
Extended Precordial T Wave Inversions Are Associated with Right Ventricular Enlargement and Poor Prognosis in Pulmonary Hypertension

 , , , ,
, , , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Clinical Assessment
2.3. Cardiac Catheterization
2.4. Cardiovascular Magnetic Resonance Imaging
2.5. Electrocardiography
2.6. Follow-Up
2.7. Statistical Analysis
3. Results
3.1. Characteristics of the Study Sample
3.2. T Wave Inversions
3.3. Comparison of Patients with and without TWI Range Improvement in Follow-Up
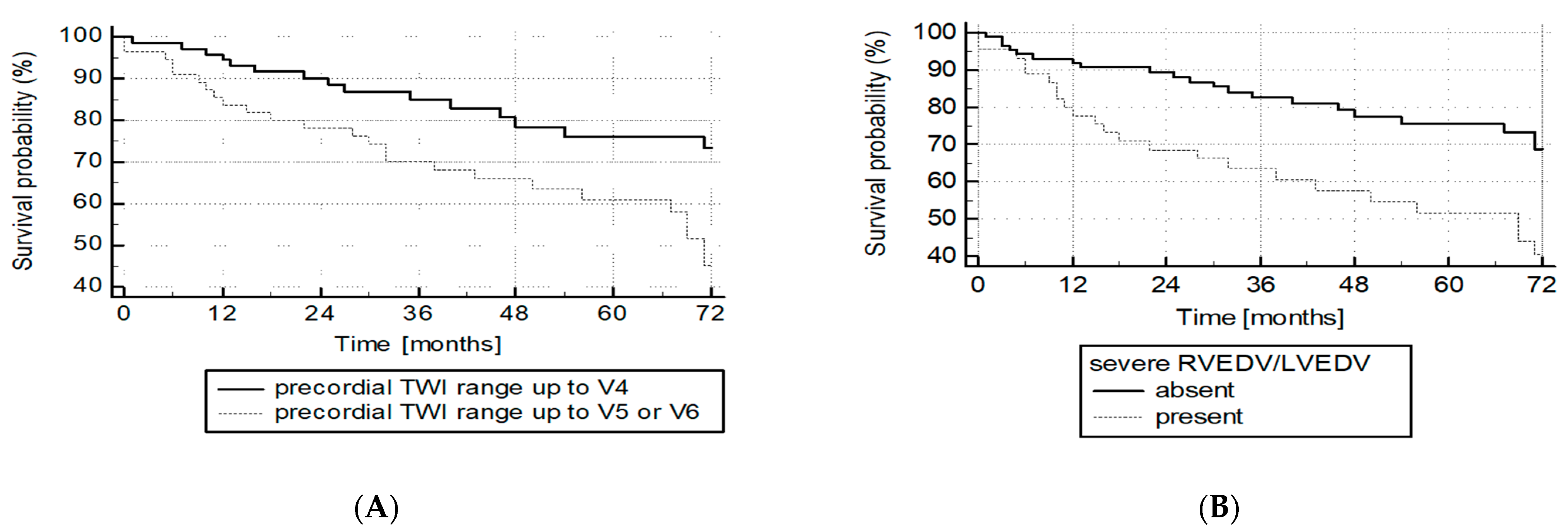
3.4. Follow-Up
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Waligóra, M.; Tyrka, A.; Podolec, P.; Kopeć, G. ECG Markers of Hemodynamic Improvement in Patients with Pulmonary Hypertension. BioMed Res. Int. 2018, 2018, 4606053. [Google Scholar] [CrossRef]
- Kopeć, G.; Tyrka, A.; Miszalski-Jamka, T.; Sobień, M.; Waligóra, M.; Brózda, M.; Podolec, P. Electrocardiogram for the diagnosis of right ventricular hypertrophy and dilation in idiopathic pulmonary arterial hypertension. Circ. J. 2012, 76, 1744–1749. [Google Scholar] [CrossRef]
- Bossone, E.; Paciocco, G.; Iarussi, D.; Agretto, A.; Iacono, A.; Gillespie, B.W.; Rubenfire, M. The prognostic role of the ECG in primary pulmonary hypertension. Chest 2002, 121, 513–518. [Google Scholar] [CrossRef] [PubMed]
- Waligóra, M.; Kopeć, G.; Jonas, K.; Tyrka, A.; Sarnecka, A.; Miszalski-Jamka, T.; Urbańczyk-Zawadzka, M.; Podolec, P. Mechanism and prognostic role of qR in V1 in patients with pulmonary arterial hypertension. J. Electrocardiol. 2017, 50, 476–483. [Google Scholar] [CrossRef] [PubMed]
- Altmayer, S.P.L.; Joyce Han, Q.; Addetia, K.; Patel, A.R.; Forfia, P.R.; Han, Y. Using all-cause mortality to define severe RV dilation with RV/LV volume ratio. Sci. Rep. 2018, 8, 7200. [Google Scholar] [CrossRef]
- Rautaharju, P.M.; Surawicz, B.; Gettes, L.S. AHA/ACCF/HRS Recommendations for the Standardization and Interpretation of the Electrocardiogram. Part IV: The ST Segment, T and U Waves, and the QT Interval A Scientific Statement From the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society. J. Am. Coll. Cardiol. 2009, 53, 982–991. [Google Scholar]
- Bonderman, D.; Wexberg, P.; Martischnig, A.M.; Heinzl, H.; Lang, M.B.; Sadushi, R.; Skoro-Sajer, N.; Lang, I.M. A noninvasive algorithm to exclude pre-capillary pulmonary hypertension. Eur. Respir. J. 2011, 37, 1096–1103. [Google Scholar] [CrossRef] [PubMed]
