
Endoscopic Vacuum Therapy in Patients with Transmural Defects of the Upper Gastrointestinal Tract: A Systematic Review with Meta-Analysis


Abstract
1. Introduction
2. Material and Methods
2.1. Literature Search Strategy
2.2. Study Selection
2.3. Data Extraction
2.4. Primary and Secondary Outcomes
2.5. Methodological Quality
2.6. Statistical Analysis
3. Results
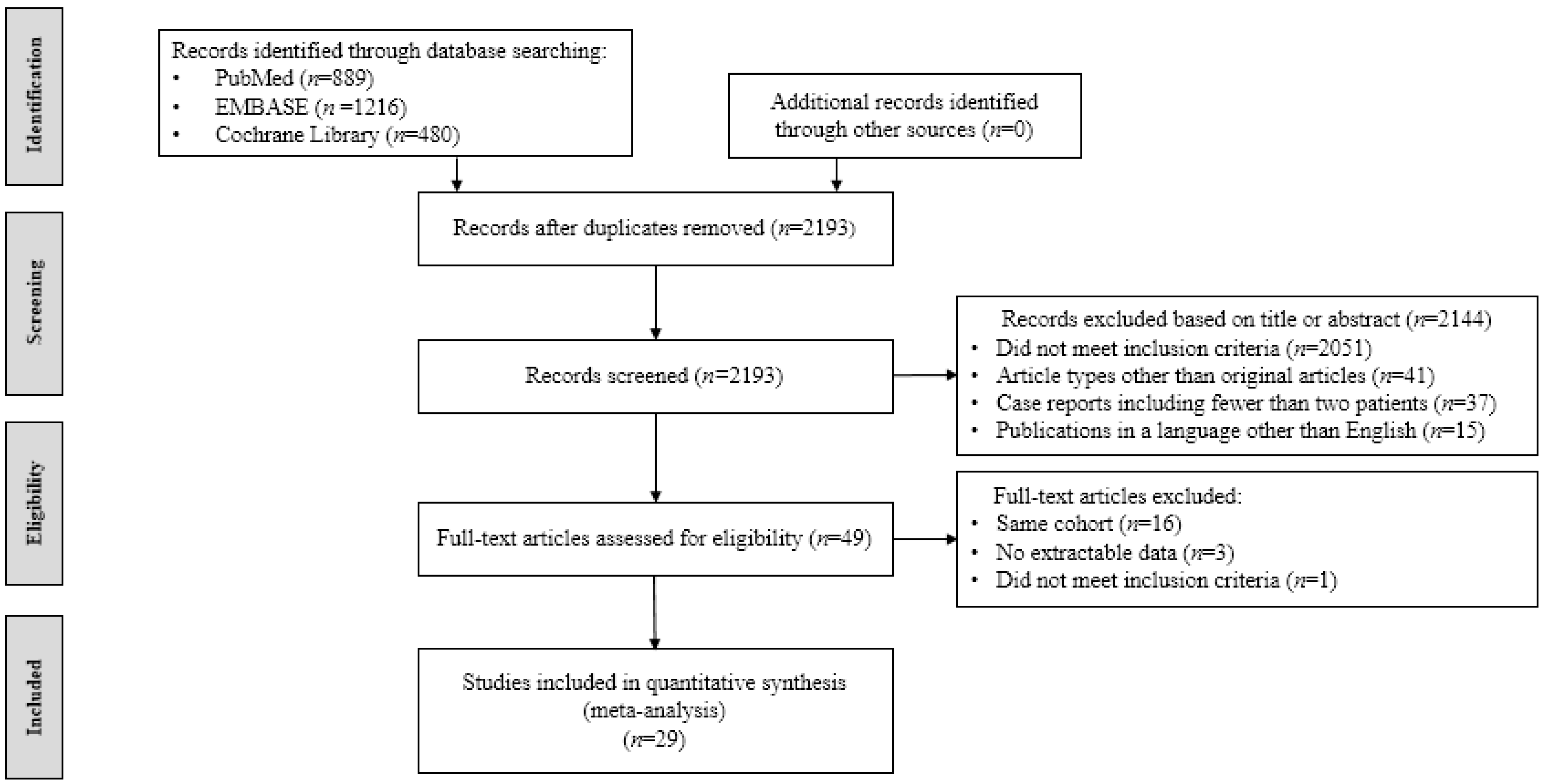
3.1. Study Selection
3.2. Study Characteristics and Methodological Quality
3.3. Primary and Secondary Outcomes
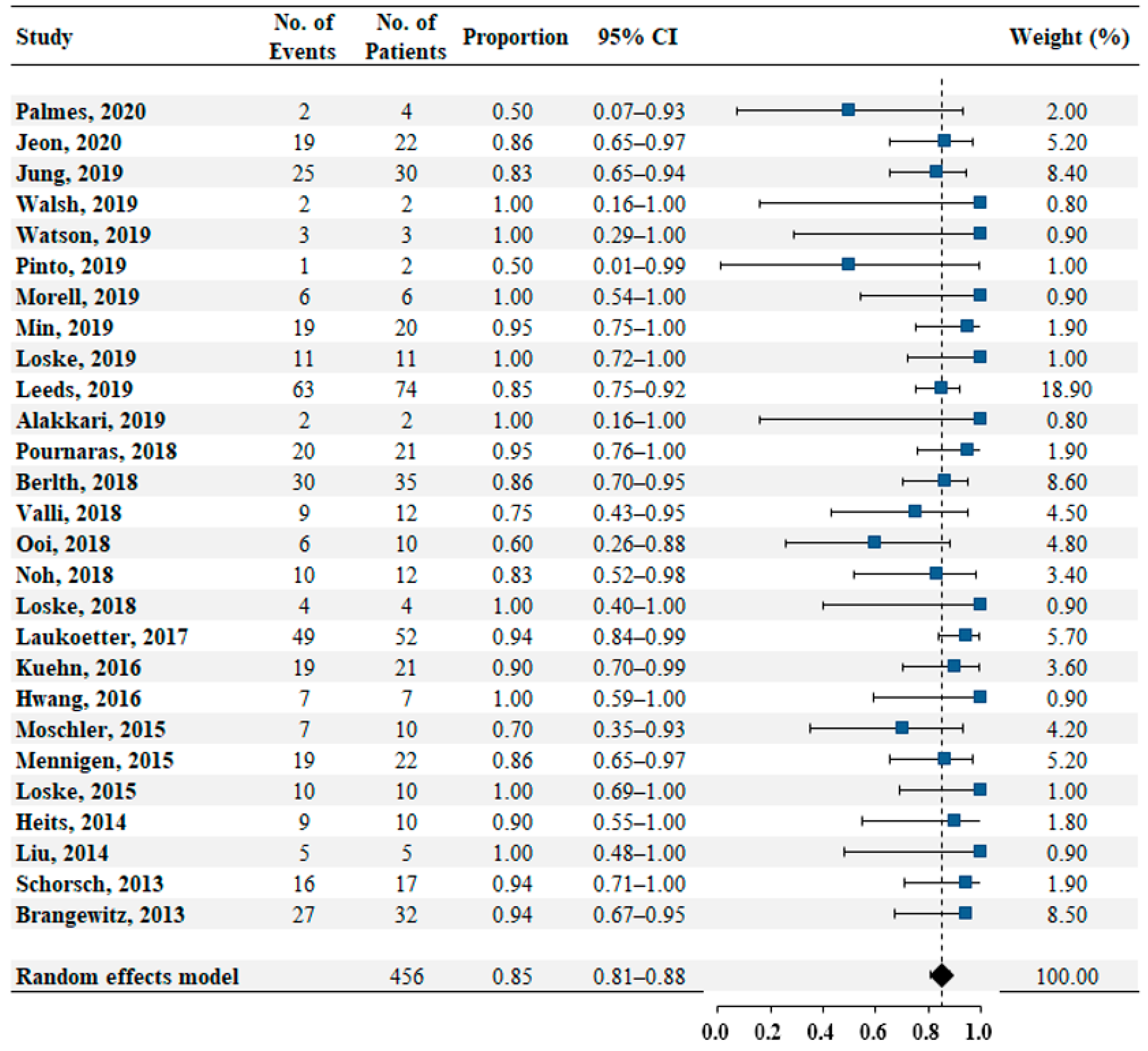
3.3.1. Primary Outcome—Successful Closure Rate
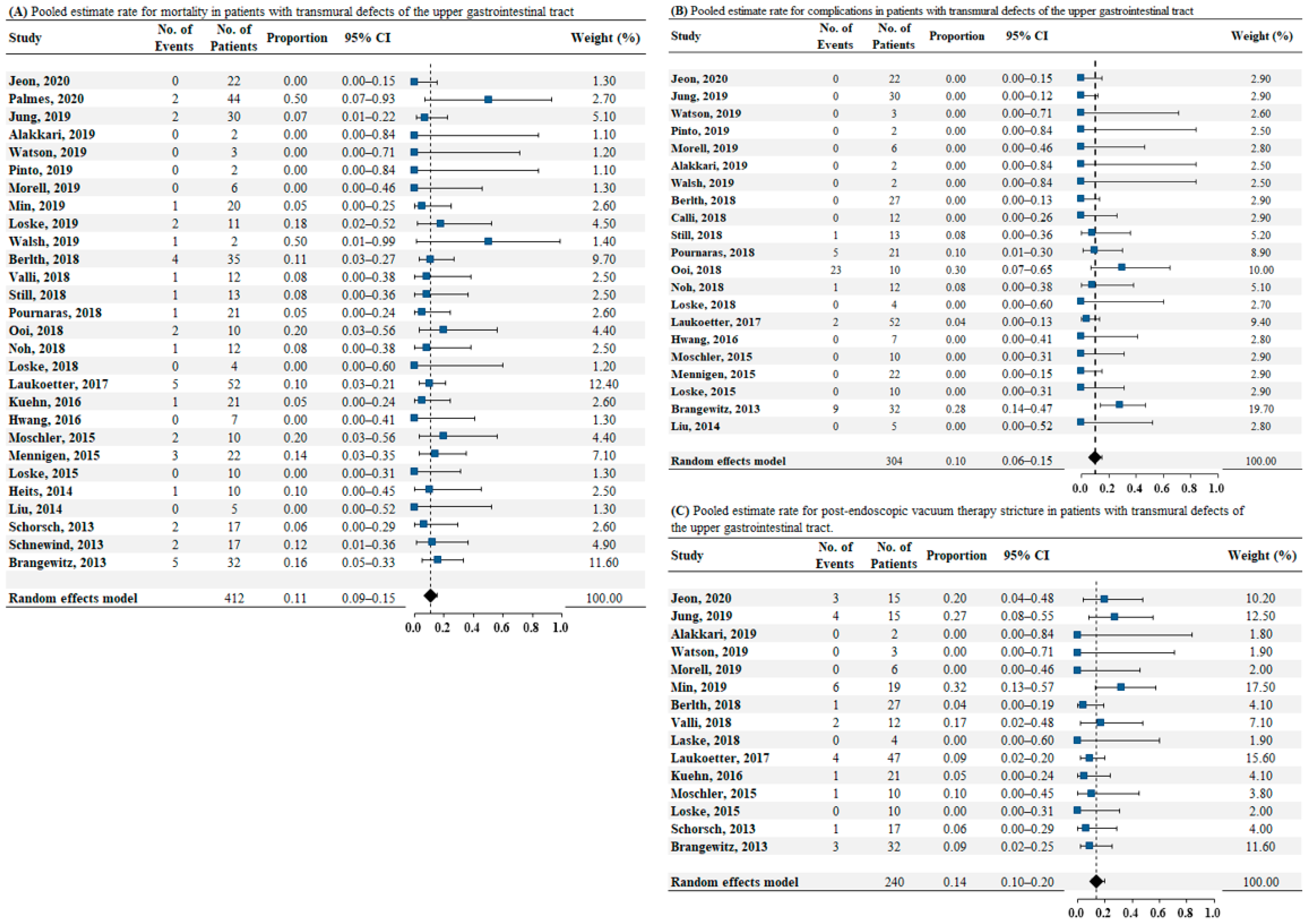
3.3.2. Secondary Outcomes—Mortality, Complication, and Post-EVT Stricture Rates
3.4. Subgroup Analysis
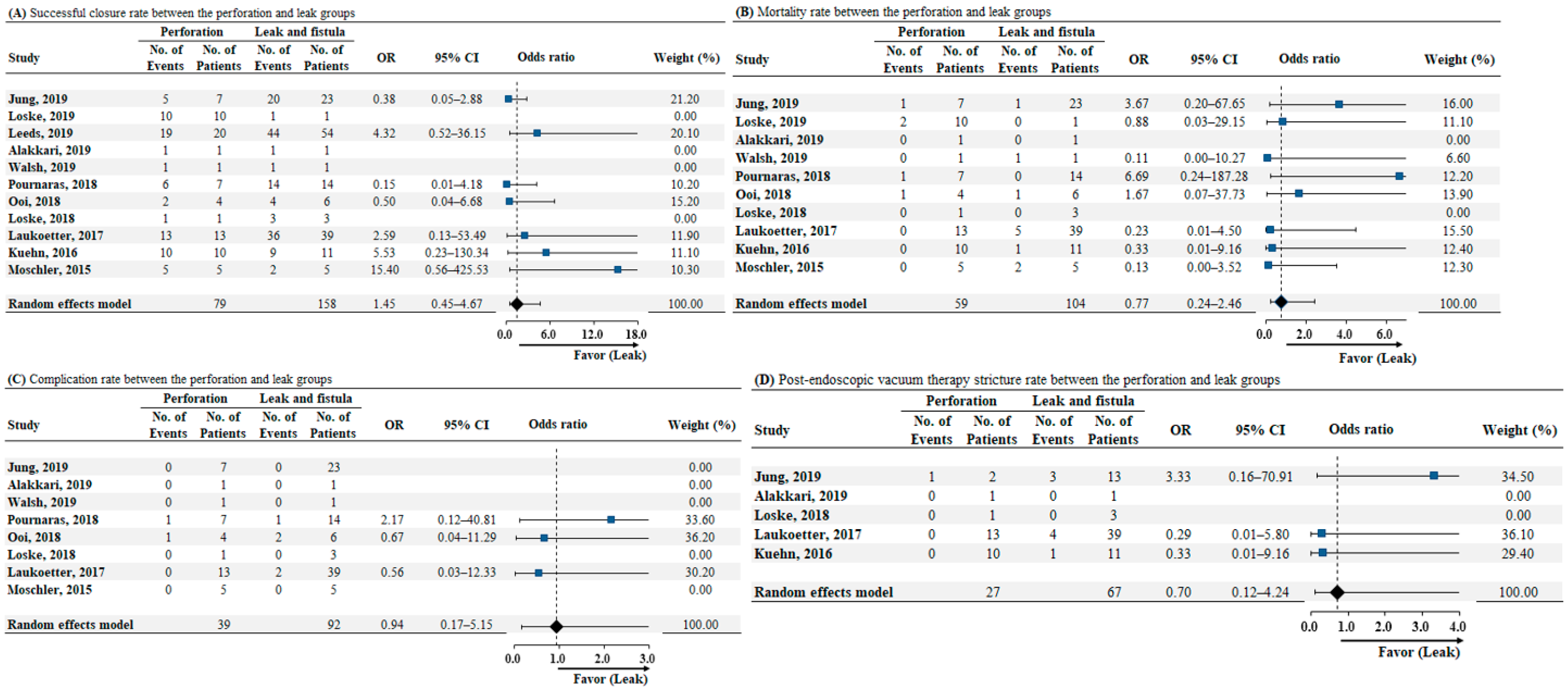
3.4.1. Perforation vs. Leak and Fistula—Successful Closure, Mortality, Complications, and Post-EVT Stricture Rates
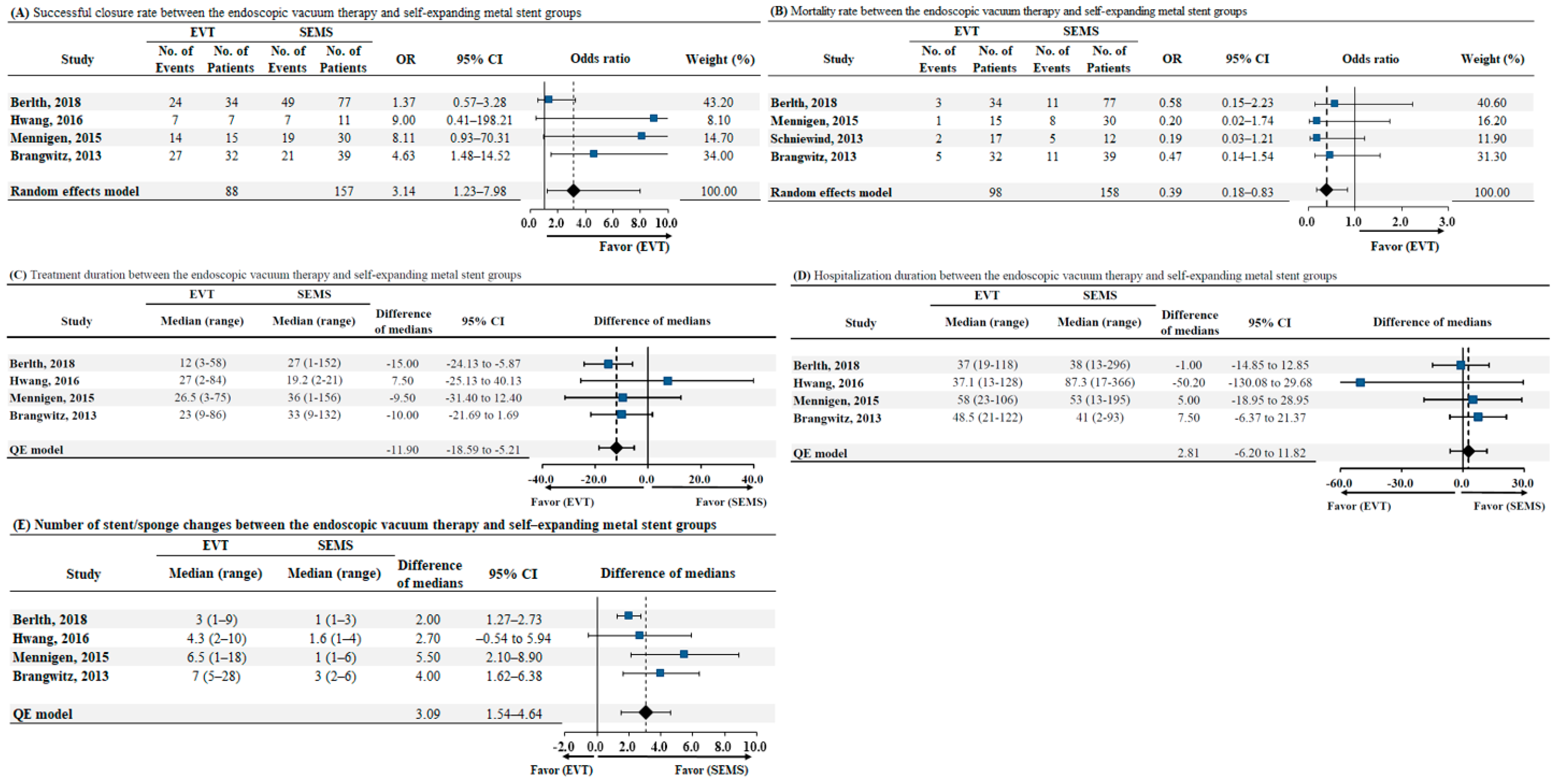
3.4.2. EVT vs. SEMS—Successful Closure, Mortality, Treatment Duration, Length of Hospital Stay, and the Number of Endoscopic Stent/Sponge Changes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Freni, F.; Galletti, B.; Bruno, R.; Martines, F.; Abita, P.; Gazia, F.; Sireci, F.; Galletti, F. Multidisciplinary approach in the removal of post-trauma foreign bodies in the head and neck district: Cases report and review of literature. Acta Med. Mediterr. 2019, 35, 405–410. [Google Scholar]
- Canevari, F.R.; Martines, F.; Sorrentino, R.; Nicolotti, M.; Sireci, F. Pseudoaneurysm of Superior Thyroid Artery Following A Transesophageal Echocardiography: A Case Presentation. Euromediter. Biomed. J. 2017, 12, 010–012. [Google Scholar]
- Bufkin, B.L.; Miller, J.I., Jr.; Mansour, K.A. Esophageal perforation: Emphasis on management. Ann. Thorac. Surg. 1996, 61, 1447–1451. [Google Scholar] [CrossRef]
- Altorjay, A.; Kiss, J.; Voros, A.; Bohak, A. Nonoperative management of esophageal perforations. Is it justified? Ann. Surg. 1997, 225, 415–421. [Google Scholar] [CrossRef]
- Brinster, C.J.; Singhal, S.; Lee, L.; Marshall, M.B.; Kaiser, L.R.; Kucharczuk, J.C. Evolving options in the management of esophageal perforation. Ann. Thorac. Surg. 2004, 77, 1475–1483. [Google Scholar] [CrossRef]
- Rohatgi, A.; Papanikitas, J.; Sutcliffe, R.; Forshaw, M.; Mason, R. The role of oesophageal diversion and exclusion in the management of oesophageal perforations. Int. J. Surg. 2009, 7, 142–144. [Google Scholar] [CrossRef]
- Kauer, W.K.; Stein, H.J.; Dittler, H.J.; Siewert, J.R. Stent implantation as a treatment option in patients with thoracic anastomotic leaks after esophagectomy. Surg. Endosc. 2008, 22, 50–53. [Google Scholar] [CrossRef] [PubMed]
- Huh, C.W.; Kim, J.S.; Choi, H.H.; Lee, J.I.; Ji, J.S.; Kim, B.W.; Choi, H. Treatment of benign perforations and leaks of the esophagus: Factors associated with success after stent placement. Surg. Endosc. 2018, 32, 3646–3651. [Google Scholar] [CrossRef] [PubMed]
