
Validation of a Visual-Based Analytics Tool for Outcome Prediction in Polytrauma Patients (WATSON Trauma Pathway Explorer) and Comparison with the Predictive Values of TRISS


Abstract
:1. Introduction
- (i)
- to validate the WATSON Explorer in a different patient population;
- (ii)
- to expand the predictive capacity from mortality to clinical complications, such as SIRS and sepsis;
- (iii)
- to compare aspects of prediction with the TRISS methodology.
2. Methods
2.1. Inclusion/Exclusion Criteria
2.2. Definitions
2.3. Clinical Course
2.4. Statistics
2.5. Development of the Model and Validation
3. Results
3.1. General Characteristics
3.2. Model Performance
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mica, L.; Niggli, C.; Bak, P.; Yaeli, A.; McClain, M.; Lawrie, C.M.; Pape, H.C. Development of a Visual Analytics Tool for Polytrauma Patients: Proof of Concept for a New Assessment Tool Using a Multiple Layer Sankey Diagram in a Single-Center Database. World J. Surg. 2020, 44, 764–772. [Google Scholar] [CrossRef]
- Cameron, P. 30 years after the Major Trauma Outcome Study ( MTOS )—Benchmarking trauma Centre outcomes, the Challenge continues. Injury 2020, 51, 588–589. [Google Scholar] [CrossRef]
- Cuenca, A.G.; Maier, R.V.; Cuschieri, J.; Moore, E.E.; Moldawer, L.L.; Tompkins, R.G.; Scale, L. The Glue Grant experience: Characterizing the post injury genomic response. Eur. J. Trauma Emerg. Surg. 2011, 37, 549–558. [Google Scholar] [CrossRef]
- Icay, K.; Liu, C.; Hautaniemi, S. Dynamic visualization of multi-level molecular data: The Director package in R. Comput. Methods Programs Biomed. 2018, 153, 129–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G.M. Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): The TRIPOD Statement. BMC Med. 2015, 13, 214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker, S.P.; O’Neill, B.; Haddon, W.; Long, W.B. The injury severity score: A method for describing patients with multiple injuries and evaluating emergency care. J. Trauma 1974, 14, 187–196. [Google Scholar] [CrossRef]
- Bone, R.C.; Balk, R.A.; Cerra, F.B.; Dellinger, R.P.; Fein, A.M.; Knaus, W.A.; Schein, R.M.H.; Sibbald, W.J. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Chest 1992, 101, 1644–1655. [Google Scholar] [CrossRef] [Green Version]
- Dübendorfer, C.; Billeter, A.T.; Seifert, B.; Keel, M.; Turina, M. Serial lactate and admission SOFA scores in trauma: An analysis of predictive value in 724 patients with and without traumatic brain injury. Eur. J. Trauma Emerg. Surg. 2013, 39, 25–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mica, L.; Albrecht, K. Independent Predictors of Early Death of Polytrauma Patients: An Analysis of 696 Patients. J. Trauma Treat. 2012, 1, 118. [Google Scholar] [CrossRef]
- Schluter, P.J.; Nathens, A.; Neal, M.L.; Goble, S. Trauma and Injury Severity Score (TRISS) Coefficients 2009 Revision. J. Trauma 2010, 68, 761–770. [Google Scholar] [CrossRef]