- Okin, P.M.; Devereux, R.B.; Nieminen, M.S.; Jern, S.; Oikarinen, L.; Viitasalo, M.; Toivonen, L.; Kjeldsen, S.E.; Julius, S.; Dahlöf, B. Relationship of the electrocardiographic strain pattern to left ventricular structure and function in hypertensive patients: The LIFE study. J. Am. Coll. Cardiol. 2001, 38, 514–520. [Google Scholar] [CrossRef]
- Bang, C.N.; Devereux, R.B.; Okin, P.M. Regression of electrocardiographic left ventricular hypertrophy strain is associated with lower incidence of cardiovascular morbidity and mortality in hypertensive patients independent of blood pressure reduction—A LIFE review. J. Electrocardiol. 2014, 47, 630–635. [Google Scholar] [CrossRef]
- Xin, D.; Zheng, W.; Xuyu, J.; Yuemin, S.; Wenjuan, Z.; Bo, B.; Xuefang, Y.; Canliang, H. Changes of the electrocardiographic strain pattern in patients with aortic stenosis and its underlying mechanisms. Heart 2011, 97, A239–A240. [Google Scholar] [CrossRef][Green Version]
- Piłka, M.; Darocha, S.; Banaszkiewicz, M.; Florczyk, M.; Wieteska, M.; Dobosiewicz, A.; Mańczak, M.; Mańczak, R.; Pietrasik, A.; Pietura, R.; et al. The evolution of electrocardiographic signs of right ventricular overload after balloon pulmonary angioplasty in chronic thromboembolic pulmonary hypertension. Pol. Arch. Intern. Med. 2019, 129, 451–459. [Google Scholar] [CrossRef] [PubMed]
- Kopeć, G. Electrocardiography in pulmonary hypertension. Pol. Arch. Intern. Med. 2019, 129, 440–441. [Google Scholar] [CrossRef] [PubMed]
- Nishiyama, T.; Takatsuki, S.; Kawakami, T.; Katsumata, Y.; Kimura, T.; Kataoka, M.; Tsuruta, H.; Itabashi, Y.; Murata, M.; Yuasa, S.; et al. Improvement in the electrocardiograms associated with right ventricular hypertrophy after balloon pulmonary angioplasty in chronic thromboembolic pulmonary hypertension. IJC Heart Vasc. 2018, 19, 75–82. [Google Scholar] [CrossRef]
- Sato, S.; Ogawa, A.; Matsubara, H. Changes in R wave in lead V1 predicts the survival of patients with pulmonary arterial hypertension. Pulm. Circ. 2018, 8, 2045894018776496. [Google Scholar] [CrossRef] [PubMed]
- Tonelli, A.R.; Baumgartner, M.; Alkukhun, L.; Minai, O.A.; Dweik, R.A. Electrocardiography at diagnosis and close to the time of death in pulmonary arterial hypertension. Ann. Noninvasive Electrocardiol. 2014, 19, 258–265. [Google Scholar] [CrossRef]