- Boulis, N.M.; Armstrong, W.S.; Chandler, W.F.; Orringer, M.B. Epidural abscess: A delayed complication of esophageal stenting for benign stricture. Ann. Thorac. Surg. 1999, 68, 568–570. [Google Scholar] [CrossRef]
- Ho, H.S.; Ong, H.S. A rare life-threatening complication of migrated nitinol self-expanding metallic stent (ultraflex). Surg. Endosc. 2004, 18, 347. [Google Scholar] [CrossRef]
- Swinnen, J.; Eisendrath, P.; Rigaux, J.; Kahegeshe, L.; Lemmers, A.; Le Moine, O.; Deviere, J. Self-expandable metal stents for the treatment of benign upper GI leaks and perforations. Gastrointest. Endosc. 2011, 73, 890–899. [Google Scholar] [CrossRef] [PubMed]
- Bludau, M.; Fuchs, H.F.; Herbold, T.; Maus, M.K.H.; Alakus, H.; Popp, F.; Leers, J.M.; Bruns, C.J.; Holscher, A.H.; Schroder, W.; et al. Results of endoscopic vacuum-assisted closure device for treatment of upper gi leaks. Surg. Endosc. 2018, 32, 1906–1914. [Google Scholar] [CrossRef] [PubMed]
- Min, Y.W.; Kim, T.; Lee, H.; Min, B.H.; Kim, H.K.; Choi, Y.S.; Lee, J.H.; Rhee, P.L.; Kim, J.J.; Zo, J.I.; et al. Endoscopic vacuum therapy for postoperative esophageal leak. BMC Surg. 2019, 19, 37. [Google Scholar] [CrossRef] [PubMed]
- Jung, C.F.M.; Muller-Dornieden, A.; Gaedcke, J.; Kunsch, S.; Gromski, M.A.; Biggemann, L.; Hosseini, A.S.A.; Ghadimi, M.; Ellenrieder, V.; Wedi, E. Impact of endoscopic vacuum therapy with low negative pressure for esophageal perforations and postoperative anastomotic esophageal leaks. Digestion 2020, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Wedemeyer, J.; Schneider, A.; Manns, M.P.; Jackobs, S. Endoscopic vacuum-assisted closure of upper intestinal anastomotic leaks. Gastrointest. Endosc. 2008, 67, 708–711. [Google Scholar] [CrossRef]
- Loske, G.; Schorsch, T.; Muller, C. Endoscopic vacuum sponge therapy for esophageal defects. Surg. Endosc. 2010, 24, 2531–2535. [Google Scholar] [CrossRef] [PubMed]
- Smallwood, N.R.; Fleshman, J.W.; Leeds, S.G.; Burdick, J.S. The use of endoluminal vacuum (E-vac) therapy in the management of upper gastrointestinal leaks and perforations. Surg. Endosc. 2016, 30, 2473–2480. [Google Scholar] [CrossRef]
- Laukoetter, M.G.; Mennigen, R.; Neumann, P.A.; Dhayat, S.; Horst, G.; Palmes, D.; Senninger, N.; Vowinkel, T. Successful closure of defects in the upper gastrointestinal tract by endoscopic vacuum therapy (EVT): A prospective cohort study. Surg. Endosc. 2017, 31, 2687–2696. [Google Scholar] [CrossRef]
- Virgilio, E.; Ceci, D.; Cavallini, M. Surgical endoscopic vacuum-assisted closure therapy (EVAC) in treating anastomotic leakages after major resective surgery of esophageal and gastric cancer. Anticancer Res. 2018, 38, 5581–5587. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Brangewitz, M.; Voigtlander, T.; Helfritz, F.A.; Lankisch, T.O.; Winkler, M.; Klempnauer, J.; Manns, M.P.; Schneider, A.S.; Wedemeyer, J. Endoscopic closure of esophageal intrathoracic leaks: Stent versus endoscopic vacuum-assisted closure, a retrospective analysis. Endoscopy 2013, 45, 433–438. [Google Scholar] [CrossRef]
