
ST-Segment Elevation Acute Myocardial Infarction Complicated by Cardiogenic Shock: Early Predictors of Very Long-Term Mortality


 , , ,
, , ,  ,
, 
Abstract
1. Introduction
2. Methods
2.1. Study Population
2.2. Study Protocol
2.3. Statistical Analysis
3. Results
3.1. Primary Endpoint
3.2. Secondary Endpoints
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Goldberg, R.J.; Samad, N.A.; Yarzebski, J.; Gurwitz, J.; Bigelow, C.; Gore, J.M. Temporal trends in cardiogenic shock complicating acute myocardial infarction—incidence and mortality from a community wide perspective 1975–1988. N. Engl. J. Med. 1999, 340, 1162–1168. [Google Scholar] [CrossRef] [PubMed]
- Bahit, M.C.; Lopes, R.D.; Clare, R.M.; Newby, L.K.; Pieper, K.S.; Van de Werf, F.; Armstrong, P.W.; Mahaffey, K.W.; Harrington, R.A.; Diaz, R.; et al. Heart failure complicating non-ST-segment elevation acute coronary syndrome: Timing, predictors, and clinical outcomes. JACC Heart Fail. 2013, 1, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Hochman, J.S.; Sleeper, L.A.; Webb, J.G.; Sanborn, T.A.; White, H.D.; Talley, J.D.; Buller, C.E.; Jacobs, A.K.; Slater, J.N.; Col, J.; et al. Early revascularization in acute myocardial infarction complicated by cardiogenic shock. N. Engl. J. Med. 1999, 341, 625–634. [Google Scholar] [CrossRef]
- Levine, G.N.; Bates, E.R.; Blankenship, J.C.; Bailey, S.R.; Bittl, J.A.; Cercek, B.; Chambers, C.E.; Ellis, S.G.; Guyton, R.A.; Hollenberg, S.M.; et al. 2015 ACC/AHA/SCAI Focused update on primary percutaneous coronary intervention for patients with ST-elevation myocardial infarction: An update of the 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention and the 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Circulation 2016, 133, 1135–1147. [Google Scholar]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 32, 119–177. [Google Scholar]
- Hashmi, K.A.; Abbas, K.; Hashmi, A.A.; Irfan, M.; Edhi, M.M.; Ali, N.; Khan, A. In-hospital mortality of patients with cardiogenic shock after acute myocardial infarction; impact of early revascularization. BMC Res. Notes 2018, 11, 721. [Google Scholar] [CrossRef]
- Shah, A.H.; Puri, R.; Kalra, A. Management of cardiogenic shock complicating acute myocardial infarction: A review. Clin. Cardiol. 2019, 42, 484–493. [Google Scholar] [CrossRef] [PubMed]
