
Microcirculation in Patients with Takotsubo Syndrome—The Prospective CIRCUS-TTS Study

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Study Protocol
2.3. Sidestream Dark-Field (SDF) Imaging
2.4. Statistical Analyses
3. Results
3.1. Baseline Clinical Characteristics
3.2. Assessment of Systemic Microcirculation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lyon, A.R.; Bossone, E.; Schneider, B.; Sechtem, U.; Citro, R.; Underwood, S.R.; Sheppard, M.N.; Figtree, G.N.; Parodi, G.; Akashi, Y.J.; et al. Current state of knowledge on Takotsubo syndrome: A Position Statement from the Taskforce on Takotsubo Syndrome of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2016, 18, 8–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stiermaier, T.; Möller, C.; Graf, T.; Eitel, C.; Desch, S.; Thiele, H.; Eitel, I. Prognostic Usefulness of the Ballooning Pattern in Patients with Takotsubo Cardiomyopathy. Am. J. Cardiol. 2016, 118, 1737–1741. [Google Scholar] [CrossRef] [PubMed]
- Stiermaier, T.; Santoro, F.; El-Battrawy, I.; Möller, C.; Graf, T.; Novo, G.; Santangelo, A.; Mariano, E.; Romeo, F.; Caldarola, P.; et al. Prevalence and Prognostic Impact of Diabetes in Takotsubo Syndrome: Insights from the International, Multicenter GEIST Registry. Diabetes Care 2018, 41, 1084–1088. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Möller, C.; Stiermaier, T.; Brabant, G.; Graf, T.; Thiele, H.; Eitel, I. Comprehensive assessment of sex hormones in Takotsubo syndrome. Int. J. Cardiol. 2018, 250, 11–15. [Google Scholar] [CrossRef]
- Eitel, I.; Moeller, C.; Munz, M.; Stiermaier, T.; Meitinger, T.; Thiele, H.; Erdmann, J. Genome-wide association study in takotsubo syndrome—Preliminary results and future directions. Int. J. Cardiol. 2017, 236, 335–339. [Google Scholar] [CrossRef]
- Ghadri, J.R.; Wittstein, I.S.; Prasad, A.; Sharkey, S.; Dote, K.; Akashi, Y.J.; Cammann, V.L.; Crea, F.; Galiuto, L.; Desmet, W.; et al. International Expert Consensus Document on Takotsubo Syndrome (Part I): Clinical Characteristics, Diagnostic Criteria, and Pathophysiology. Eur. Heart J. 2018, 39, 2032–2046. [Google Scholar] [CrossRef] [Green Version]
- Eitel, I.; Stiermaier, T.; Graf, T.; Möller, C.; Rommel, K.P.; Eitel, C.; Schuler, G.; Thiele, H.; Desch, S. Optical Coherence Tomography to Evaluate Plaque Burden and Morphology in Patients with Takotsubo Syndrome. J. Am. Heart Assoc. 2016, 5, e004474. [Google Scholar] [CrossRef]
