
Treatment Outcomes of Patients with Glomus Tympanicum Tumors Presenting with Pulsatile Tinnitus

 ,
, 

Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
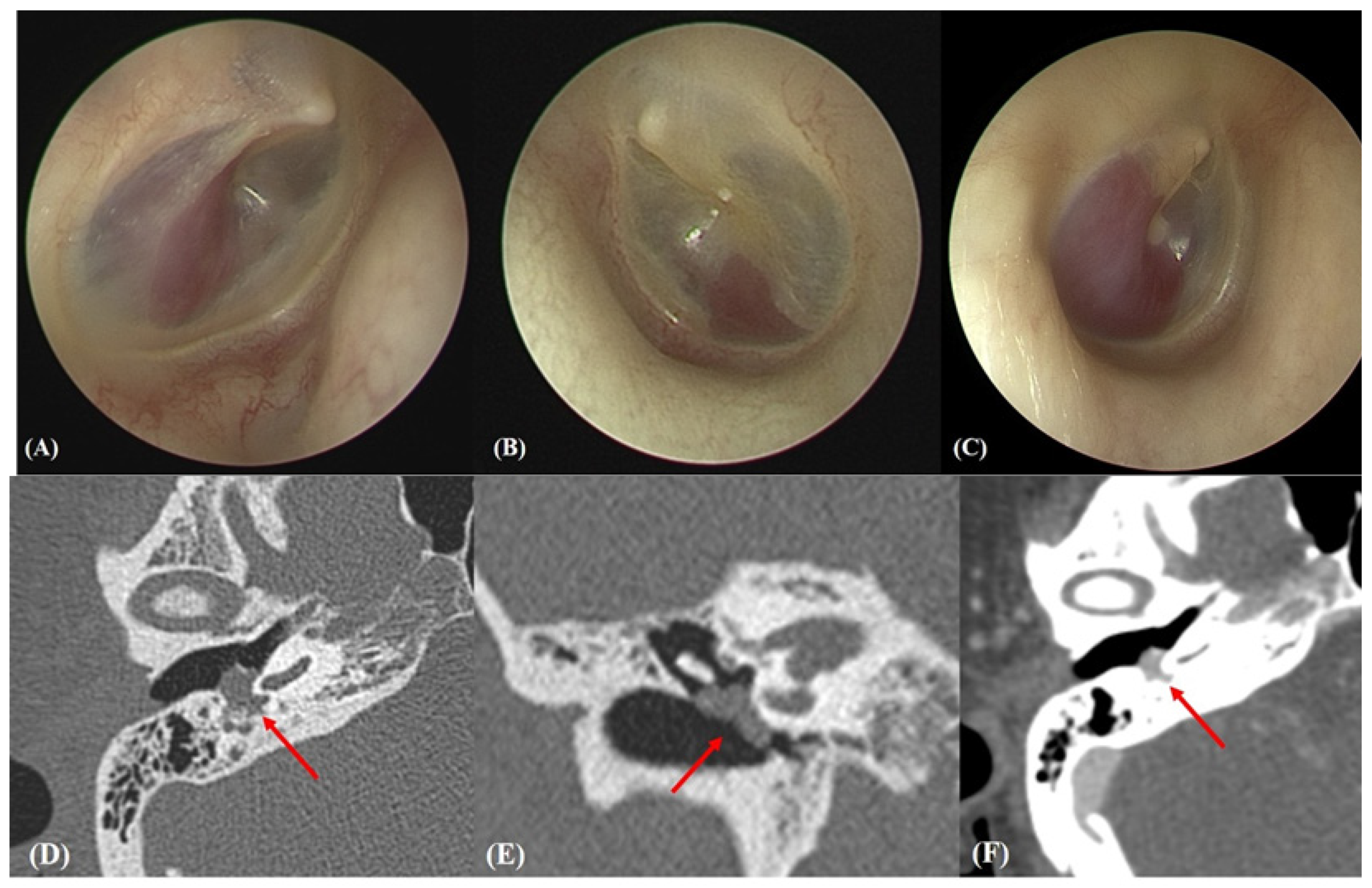
2.2. Otoendoscopic and Radiological Evaluations
2.3. Subjective Evaluation
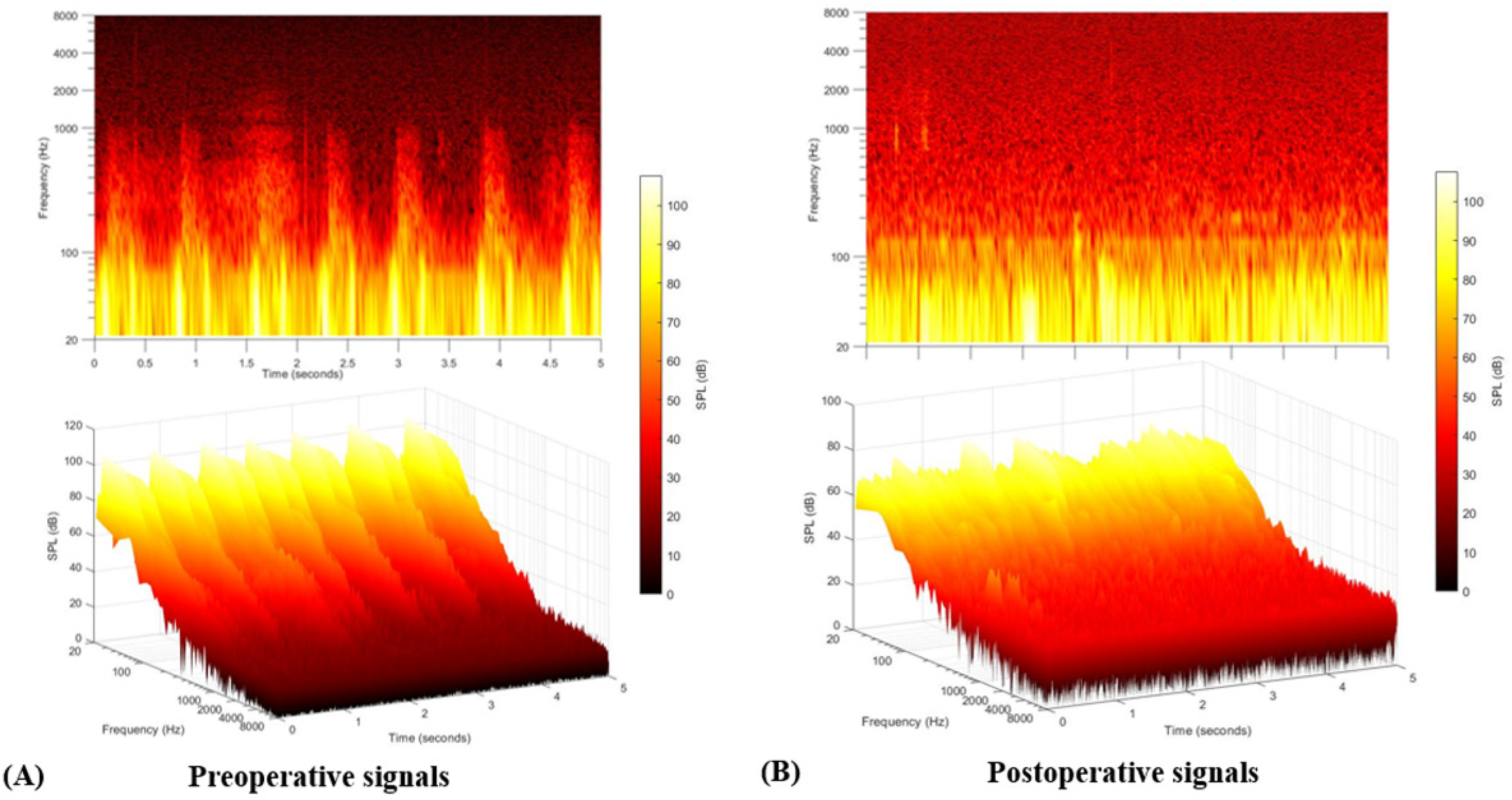
2.4. Objective Evaluation
2.5. Surgical Management
2.6. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics
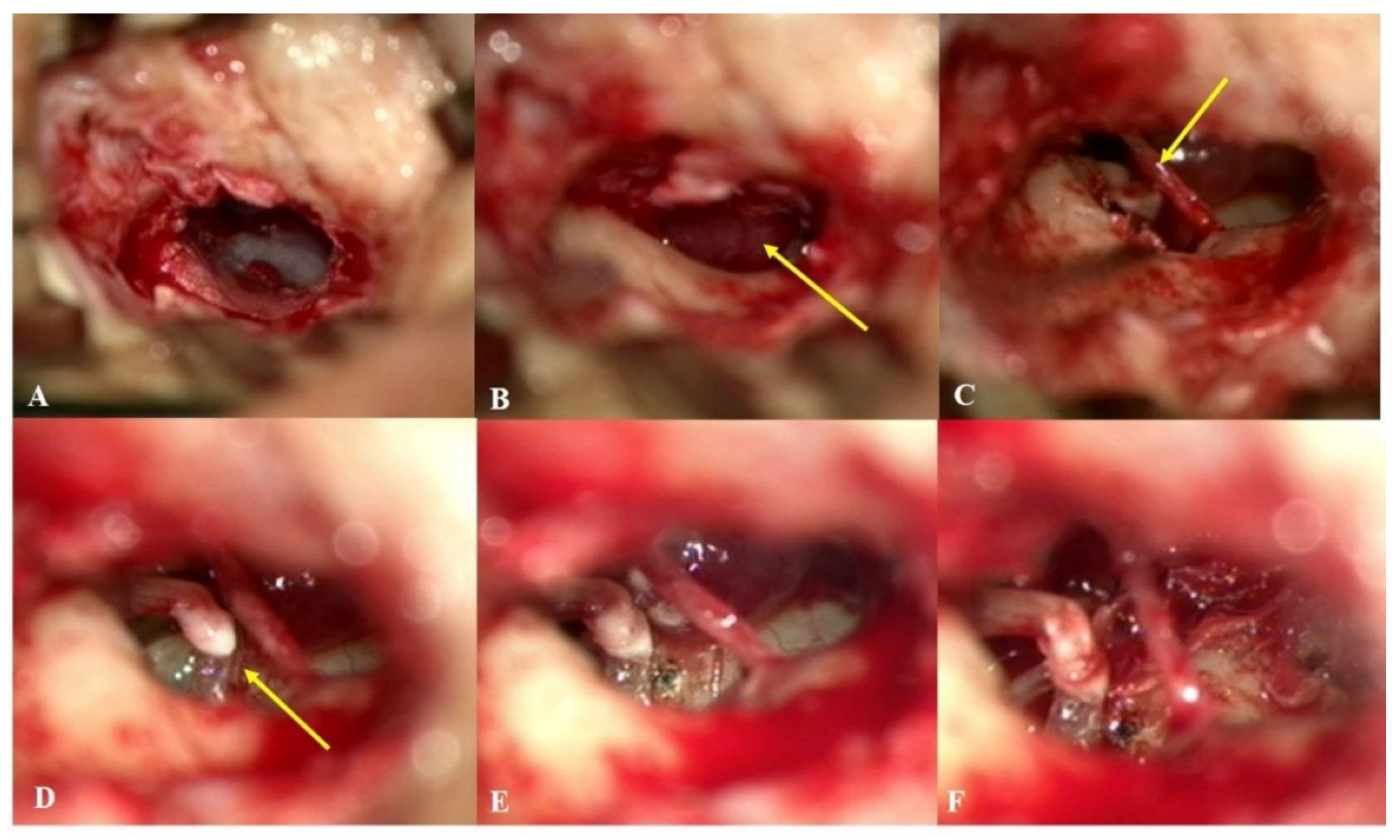
3.2. Intraoperative Findings
3.3. Subjective Outcomes
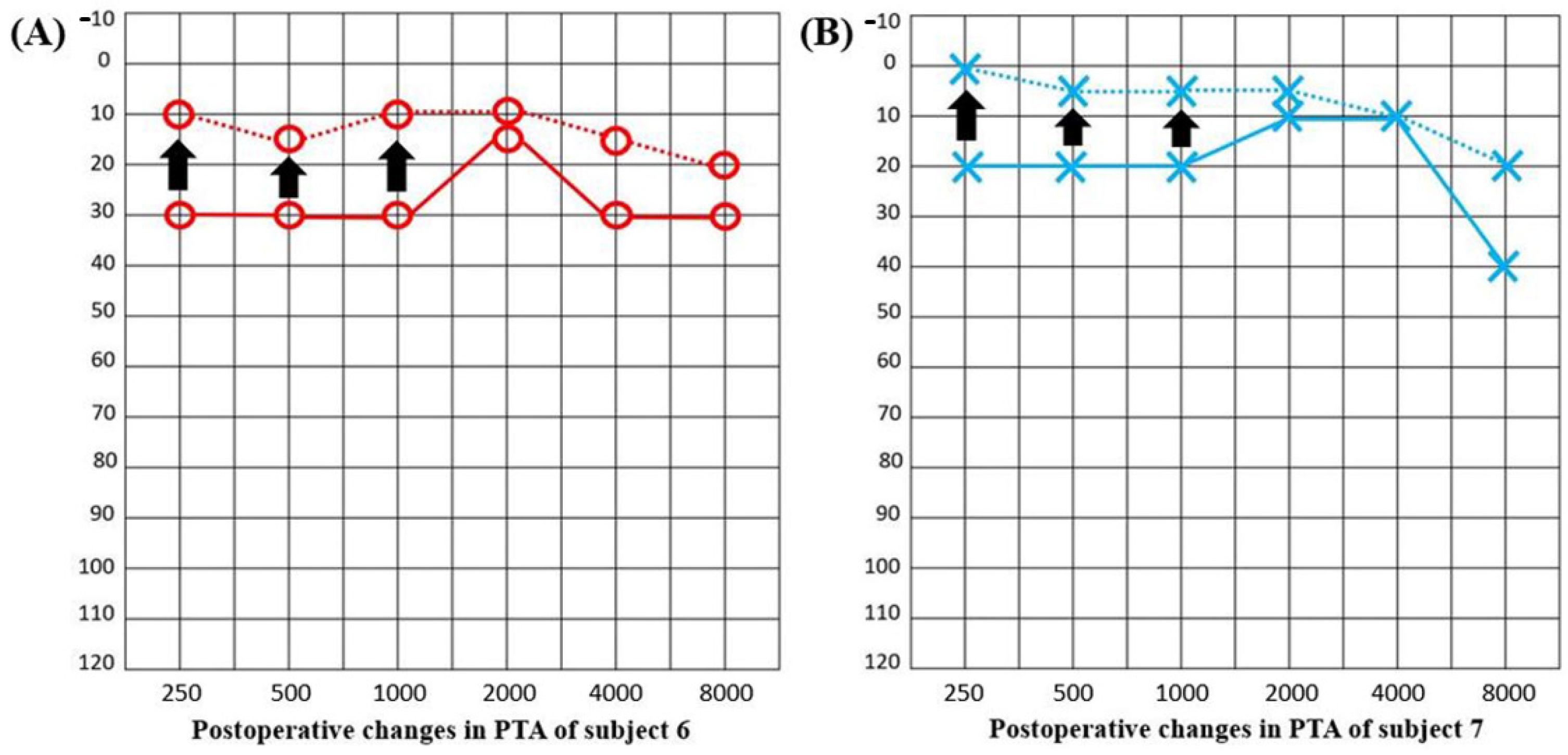
3.4. Objective Outcomes
3.5. Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ahsan, S.F.; Seidman, M.; Yaremchuk, K. What is the best imaging modality in evaluating patients with unilateral pulsatile tinnitus? Laryngoscope 2014, 125, 284–285. [Google Scholar] [CrossRef] [PubMed]
- Wanna, G.B. Tumors of the Ear and Lateral Skull Base: Part 1, An Issue of Otolaryngologic Clinics of North America, E-Book; Elsevier Health Sciences: Amsterdam, The Netherlands, 2015; Volume 48. [Google Scholar]
- Forest, J.A.; Jackson, C.G.; McGrew, B.M. Long-Term Control of Surgically Treated Glomus Tympanicum Tumors. Otol. Neurotol. 2001, 22, 232–236. [Google Scholar] [CrossRef] [PubMed]