- Becalick, D.C.; Coats, T.J. Comparison of artificial intelligence techniques with UKTRISS for estimating probability of survival after trauma. J. Trauma Inj. Infect. Crit. Care 2001, 51, 123–133. [Google Scholar] [CrossRef] [PubMed]
- Steyerberg, E.W.; Vickers, A.J.; Cook, N.R.; Gerds, T.; Gonen, M.; Obuchowski, N.; Pencina, M.J.; Kattan, M.W. Assessing the performance of prediction models: A framework for traditional and novel measures. Epidemiology 2010, 21, 128–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hajian-Tilaki, K. Receiver operating characteristic (ROC) curve analysis for medical diagnostic test evaluation. Casp. J. Intern. Med. 2013, 4, 627–635. [Google Scholar]
- Mandrekar, J.N. Receiver operating characteristic curve in diagnostic test assessment. J. Thorac. Oncol. 2010, 5, 1315–1316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hosmer, D.W.; Hosmer, T.; Le Cessie, S.; Lemeshow, S. A comparison of goodness-of-fit tests for the logistic regression model. Stat. Med. 1997, 16, 965–980. [Google Scholar] [CrossRef]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the Areas under Two or More Correlated Receiver Operating Characteristic Curves: A Nonparametric Approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Rufibach, K. Use of Brier score to assess binary predictions. J. Clin. Epidemiol. 2010, 63, 938–939. [Google Scholar] [CrossRef]
- Abelson-Mitchell, N. Epidemiology and prevention of head injuries: Literature review. J. Clin. Nurs. 2008, 17, 46–57. [Google Scholar] [CrossRef]
- Chiara, O.; Cimbanassi, S.; Pitidis, A.; Vesconi, S. Preventable trauma deaths: From panel review to population based-studies. World J. Emerg. Surg. 2006, 1, 12. [Google Scholar] [CrossRef] [Green Version]
- Krug, E.G.; Sharma, G.K.; Lozano, R. The global burden of injuries. Am. J. Public Health 2000, 90, 523–526. [Google Scholar] [CrossRef] [Green Version]
- Senkowski, C.K.; McKenney, M.G. Trauma scoring systems: A review. J. Am. Coll. Surg. 1999, 189, 491–503. [Google Scholar] [CrossRef]
- Gaikwad, U.G.; Wasnik, N.; Saxena, D.; Akhtar, M. Assessment of trauma and injury severity score model for survival of trauma patients: A single centre experience. Int. Surg. J. 2018, 5, 2550. [Google Scholar] [CrossRef]
- Schluter, P.J. The Trauma and Injury Severity Score (TRISS) revised. Injury 2011, 42, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Boyd, C.R.; Tolson, M.A.; Copes, W.S. Evaluating trauma care: The TRISS method. Trauma Score and the Injury Severity Score. J. Trauma Inj. Infect. Crit. Care 1987, 27, 370–378. [Google Scholar] [CrossRef]
- Champion, H.R.; Sacco, W.J.; Copes, W.S. Injury severity scoring again. J. Trauma 1995, 38, 94–95. [Google Scholar] [CrossRef]
- Valderrama-Molina, C.O.; Giraldo, N.; Constain, A.; Puerta, A.; Restrepo, C.; León, A.; Jaimes, F. Validation of trauma scales: ISS, NISS, RTS and TRISS for predicting mortality in a Colombian population. Eur. J. Orthop. Surg. Traumatol. 2017, 27, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.S.; Tan, J.H.; Mohamad, Y.; Imran, R. External validation of a modified trauma and injury severity score model in major trauma injury. Injury 2019, 50, 1118–1124. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.H.; Tan, H.C.L.; Noh, N.A.M.; Mohamad, Y.; Alwi, R.I. Validation of the trauma mortality prediction scores from a Malaysian population. Burn. Trauma 2017, 5, 1–6. [Google Scholar] [CrossRef]