- Schniewind, B.; Schafmayer, C.; Voehrs, G.; Egberts, J.; von Schoenfels, W.; Rose, T.; Kurdow, R.; Arlt, A.; Ellrichmann, M.; Jurgensen, C.; et al. Endoscopic endoluminal vacuum therapy is superior to other regimens in managing anastomotic leakage after esophagectomy: A comparative retrospective study. Surg. Endosc. 2013, 27, 3883–3890. [Google Scholar] [CrossRef]
- Heits, N.; Stapel, L.; Reichert, B.; Schafmayer, C.; Schniewind, B.; Becker, T.; Hampe, J.; Egberts, J.H. Endoscopic endoluminal vacuum therapy in esophageal perforation. Ann. Thorac. Surg. 2014, 97, 1029–1035. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.N.; Yan, Y.; Li, S.J.; Liu, H.; Wu, Q.; Zhang, L.J.; Yang, Y.; Chen, J.F. Reliable management of post-esophagectomy anastomotic fistula with endoscopic trans-fistula negative pressure drainage. World J. Surg. Oncol. 2014, 12, 240. [Google Scholar] [CrossRef] [PubMed]
- Schorsch, T.; Muller, C.; Loske, G. Endoscopic vacuum therapy of perforations and anastomotic insufficiency of the esophagus. Chirurg 2014, 85, 1081–1093. [Google Scholar] [CrossRef]
- Loske, G.; Schorsch, T.; Dahm, C.; Martens, E.; Muller, C. Iatrogenic perforation of esophagus successfully treated with endoscopic vacuum therapy (EVT). Endosc. Int. Open 2015, 3, E547–E551. [Google Scholar] [CrossRef]
- Mennigen, R.; Harting, C.; Lindner, K.; Vowinkel, T.; Rijcken, E.; Palmes, D.; Senninger, N.; Laukoetter, M.G. Comparison of endoscopic vacuum therapy versus stent for anastomotic leak after esophagectomy. J. Gastrointest. Surg. 2015, 19, 1229–1235. [Google Scholar] [CrossRef]
- Moschler, O.; Nies, C.; Mueller, M.K. Endoscopic vacuum therapy for esophageal perforations and leakages. Endosc. Int. Open 2015, 3, E554–E558. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.J.; Jeong, Y.S.; Park, Y.S.; Yoon, H.; Shin, C.M.; Kim, N.; Lee, D.H. Comparison of endoscopic vacuum therapy and endoscopic stent implantation with self-expandable metal stent in treating postsurgical gastroesophageal leakage. Medicine 2016, 95, e3416. [Google Scholar] [CrossRef]
- Kuehn, F.; Schiffmann, L.; Janisch, F.; Schwandner, F.; Alsfasser, G.; Gock, M.; Klar, E. Surgical endoscopic vacuum therapy for defects of the upper gastrointestinal tract. J. Gastrointest. Surg. 2016, 20, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Loske, G.; Schorsch, T.; Rucktaeschel, F.; Schulze, W.; Riefel, B.; van Ackeren, V.; Mueller, C.T. Open-pore film drainage (OFD): A new multipurpose tool for endoscopic negative pressure therapy (ENPT). Endosc. Int. Open 2018, 6, E865–E871. [Google Scholar] [CrossRef] [PubMed]
- Noh, S.M.; Ahn, J.Y.; Lee, J.H.; Jung, H.Y.; AlGhamdi, Z.; Kim, H.R.; Kim, Y.H. Endoscopic vacuum-assisted closure therapy in patients with anastomotic leakage after esophagectomy: A single-center experience. Gastroenterol. Res. Pr. 2018, 2018, 1697968. [Google Scholar] [CrossRef] [PubMed]
