
Fetal and Perinatal Outcome Following First and Second Trimester COVID-19 Infection: Evidence from a Prospective Cohort Study

 , and
, and 
Abstract
1. Introduction
2. Methods
2.1. Study Population
2.2. Data Collection
2.3. Follow up of SARS-CoV-2 Infected Pregnant Women
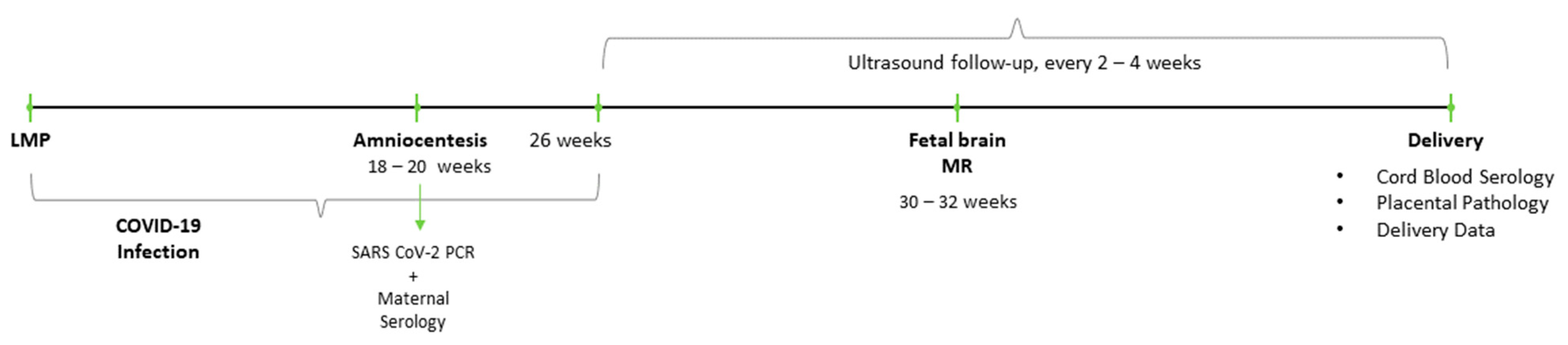
- Vertical transmission rates—all women in our cohort were offered amniocentesis for amniotic fluid RT-PCR test of SARS CoV-2 at the time of genetic amniocentesis. Those who opted for the test, were tested for amniotic fluid SARS CoV-2 RT-PCR as well as maternal serum serology for SARS CoV-2 IgG and IgM.
- Fetal imaging throughout pregnancy—women were followed with serial ultrasound investigations looking for sonographic evidence of fetal disease secondary to viral infection from the time of recruitment and every 4–6 weeks thereafter. To complete fetal brain evaluation, we offered a fetal brain magnetic resonance (MR) study at 30–32 weeks gestation.
- Delivery and newborn data were collected from medical charts or by telephone survey. Small for gestational age (SGA) was defined as birthweight <10th percentile. When possible, we collected umbilical cord blood and tested for SARS CoV-2 IgG and IgM antibodies.
2.4. Serology
2.5. Statistical Analysis
3. Results
3.1. Vertical Transmission Rates
3.2. Fetal Imaging Findings Along Pregnancy
3.3. Obstetric Outcome and Neonatal Data
4. Discussion
4.1. Main Findings
- No evidence of vertical SARS-COV-2 transmission was found upon amniotic fluid PCR testing or cord blood serology at delivery.
- No evidence of adverse fetal effects was found on serial ultrasound anatomy scans, fetal growth as well as a few cases of fetal brain MR imaging.
- No increased rates of obstetric complications were found. Deliveries occurred at term and newborns were appropriate for gestational age. Neonatal outcome was overall reassuring.
- There was no significant difference for the above outcome measures when comparing first to second trimester infections.
4.2. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. 2020. Available online: https://covid19.who.int/ (accessed on 3 March 2021).