- Carlson, M.L.; Sweeney, A.D.; Pelosi, S.; Wanna, G.B.; Glasscock III, M.E.; Haynes, D.S. Glomus tympanicum: A review of 115 cases over 4 decades. Otolaryngol. Head Neck Surg. 2015, 152, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Jackson, C.G.; Glasscock, M.E.; Harris, P.F. Glomus Tumors: Diagnosis, Classification, and Management of Large Lesions. Arch. Otolaryngol. Head Neck Surg. 1982, 108, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Fayad, J.N.; Keles, B.; Brackmann, D.E. Jugular foramen tumors: Clinical characteristics and treatment outcomes. Otol. Neurotol. 2010, 31, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Foote, R.L.; Pollock, B.E.; Gorman, D.A.; Schomberg, P.J.; Stafford, S.L.; Link, M.J.; Kline, R.W.; Strome, S.E.; Kasperbauer, J.L.; Olsen, K.D. Glomus jugulare tumor: Tumor control and complications after stereotactic radiosurgery. Head Neck 2002, 24, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Jeon, H.W.; Kim, S.Y.; Choi, B.S.; Bae, Y.J.; Koo, J.-W.; Song, J.-J. Pseudo-low Frequency Hearing Loss and Its Improvement After Treatment May Be Objective Signs of Significant Vascular Pathology in Patients with Pulsatile Tinnitus. Otol. Neurotol. 2016, 37, 1344–1349. [Google Scholar] [CrossRef] [PubMed]
- Song, J.-J.; An, G.S.; Choi, I.; De Ridder, D.; Kim, S.Y.; Choi, H.S.; Park, J.H.; Choi, B.Y.; Koo, J.-W.; Lee, K. Objectification and differential diagnosis of vascular pulsatile tinnitus by transcanal sound recording and spectrotemporal analysis: A preliminary study. Otol. Neurotol. 