- Ooi, G.; Burton, P.; Packiyanathan, A.; Loh, D.; Chen, R.; Shaw, K.; Brown, W.; Nottle, P. Indications and efficacy of endoscopic vacuum-assisted closure therapy for upper gastrointestinal perforations. ANZ J. Surg. 2018, 88, E257–E263. [Google Scholar] [CrossRef]
- Pournaras, D.J.; Hardwick, R.H.; Safranek, P.M.; Sujendran, V.; Bennett, J.; Macaulay, G.D.; Hindmarsh, A. Endoluminal vacuum therapy (E-vac): A treatment option in oesophagogastric surgery. World J. Surg. 2018, 42, 2507–2511. [Google Scholar] [CrossRef]
- Still, S.; Mencio, M.; Ontiveros, E.; Burdick, J.; Leeds, S.G. Primary and rescue endoluminal vacuum therapy in the management of esophageal perforations and leaks. Ann. Thorac. Cardiovasc. Surg. 2018, 24, 173–179. [Google Scholar] [CrossRef]
- Valli, P.V.; Mertens, J.C.; Kroger, A.; Gubler, C.; Gutschow, C.; Schneider, P.M.; Bauerfeind, P. Stent-over-sponge (SOS): A novel technique complementing endosponge therapy for foregut leaks and perforations. Endoscopy 2018, 50, 148–153. [Google Scholar] [CrossRef]
- Alakkari, A.; Sood, R.; Everett, S.M.; Rembacken, B.J.; Hayden, J.; Sarela, A.; Mohammed, N. First UK experience of endoscopic vacuum therapy for the management of oesophageal perforations and postoperative leaks. Frontline Gastroenterol. 2019, 10, 200–203. [Google Scholar] [CrossRef]
- Berlth, F.; Bludau, M.; Plum, P.S.; Herbold, T.; Christ, H.; Alakus, H.; Kleinert, R.; Bruns, C.J.; Holscher, A.H.; Chon, S.H. Self-expanding metal stents versus endoscopic vacuum therapy in anastomotic leak treatment after oncologic gastroesophageal surgery. J. Gastrointest. Surg. 2019, 23, 67–75. [Google Scholar] [CrossRef]
- Leeds, S.G.; Mencio, M.; Ontiveros, E.; Ward, M.A. Endoluminal vacuum therapy: How I do it. J. Gastrointest. Surg. 2019, 23, 1037–1043. [Google Scholar] [CrossRef]
- Loske, G.; Rucktaeschel, F.; Schorsch, T.; Moenkemueller, K.; Mueller, C.T. Endoscopic negative pressure therapy (ENPT) for duodenal leakage—novel repair technique using open-pore film (OFD) and polyurethane-foam drainages (OPD). Endosc. Int. Open 2019, 7, E1424–E1431. [Google Scholar] [CrossRef] [PubMed]
- Morell, B.; Murray, F.; Vetter, D.; Bueter, M.; Gubler, C. Endoscopic vacuum therapy (EVT) for early infradiaphragmal leakage after bariatric surgery-outcomes of six consecutive cases in a single institution. Langenbecks Arch. Surg. 2019, 404, 115–121. [Google Scholar] [CrossRef]
- Rodrigues-Pinto, E.; Morais, R.; Vilas-Boas, F.; Pereira, P.; Macedo, G. Role of endoscopic vacuum therapy, internal drainage, and stents for postbariatric leaks. VideoGIE 2019, 4, 481–485. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Walsh, L.T.; Loloi, J.; Manzo, C.E.; Mathew, A.; Maranki, J.; Dye, C.E.; Levenick, J.M.; Taylor, M.D.; Moyer, M.T. Successful treatment of large cavity esophageal disruptions with transluminal washout and endoscopic vacuum therapy: A report of two cases. Adv. Gastrointest. Endosc. 2019, 12, 2631774519860300. [Google Scholar] [CrossRef]