- Vitale, C.; Rosano, G.M.; Kaski, J.C. Role of Coronary Microvascular Dysfunction in Takotsubo Cardiomyopathy. Circ. J. 2016, 80, 299–305. [Google Scholar] [CrossRef] [Green Version]
- Braunwald, E.; Kloner, R.A. The stunned myocardium: Prolonged, postischemic ventricular dysfunction. Circulation 1982, 66, 1146–1149. [Google Scholar] [CrossRef] [Green Version]
- Wittstein, I.S.; Thiemann, D.R.; Lima, J.A.; Baughman, K.L.; Schulman, S.P.; Gerstenblith, G.; Wu, K.C.; Rade, J.J.; Bivalacqua, T.J.; Champion, H.C. Neurohumoral features of myocardial stunning due to sudden emotional stress. N. Engl. J. Med. 2005, 352, 539–548. [Google Scholar] [CrossRef] [PubMed]
- Jaguszewski, M.; Osipova, J.; Ghadri, J.R.; Napp, L.C.; Widera, C.; Franke, J.; Fijalkowski, M.; Nowak, R.; Fijalkowska, M.; Volkmann, I.; et al. A signature of circulating microRNAs differentiates takotsubo cardiomyopathy from acute myocardial infarction. Eur. Heart J. 2014, 35, 999–1006. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D. ESC Scientific Document Group. Fourth universal definition of myocardial infarction (2018). Eur. Heart J. 2019, 40, 237–269. [Google Scholar] [CrossRef] [Green Version]
- Thiele, H.; Ohman, E.M.; Desch, S.; Eitel, I.; de Waha, S. Management of cardiogenic shock. Eur. Heart J. 2015, 36, 1223–1230. [Google Scholar] [CrossRef] [Green Version]
- Eitel, I.; von Knobelsdorff-Brenkenhoff, F.; Bernhardt, P.; Carbone, I.; Muellerleile, K.; Aldrovandi, A.; Francone, M.; Desch, S.; Gutberlet, M.; Strohm, O.; et al. Clinical characteristics and cardiovascular magnetic resonance findings in stress (takotsubo) cardiomyopathy. JAMA 2011, 306, 277–286. [Google Scholar] [CrossRef]
- Ince, C. The microcirculation is the motor of sepsis. Crit. Care 2005, 9 (Suppl. 4), S13–S19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vellinga, N.A.; Boerma, E.C.; Koopmans, M.; Donati, A.; Dubin, A.; Shapiro, N.I.; Pearse, R.M.; Machado, F.R.; Fries, M.; Akarsu-Ayazoglu, T.; et al. International study on microcirculatory shock occurrence in acutely ill patients. Crit. Care Med. 2015, 43, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Jung, C.; Fuernau, G.; de Waha, S.; Eitel, I.; Desch, S.; Schuler, G.; Figulla, H.R.; Thiele, H. Intraaortic balloon counterpulsation and microcirculation in cardiogenic shock complicating myocardial infarction: An IABP-SHOCK II substudy. Clin. Res. Cardiol. 2015, 104, 679–687. [Google Scholar] [CrossRef]