2016, 37, 613–620. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; An, G.S.; Choi, I.; Koo, J.-W.; Lee, K.; Song, J.-J. Pre-Treatment Objective Diagnosis and Post-Treatment Outcome Evaluation in Patients with Vascular Pulsatile Tinnitus Using Transcanal Recording and Spectro-Temporal Analysis. PLoS ONE 2016, 11, e0157722. [Google Scholar] [CrossRef]
- Lee, S.-Y.; Kim, M.-K.; Bae, Y.J.; An, G.S.; Lee, K.; Choi, B.Y.; Koo, J.-W.; Song, J.-J. Longitudinal analysis of surgical outcome in subjects with pulsatile tinnitus originating from the sigmoid sinus. Sci. Rep. 2020, 10, 18194. [Google Scholar] [CrossRef]
- Honkura, Y.; Hidala, H.; Ohta, J.; Gorai, S.; Katori, Y.; Kobayashi, T. Surgical treatment for the aberrant internal carotid artery in the middle ear with pulsatile tinnitus. Auris Nasus Larynx 2014, 41, 215–218. [Google Scholar] [CrossRef] [PubMed]
- Gandía-González, M.L.; Kusak, M.E.; Moreno, N.M.; Sárraga, J.G.; Rey, G.; Álvarez, R.M. Jugulotympanic paragangliomas treated with Gamma Knife radiosurgery: A single-center review of 58 cases. J. Neurosurg. 2014, 121, 1158–1165. [Google Scholar] [CrossRef] [PubMed]
- Appannan, V.; Daud, M.M. Glomus tympanicum. Malays. Fam. Physician 2018, 13, 45–48. [Google Scholar] [PubMed]