- Watson, A.; Zuchelli, T. Repair of upper-GI fistulas and anastomotic leakage by the use of endoluminal vacuum-assisted closure. VideoGIE 2019, 4, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Jeon, J.H.; Jang, H.J.; Han, J.E.; Park, Y.S.; Seong, Y.W.; Cho, S.; Jheon, S.; Kim, K. Endoscopic vacuum therapy in the management of postoperative leakage after esophagectomy. World J. Surg. 2020, 44, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Palmes, D.; Kebschull, L.; Bahde, R.; Senninger, N.; Pascher, A.; Laukotter, M.G.; Eichelmann, A.K. Management of nonmalignant tracheo- and bronchoesophageal fistula after esophagectomy. Thorac. Cardiovasc. Surg. 2020, 69, 216–222. [Google Scholar] [CrossRef]
- Kuehn, F.; Loske, G.; Schiffmann, L.; Gock, M.; Klar, E. Endoscopic vacuum therapy for various defects of the upper gastrointestinal tract. Surg. Endosc. 2017, 31, 3449–3458. [Google Scholar] [CrossRef]
- Verstegen, M.H.P.; Bouwense, S.A.W.; van Workum, F.; Ten Broek, R.; Siersema, P.D.; Rovers, M.; Rosman, C. Management of intrathoracic and cervical anastomotic leakage after esophagectomy for esophageal cancer: A systematic review. World J. Emerg. Surg. 2019, 14, 17. [Google Scholar] [CrossRef]
- Newton, N.J.; Sharrock, A.; Rickard, R.; Mughal, M. Systematic review of the use of endo-luminal topical negative pressure in oesophageal leaks and perforations. Dis. Esophagus 2017, 30, 1–5. [Google Scholar] [CrossRef]
- Argenta, L.C.; Morykwas, M.J. Vacuum-assisted closure: A new method for wound control and treatment: Clinical experience. Ann. Plast. Surg. 1997, 38, 563–576. [Google Scholar] [CrossRef]
- Wedemeyer, J.; Brangewitz, M.; Kubicka, S.; Jackobs, S.; Winkler, M.; Neipp, M.; Klempnauer, J.; Manns, M.P.; Schneider, A.S. Management of major postsurgical gastroesophageal intrathoracic leaks with an endoscopic vacuum-assisted closure system. Gastrointest. Endosc. 2010, 71, 382–386. [Google Scholar] [CrossRef] [PubMed]
- Schaheen, L.; Blackmon, S.H.; Nason, K.S. Optimal approach to the management of intrathoracic esophageal leak following esophagectomy: A systematic review. Am. J. Surg. 2014, 208, 536–543. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | Study Design | N | Male (n) | Age (Median, Years) | BMI (Median) | Region of Study | Follow-Up (Median, Months) | Method of Diagnosis | Defect Size (Median, mm) | Time to Diagnosis (Median, Days) | Time to Treatment (Median, Days) | Intracavitary/Intraluminary |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Palmes 2020 | Case series | Fistula: 4 | NA | NA | NA | Western (Germany) | MA | Endoscopy CT Esophagogram | NA | NA | NA | NA |
| Jung 2019 | Retrospective | Leak: 23 Perforation: 7 | 20 | 65.1 † | NA | Western (Germany) | 11.8 † | NA | NA | Leak: 8.5 Perforation: <1 | NA | IC: 6, IL: 24 |
| Jeon 2019 | Retrospective | Leak: 22 | 17 | 68 | NA | Eastern (Korea) | 29.8 | Endoscopy CT Esophagogram | NA | 11 | NA | IC: 10, IL: 12 |
| Watson 2019 | Case series | Leak: 2 Fistula: 1 | 2 | 69.6 † | NA | Western (USA) | 2.7 | Endoscopy | NA | NA | NA | NA |