- van Wolferen, S.A.; Marcus, J.T.; Boonstra, A.; Marques, K.M.J.; Bronzwaer, J.G.F.; Spreeuwenberg, M.D.; Postmus, P.E.; Vonk-Noordegraaf, A. Prognostic value of right ventricular mass, volume, and function in idiopathic pulmonary arterial hypertension. Eur. Heart J. 2007, 28, 1250–1257. [Google Scholar] [CrossRef]
- Baggen, V.J.M.; Leiner, T.; Post, M.C.; van Dijk, A.P.; Roos-Hesselink, J.W.; Boersma, E.; Habets, J.; Sieswerda, G.T. Cardiac magnetic resonance findings predicting mortality in patients with pulmonary arterial hypertension: A systematic review and meta-analysis. Eur. Radiol. 2016, 26, 3771–3780. [Google Scholar] [CrossRef]
- Badagliacca, R.; Poscia, R.; Pezzuto, B.; Papa, S.; Pesce, F.; Manzi, G.; Giannetta, E.; Raineri, C.; Schina, M.; Sciomer, S.; et al. Right ventricular concentric hypertrophy and clinical worsening in idiopathic pulmonary arterial hypertension. J. Heart Lung Transplant. 2016, 35, 1321–1329. [Google Scholar] [CrossRef]
- Brewis, M.J.; Bellofiore, A.; Vanderpool, R.R.; Chesler, N.C.; Johnson, M.K.; Naeije, R.; Peacock, A.J. Imaging right ventricular function to predict outcome in pulmonary arterial hypertension. Int. J. Cardiol. 2016, 218, 206–211. [Google Scholar] [CrossRef]
- Kopeć, G.; Moertl, D.; Miszalski-Jamka, T.; Waligóra, M.; Tyrka, A.; Sarnecka, A.; Podolec, P. Left ventricular mass is preserved in patients with idiopathic pulmonary arterial hypertension and eisenmenger’s syndrome. Heart Lung Circ. 2014, 23, 454–461. [Google Scholar] [CrossRef]
- Kopeć, G.; Kurzyna, M.; Mroczek, E.; Chrzanowski, Ł.; Mularek-Kubzdela, T.; Skoczylas, I.; Kuśmierczyk, B.; Pruszczyk, P.; Błaszczak, P.; Lewicka, E.; et al. Characterization of Patients with Pulmonary Arterial Hypertension: Data from the Polish Registry of Pulmonary Hypertension (BNP-PL). J. Clin. Med. 2020, 9, 173. [Google Scholar] [CrossRef] [PubMed]
- Kopeć, G.; Dzikowska-Diduch, O.; Mroczek, E.; Mularek-Kubzdela, T.; Chrzanowski, Ł.; Skoczylas, I.; Tomaszewski, M.; Peregud-Pogorzelska, M.; Karasek, D.; Lewicka, E.; et al. Characteristics and outcomes of patients with chronic thromboembolic pulmonary hypertension in the era of modern therapeutic approaches: Data from the Polish multicenter registry (BNP-PL). Ther. Adv. Chronic Dis. 