- Abdelmoneim, S.S.; Mankad, S.V.; Bernier, M.; Dhoble, A.; Hagen, M.E.; Ness, S.A.; Chandrasekaran, K.; Pellikka, P.A.; Oh, J.K.; Mulvagh, S.L. Microvascular function in Takotsubo cardiomyopathy with contrast echocardiography: Prospective evaluation and review of literature. J. Am. Soc. Echocardiogr. 2009, 22, 1249–1255. [Google Scholar] [CrossRef] [PubMed]
- Bybee, K.A.; Prasad, A.; Barsness, G.W.; Lerman, A.; Jaffe, A.S.; Murphy, J.G.; Wright, R.S.; Rihal, C.S. Clinical characteristics and thrombolysis in myocardial infarction frame counts in women with transient left ventricular apical ballooning syndrome. Am. J. Cardiol. 2004, 94, 343–346. [Google Scholar] [CrossRef] [PubMed]
- Meimoun, P.; Malaquin, D.; Sayah, S.; Benali, T.; Luycx-Bore, A.; Levy, F.; Zemir, H.; Tribouilloy, C. The coronary flow reserve is transiently impaired in tako-tsubo cardiomyopathy: A prospective study using serial Doppler transthoracic echocardiography. J. Am. Soc. Echocardiogr. 2008, 21, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.M.; Lerman, A.; Lennon, R.J.; Prasad, A. Impaired coronary microvascular reactivity in women with apical ballooning syndrome (Takotsubo/stress cardiomyopathy). Eur. Heart J. Acute Cardiovasc. Care 2013, 2, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Kume, T.; Akasaka, T.; Kawamoto, T.; Yoshitani, H.; Watanabe, N.; Neishi, Y.; Wada, N.; Yoshida, K. Assessment of coronary microcirculation in patients with takotsubo-like left ventricular dysfunction. Circ. J. 2005, 69, 934–939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galiuto, L.; De Caterina, A.R.; Porfidia, A.; Paraggio, L.; Barchetta, S.; Locorotondo, G.; Rebuzzi, A.G.; Crea, F. Reversible coronary microvascular dysfunction: A common pathogenetic mechanism in Apical Ballooning or Tako-Tsubo Syndrome. Eur. Heart J. 2010, 31, 1319–1327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- den Uil, C.A.; Lagrand, W.K.; van der Ent, M.; Jewbali, L.S.; Cheng, J.M.; Spronk, P.E.; Simoons, M.L. Impaired microcirculation predicts poor outcome of patients with acute myocardial infarction complicated by cardiogenic shock. Eur. Heart J. 2010, 31, 3032–3039. