. 2012, 59, 1968–1976. [Google Scholar] [CrossRef]
- Scott, J.; Jones, T.; Redaniel, M.T.; May, M.T.; Ben-Shlomo, Y.; Caskey, F. Estimating the risk of acute kidney injury associated with use of diuretics and renin angiotensin aldosterone system inhibitors: A population based cohort study using the clinical practice research datalink. BMC Nephrol. 2019, 20, 481. [Google Scholar] [CrossRef] [PubMed]
- Peerapornratana, S.; Manrique-Caballero, C.L.; Gómez, H.; Kellum, J.A. Acute kidney injury from sepsis: Current concepts, epidemiology, pathophysiology, prevention and treatment. Kidney Int. 2019, 96, 1083–1099. [Google Scholar] [CrossRef] [PubMed]
- Hsu, W.T.; Galm, B.P.; Schrank, G.; Hsu, T.C.; Lee, S.H.; Park, J.Y.; Lee, C.C. Effect of Renin-Angiotensin-Aldosterone System Inhibitors on Short-Term Mortality After Sepsis: A Population-Based Cohort Study. Hypertension 2020, 75, 483–491. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.-Y.; Moon, A.-R. Drug-Induced Nephrotoxicity and Its Biomarkers. Biomol. Ther. 2012, 20, 268–272. [Google Scholar] [CrossRef]


{kind=link}
| Total = 123 | AKI Group = 42 | Non-AKI Group = 81 | p | |
|---|---|---|---|---|
| Gender n (%) | 0.224 | |||
| Male | 85 (69.1) | 26 (61.9) | 59 (72.8) | |
| Age n (%) | 0.002 | |||
| ≤75 years | 62 (50.4) | 13 (31) | 49 (60.5) | |
| >75 years | 61 (49.6) | 29 (69) | 32 (39.5) | |
| Median age (IQR) (min-max) * | 75 (61–84) (36–101) | 81 (69–88) (51–96) | 70 (60–82) (36–101) | 0.0007 |
| Mean BMI (std) ** | 26.5 (5.9) | 26.5 (6.4) | 26.1 (5.5) | 0.2202 |
| CKD n (%) | 47 (38.2) | 20 (47.6) | 27 (33.3) | 0.122 |
| Diabetes n (%) | 37 (30.1) | 12 (38.6) | 25 (30.9) | 0.838 |
| Medical history of hypertension n (%) | 79 (64.2) | 31 (73.8) | 48 (58.3) | 0.119 |
| Median Charlson score (IQR) | 6 (4–8) | 6 (5–8) | 5 (4–7) | 0.1228 |
| Smokers n (%) | 16 (13) | 3 (7.1) | 13 (16.1) | 0.258 |
| High alcohol consumption n (%) | 19 (15.5) | 4 (9.5) | 15 (18.5) | 0.293 |
| Mean serum albumin (g/l) (std) *** | 23.7 (6.7) | 22.7 (6.3) | 24.2 (7) | 0.3669 |
| PPI n (%) | 53 (43.1) | 22 (52.4) | 31 (38.3) | 0.179 |
| NSAID n (%) | 9 (7.3) | 3 (7.1) | 6 (7.4) | 1.000 |
| RAAS inhibitors n (%) | 45 (36.6) | 20 (47.6) | 25 (30.9) | 0.078 |
| Loop diuretics n (%) | 45 (36.6) | 22 (52.4) | 23 (28.4) | 0.011 |
| Non-loop diuretics n (%) | 30 (24.4) | 15 (35.7) | 15 (18.5) | 0.046 |
| Statins n (%) | 38 (30.9) | 13 (30.9) | 25 (30.9) | 1.000 |
| Vancomycin n (%) | 26 (21.1) | 13 (30.9) | 13 (16.1) | 0.065 |
| Aminoglycosides n (%) | 69 (56.1) | 28 (66.7) | 41 (50.6) | 0.125 |
| Other penicillins n (%) | 45 (36.6) | 15 (35.7) | 30 (37) | 1.000 |
| Iodinated contrast media injection (%) | 37 (30.1) | 15 (33.3) | 23 (28.4) | 0.679 |
| Hypotension | 16 (13) | 9 (21.4) | 7 (8.6) | 0.054 |
| Infection n (%) | 0.001 | |||
| Endocarditis | 30 (24.4) | 18 (42.9) | 12 (14.8) | |
| Other infections | 93 (75.6) | 24 (57.1) | 69 (85.2) | |
| Bacteremia | 47 (38.2) | 13 (30.9) | 34 (42) | |
| Bones infection | 31 (25.2) | 9 (21.4) | 22 (27.2) | |
| Catheter blood stream infection | 11 (8.94) | 1 (2.4) | 10 (12.3) | |
| Urinary tract infection | 4 (3.3) | 1 (2.4) | 3 (3.7) | |
| Median dose g per day (min-max) * | 10 (3–16) | 12 (3–16) | 10 (3–12) | 0.4168 |
| Method of administration n (%) | 0.550 | |||
| IV | 120 (97.6) | 42 (100) | 78 (96.3) | |
| Oral | 3 (2.4) | 0 | 3 (3.7) | |
| Infusion type n (%) | 0.329 | |||
| Continuous | 11 (8.9) | 2 (4.8) | 9 (11.1) | |
| Intermittent | 112 (91.1) | 40 (95.2) | 72 (88.9) | |
| Median days of treatment (IQR) (min-max) * | 9 (5–14) (2–45) | 7 (3–13) (2–45) | 10 (6–15) (2–45) | 0.0675 |
| Median days of hospital stay (IQR) (min-max) * | 21 (5–35) (3–80) | 27 (18.2) (3–80) | 19 (15.7) (4–75) | 0.0025 |