- Hofmann, E.; Behr, R.; Neumann-Haefelin, T.; Schwager, K. Pulsatile tinnitus: Imaging and differential diagnosis. Dtsch. Ärzteblatt Int. 2013, 110, 451. [Google Scholar]
- Liyanage, S.H.; Singh, A.; Savundra, P.; Kalan, A. Pulsatile tinnitus. J. Laryngol. Otol. 2005, 120, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Sismanis, A. Pulsatile tinnitus. A 15-year experience. Am. J. Otol. 1998, 19, 998. [Google Scholar]
- Subashini, P.; Mohanty, S. Altered clinical course of glomus tympanicum—A case report. Indian J. Otolaryngol. Head Neck Surg. 2008, 60, 35–36. [Google Scholar] [CrossRef] [PubMed]
- Tasar, M.; Yetiser, S. Glomus Tumors: Therapeutic Role of Selective Embolization. J. Craniofac. Surg. 2004, 15, 497–505. [Google Scholar] [CrossRef]
- Devuyst, L.; Defreyne, L.; Praet, M.; Geukens, S.; Dhooge, I. Treatment of glomus tympanicum tumors by preoperative embolization and total surgical resection. Am. J. Otolaryngol. 2016, 37, 544–551. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pt | Sex | Age (Year) | Site | Symptom Duration (Months) | Follow-Up Period (Months) | C.C | Preop PTA (dB) | Postop PTA (dB) | Preop NRS Score for Loudness | Postop NRS Score for Loudness |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | F | 39 | R | 3 | 49 | PT | 10.84 | 10 | N/A | N/A |
| 2 | F | 80 | L | 1 | 15 | PT | 29.17 | 32.5 | N/A | N/A |
| 3 | F | 80 | R | 1 | 7 | PT | 43.33 | 48.33 | N/A | N/A |