- Siston, A.M.; Rasmussen, S.A.; Honein, M.A.; Fry, A.M.; Seib, K.; Callaghan, W.M.; Louie, J.; Doyle, T.J.; Crockett, M.; Lynfield, R.; et al. Pandemic 2009 influenza A(H1N1) virus illness among pregnant women in the United States. JAMA 2010, 303, 1517–1525. [Google Scholar] [CrossRef] [PubMed]
- Moore, C.A.; Staples, J.E.; Dobyns, W.B.; Pessoa, A.; Ventura, C.V.; Da Fonseca, E.B.; Ribeiro, E.M.; Ventura, L.O.; Neto, N.N.; Arena, J.F.; et al. Characterizing the Pattern of Anomalies in Congenital Zika Syndrome for Pediatric Clinicians. JAMA Pediatr. 2017, 171, 288–295. [Google Scholar] [CrossRef] [PubMed]
- Zambrano, L.D.; Ellington, S.; Strid, P.; Galang, R.R.; Oduyebo, T.; Tong, V.T.; Woodworth, K.R.; Nahabedian III, J.F.; Azziz-Baumgartner, E.; Gilboa, S.M.; et al. Update: Characteristics of symptomatic women of reproductive age with laboratory-confirmed SARS-CoV-2 infection by pregnancy status-United States, January 22-October 3, 2020. CDC Morb. Mortal. Wkly. Rep. 2020, 69, 1641–1647. [Google Scholar] [CrossRef] [PubMed]
- Allotey, J.; Stallings, E.; Bonet, M.; Yap, M.; Chatterjee, S.; Kew, T.; Debenham, L.; Llavall, A.C.; Dixit, A.; Zhou, D.; et al. Clinical manifestations, risk factors, and maternal and perinatal outcomes of coronavirus disease 2019 in pregnancy: Living systematic review and meta-analysis. BMJ 2020, 370, m3320. [Google Scholar] [CrossRef] [PubMed]
- Knight, M.; Bunch, K.; Vousden, N.; Morris, E.; Simpson, N.; Gale, C.; O’Brien, P.; Quigley, M.; Brocklehurst, P.; Kurinczuk, J.J. Characteristics and outcomes of pregnant women admitted to hospital with confirmed SARS-CoV-2infection in UK: National population cohort study. BMJ 2020, 8, 369. [Google Scholar]
- Fenizia, C.; Biasin, M.; Cetin, I.; Vergani, P.; Mileto, D.; Spinillo, A.; Gismondo, M.R.; Perotti, F.; Callegari, C.; Mancon, A.; et al. Analysis of SARS-CoV-2 vertical transmission during pregnancy. Nat. Commun. 2020, 11, 5128. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Guo, J.; Wang, C.; Luo, F.; Yu, X.; Zhang, W.; Li, J.; Zhao, D.; Xu, D.; Gong, Q.; et al. Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: A retrospective review of medical records. Lancet 2020, 395, 809–815. [Google Scholar] [CrossRef]
- Kotlyar, A.M.; Grechukhina, O.; Chen, A.; Popkhadze, S.; Grimshaw, A.; Tal, O.; Taylor, H.S.; Tal, R. Vertical transmission of coronavirus disease 2019: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2021, 224, 35–53.e3. [Google Scholar] [CrossRef] [PubMed]
- Pediatrics AAP. FAQs: Management of Infants Born to Mothers with Suspected or Confirmed COVID-19; Pediatrics AAP: Itasca, IL, USA, 2020. [Google Scholar]
- Cosma, S.; Carosso, A.R.; Cusato, J.; Borella, F.; Carosso, M.; Bovetti, M.; Filippini, C.; D’Avolio, A.; Ghisetti, V.; Di Perri, G.; et al. Coronavirus disease 2019 and first-trimester spontaneous abortion: A case-control study of 225 pregnant patients. Am. J. Obstet. Gynecol. 2021, 224, 391.e1–391.e7. [Google Scholar] [CrossRef] [PubMed]
- Indenbaum, V.; Koren, R.; Katz-Likvornik, S.; Yitzchaki, M.; Halpern, O.; Regev-Yochay, G.; Cohen, C.; Biber, A.; Feferman, T.; Cohen Saban, N.; et al. Testing IgG antibodies against the RBD of SARS-CoV-2 is sufficient and necessary for COVID-19 diagnosis. PLoS ONE 2020, 15, e0241164. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. National Institutes of Health. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 25 January 2021).