- Skaga, N.O.; Eken, T.; Søvik, S. Validating performance of TRISS, TARN and NORMIT survival prediction models in a Norwegian trauma population. Acta Anaesthesiol. Scand. 2018, 62, 253–266. [Google Scholar] [CrossRef]
- Chico-Fernández, M.; Sánchez-Casado, M.; Alberdi-Odriozola, F.; Guerrero-López, F.; Mayor-García, M.; Egea-Guerrero, J.; Fernández-Ortega, J.; Bueno-González, A.; González-Robledo, J.; Servià-Goixart, L.; et al. Validation of the probability of survival using the triss methodology in the Spanish Trauma ICU registry (RETRAUCI). Intensive Care Med. Exp. 2015, 3, A856. [Google Scholar] [CrossRef] [Green Version]
- Liu, N.T.; Salinas, J. Machine Learning for Predicting Outcomes in Trauma. Shock 2017, 48, 504–510. [Google Scholar] [CrossRef] [PubMed]
- Mc Gonigal, M.D.; Cole, J.; Schwab, C.W.; Kauder, D.R.; Rotondo, M.F.; Angood, P.B. A new approach to probability of survival scoring for trauma quality assurance. J. Trauma Inj. Infect. Crit. Care 1993, 34, 863–870. [Google Scholar] [CrossRef] [PubMed]
- Rughani, A.I.; Dumont, T.S.M.; Lu, Z.; Bongard, J.; Horgan, M.A.; Penar, P.L.; Tranmer, B.I. Use of an artificial neural network to predict head injury outcome: Clinical article. J. Neurosurg. 2010, 113, 585–590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eftekhar, B.; Mohammad, K.; Ardebili, H.E.; Ghodsi, M.; Ketabchi, E. Comparison of artificial neural network and logistic regression models for prediction of mortality in head trauma based on initial clinical data. BMC Med. Inform. Decis. Mak. 2005, 5, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, H.; Du, J.; Wen, D.; Sun, J.; Chen, M.; Zhang, A.; Jiang, J. Development and validation of a novel predictive score for sepsis risk among trauma patients. World J. Emerg. Surg. 2019, 8, 11. [Google Scholar] [CrossRef]
- Mica, L.; Furrer, E.; Keel, M.T. Predictive ability of the ISS, NISS, and APACHE II score for SIRS and sepsis in polytrauma patients. Eur. J. Trauma Emerg. Surg. 2012, 38, 665–671. [Google Scholar] [CrossRef] [Green Version]
- Hopson, L.R.; Hirsh, E.; Delgado, J.; Domeier, R.M.; McSwain, N.E.; Krohmer, J.; National Association of EMS Physicians; American College of Surgeons Committee on Trauma. Guidelines for Withholding or Termination of Resuscitation in Prehospital Traumatic Cardiopulmonary Arrest: Joint Position Statement of the National Association of EMS Physicians and the American College of Surgeons Committee on Trauma. J. Am. Coll. Surg. 2003, 7515, 106–112. [Google Scholar] [CrossRef]
- Rosemurgy, A.S.; Morris, P.A.; Olson, S.M.; Hurst, J.M.; Albrink, M.H. Prehospital traumatic cardiac arrest: The cost of futility. J. Trauma Inj. Infect. Crit. Care 1993, 35, 468–473. [Google Scholar] [CrossRef]