| Pinto 2019 | Case series | Leak: 2 | 1 | 44.0 † | NA | Western (Portugal) | NA | Endoscopy CT | NA | NA | NA | IC: 2, IL: 1 |
| Morell 2019 | Case series | Leak: 6 | 2 | 49.0 † | 44.2 | Western (Switzerland) | NA | Endoscopy CT | 20† | 4.5 † | 3.3 † | NA |
| Min 2019 | Retrospective | Leak: 20 | 20 | 66.5 | NA | Eastern (Korea) | 7.1 | Endoscopy Esophagogram | 17.5 | 12.5 | 3 | IC: 20 |
| Loske 2019 | Case series | Leak: 1 Perforation: 10 | 4 | 65.7 † | NA | Western (Germany) | NA | Endoscopy CT | NA | NA | NA | IC: 1 IL: 10 |
| Leeds 2019 | Retrospective | Leak: 54 Perforation: 20 | NA | NA | NA | Western (USA) | NA | NA | NA | NA | NA | NA |
| Walsh 2019 | Case series | Leak: 1 Perforation: 1 | 1 | 69.5 | NA | Western (USA) | NA | NA | 20 | 21 | NA | NA |
| Alakkari 2019 | Case series | Leak: 1 Perforation: 1 | 0 | 67 † | NA | Western (UK) | NA | NA | NA | NA | 19 † | IC: 2 |
| Berlth 2018 | Retrospective | Leak: 111 EVT: 34 SEMS 77 | 92 | EVT: 65 SEMS: 64 | EVT: 26 SEMS: 26 | Western (Germany) | NA | Endoscopy CT Esophagogram | NA | EVT: 8 SEMS: 8 | EVT: 0 SEMS: 0 | NA |
| Valli 2018 | Retrospective | Leak: 11 Fistula: 1 | 9 | Leak: 57.5 Fistula: 80 | NA | Western (Switzerland) | NA | Endoscopy CT Esophagogram | NA | NA | Leak: 18.4 Fistula: 52 | IC: 7, IL: 5 |
| Still 2018 | Retrospective | Leak: 2 Perforation: 9 Fistula: 2 | 6 | 63 | 23 | Western (USA) | NA | Endoscopy CT Esophagogram | NA | NA | NA | IC: 3, IL: 7 |
| Pournaras 2018 | Retrospective | Leak: 14 Perforation: 7 | NA | NA | NA | Western (UK) | NA | NA | NA | NA | NA | NA |
| Ooi 2018 | Retrospective | Leak: 6 Perforation: 4 | NA | 56.7 † | NA | Western (Australia) | NA | NA | 18.3 | NA | 33.6 | NA |
| Noh 2018 | Retrospective | Leak: 12 | 12 | 57.0 | NA | Eastern (Korea) | 12.9 | CT Esophagogram | 13 | 13.5 | 11 | IC: 3, IL: 9 |
| Loske 2018 | Case series | Leak: 3 Perforation: 1 | NA | NA | NA | Western (Germany) | NA | NA | NA | NA | NA | NA |
| Laukoetter 2017 | Retrospective | Leak: 39 Perforation: 13 | 31 | 65 | NA | Western (Germany) | 5.4 | Endoscopy CT Esophagogram | NA | NA | 8 | NA |
| Kuehn 2016 | Retrospective | Leak: 11 Perforation: 10 | 15 | 72 | NA | Western (Germany) | 17 | Endoscopy CT Esophagogram | NA | NA | NA | IC: 10, IL: 11 |
| Hwang 2016 | Retrospective | Leak: 18 EVT: 7 SEMS 11 | 14 | EVT: 71.1 SEMS: 67.3 | NA | Eastern (Korea) | NA | NA | EVT: 8.1 SEMS: 6.6 | NA | NA | NA |
| Möschler 2015 | Retrospective | Leak: 5 Perforation: 5 | 5 | 73.9 † | NA | Western (Germany) | 4 | NA | NA | NA | NA | IC: 6, IL: 4 |
| Mennigen 2015 | Retrospective | Leak: 45 EVT: 15 SEMS 30 | 35 | EVT: 56 SEMS: 65.5 | NA | Western (Germany) | EVT: 8.3 SEMS: 16.8 | Endoscopy CT Esophagogram | NA | EVT: 7 SEMS: 7 | NA | IC: 22 |
| Loske 2015 | Case series | Perforation: 10 | NA | NA | NA | Western (Germany) | 2.8 | Endoscopy | 19 | <1 | NA | IC: 1, IL: 9 |
| Heits 2014 | Retrospective | Perforation: 10 | 5 | 66 † | NA | Western (Germany) | 9 | Endoscopy CT Esophagogram | 4.2 | NA | NA | NA |