- Shah, P.; Cowger, J.A. Cardiogenic shock. Crit. Care Clin. 2014, 30, 391–412. [Google Scholar] [CrossRef]
- Taniguchi, Y.; Sakakura, K.; Adachi, Y.; Akashi, N.; Watanabe, Y.; Noguchi, M.; Yamamoto, K.; Ugata, Y.; Wada, H.; Momomura, S.I.; et al. In-hospital outcomes of acute myocardial infarction with cardiogenic shock caused by right coronary artery occlusion vs. left coronary artery occlusion. Cardiovasc. Interv. Ther. 2018, 33, 338–344. [Google Scholar] [CrossRef]
- Desta, L.; Jernberg, T.; Löfman, I.; Hofman-Bang, C.; Hagerman, I.; Spaak, J.; Persson, H. Incidence, temporal trends, and prognostic impact of heart failure complicating acute myocardial infarction: The SWEDEHEART Registry (Swedish Web-System for Enhancement and Development of Evidence-Based Care in Heart Disease Evaluated According to Recommended Therapies): A study of 199,851 patients admitted with index acute myocardial infarctions, 1996 to 2008. JACC Heart Fail. 2015, 3, 234–242. [Google Scholar]
- Hemradj, V.V.; Ottervanger, J.P.; van’t Hof, A.W.; Dambrink, J.H.; Gosselink, M.; Kedhi, E.; Suryapranata, H.; Zwolle Myocardial Infarction Study Group. Cardiogenic shock predicts long-term mortality in hospital survivors of STEMI treated with primary percutaneous coronary intervention. Clin. Cardiol. 2016, 39, 665–669. [Google Scholar] [CrossRef]
- Doost Hosseiny, A.; Moloi, S.; Chandrasekhar, J.; Farshid, A. Mortality pattern and cause of death in a long-term follow-up of patients with STEMI treated with primary PCI. Open Heart 2016, 3, e000405. [Google Scholar] [CrossRef]
- Spyridopoulos, I.; Noman, A.; Ahmed, J.M.; Das, R.; Edwards, R.; Purcell, I.; Bagnall, A.; Zaman, A.; Egred, M. Shock-index as a novel predictor of long-term outcome following primary percutaneous coronary intervention. Eur. Heart J. Acute Cardiovasc. Care 2015, 4, 270–277. [Google Scholar] [CrossRef] [PubMed]
- Kawaji, T.; Shiomi, H.; Morimoto, T.; Furukawa, Y.; Nakagawa, Y.; Kadota, K.; Ando, K.; Mizoguchi, T.; Abe, M.; Takahashi, M.; et al. CREDO-Kyoto AMI investigators. Long-term clinical outcomes in patients with ST-segment elevation acute myocardial infarction complicated by cardiogenic shock due to acute pump failure. Eur. Heart J. Acute Cardiovasc. Care 2018, 7, 743–754. [Google Scholar] [CrossRef]