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lam, K.; Sjauw, K.D.; Henriques, J.P.; Ince, C.; de Mol, B.A. Improved microcirculation in patients with an acute ST-elevation myocardial infarction treated with the Impella LP2.5 percutaneous left ventricular assist device. Clin. Res. Cardiol. 2009, 98, 311–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dilken, O.; Ergin, B.; Ince, C. Assessment of sublingual microcirculation in critically ill patients: Consensus and debate. Ann. Transl. Med. 2020, 8, 793. [Google Scholar] [CrossRef]
- Madhavan, M.; Borlaug, B.A.; Lerman, A.; Rihal, C.S.; Prasad, A. Stress hormone and circulating biomarker profile of apical ballooning syndrome (Takotsubo cardiomyopathy): Insights into the clinical significance of B-type natriuretic peptide and troponin levels. Heart 2009, 95, 1436–1441. [Google Scholar] [CrossRef]
- Kume, T.; Kawamoto, T.; Okura, H.; Toyota, E.; Neishi, Y.; Watanabe, N.; Hayashida, A.; Okahashi, N.; Yoshimura, Y.; Saito, K.; et al. Local release of catecholamines from the hearts of patients with tako-tsubo-like left ventricular dysfunction. Circ. J. 2008, 72, 106–108. [Google Scholar] [CrossRef] [Green Version]
- Kanoore Edul, V.S.; Ince, C.; Dubin, A. What is microcirculatory shock? Curr. Opin. Crit. Care 2015, 21, 245–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Variable | TTS (n = 22) | MI (n = 20) | p | Control (n = 20) |
|---|---|---|---|---|
| Age, years, mean (SD) | 72.3 (12.5) | 66.1 (11.3) | 0.098 | 28.8 (6.6) |
| Female sex, n/N (%) | 17/22 (77) | 13/20 (65) | 0.499 | 12/20 (60) |
| Cardiovascular risk factors | ||||
| Hypertension, n/N (%) | 13/22 (59) | 14/20 (70) | 0.531 | - |
| Diabetes mellitus, n/N (%) | 0/22 (0) | 6/20 (30) | 0.007 | - |
| Hypercholesterolemia, n/N (%) | 2/22 (9) | 10/20 (50) | 0.006 | - |
| Current smoking, n/N (%) | 4/22 (18) | 10/20 (50) | 0.049 | - |
| Body mass index, kg/m2, mean (SD) | 23.3 (2.9) | 26.3 (3.7) | 0.007 | - |
| Days of hospitalization, median (IQR) | 9.5 (6.8; 11.0) | 4.0 (4.0; 8.3) | 0.001 | |
| Stressful event, n/N (%) | 11/22 (50) | - | - | |
| Emotional, n/N (%) | 7/22 (31.8) | - | - | - |
| Physical, n/N (%) | 6/22 (27.3) | - | - | - |
| Ballooning pattern | ||||
| Apical, n/N (%) | 14/22 (63.6) | - | - | - |
| Midventricular, n/N (%) | 7/22 (31.8) | - | - | - |
| Basal, n/N (%) | 1/22 (4.5) | - | - | - |
| Number of diseased vessels | ||||
| 1, n/N (%) | - | 6/20 (30.0) | - | - |
| 2, n/N (%) | - | 8/20 (40.0) | - | - |