- WAPM (World Association of Perinatal Medicine) Working Group on COVID-19. Maternal and perinatal outcomes of pregnant women with SARS-CoV-2 infection. Ultrasound Obstet. Gynecol. 2021, 57, 232–241. [Google Scholar] [CrossRef] [PubMed]
- Goh, X.L.; Low, Y.F.; Ng, C.H.; Amin, Z.; Ng, Y.P.M. Incidence of SARS-CoV-2 vertical transmission: A meta-analysis. Arch. Dis. Child. Fetal Neonatal Ed. 2021, 106, 112–113. [Google Scholar] [CrossRef] [PubMed]
- Zeng, L.; Xia, S.; Yuan, W.; Yan, K.; Xiao, F.; Shao, J.; Zhou, W. Neonatal Early-Onset Infection with SARS-CoV-2 in 33 Neonates Born to Mothers with COVID-19 in Wuhan, China. JAMA Pediatr. 2020, 174, 722–725. [Google Scholar] [CrossRef] [PubMed]
- Di Mascio, D.; Sen, C.; Saccone, G.; Galindo, A.; Grünebaum, A.; Yoshimatsu, J.; Stanojevic, M.; Kurjak, A.; Chervenak, F.; Suárez, M.J.R.; et al. Risk factors associated with adverse fetal outcomes in pregnancies affected by Coronavirus disease 2019 (COVID-19): A secondary analysis of the WAPM study on COVID-19. J. Perinat Med. 2020, 48, 950–958. [Google Scholar] [CrossRef] [PubMed]
- Vivanti, A.J.; Vauloup-Fellous, C.; Prevot, S.; Zupan, V.; Suffee, C.; Do Cao, J.; Benachi, A.; De Luca, D. Transplacental transmission of SARS-CoV-2 infection. Nat Commun. 2020, 11, 3572. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Evaluation and Management Considerations for Neonates at Risk for COVID-19. 8 December 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/caring-for-newborns.html (accessed on 20 February 2021).


{kind=link}
| Variable | Overall (n = 55) | First Trimester Infection (n = 28) | Second Trimester Infection (n = 27) | p-Value |
|---|---|---|---|---|
| Age (year mean ± SD) | 29.6 ± 6.2 | 28.9 ± 6.0 | 30.3 ± 6.4 | 0.30 |
| Gravity | 2 (1–5) | 2 (1.2–4) | 2.5 (1–5) | 0.52 |
| Parity | 1 (0–3) | 1 (0–2.7) | 1 (0–3.2) | 0.70 |
| Singleton | 51 (92.7) | 24 (85.7) | 27 (100) | 0.04 |
| BMI | 23.6 ± 4.1 | 22.1 ± 2.1 | 24.9 ± 5.1 | <0.01 |
| 19–25 | 23 (71.9) | 15 (93.8) | 8 (50.0) | <0.01 |
| 25–30 | 6 (18.8) | 1 (6.3) | 5 (31.3) | 0.07 |
| Gestational week at infection (avg) | 14.2 ± 6.7 | 8.4 ± 3.3 | 20.1 ± 3.2 | <0.01 |
| Severity of symptoms | ||||
| Asymptomatic | 5 (9.6) | 1 (3.8) | 4 (15.4) | 0.16 |
| Mild | 42 (80.8) | 23 (88.5) | 19 (73.1) | 0.16 |
| Moderate | 4 (7.7) | 2 (7.7) | 2 (7.7) | 1.00 |
| Severe | 1 (1.9) | 0 | 1 (3.8) | 0.31 |
| Length of illness (days) | 17.8 ± 13.5 | 15.6 ± 11.7 | 20.4 ± 15.2 | 0.28 |
| Symptoms | ||||
| Fever | 16 (31.4) | 7 (28.0) | 9 (34.6) | 0.61 |
| Shortness of breath | 6 (11.5) | 1 (3.8) | 5 (19.2) | 0.08 |
| Cough | 14 (26.9) | 5 (19.2) | 9 (34.6) | 0.21 |
| Fatigue | 27 (51.9) | 15 (57.7) | 12 (46.2) | 0.41 |
| Anorexia | 3 (6.3) | 2 (8.3) | 1 (4.2) | 0.55 |
| Loss of smell/taste | 29 (55.8) | 17 (65.4) | 12 (46.2) | 0.16 |