| 4 | F | 56 | R | 6 | 6 | PT | 9.17 | 12.5 | 5 | 1 |
| 5 | F | 68 | L | 12 | 5 | PT | 21.67 | 32.5 | 5 | 0 |
| 6 | F | 45 | R | 3 | 5 | PT | 22.5 (LFHL) | 10.83 | 8 | 0 |
| 7 | F | 34 | L | 11 | 38 | PT | 13.33 (LFHL) | 5 | 2 | 0 |
| 8 | F | 63 | R | 7 | 2 | PT | 24.17 | 29.17 | 2 | 0 |
| 9 | F | 52 | R | 0 | 15 | Incidentally | 7.5 | 10 | N/A | N/A |
| 10 | F | 38 | R | 0 | 26 | Incidentally | 3.33 | 6.67 | N/A | N/A |
| 11 | F | 77 | R | 0 | 2 | Incidentally | 42.5 | 42.5 | N/A | N/A |
| 12 | F | 41 | R | 5 | 73 | Otalgia | 7.5 | 8.33 | N/A | N/A |
| 13 | F | 63 | R | 10 | 12 | Otalgia | 34.17 | 36.67 | N/A | N/A |
| Pt | Surgery | Preop. TFCA | Preop. Embolization | Feeding Vessel | Postop. Complications | Final Pathology |
|---|---|---|---|---|---|---|
| 1 | Transcanal | N | N | Unknown | None | GTT |
| 2 | Retroauricular transcanal | N | N | Unknown | None | GTT |
| 3 | Endaural, T1 | Y | N | Distal small branch of the APA | None | GTT |
| 4 | Retroauricular | Y | N | Small petrous branch of the MMA | None | GTT |
| 5 | Endaural | Y | Y | Collateral vessels of the VA | None | GTT |
| 6 | Endaural, T1 | Y | N | Collateral vessels of the APA, IMA | Delayed FNP | GTT |
| 7 | Retroauricular transcanal | Y | Y | Collateral vessels of the APA | None | GTT |
| 8 | Endaural | Y | N | Small branch of the ECA | None | GTT |