| Liu 2014 | Case series | Leak: 5 | NA | 61.8 † | NA | Eastern (China) | NA | Endoscopy CT Esophagogram | NA | 9.2 | NA | NA |
| Schorsch 2013 | Retrospective | Leak: 17 | NA | NA | NA | Western (Germany) | NA | NA | 14.7 | 10 | NA | IC: 8, IL: 9 |
| Schniewind 2013 | Retrospective | Leak: 47 | NA | NA | NA | Western (Germany) | NA | NA | NA | NA | NA | NA |
| Brangewitz 2013 | Retrospective | EVT:32 SEMS: 39 | 58 | EVT:63 SEMS: 62 | EVT: 25.2 SEMS: 26.4 | Western (Germany) | NA | NA | NA | NA | NA | NA |
| Authors | N | Successful Closure Rate (n, %) | Mortality Rate (n, %) | Complication Rate (n, %) | Stricture Rate (n, %) | Hospital Stay (Median, Days) | ICU Stay (Median, Days) | Duration of Therapy (Median, Days) | Sponge Changes |
|---|---|---|---|---|---|---|---|---|---|
| Palmes 2020 | Fistula: 4 | 2/4 (50) | 2/4 (50) | NA | NA | NA | NA | 88.5 | NA |
| Jung 2019 | Leak: 23 | 20/23 (87.0) | 1/23 (4.3) | 0/23 (0) | 3/13 (23.1) | 54.4 | NA | 15.7 | 3.4 |
| Perforation: 7 | 5/7 (71.4) | 1/7 (14.3) | 0/7 (0) | 1/2 (50.0) | 33.7 | 27.0 | 6.4 | ||
| Jeon 2019 | Leak: 22 | 19/22 (86.4) | 0/22 (0) | 0/22 (0) | 3/15 (20.0) | 24 | NA | 13 | 3 |
| Watson 2019 | Leak: 2 | 2/2 (100.0) | 0/2 (0) | 0/2 (0) | 0/2 (0) | NA | NA | 16 | 3 |
| Fistula: 1 | 1/1 (100.0) | 0/1 (0) | 0/1 (0) | 0/1 (0) | 40 | 9 | |||
| Pinto 2019 | Leak: 2 | 1/2 (50.0) | 0/2 (0) | 0/2 (0) | NA | NA | NA | 22 | 3 |
| Morell 2019 | Leak: 6 | 6/6 (100.0) | 0/6 (0) | 0/6 (0) | 0/6 (0) | 39.8 † | 10.2 † | 32.3 † | 4 |
| Min 2019 | Leak: 20 | 19/20 | 1/20 | NA | 6/19 | 49 | NA | 14.5 | 5 |
| Loske 2019 | Leak: 1 | 1/1 (100.0) | 0/1 (0) | NA | NA | NA | NA | 11 | 1.8 |
| Perforation: 10 | 10/10 (100.0) | 2/10 (20.0) | |||||||
| Leeds 2019 | Leak: 54 | 44/54 (81.5) | NA | NA | NA | NA | NA | NA | NA |
| Perforation: 20 | 19/20 (95.0) | ||||||||
| Walsh 2019 | Leak: 1 | 2/2 (100.0) | 1/1 (100.0) | 0/1 (0) | NA | NA | NA | 55 | 10 |
| Perforation: 1 | 0/1 (0) | 0/1 (0) | 42 | 3 | |||||
| Alakkari 2019 | Leak: 1 | 1/1 (100.0) | 0/1 (0) | 0/1 (0) | 0/1 (0) | NA | NA | 28 | 6 |
| Perforation: 1 | 1/1 (100.0) | 0/1 (0) | 0/1 (0) | 0/1 (0) | 56 | 13 | |||
| Berlth 2018 | Leak: 111 EVT: 34 SEMS 77 | 24/34 (70.6) | 3/34 (0.9) | 0/27 (0) | 1/27 (3.7) | 37 | 8 | 12 | 3 |
| 49/77 (63.6) | 11/77 (14.3) | 13/69 (18.8) | 5/69 (7.2) | 38 | 7 | 27 | 1 | ||
| Valli 2018 | Leak: 11 | 9/11 (81.8) | 0/11 (0) | 0/11 (0) | 2/11 (18.1) | NA | NA | 20.8 | 5 |
| Fistula: 1 | 0/1 (0) | 1/1 (100.0) | 0/1 (0) | 0/1 (0) | 16 | 4 | |||
| Still 2018 | Leak: 2 | NA | 1/13 ‡ | 1/13 ‡ | NA | NA | NA | NA | NA |
| Perforation: 9 | |||||||||
| Fistula: 2 | |||||||||
| Pournaras 2018 | Leak: 14 | 14/14 (100.0) | 0/14 (0) | 1/14 (7.1) | NA | 35 | NA | NA | 7 |
| Perforation: 7 | 6/7 (85.7) | 1/7 (14.3) | 1/7 (14.3) | ||||||
| Ooi 2018 | Leak: 6 | 4/6 (66.7) | 1/6 (16.7) | 2/6 (33.3) | NA | 62 | 12 | 25.5 † | 8.3 † |
| Perforation: 4 | 2/4 (50.0) | 1/4 (25.0) | 1/4 (25.0) | ||||||