| Myalgia | 14 (26.9) | 6 (23.1) | 8 (30.8) | 0.53 |
| Headache | 15 (29.4) | 11 (44.0) | 4 (15.4) | 0.02 |
| Hospitalization | 6 (11.1) | 4 (14.8) | 2 (7.4) | 0.39 |
| Investigation | Number of Patients | Results | |
|---|---|---|---|
| Positive Findings | Negative Findings | ||
| Amniocentesis | |||
| Amniotic fluid COVID-19 PCR | 22 | 0 | 22 |
| Fetal Brain MRI | 5 | 0 | 5 |
| Fetal anomaly scans | 38 | 8 Ɨ | 30 |
| Cord blood at delivery | |||
| IgM | 4 | 0 | |
| IgG | 4 | 3 | |
| Overall | First Trimester COVID (n = 7) | Second Trimester COVID (n = 22) | p-Value | |
|---|---|---|---|---|
| Perinatal survival | 29 (100) | 7 (100) | 22 (100) | 1.00 |
| Gestational week at delivery | 38.6 ± 3.0 | 39.3 ± 1.6 | 38.3 ± 3.3 | 0.67 |
| Preterm birth | 1 (3.4) | 0 (0) | 1 (4.3) | |
| Mode of delivery | ||||
| Vaginal | 24 (82.8) | 6 (85.7) | 18 (81.8) | 1.00 |
| Operative | 2 (6.9) | 1 (14.3) | 1 (4.5) | 0.43 |
| Cesarean Section | 3 (10.3) | 0 | 3 (13.6) | 0.56 |
| Labor induction | 6 (21.4) | 0 | 6 (28.6) | 0.29 |
| Birthweight | 3260 ± 411 | 3132 ± 449 | 3301 ± 400 | 0.69 |
| Apgar | ||||
| 1 min | 9 (9–9) | 9 (9–9) | 9 (9–9) | 1.00 |
| 5 min | 10 (10–10) | 10 (10–10) | 10 (10–10) | 1.00 |
| Arterial pH | ||||
| Post-Partum Complication | ||||
| PPH | 1 (3.4) | 0 | 1 (4.5) | 1.00 |
| Fever | 3 (10.3) | 1 (14.3) | 2 (9.1) | 1.00 |
| Thromboembolic event | 1 (3.6) | 0 | 1 (4.8) | 1.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rosen, H.; Bart, Y.; Zlatkin, R.; Ben-Sira, L.; Ben Bashat, D.; Amit, S.; Cohen, C.; Regev-Yochay, G.; Yinon, Y. Fetal and Perinatal Outcome Following First and Second Trimester COVID-19 Infection: Evidence from a Prospective Cohort Study. J. Clin. Med. 2021, 10, 2152. https://doi.org/10.3390/jcm10102152
Rosen H, Bart Y, Zlatkin R, Ben-Sira L, Ben Bashat D, Amit S, Cohen C, Regev-Yochay G, Yinon Y. Fetal and Perinatal Outcome Following First and Second Trimester COVID-19 Infection: Evidence from a Prospective Cohort Study. Journal of Clinical Medicine. 2021; 10(10):2152. https://doi.org/10.3390/jcm10102152
Chicago/Turabian StyleRosen, Hadar, Yossi Bart, Rita Zlatkin, Liat Ben-Sira, Dafna Ben Bashat, Sharon Amit, Carmit Cohen, Gili Regev-Yochay, and Yoav Yinon. 2021. "Fetal and Perinatal Outcome Following First and Second Trimester COVID-19 Infection: Evidence from a Prospective Cohort Study" Journal of Clinical Medicine 10, no. 10: 2152. https://doi.org/10.3390/jcm10102152
APA StyleRosen, H., Bart, Y., Zlatkin, R., Ben-Sira, L., Ben Bashat, D., Amit, S., Cohen, C., Regev-Yochay, G., & Yinon, Y. (2021). Fetal and Perinatal Outcome Following First and Second Trimester COVID-19 Infection: Evidence from a Prospective Cohort Study. Journal of Clinical Medicine, 10(10), 2152. https://doi.org/10.3390/jcm10102152