
Clinical Manifestations of COVID-19 in the Feet: A Review of Reviews

 , , ,
, , ,
Abstract
1. Introduction
2. Methods
2.1. Eligibility Criteria
2.1.1. Inclusion Criteria
Case Study Design: Participants
Outcome Measures
Language
2.1.2. Exclusion Criteria
2.2. Research Methods for Identifying Other Studies
2.3. Data Collection, Analysis, and Extraction
2.4. Data Management
- First author and year of publication;
- Title;
- Type of review (systematic or narrative);
- Study designs (from studies included in the review, all of which were descriptive);
- Number of included studies (studies included in the review);
- Results: clinical manifestations in the feet of patients with COVID-19.
2.5. Quality Assessment Tools
3. Results
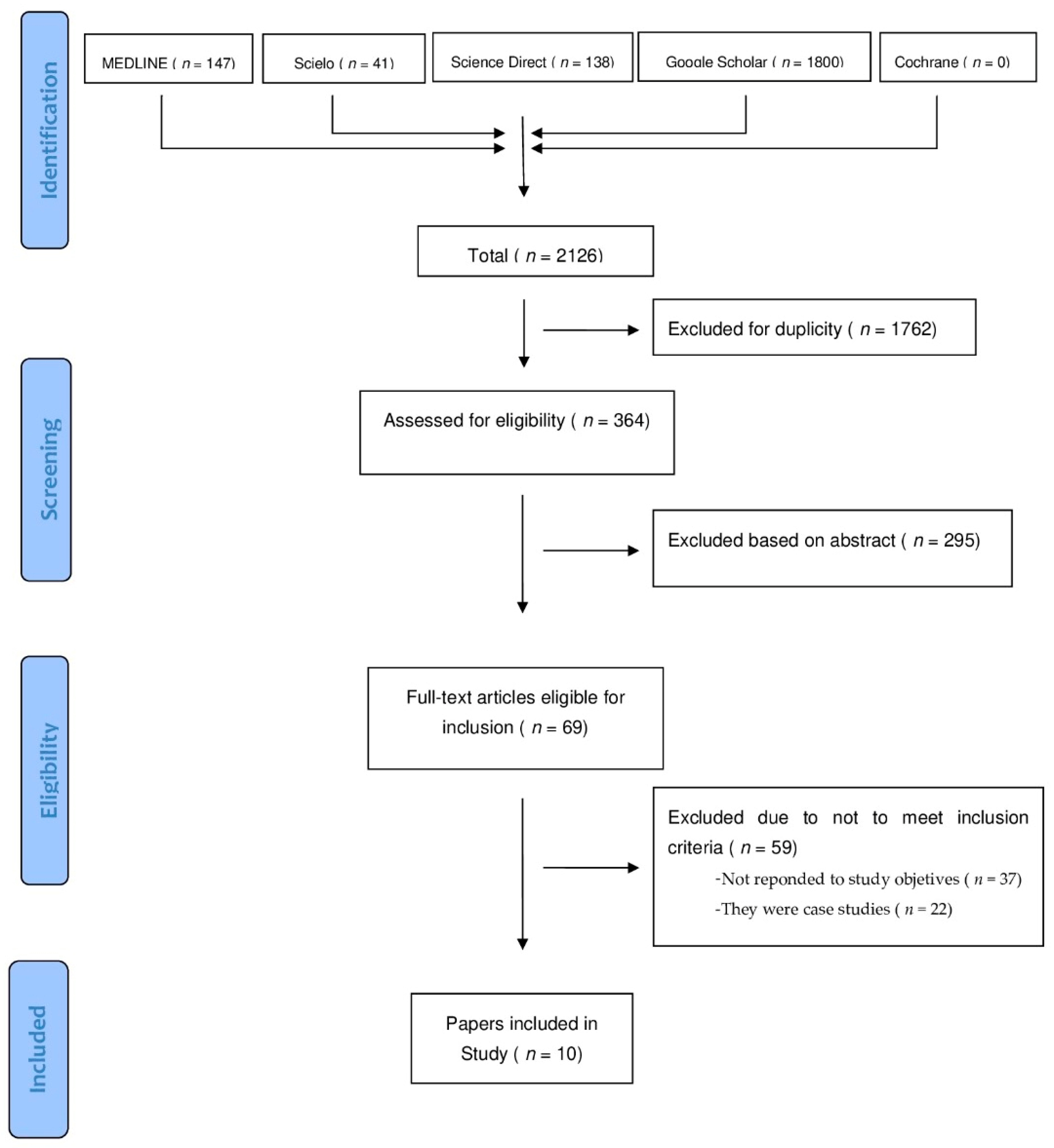
3.1. Review Selection
3.2. Methodological Quality
3.3. Characteristics of the Included Reviews
3.4. Clinical Manifestations of COVID-19 in the Foot
3.4.1. Integumentary System
3.4.2. Neurological System
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gane, S.B.C.; Kelly, C.; Hopkins, C. Isolated Sudden onset anosmia in COVID-19 infection. A novel syndrome? Rhinology 2020, 58, 299–301. [Google Scholar] [CrossRef]
- Recalcati, S.; Barbagallo, T.; Frasin, L.A.; Prestinari, F.; Cogliardi, A.; Provero, M.C.; Dainese, E.; Vanzati, A.; Fantini, F. Acral cutaneous lesions in the time of COVID-19. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e346–e347. [Google Scholar] [CrossRef]
- Chen, J.; Wu, L.; Zhang, J.; Zhang, L.; Gong, D.; Zhao, Y.; Chen, Q.; Huang, S.; Yang, M.; Yang, X.; et al. Deep learning-based model for detecting 2019 novel coronavirus pneumonia on high-resolution computed tomography. Sci. Rep. 2020, 10, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Chan, H.P.; Hadjiiski, L.M.; Samala, R.K. Computer-aided diagnosis in the era of deep learning. Med. Phys. 2020, 47, e218–e227. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.A.; Kim, Y. Cardiac arrhythmia disease classification using LSTM deep learning approach. CMC Comput. Mater. Contin. 2021, 67, 427–443. [Google Scholar]
- Morel Ayala, Z.; Buongermini, A.E.; Martínez de Cuéllar, C.; Zacur de Jiménez, M.; Ramírez Pastore, L.; Lezcano, M.C.; Greco, J.; Meza Brítez, R. Extra Pulmonary Manifestations of SARS-CoV-2 Infection in Pediatrics. Review. An. la Fac. Cienc. Médicas 2020, 53, 87–104. [Google Scholar] [CrossRef]
- Fundora, E.Z.; Carlos Junior, G.R.; Antonio, P.P. Repercusión en el sistema nervioso de pacientes infectados por COVID-19. In Proceedings of the Morfovirtual 2020, Catedra de Santiago Ramón y Cajal, Madrid, Spain, 11 November 2020. [Google Scholar]
- Benavides Reina, I.; López Medina, E.; López López, P. Diferencias entre niños y adultos por el nuevo coronavirus 2019, SARS-CoV-2/COVID-19. Rev. Latinoam. Infectol. Pediátrica 2020, 33, 165–173. [Google Scholar] [CrossRef]
- Garcia Molina, C. Manifestaciones cutáneas del COVID-19. NPunto 2020, III, 112–116. [Google Scholar]