- Hochman, J.S.; Sleeper, L.A.; Webb, J.G.; Dzavik, V.; Buller, C.E.; Aylward, P.; Col, J.; White, H.D.; SHOCK Investigators. Early revascularization and long-term survival in cardiogenic shock complicating acute myocardial infarction. JAMA 2006, 295, 2511–2515. [Google Scholar] [CrossRef] [PubMed]
- Thiele, H.; Zeymer, U.; Thelemann, N.; Neumann, F.J.; Hausleiter, J.; Abdel-Wahab, M.; Meyer-Saraei, R.; Fuernau, G.; Eitel, I.; Hambrecht, R.; et al. Intraaortic balloon pump in cardiogenic shock complicating acute myocardial infarction: Long-term 6-year outcome of the randomized IABP-SHOCK II trial. Circulation 2019, 139, 395–403. [Google Scholar] [CrossRef]
- Kolte, D.; Khera, S.; Aronow, W.S.; Mujib, M.; Palaniswamy, C.; Sule, S.; Jain, D.; Gotsis, W.; Ahmed, A.; Frishman, W.H.; et al. Trends in incidence, management, and outcomes of cardiogenic shock complicating ST-elevation myocardial infarction in the United States. J. Am. Heart Assoc. 2014, 3, e000590. [Google Scholar] [CrossRef]
- Marenzi, G.; Cosentino, N.; Moltrasio, M.; Rubino, M.; Crimi, G.; Buratti, S.; Grazi, M.; Milazzo, V.; Somaschini, A.; Camporotondo, R.; et al. Acute kidney injury definition and in-hospital mortality in patients undergoing primary percutaneous coronary intervention for ST-segment elevation myocardial infarction. J. Am. Heart Assoc. 2016, 5, e003522. [Google Scholar] [CrossRef]
- Marenzi, G.; Assanelli, E.; Campodonico, J.; Lauri, G.; Marana, I.; De Metrio, M.; Moltrasio, M.; Grazi, M.; Rubino, M.; Veglia, F.; et al. Contrast volume during primary percutaneous coronary intervention and subsequent contrast-induced nephropathy and mortality. Ann. Intern Med. 2009, 150, 170–177. [Google Scholar] [CrossRef] [PubMed]
- Roques, F.; Michel, P.; Goldstone, A.R.; Nashef, S.A.M. The logistic Euro-SCORE. Eur. Heart J. 2003, 24, 1–2. [Google Scholar] [CrossRef]
- Goldberg, R.J.; Spencer, F.A.; Gore, J.M.; Lessard, D.; Yarzebski, J. Thirty-year trends (1975 to 2005) in the magnitude of, management of, and hospital death rates associated with cardiogenic shock in patients with acute myocardial infarction: A population-based perspective. Circulation 2009, 119, 1211–1219. [Google Scholar] [CrossRef] [PubMed]
- Aissaoui, N.; Puymirat, E.; Tabone, X.; Charbonnier, B.; Schiele, F.; Lefèvre, T.; Durand, E.; Blanchard, D.; Simon, T.; Cambou, J.P.; et al. Improved outcome of cardiogenic shock at the acute stage of myocardial infarction: A report from the USIK 1995, USIC 2000, and FAST-MI French Nationwide Registries. Eur. Heart J. 2012, 33, 2535–2543. [Google Scholar] [CrossRef]