| Noh 2018 | Leak: 12 | 10/12 (83.3) | 1/12 (8.3) | 1/12 (8.3) | 1/12 (8.3) | NA | NA | 25 | 2.7 † |
| Loske 2018 | Leak: 3 | 3/3 (100.0) | 0/3 (0) | 0/3 (0) | 0/3 (0) | NA | NA | NA | NA |
| Perforation: 1 | 1/1 (100.0) | 0/1 (0) | 0/1 (0) | 0/1 (0) | |||||
| Laukoetter 2017 | Leak: 39 | 36/39 (92.3) | 5/39 (12.8) | 2/39 (5.1) § | 4/39 (10.2) | 60 | NA | 20 | 6 |
| Perforation: 13 | 13/13 (100.0) | 0/13 (0) | 0/13 (0) | 0/13 (0) | 46 | 24 | 6 | ||
| Kuehn 2016 | Leak: 11 | 9/11 (81.8) | 1/11 (18.2) | NA | 1/11 (18.2) | NA | NA | 12 | 4 |
| Perforation: 10 | 10/10 (100.0) | 0/10 (0) | 0/10 (0) | 15 | 5 | ||||
| Hwang 2016 | Leak: 18 EVT: 7 SEMS 11 | 7/7 (100.0) | NA | 0/7 (0) | NA | 37.1 | NA | 27 | 4.3 |
| 7/11 (63.6) | 6/11 (54.5) | 87.3 | 19.2 | 1.6 | |||||
| Möschler 2015 | Leak: 5 | 2/5 (40.0) | 2/5 (40.0) | 0/5 (0) | 1/10 (10.0) § | 38 | NA | 34.2 | 8.4 |
| Perforation: 5 | 5/5 (100.0) | 0/5 (0) | 0/5 (0) | 13 | 2 | ||||
| Mennigen 2015 | Leak: 45 EVT: 15 SEMS 30 | 14/15 (93.3) | 1/15 (6.6) | 0/15 (0) | NA | 58 | NA | 26.5 | 6.5 |
| 19/30 (63.3) | 8/30 (26.6) | 0/30 (0) | 53 | 36 | 1 | ||||
| Loske 2015 | Perforation: 10 | 10/10 (100.0) | 0/10 (0) | 0/10 (0) | 0/10 (0) | NA | NA | 5 | 2 |
| Heits 2014 | Perforation: 10 | 9/10 (90.0) | 1/10 (10.0) | NA | NA | 48 † | 22 † | NA | 5.4 † |
| Liu 2014 | Leak: 5 | 5/5 (100.0) | 0/5 (0) | 0/5 (0) | NA | NA | NA | 34.2 | NA |
| Schorsch 2013 | Leak: 17 | 16/17 (94.1) | 1/17 (5.9) | NA | 1/17 (5.9) | NA | NA | 12 | NA |
| Schniewind 2013 | Leak: 29 EVT: 17 SEMS 12 | NA | 2/17 (11.8) | NA | NA | 57 † | 26 † | NA | NA |
| 5/12 (41.7) | 62 † | 38 † | |||||||
| Brangewitz 2013 | EVT:32 | 27/32 (84.4) | 5/32 (15.6) | 9/32 (28.1) | 3/32 (9.4) | 48.5 | NA | 23 | 7 |
| SEMS: 39 | 21/39 (53.8) | 11/39 (28.2) | 3/39 (76.9) | 11/39 (28.2) | 41 | 33 | 3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, D.H.; Yun, H.-R.; Lee, S.J.; Kim, N.W.; Huh, C.W. Endoscopic Vacuum Therapy in Patients with Transmural Defects of the Upper Gastrointestinal Tract: A Systematic Review with Meta-Analysis. J. Clin. Med. 2021, 10, 2346. https://doi.org/10.3390/jcm10112346
Jung DH, Yun H-R, Lee SJ, Kim NW, Huh CW. Endoscopic Vacuum Therapy in Patients with Transmural Defects of the Upper Gastrointestinal Tract: A Systematic Review with Meta-Analysis. Journal of Clinical Medicine. 2021; 10(11):2346. https://doi.org/10.3390/jcm10112346
Chicago/Turabian StyleJung, Da Hyun, Hae-Ryong Yun, Se Joon Lee, Na Won Kim, and Cheal Wung Huh. 2021. "Endoscopic Vacuum Therapy in Patients with Transmural Defects of the Upper Gastrointestinal Tract: A Systematic Review with Meta-Analysis" Journal of Clinical Medicine 10, no. 11: 2346. https://doi.org/10.3390/jcm10112346
APA StyleJung, D. H., Yun, H.-R., Lee, S. J., Kim, N. W., & Huh, C. W. (2021). Endoscopic Vacuum Therapy in Patients with Transmural Defects of the Upper Gastrointestinal Tract: A Systematic Review with Meta-Analysis. Journal of Clinical Medicine, 10(11), 2346. https://doi.org/10.3390/jcm10112346