- Fernandez-Nieto, D.; Jimenez-Cauhe, J.; Suarez-Valle, A.; Moreno-Arrones, O.M.; Saceda-Corralo, D.; Arana-Raja, A.; Ortega-Quijano, D. Characterization of acute acral skin lesions in nonhospitalized patients: A case series of 132 patients during the COVID-19 outbreak. J. Am. Acad. Dermatol. 2020, 83, e61–e63. [Google Scholar] [CrossRef] [PubMed]
- Nirenberg, M.S.; Herrera, M.D.M.R. Foot manifestations in a patient with COVID-19 and Epstein-Barr virus: A case study. Foot 2021, 46, 101707. [Google Scholar] [CrossRef]
- Landa, N.; Mendieta-Eckert, M.; Fonda-Pascual, P.; Aguirre, T. Chilblain-like lesions on feet and hands during the COVID-19 Pandemic. Int. J. Dermatol. 2020, 59, 739–743. [Google Scholar] [CrossRef]
- Aghazadeh, N.; Homayouni, M.; Sartori-Valinotti, J.C. Oral vesicles and acral erythema: Report of a cutaneous manifestation of COVID-19. Int. J. Dermatol. 2020, 59, 1153–1154. [Google Scholar] [CrossRef] [PubMed]
- Estébanez, A.; Pérez-Santiago, L.; Silva, E.; Guillen-Climent, S.; García- Vázquez, A.; Ramón, M.D. Cutaneous manifestations in COVID-19: A new contribution. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e250–e251. [Google Scholar] [CrossRef] [PubMed]
- Gagliardi, I.; Patella, G.; Michael, A.; Serra, R.; Provenzano, M.; Andreucci, M. COVID-19 and the Kidney: From Epidemiology to Clinical Practice. J. Clin. Med. 2020, 9, 2506. [Google Scholar] [CrossRef]
- Giavedoni, P.; Podlipnik, S.; Pericàs, J.M.; Fuertes de Vega, I.; García-Herrera, A.; Alós, L.; Carrera, C.; Andreu-Febrer, C.; Sanz-Beltran, J.; Riquelme-Mc Loughlin, C.; et al. Skin Manifestations in COVID-19: Prevalence and Relationship with Disease Severity. J. Clin. Med. 2020, 9, 3261. [Google Scholar] [CrossRef] [PubMed]
- Kolivras, A.; Dehavay, F.; Delplace, D.; Feoli, F.; Meiers, I.; Milone, L.; Olemans, C.; Sass, U.; Theunis, A.; Thompson, C.T.; et al. Coronavirus (COVID-19) infection–induced chilblains: A case report with histopathologic findings. JAAD Case Rep. 2020, 6, 489–492. [Google Scholar] [CrossRef]
- Garduño-Soto, M.; Choreño-Parra, J.A.; Cazarin-Barrientos, J. Dermatological aspects of SARS-CoV-2 infection: Mechanisms and manifestations. Arch. Dermatol. Res. 2020, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Carrascosa, J.M.; Morillas, V.; Bielsa, I.; Munera-Campos, M. Cutaneous Manifestations in the Context of SARS-CoV-2 Infection (COVID-19). Actas Dermosifiliogr. 2020, 111, 734–742. [Google Scholar] [CrossRef]
- Carod-Artal, F.J. Neurological complications of coronavirus and COVID-19. Rev. Neurol. 2020, 70, 311–322. [Google Scholar]
- Black, J.; Cuddigan, J. Skin manifestations with COVID-19: The purple skin and toes that you are seeing may not be deep tissue pressure injury. WCET J. 2020, 40, 18–22. [Google Scholar] [CrossRef]