| In-hospital death n (%) | 24 (19.5) | 12 (28.6) | 12 (14.8) | 0.093 |
| AKI Group n = 42 | |
|---|---|
| Median creatinine at baseline μmol/L (IQR) (min–max) | 93.5 (73–112) (45–183) |
| Median peak creatinine μmol/L (IQR) (min–max) | 221 (150–332) (95–1006) |
| Dialysis n (%) | 6 (14.3%) |
| Encephalopathy n (%) | 4 (9.5%) |
| Skin reaction n (%) | 4 (9.5%) |
| Hepatitis n (%) | 13 (32.5%) |
| Eosinophilia n (%) | 4 (9.5%) |
| Median proteinuria g/L (IQR) (min–max) * | 0.52 (0.2–0.8) (0–4.34) |
| Median PCR g/g (IQR) (min–max) ** | 0.64 (0.38–2) (0–5.31) |
| Hematuria n (%) *** | 9 (27.3%) |
| Leukocyturia n (%) **** | 18 (56.3%) |
| Median creatinine at hospital discharge (IQR) (min–max) | 140 (104–210) (49–429) |
| Median creatinine at M3 (IQR) (min–max) ***** | 102 (74–163) (62–230) |
| Factors Studied | Crude OR | (95% CI) * | p |
|---|---|---|---|
| Age | 0.0017 | ||
| ≤75 | ref. | ||
| >75 | 3.42 | (1.55–7.54) | |
| CKD | 0.124 | ||
| No | ref | ||
| Yes | 1.82 | (0.85–3.89) | |
| RAAS inhibitors | 0.0691 | ||
| No | ref. | ||
| Yes | 2.04 | (0.95–4.39) | |
| Loop diuretics | 0.0093 | ||
| No | ref. | ||
| Yes | 2.77 | (1.28–6.02) | |
| Non-loop diuretics | 0.0383 | ||
| No | ref. | ||
| Yes | 2.44 | (1.05–5.69) | |
| Vancomycin | 0.0595 | ||
| No | ref. | ||
| Yes | 2.34 | (0.97–5.67) | |
| Aminoglycosides | 0.0866 | ||
| No | ref. | ||
| Yes | 1.95 | (0.90–4.24) | |
| Infection | 0.0008 | ||
| Other infections | ref. | ||
| Endocarditis | 4.31 | (1.81–10.25) | |
| Hypotension | 0.0516 | ||
| No | ref. | ||
| Yes | 2.88 | (0.99–8.40) |
| Factors Studied | Adjusted OR | (95% CI) * | p |
|---|---|---|---|
| Age | 0.002 | ||
| ≤75 | ref. | ||
| >75 | 4.38 | (1.73–11.07) | |
| CKD | 0.693 | ||
| No | ref. | ||
| Yes | 0.82 | (0.30–2.22) | |
| RAAS inhibitors | NS | ||
| Loop diuretics | 0.036 | ||
| No | ref. | ||
| Yes | 2.94 | (1.07–8.04) | |
| Non-loop diuretics | 0.027 | ||
| No | ref. | ||
| Yes | 3.05 | (1.13–8.19) | |
| Vancomycin | NS | ||
| Aminoglycosides | NS | ||
| Infection | 0.012 | ||
| Other infections | ref. | ||
| Endocarditis | 3.42 | (1.31–8.94) | |
| Hypotension | NS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Crochette, R.; Ravaiau, C.; Perez, L.; Coindre, J.-P.; Piccoli, G.B.; Blanchi, S. Incidence and Risk Factors for Acute Kidney Injury during the Treatment of Methicillin-Sensitive Staphylococcus aureus Infections with Cloxacillin Based Antibiotic Regimens: A French Retrospective Study. J. Clin. Med. 2021, 10, 2603. https://doi.org/10.3390/jcm10122603
Crochette R, Ravaiau C, Perez L, Coindre J-P, Piccoli GB, Blanchi S. Incidence and Risk Factors for Acute Kidney Injury during the Treatment of Methicillin-Sensitive Staphylococcus aureus Infections with Cloxacillin Based Antibiotic Regimens: A French Retrospective Study. Journal of Clinical Medicine. 2021; 10(12):2603. https://doi.org/10.3390/jcm10122603
Chicago/Turabian StyleCrochette, Romain, Camille Ravaiau, Lucia Perez, Jean-Philippe Coindre, Giorgina Barbara Piccoli, and Sophie Blanchi. 2021. "Incidence and Risk Factors for Acute Kidney Injury during the Treatment of Methicillin-Sensitive Staphylococcus aureus Infections with Cloxacillin Based Antibiotic Regimens: A French Retrospective Study" Journal of Clinical Medicine 10, no. 12: 2603. https://doi.org/10.3390/jcm10122603
APA StyleCrochette, R., Ravaiau, C., Perez, L., Coindre, J.-P., Piccoli, G. B., & Blanchi, S. (2021). Incidence and Risk Factors for Acute Kidney Injury during the Treatment of Methicillin-Sensitive Staphylococcus aureus Infections with Cloxacillin Based Antibiotic Regimens: A French Retrospective Study. Journal of Clinical Medicine, 10(12), 2603. https://doi.org/10.3390/jcm10122603