| 3, n/N (%) | - | 6/20 (30.0) | - | - |
| Infarct related vessel | ||||
| Left anterior descending, n/N (%) | - | 12/20 (60.0) | - | - |
| Right coronary artery, n/N (%) | - | 6/20 (30.0) | - | - |
| Left circumflex, n/N (%) | - | 2/20 (10.0) | - | - |
| Initial LV ejection fraction, %, mean (SD) | 41.1 (10.4) | 49.8 (10.0) | 0.009 | - |
| Follow-up LV ejection fraction, %, mean (SD) | 58.2 (5.4) | 49.3 (9.3) | 0.002 | - |
| CK at admission, U/L, median (IQR) | 167.5 (79.5; 340.3) | 153.0 (97.0; 610.0) | 0.583 | - |
| Troponin T at admission, ng/L, median (IQR) | 216.0 (69.9; 618.5) | 193.0 (65.0; 1785.0) | 0.734 | - |
| Death during follow up, n/N (%) | 2/22 (9.1) | 0/20 (0.0) | 0.489 | - |
| Date | Variable | TTS (n = 22) | MI (n = 20) | Control (n = 20) | p |
|---|---|---|---|---|---|
| Day 1 | NC | 64.0 (60.3; 67.8) | 57.5 (54.8; 62.0) | 61.6 (54.8; 64.4) | 0.014 |
| PNC | 64.0 (57.3; 65.8) | 55.0 (53.0; 59.0) | 55.1 (50.9; 60.8) | 0.006 | |
| PPV (%) | 99.12 (94.98; 99.97) | 97.69 (93.16; 99.67) | 96.30 (85.74; 99.96) | 0.268 | |
| TVD (mm/mm2) | 9.15 (7.93; 11.38) | 7.42 (6.50; 10.04) | 8.08 (7.39; 10.36) | 0.134 | |
| PVD (mm/mm2) | 9.09 (7.79; 11.11) | 7.29 (6.32; 9.78) | 7.31 (7.08; 9.24) | 0.053 | |
| Day 3 | NC | 62.0 (59.8; 67.0) | 61.0 (57.0; 63.0) | 61.6 (54.8; 64.4) | 0.198 |
| PNC | 61.0 (58.0; 65;3) | 59.5 (56.5; 62.8) | 55.1 (50.9; 60.8) | 0.022 | |
| PPV (%) | 98.96 (95.08; 99.97) | 99.99 (99.91; 100.00) | 96.30 (85.74; 99.96) | 0.001 | |
| TVD (mm/mm2) | 8.80 (7.71; 10.42) | 8.84 (7.19; 10.49) | 8.08 (7.39; 10.36) | 0.700 | |
| PVD (mm/mm2) | 8.69 (7.28; 9.34) | 8.84 (7.17; 10.06) | 7.31 (7.08; 9.24) | 0.323 | |
| Day 5 | NC | 61.0 (60.5; 66.0) | 58.0 (51.5; 63.5) | 61.6 (54.8; 64.4) | 0.175 |
| PNC | 60.0 (57.0; 54.5) | 53.0 (47.0; 61.0) | 55.1 (50.9; 60.8) | 0.018 | |
| PPV (%) | 98.98 (94.02; 99.88) | 97.08 (84.92; 99.98) | 96.30 (85.74; 99.96) | 0.691 | |
| TVD (mm/mm2) | 9.39 (8.65; 10.84) | 7.67 (6.52; 9.86) | 8.08 (7.39; 10.36) | 0.052 | |
| PVD (mm/mm2) | 8.89 (8.33; 9.84) | 7.67 (5.77; 8.56) | 7.31 (7.08; 9.24) | 0.045 | |
| Follow-up | NC | 62.0 (56.5; 65.0) | 63.5 (57.8; 66.0) | 61.6 (54.8; 64.4) | 0.407 |
| PNC | 59.0 (52.0; 63.0) | 62.0 (56.8; 66.0) | 55.1 (50.9; 60.8) | 0.075 | |
| PPV (%) | 95.74 (89.87; 99.56) | 99.60 (97.88; 99.97) | 96.30 (85.74; 99.96) | 0.248 | |
| TVD (mm/mm2) | 8.29 (7.12; 10.79) | 9.00 (7.30; 9.90) | 8.08 (7.39; 10.36) | 0.813 | |