- Ramani, S.L.; Samet, J.; Franz, C.K.; Hsieh, C.; Nguyen, C.V.; Horbinski, C.; Deshmukh, S. Musculoskeletal involvement of COVID-19: Review of imaging. Skelet. Radiol. 2021, 1–11. [Google Scholar] [CrossRef]
- Shea, B.J.; Grimshaw, J.M.; Wells, G.A.; Boers, M.; Andersson, N.; Hamel, C.; Porter, A.C.; Tugwell, P.; Moher, D.; Bouter, L.M. Development of AMSTAR: A measurement tool to assess the methodological quality of systematic reviews. BMC Med. Res. Methodol. 2007, 7, 1–7. [Google Scholar] [CrossRef]
- Shea, B.J.; Hamel, C.; Wells, G.A.; Bouter, L.M.; Kristjansson, E.; Grimshaw, J.; Henry, D.A.; Boers, M. AMSTAR is a reliable and valid measurement tool to assess the methodological quality of systematic reviews. J. Clin. Epidemiol. 2009, 62, 1013–1020. [Google Scholar] [CrossRef] [PubMed]
- González González, F.; Cortés Correa, C.; Peñaranda Contretas, E. Manifestaciones cutáneas en pacientes con COVID-19: Características clínicas y mecanismos fisiopatológicos postulados. Ann. Oncol. 2020, 7, 19–21. [Google Scholar]
- Jia, J.L.; Kamceva, M.; Rao, S.A.; Linos, E. Cutaneous manifestations of COVID-19: A preliminary review. J. Am. Acad. Dermatol. 2020, 83, 687–690. [Google Scholar] [CrossRef]
- Santos, B.S.D.; Santos, F.S.D.; Ribeiro, E.R. Clinical-Epidemiological Relation between Sars-Cov-2 and Kawasaki Disease: An Integrative Literature. Rev. Paul. Pediatr. 2021, 39, e2020217. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, M.; Long, B. Dermatologic manifestations and complications of COVID-19. Am. J. Emerg. Med. 2020, 38, 1715–1721. [Google Scholar] [CrossRef]
- Yamamoto, L.; Dos Santos, E.H.; Pinto, L.S.; Rocha, M.C.; Kanunfre, K.A.; Vallada, M.G.; Okay, T.S. SARS-CoV-2 infections with emphasis on pediatric patients: A narrative review. Rev. Inst. Med. Trop. Sao Paulo 2020, 62, 1–12. [Google Scholar] [CrossRef]
- Trujillo Gittermann, L.M.; Valenzuela Feris, S.N.; von Oetinger Giacoman, A. Relation between COVID-19 and Guillain-Barré syndrome in adults. Systematic review. Neurologia 2020, 35, 646–654. [Google Scholar] [CrossRef] [PubMed]
- Ellul, M.A.; Benjamin, L.; Singh, B.; Lant, S.; Michael, B.D.; Easton, A.; Kneen, R.; Defres, S.; Sejvar, J.; Solomon, T. Neurological associations of COVID-19. Lancet Neurol. 2020, 19, 767–783. [Google Scholar] [CrossRef]
- Gawronska, K.; Lorkowski, J. Falls as One of the Atypical Presentations of COVID-19 in Older Population. Geriatr. Orthop. Surg. Rehabil. 2021, 12, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Bristow, I.R. The mystery of the COVID toes-turning evidence-based medicine on its head. J. Foot Ankle Res. 2020, 13, 4–5. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Element | Inclusion Criteria |
|---|---|
| (P) Population | Adults and children with clinical manifestations on the foot due to COVID-19 |
| (E) Exposure | Exposed to COVID-19 |
| (O) Outcome | Signs and symptoms of COVID-19 in the foot; neurological, vascular, dermatological… |
| Database | Search String | N |
|---|---|---|