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Kopeć, G.; Kurzyna, M.; Mroczek, E.; Chrzanowski, Ł.; Mularek-Kubzdela, T.; Skoczylas, I.; Kuśmierczyk, B.; Pruszczyk, P.; Błaszczak, P.; Lewicka, E.; et al. Database of pulmonary hypertension in the Polish population (BNP--PL): Design of the registry. Kardiol. Pol. 2019, 77, 972–974. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n | 133 |
|---|---|
| Etiology: | |
| PAH (n (%)) | 77 |
| IPAH (n (%)) | 64 (48.1%) |
| CTD-APAH (n (%)) | 13 (9.8%) |
| CTEPH (n (%)) | 56 (42.1%) |
| Concomitant diseases: | |
| CAD with prior PCI (n (%)) | 4 (3%) |
| Arterial hypertension (n (%)) | 43 (32.3%) |
| Diabetes (n (%)) | 11 (8.3%) |
| COPD (n (%)) | 4 (3%) |
| Thyroid gland disease (n (%)) | 21 (15.8%) |
| Sex, female (n (%)) | 86 (64.7%) |
| Age (years) | 54.7 ± 15.6 |
| Weight (kg) | 72.2 ± 17 |
| WHO FC: | |
| I | 0 |
| II | 18 (13.5%) |
| III | 97 (72.9%) |
| IV | 18 (13.5%) |
| Newly diagnosed (“incident cases”) (n (%)) | 113 (85%) |
| NT-proBNP (pg/mL) | 2539 ± 3167 |
| 6 MWD (m) | 337.5 ± 117.4 |
| ECG: | |
| Heart rate (bpm) | 77.6 ± 14 |
| RHC: | |
| mPAP (mmHg) | 48.1 ± 14.3 |
| RAP (mmHg) | 6.1 ± 4.6 |
| Systolic blood pressure (mmHg) | 127 ± 21.3 |
| Diastolic blood pressure (mmHg) | 77.8 ± 17.2 |
| CO (L/min) | 3.3 ± 1.4 |
| CI (L/min/m2) | 1.8 ± 0.7 |
| Peripheral blood SpO2 (%) | 92.2 ± 5.3 |
| MVB SpO2 (%) | 59.7 ± 9.7 |
| PVR (WU) | 12.1 ± 6.1 |
| cMR: | |
| LVm (g) | 96.4 ± 28.7 |
| LVEDV (mL) | 105 ± 42.8 |
| LVEF (%) | 61.8 ± 9.5 |
| RVEDV (mL) | 200 ± 75 |
| RVm (g) | 57.3 ± 32.4 |
| RVEF (%) | 37.2 ± 11.7 |
| RAA (cm2) | 30.9 ± 9.4 |
| R Coefficient for Comparison with Listed Variable and Precordial TWI Range | p | |
|---|---|---|
| Clinical variables | ||
| Age (years) | −0.04 | 0.69 |
| NT-proBNP (pg/mL) | 0.46 | <0.0001 |
| 6 MWD (m) | −0.37 | 0.0001 |
| cMR variables | ||
| RVEDV (mL) | 0.44 | <0.0001 |
| RVm (g) | 0.43 | <0.0001 |
| (g/mL) | 0.09 | 0.34 |
| RVEF (%) | −0.61 | <0.0001 |
| LVEDV (mL) | 0.35 | 0.0001 |
| LVm (g) | −0.07 | 0.4 |
| LVEF (%) | −0.19 | 0.03 |
| 0.68 | <0.0001 | |
| RAA (cm2) | 0.42 | <0.0001 |
| Hemodynamic variables | ||
| mPAP (mmHg) | 0.42 | <0.0001 |
| PVR (WU) | 0.48 | <0.0001 |
| CI (L/min/m2) | −0.26 | 0.004 |
| RAP (mmHg) | 0.27 | 0.002 |
| Patients with No Improvement in Precordial TWI Range (n = 20) | Patients with Improvement in Precordial TWI Range (n = 18) | p | |