| 9 | Endaural, T1 | N | N | Unknown | None | GTT |
| 10 | Retroauricular transcanal | N | N | Unknown | None | GTT |
| 11 | Endaural | N | N | Unknown | None | GTT |
| 12 | Endaural, T1 | N | N | Unknown | None | GTT |
| 13 | Endaural | N | N | Unknown | None | GTT |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.-J.; Lee, S.-Y.; An, G.-S.; Lee, K.; Choi, B.-Y.; Koo, J.-W.; Song, J.-J. Treatment Outcomes of Patients with Glomus Tympanicum Tumors Presenting with Pulsatile Tinnitus. J. Clin. Med. 2021, 10, 2348. https://doi.org/10.3390/jcm10112348
Lee S-J, Lee S-Y, An G-S, Lee K, Choi B-Y, Koo J-W, Song J-J. Treatment Outcomes of Patients with Glomus Tympanicum Tumors Presenting with Pulsatile Tinnitus. Journal of Clinical Medicine. 2021; 10(11):2348. https://doi.org/10.3390/jcm10112348
Chicago/Turabian StyleLee, Seung-Jae, Sang-Yeon Lee, Gwang-Seok An, Kyogu Lee, Byung-Yoon Choi, Ja-Won Koo, and Jae-Jin Song. 2021. "Treatment Outcomes of Patients with Glomus Tympanicum Tumors Presenting with Pulsatile Tinnitus" Journal of Clinical Medicine 10, no. 11: 2348. https://doi.org/10.3390/jcm10112348
APA StyleLee, S.-J., Lee, S.-Y., An, G.-S., Lee, K., Choi, B.-Y., Koo, J.-W., & Song, J.-J. (2021). Treatment Outcomes of Patients with Glomus Tympanicum Tumors Presenting with Pulsatile Tinnitus. Journal of Clinical Medicine, 10(11), 2348. https://doi.org/10.3390/jcm10112348