- Pöss, J.; Köster, J.; Fuernau, G.; Eitel, I.; de Waha, S.; Ouarrak, T.; Lassus, J.; Harjola, V.P.; Zeymer, U.; Thiele, H.; et al. Risk stratification for patients in cardiogenic shock after acute myocardial infarction. J. Am. Coll. Cardiol. 2017, 69, 1913–1920. [Google Scholar] [CrossRef]
- Katz, J.N.; Stebbins, A.L.; Alexander, J.H.; Reynolds, H.R.; Pieper, K.S.; Ruzyllo, W.; Werdan, K.; Geppert, A.; Dzavik, V.; Van de Werf, F.; et al. Predictors of 30-day mortality in patients with refractory cardiogenic shock following acute myocardial infarction despite a patent infarct artery. Am. Heart J. 2009, 158, 680–687. [Google Scholar] [CrossRef]
- Sutton, A.G.; Finn, P.; Hall, J.A.; Harcombe, A.A.; Wright, R.A.; de Belder, M.A. Predictors of outcome after percutaneous treatment for cardiogenic shock. Heart 2005, 91, 339–344. [Google Scholar] [CrossRef] [PubMed]
- Isorni, M.A.; Aissaoui, N.; Angoulvant, D.; Bonello, L.; Lemesle, G.; Delmas, C.; Henry, P.; Schiele, F.; Ferrières, J.; Simon, T.; et al. Temporal trends in clinical characteristics and management according to sex in patients with cardiogenic shock after acute myocardial infarction: The FAST-MI programme. Arch. Cardiovasc. Dis. 2018, 111, 555–563. [Google Scholar] [CrossRef]
- Pocock, S.J.; Huo, Y.; Van de Werf, F.; Newsome, S.; Chin, C.T.; Vega, A.M.; Medina, J.; Bueno, H. Predicting two-year mortality from discharge after acute coronary syndrome: An internationally-based risk score. Eur. Heart J. Acute Cardiovasc. Care 2019, 8, 727–737. [Google Scholar] [CrossRef]
- Rossello, X.; Bueno, H.; Pocock, S.J.; Van de Werf, F.; Danchin, N.; Annemans, L.; Medina, J.; Zeymer, U. Predictors of all-cause mortality and ischemic events within and beyond 1 year after an acute coronary syndrome: Results from the EPICOR registry. Clin. Cardiol. 2019, 42, 111–119. [Google Scholar] [CrossRef]
- Tomassini, F.; Gagnor, A.; Migliardi, A.; Tizzani, E.; Infantino, V.; Giolitto, S.; Conte, M.R.; Lanza, G.A.; Gnavi, R.; Varbella, F. Cardiogenic shock complicating acute myocardial infarction in the elderly: Predictors of long-term survival. Catheter. Cardiovasc. Interv. 2011, 78, 505–511. [Google Scholar] [CrossRef]