|---|---|---|---|
| Clinical and ECG characteristics | |||
| Baseline WHO FC | 3.05 ± 0.22 | 2.94 ± 0.42 | 0.33 |
| Δ WHO FC | −0.33 ± 0.7 | −0.61 ± 0.85 | 0.27 |
| Baseline NT-proBNP (pg/mL) | 1812 ± 1664 | 2407 ± 2483 | 0.4 |
| Δ NT-proBNP (pg/mL) | −714 ± 1112 | −2202 ± 2198 | 0.01 |
| Baseline 6 MWD (m) | 358 ± 110 | 316 ± 81.7 | 0.21 |
| Δ 6 MWD (m) | +51.4 ± 58.9 | + 77.9 ± 68.2 | 0.22 |
| cMR | |||
| Baseline RVEF (%) | 35.9 ± 12.1 | 39.2 ± 9.4 | 0.35 |
| Δ RVEF (%) | +4.8 ± 9.4 | +10.2 ± 13.5 | 0.25 |
| Baseline RVEDV (mL) | 188.1 ± 58.2 | 182 ± 53.1 | 0.74 |
| Δ RVEDV (mL) | +10.9 ± 41 | −40.9 ± 37.4 | <0.0001 |
| Baseline RVm (g) | 52.8 ± 18.2 | 50.4 ± 26.9 | 0.75 |
| Δ RVm (g) | −3.1 ± 19 | −15.1 ± 27.8 | 0.17 |
| Baseline LVEDV (mL) | 95.1 ± 35.8 | 95.2 ± 26.1 | 0.99 |
| Δ LVEDV (mL) | +2.5 ± 18.3 | +29.6 ± 26.6 | 0.005 |
| 2.16 ± 0.87 | 1.97 ± 0.52 | ||
| 0 ± 0.55 | −0.8 ± 0.46 | <0.0001 | |
| Baseline RAA (cm2) | 31.3 ± 13.6 | 29 ± 13.6 | 0.53 |
| Δ RAA (cm2) | +0.3 ± 5.2 | −4.8 ± 7.5 | 0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Waligóra, M.; Gliniak, M.; Bylica, J.; Pasieka, P.; Łączak, P.; Podolec, P.; Kopeć, G. Extended Precordial T Wave Inversions Are Associated with Right Ventricular Enlargement and Poor Prognosis in Pulmonary Hypertension. J. Clin. Med. 2021, 10, 2147. https://doi.org/10.3390/jcm10102147
Waligóra M, Gliniak M, Bylica J, Pasieka P, Łączak P, Podolec P, Kopeć G. Extended Precordial T Wave Inversions Are Associated with Right Ventricular Enlargement and Poor Prognosis in Pulmonary Hypertension. Journal of Clinical Medicine. 2021; 10(10):2147. https://doi.org/10.3390/jcm10102147
Chicago/Turabian StyleWaligóra, Marcin, Matylda Gliniak, Jan Bylica, Paweł Pasieka, Patrycja Łączak, Piotr Podolec, and Grzegorz Kopeć. 2021. "Extended Precordial T Wave Inversions Are Associated with Right Ventricular Enlargement and Poor Prognosis in Pulmonary Hypertension" Journal of Clinical Medicine 10, no. 10: 2147. https://doi.org/10.3390/jcm10102147
APA StyleWaligóra, M., Gliniak, M., Bylica, J., Pasieka, P., Łączak, P., Podolec, P., & Kopeć, G. (2021). Extended Precordial T Wave Inversions Are Associated with Right Ventricular Enlargement and Poor Prognosis in Pulmonary Hypertension. Journal of Clinical Medicine, 10(10), 2147. https://doi.org/10.3390/jcm10102147