| PUBMED | (COVID-19 AND FOOT) AND LIMIT TO (HUMANS) AND LIMIT TO (SPANISH OR ENGLISH) AND LIMIT TO (NOT SURGERY) AND TITLE, ABSTRACT AND LIMIT TO (NO STUDY CASES) AND (REVIEW) | 147 |
| SCIELO | (COVID-19) AND (CLINICAL MANIFESTATION) AND LIMIT TO (SPANISH OR ENGLISH) AND TITLE, ABSTRACT AND LIMIT TO (NO STUDY CASES) AND (REVIEW) | 41 |
| SCIENCE DIRECT | (COVID-19) AND (FOOT MANIFESTATION), AND LIMIT TO (NOT DIABETIC)) AND TITLE, ABSTRACT AND LIMIT TO (NO STUDY CASES) AND (REVIEW) | 138 |
| COCHRANE DATABASE SYSTEMATIC REVIEWS | (COVID-19) AND (SIGNS AND SYMPTOMS OR CLINICAL MANIFESTATION) AND (FOOT) AND LIMIT TO (LAST YEAR) | 0 |
| GOOGLE ACADEMIC | (COVID-19) AND (CLINICAL MANIFESTATIONS IN LOWER LIMBS) AND LIMIT TO (PUBLICATION YEAR FROM 2020), AND LIMIT TO (NO ANIMALS), AND LIMIT TO (NOT RESPIRATORY, NOT LUNG), AND TITLE, ABSTRACT AND LIMIT TO (NO STUDY CASES) AND (REVIEW) | 1800 |
| Review (Year) | Objective | Type of Review | Number of Final Studies Included | Year of Studies Included | Provides Search Terms | Language Restrictions | Quality Assessment | Synthesis of Evidence |
|---|---|---|---|---|---|---|---|---|
| Jia et al. (2020) [26] | Describe cutaneous symptoms associated with COVID-19 presentation | Preliminary review | 46 | 2020 | YES | YES | YES | Narrative and tabular |
| Santos et al. (2020) [27] | Analyze the current scientific literature to document in an integrative review the main findings that correlate Kawasaki disease (KD) to COVID-19 | Integrative literature review | 7 | 2020 | YES | NO | YES | Narrative |
| Morel-Ayala et al. (2020) [6] | Review of SARS-Cov-2 extrapulmonary manifestations | Literature review | Not specified | 2020 | YES | Not specified | Not specified | Narrative |
| Zayas-Fundora et al. (2020) [7] | Describe neurological complications caused by SARS-CoV-2 | Bibliographic review | 31 | 2020 | YES | YES | YES | Narrative |
| Benavides-Reina et al. (2020) [8] | Differences between children and adults with COVID-19, clinical manifestations (emphasizing multi-system post-inflammatory syndrome), diagnostic tests, and the role of children in community transmission of infection | Review | Not specified | 2020 | YES | Not specified | Not specified | Narrative |
| García-Molina et al. (2020) [9] | Provide an overview of skin manifestations in patients with COVID-19 | Bibliographic review | Not specified | 2020 | YES | YES | Not specified | Narrative and tabular |
| Gottlieb et al. (2020) [28] | Summarize dermatologic manifestations and complications associated with COVID-19 with an emphasis on emergency medicine clinicians | Literature review | 41 | 2020 | YES | Not specified | Not specified | Narrative |
| Yamamoto et al. (2020) [29] | Summarize the main aspects underlying the new coronavirus SARS-CoV-2 | Narrative review | Not specified | 2020 | YES | Not specified | Not specified | Narrative |