- Marenzi, G.; Assanelli, E.; Campodonico, J.; De Metrio, M.; Lauri, G.; Marana, I.; Moltrasio, M.; Rubino, M.; Veglia, F.; Montorsi, P.; et al. Acute kidney injury in ST-segment elevation acute myocardial infarction complicated by cardiogenic shock at admission. Crit. Care Med. 2010, 38, 438–444. [Google Scholar] [CrossRef]
- García-García, C.; Oliveras, T.; El Ouaddi, N.; Rueda, F.; Serra, J.; Labata, C.; Ferrer, M.; Cediel, G.; Montero, S.; Martínez, M.J.; et al. Short- and Long-Term Mortality Trends in STEMI-Cardiogenic Shock over Three Decades (1989–2018): The Ruti-STEMI-Shock Registry. J. Clin. Med. 2020, 9, 2398. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Survivors (n = 184) | Nonsurvivors (n = 281) | p Value |
|---|---|---|---|
| Age (year) | 63 ± 12 | 72 ± 11 | <0.0001 |
| Men, n (%) | 144 (78%) | 194 (69%) | 0.03 |
| Body weight (kg) | 73 ± 13 | 71 ± 13 | 0.13 |
| Hypertension, n (%) | 90 (49%) | 172 (61%) | 0.01 |
| Diabetes mellitus, n (%) | 34 (18%) | 63 (22%) | 0.31 |
| Smoking, n (%) | 97 (53%) | 128 (46%) | 0.13 |
| Dyslipidemia, n (%) | 68 (37%) | 97 (35%) | 0.59 |
| Anterior MI, n (%) | 119 (65%) | 178 (63%) | 0.77 |
| Prior MI, n (%) | 27 (15%) | 55 (20%) | 0.17 |
| Prior CABG, n (%) | 6 (3%) | 12 (4%) | 0.58 |
| LVEF (%) | 37 ± 13 | 33 ± 12 | 0.003 |
| Time-to-reperfusion (hours) | 4.7 ± 3.8 | 5.2 ± 4.2 | 0.19 |
| Serum creatinine (mg/dL) | 1.15 ± 0.6 | 1.43 ± 0.8 | <0.0001 |
| eGFR (ml/min/1.73 m2) | 73 ± 23 | 58 ± 23 | <0.0001 |
| Serum glycemia (mg/dL) | 193 ± 94 | 226 ± 108 | 0.003 |
| Contrast volume (mL) | 235 ± 107 | 230 ± 116 | 0.64 |
| Contrast ratio | 0.73 ± 0.42 | 0.94 ± 0.78 | 0.002 |
| Contrast ratio > 1, n (%) | 21 (13%) | 75 (27%) | 0.001 |
| New-onset AF, n (%) | 29 (24%) | 93 (34%) | 0.003 |
| VF before admission, n (%) | 11 (6%) | 14 (5%) | 0.64 |
| AKI, n (%) | 26 (14%) | 115 (41%) | <0.0001 |
| Blood transfusions, n (%) | 29 (16%) | 61 (22%) | 0.11 |
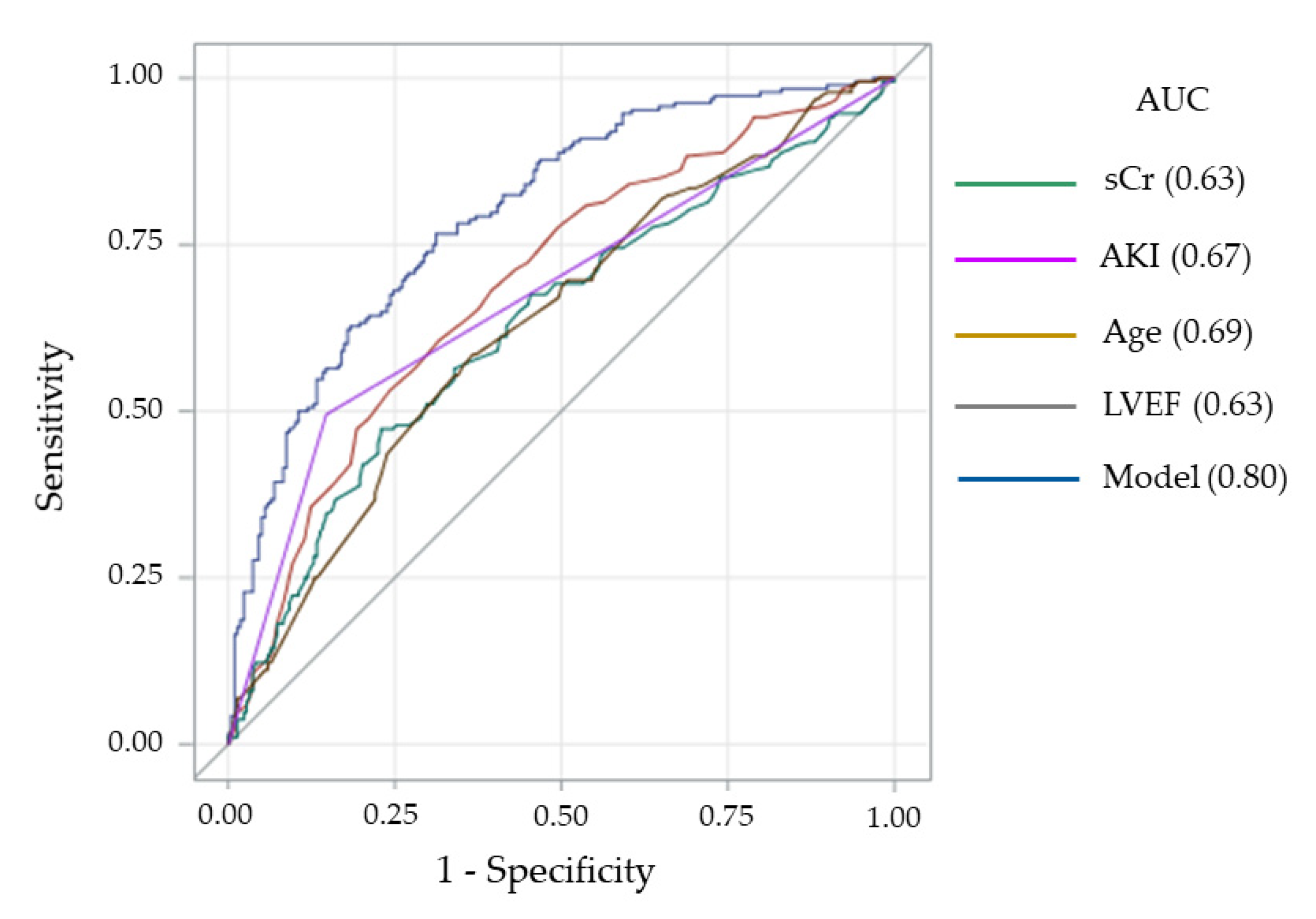
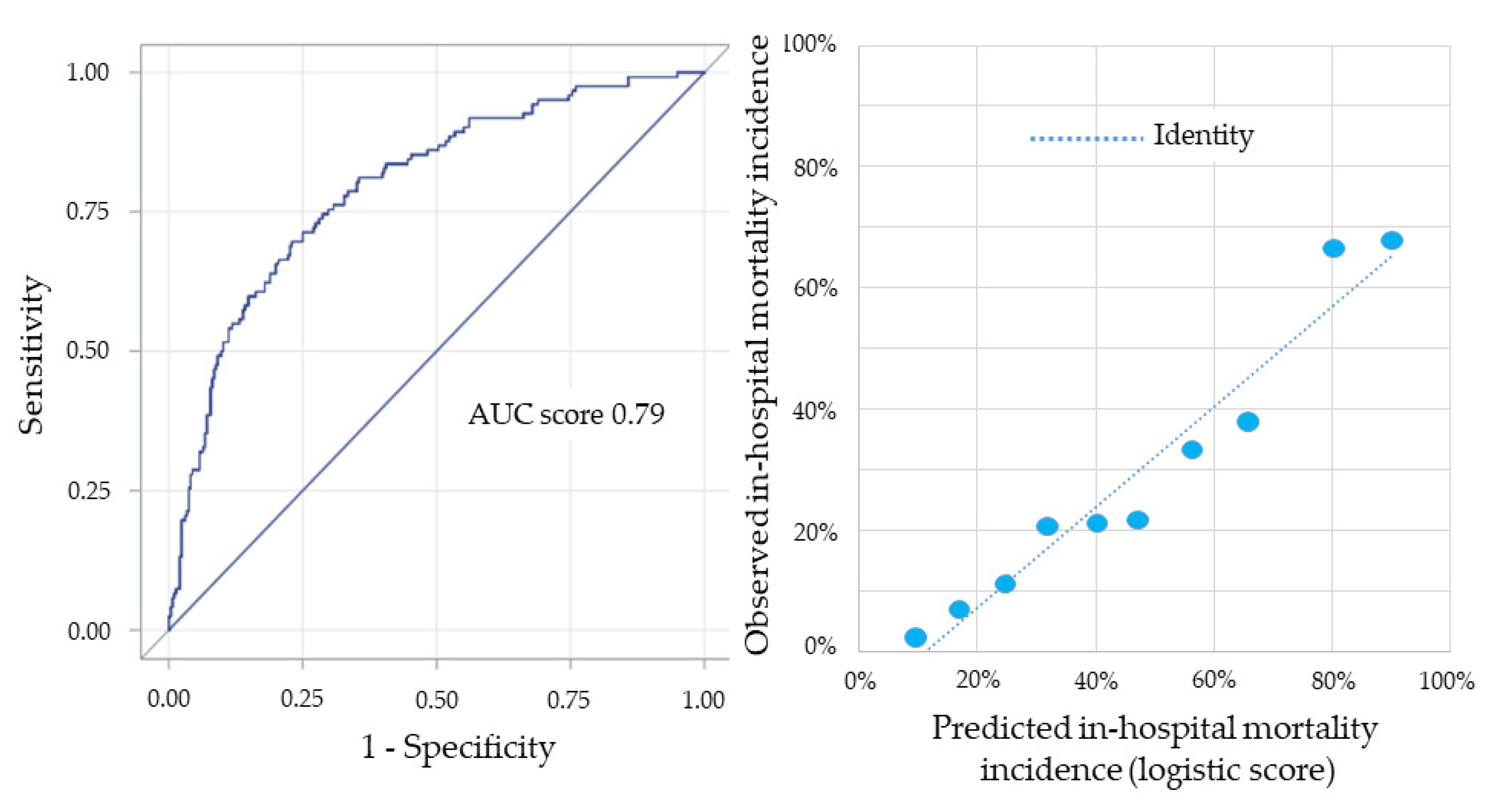
| Variables | β Coefficient |
|---|---|
| Age (years) (continuous) | 0.0431 |
| Left ventricular ejection fraction (%) (continuous) | −0.0359 |
| Serum creatinine (mg/dL) (continuous) | 0.2878 |
| Acute kidney injury (yes vs. no) | 0.6991 |
| Constant β0 | −3.6278 |
| First Author (Ref#) | Year of Publication | Study Acronym | Study Design | Study Population | Patient Treatment | Patients (n) | Follow-Up (years) | Mortality Rate (%) |