| PVD (mm/mm2) | 8.00 (6.84; 9.27) | 8.60 (6.94; 9.82) | 7.31 (7.08; 9.24) | 0.513 |
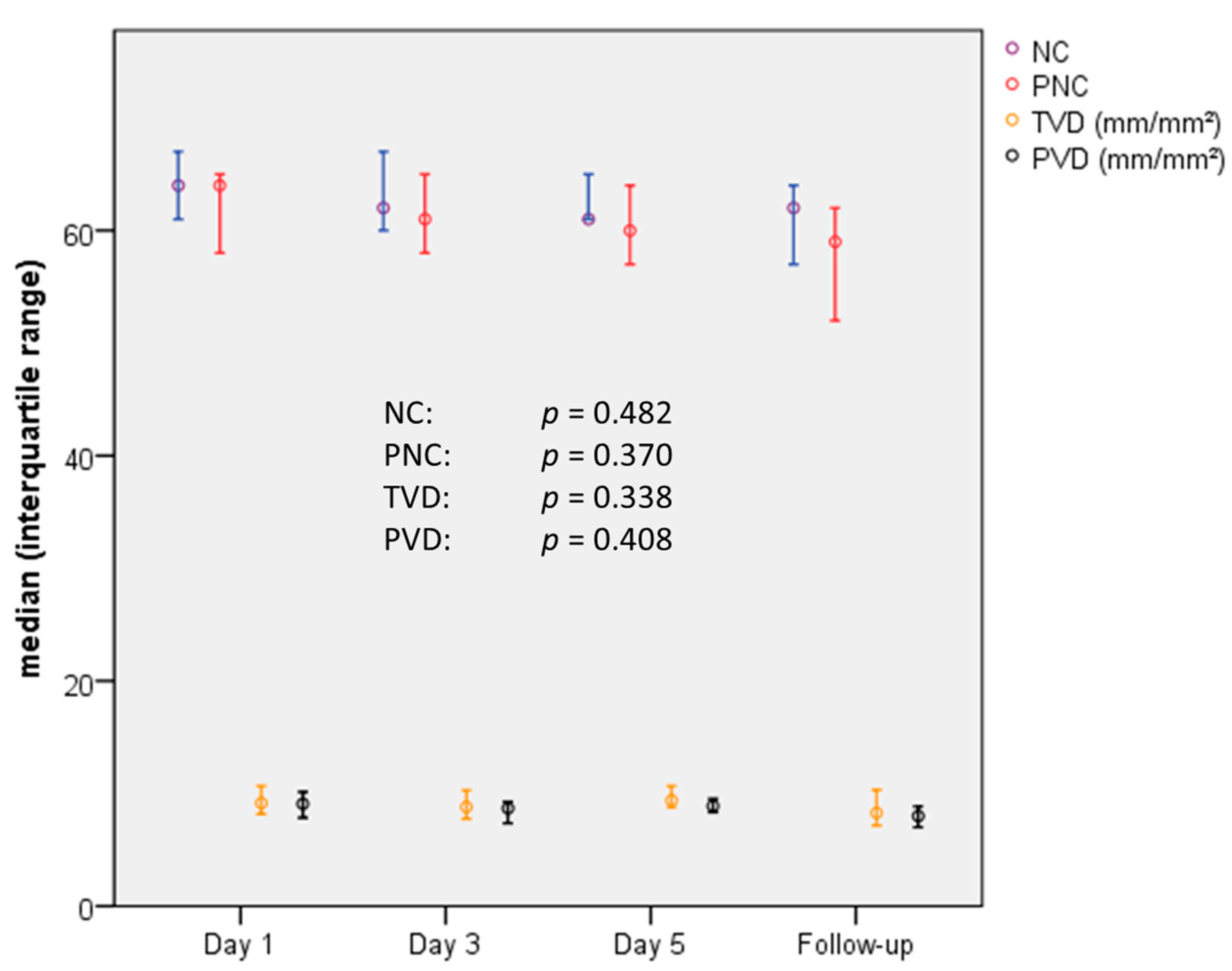
| Day 1 | Day 3 | Day 5 | FUP | p | |
|---|---|---|---|---|---|
| NC | 64.0 (60.3; 67.8) | 62.0 (59.8; 67.0) | 61.0 (60.5; 66.0) | 62.0 (56.5; 65.0) | 0.482 |
| PNC | 64.0 (57.3; 65.8) | 61.0 (58.0; 65;3) | 60.0 (57.0; 54.5) | 59.0 (52.0; 63.0) | 0.370 |
| PPV (%) | 99.12 (94.98; 99.97) | 98.96 (95.08; 99.97) | 98.98 (94.02; 99.88) | 95.74 (89.87; 99.56) | 0.507 |
| TVD (mm/mm2) | 9.15 (7.93; 11.38) | 8.80 (7.71; 10.42) | 9.39 (8.65; 10.84) | 8.29 (7.12; 10.79) | 0.338 |
| PVD (mm/mm2) | 9.09 (7.79; 11.11) | 8.69 (7.28; 9.34) | 8.89 (8.33; 9.84) | 8.00 (6.84; 9.27) | 0.408 |
| Day 1 | Day 3 | Day 5 | FUP | p | |
|---|---|---|---|---|---|
| NC | 57.5 (54.8; 62.0) | 61.0 (57.0; 63.0) | 58.0 (51.5; 63.5) | 63.5 (57.8; 66.0) | 0.095 |
| PNC | 55.0 (53.0; 59.0) | 59.5 (56.5; 62.8) | 53.0 (47.0; 61.0) | 62.0 (56.8; 66.0) | 0.054 |
| PPV (%) * | 97.69 (93.16; 99.67) | 99.99 (99.91; 100.00) | 97.08 (84.92; 99.98) | 99.60 (97.88; 99.97) | 0.008 |
| TVD (mm/mm2) | 7.42 (6.50; 10.04) | 8.84 (7.19; 10.49) | 7.67 (6.52; 9.86) | 9.00 (7.30; 9.90) | 0.738 |
| PVD (mm/mm2) | 7.29 (6.32; 9.78) | 8.84 (7.17; 10.06) | 7.67 (5.77; 8.56) | 8.60 (6.94; 9.82) | 0.459 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Möller, C.; Stiermaier, T.; Meusel, M.; Jung, C.; Graf, T.; Eitel, I. Microcirculation in Patients with Takotsubo Syndrome—The Prospective CIRCUS-TTS Study. J. Clin. Med. 2021, 10, 2127. https://doi.org/10.3390/jcm10102127
Möller C, Stiermaier T, Meusel M, Jung C, Graf T, Eitel I. Microcirculation in Patients with Takotsubo Syndrome—The Prospective CIRCUS-TTS Study. Journal of Clinical Medicine. 2021; 10(10):2127. https://doi.org/10.3390/jcm10102127
Chicago/Turabian StyleMöller, Christian, Thomas Stiermaier, Moritz Meusel, Christian Jung, Tobias Graf, and Ingo Eitel. 2021. "Microcirculation in Patients with Takotsubo Syndrome—The Prospective CIRCUS-TTS Study" Journal of Clinical Medicine 10, no. 10: 2127. https://doi.org/10.3390/jcm10102127
APA StyleMöller, C., Stiermaier, T., Meusel, M., Jung, C., Graf, T., & Eitel, I. (2021). Microcirculation in Patients with Takotsubo Syndrome—The Prospective CIRCUS-TTS Study. Journal of Clinical Medicine, 10(10), 2127. https://doi.org/10.3390/jcm10102127