| Trujillo-Gittermann et al. (2020) [31] | Analyze the available evidence that associates Guillain-Barré syndrome with COVID-19 | Systematic review | 24 | 2020 | YES | Not specified | YES | Narrative and tabular |
| Lesion | Population | Appearance | Evolution | Prognosis | Prevalence |
|---|---|---|---|---|---|
| Foot edema associated with Kawasaki Disease [2,8] | Infancy | Early, 30 days before diagnosis of KD | - | - | 60.7% |
| Exanthem in the feet associated with Kawasaki Disease [2,8] | Infancy | Early, 30 days before diagnosis of KD | - | - | 55.6% |
| Skin rash associated with multisystem inflammatory syndrome [8] | Children and teenagers | After >3 days with fever | - | - | 56.3% |
| Chilblains or perniosis [1,6,10] | Young people | Late stage of the disease | Usually lasted 14 days | Good | 19% |
| Ischemia and distal necrosis [10] | Adults | - | - | Bad | 6% |
| Vesicular breakouts [1,6,10] | Adults, small percentage in children | Prior to other symptoms or early stages of the disease | 10 day duration | Bad | 9% |
| Urticarial lesions [1,6,10] | Children | Within 3 days of diagnosis and along with respiratory symptoms | Disappeared after 8 days | Bad | 19% |
| Maculopapular lesions [1] | - | Along with respiratory symptoms | Lasted 10–14 days | - | 22.7% |
| Papulosquamous breakouts [9] | Adults | - | - | - | 47% |
| Recurrent herpes [9] | Adults | - | - | - | - |
| Muscle weakness in lower limbs, paresis, areflexias, ataxia, and difficulty walking through COVID-associated Guillain-Barré Syndrome [7,10,11,12] | Adults (more common in 35–50 years of age) | 10–21 days after COVID-19 diagnosis | - | Bad | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jimenez-Cebrian, A.M.; Castro-Mendez, A.; García-Podadera, B.; Romero-Galisteo, R.; Medina-Alcántara, M.; Garcia-Paya, I.; Páez-Moguer, J.; Córdoba-Fernández, A. Clinical Manifestations of COVID-19 in the Feet: A Review of Reviews. J. Clin. Med. 2021, 10, 2201. https://doi.org/10.3390/jcm10102201
Jimenez-Cebrian AM, Castro-Mendez A, García-Podadera B, Romero-Galisteo R, Medina-Alcántara M, Garcia-Paya I, Páez-Moguer J, Córdoba-Fernández A. Clinical Manifestations of COVID-19 in the Feet: A Review of Reviews. Journal of Clinical Medicine. 2021; 10(10):2201. https://doi.org/10.3390/jcm10102201
Chicago/Turabian StyleJimenez-Cebrian, Ana Maria, Aurora Castro-Mendez, Blanca García-Podadera, Rita Romero-Galisteo, Miguel Medina-Alcántara, Irene Garcia-Paya, Joaquín Páez-Moguer, and Antonio Córdoba-Fernández. 2021. "Clinical Manifestations of COVID-19 in the Feet: A Review of Reviews" Journal of Clinical Medicine 10, no. 10: 2201. https://doi.org/10.3390/jcm10102201
APA StyleJimenez-Cebrian, A. M., Castro-Mendez, A., García-Podadera, B., Romero-Galisteo, R., Medina-Alcántara, M., Garcia-Paya, I., Páez-Moguer, J., & Córdoba-Fernández, A. (2021). Clinical Manifestations of COVID-19 in the Feet: A Review of Reviews. Journal of Clinical Medicine, 10(10), 2201. https://doi.org/10.3390/jcm10102201