|---|---|---|---|---|---|---|---|---|
| Hochman [15] | 2006 | SHOCK | RCT | STEMI | Early PCI/CABG vs. medical stabilization | 302 | median 5.9 | 67% vs. 80% |
| Aissaoui [22] | 2012 | USIK 1995 USIC 2000 FAST-MI | Registries | STEMI/NSTEMI | PCI/TL/MT | 486 | 1 | 82% (USIK) 67% (USIC) 76% (FAST-MI) |
| Spyridopolous [13] | 2015 | - | Registry | STEMI | pPCI | 155 | median 1.2 | 46% |
| Doost Hosseiny [12] | 2016 | - | Registry | STEMI | pPCI | 92 | mean 3.5 | 59% |
| Hemradj [11] | 2016 | - | Registry | STEMI | pPCI | 387 | 1 | 30% |
| Kawaji [14] | 2018 | CREDO-KYOTO | Registry | STEMI | pPCI | 466 | 5 | 51% |
| Thiele [16] | 2018 | IABP-SHOCK II | RCT | STEMI/NSTEMI | PCI vs. PCI + IABP | 591 | median 6.2 | 66% vs. 67% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cosentino, N.; Resta, M.L.; Somaschini, A.; Campodonico, J.; D’Aleo, G.; Di Stefano, G.; Lucci, C.; Moltrasio, M.; Bonomi, A.; Cornara, S.; et al. ST-Segment Elevation Acute Myocardial Infarction Complicated by Cardiogenic Shock: Early Predictors of Very Long-Term Mortality. J. Clin. Med. 2021, 10, 2237. https://doi.org/10.3390/jcm10112237
Cosentino N, Resta ML, Somaschini A, Campodonico J, D’Aleo G, Di Stefano G, Lucci C, Moltrasio M, Bonomi A, Cornara S, et al. ST-Segment Elevation Acute Myocardial Infarction Complicated by Cardiogenic Shock: Early Predictors of Very Long-Term Mortality. Journal of Clinical Medicine. 2021; 10(11):2237. https://doi.org/10.3390/jcm10112237
Chicago/Turabian StyleCosentino, Nicola, Marta L. Resta, Alberto Somaschini, Jeness Campodonico, Giampaolo D’Aleo, Giovanni Di Stefano, Claudia Lucci, Marco Moltrasio, Alice Bonomi, Stefano Cornara, and et al. 2021. "ST-Segment Elevation Acute Myocardial Infarction Complicated by Cardiogenic Shock: Early Predictors of Very Long-Term Mortality" Journal of Clinical Medicine 10, no. 11: 2237. https://doi.org/10.3390/jcm10112237
APA StyleCosentino, N., Resta, M. L., Somaschini, A., Campodonico, J., D’Aleo, G., Di Stefano, G., Lucci, C., Moltrasio, M., Bonomi, A., Cornara, S., Demarchi, A., De Ferrari, G., Bartorelli, A. L., & Marenzi, G. (2021). ST-Segment Elevation Acute Myocardial Infarction Complicated by Cardiogenic Shock: Early Predictors of Very Long-Term Mortality. Journal of Clinical Medicine, 10(11), 2237. https://doi.org/10.3390/jcm10112237