- Duchnowski, P.; Hryniewiecki, T.; Kuśmierczyk, M.; Szymański, P. High-Sensitivity Troponin T Predicts Postoperative Cardiogenic Shock Requiring Mechanical Circulatory Support in Patients with Valve Disease. Shock 2020, 53, 175–178. [Google Scholar] [CrossRef]
- de Domingues, C.A.; Coimbra, R.; Poggetti, R.S.; de Nogueira, L.S.; de Sousa, R.M.C. New Trauma and Injury Severity Score (TRISS) adjustments for survival prediction. World J. Emerg. Surg. 2018, 13, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Perel, P.; Wasserberg, J.; Ravi, R.R.; Shakur, H.; Edwards, P.; Roberts, I. Prognosis following head injury: A survey of doctors from developing and developed countries. J. Eval. Clin. Pract. 2007, 13, 464–465. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Argentinis, E.; Weber, G. IBM Watson: How Cognitive Computing Can Be Applied to Big Data Challenges in Life Sciences Research. Clin. Ther. 2016, 38, 688–701. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Predictors in WATSON | Predictors in TRISS | Measurement |
|---|---|---|
| Age | Age | Admission report, numerical data |
| Temperature | — | Admission report, numerical data |
| ISS | ISS | Admission report, ordinal data |
| AIS filter for head injury | — | Admission report, binary data |
| — | GCS | Rescue service log, ordinal data |
| — | Systolic blood pressure | Rescue service log, numerical data |
| — | Respiratory rate | Rescue service log, numerical data |
| — | Type of trauma | Admission report, binary data |
| Validation Group | Development Group | ||||
|---|---|---|---|---|---|
| Patient Sample n = 107 | Survivors n = 96 | Non-Survivors n = 11 | p-Value | Patient Sample n = 3647 | |
| Age (mean, SD) | 48.3 ± 19.7 | 47.1 ± 19.0 | 58.7 ± 24.0 | 0.063 | 45.8 ± 20.2 |
| Male | 69.2% (n = 74) | 69.8 % (n = 67) | 63.6% (n = 7) | — | 73.5 % (n = 2680) |
| Blunt trauma | 99.1% (n = 106) | 100% (n = 96) | 90.9% (n = 10) | — | 91.3% (n = 3329) |
| ATLS shock class (median, IQR) | 1 (1–3) | 1 (1–3) | 1 (1–3.5) | 0.149 | 1 (1–2) |
| ISS (median, IQR) | 30 (23–36) | 29 (22–34.5) | 42 (31–66) | 0.009 | 25 (17–34) |
| Temperature at admission (mean, SD) | 35.9 ± 1.3 | 36.0 ± 1.2 | 34.9 ± 1.6 | 0.007 | 35.5 ± 1.7 |
| Head injury | 70.1% (n = 75) | 67.7% (n = 65) | 90.9% (n = 10) | — | 76.2% (n = 2780) |
| SIRS (within 21 days) | 76.6% (n= 82) | 75.0% (n = 72) | 90.9% (n = 10) | — | 83.5% (n = 3044) |
| Sepsis (within 21 days) | 12.1% (n = 13) | 13.5% (n = 13) | 0% (n = 0) | — | 15.0% (n = 546) |
| Early Death (within 72 h) | 10.3% (n = 11) | — | — | — | 19.4% (n = 709) |
| GCS at patient contact (median, IQR) | 13 (8.5–15) | 14 (9–15) | 3 (3–9.5) | <0.001 | — |
| SBP at patient contact (mean, SD) | 119 ± 37 | 122 ± 32 | 98 ± 66 | 0.039 | — |
| RR at patient contact (mean, SD) | 17.3 ± 6.7 | 17.8 ± 6.5 | 12.9 ± 7.4 | 0.022 | — |
| RTS at patient contact (median, IQR) | 6.90 (5.97–7.84) | 7.11 (6.38–7.84) | 4.09 (3.73–5.71) | <0.001 | — |
| AUC | H-L Statistics | Brier SCORE | |
|---|---|---|---|
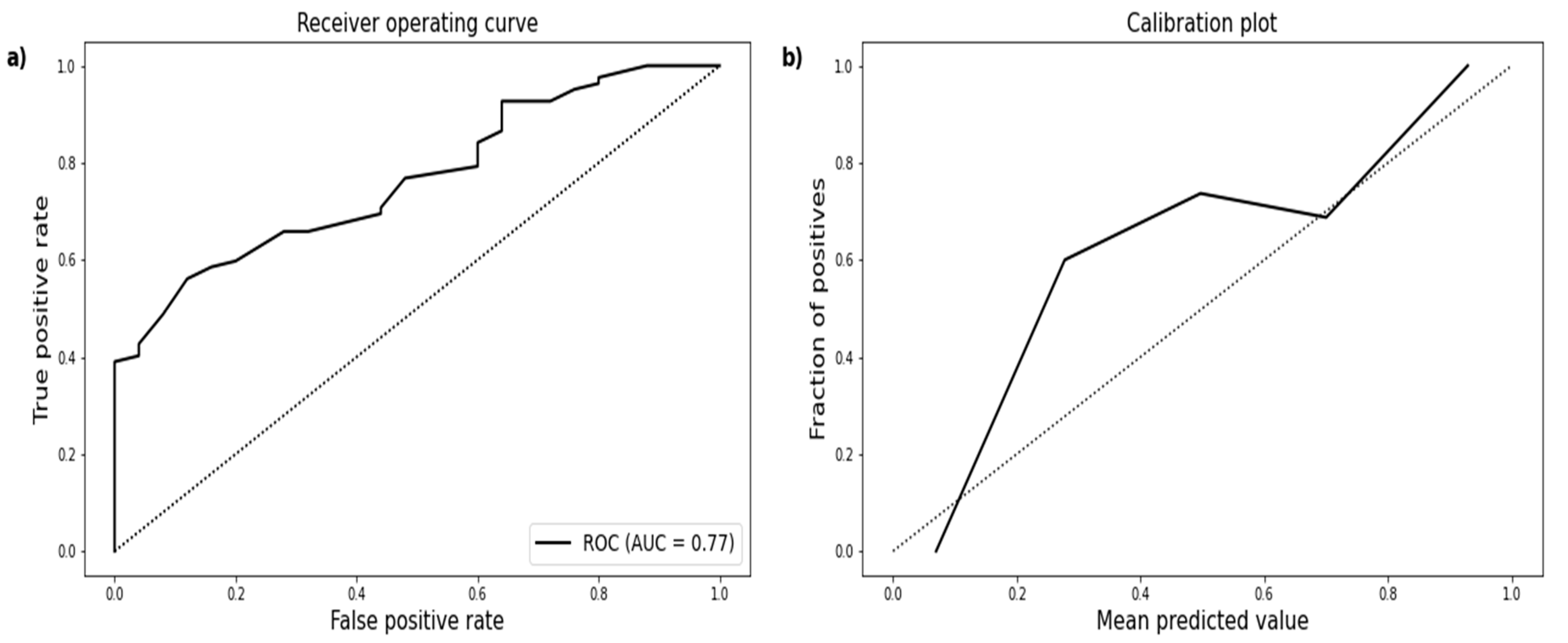
| SIRS by WATSON | 0.77 (95% CI 0.68–0.85) | X2 = 5.24, p = 0.73 | 0.15 |
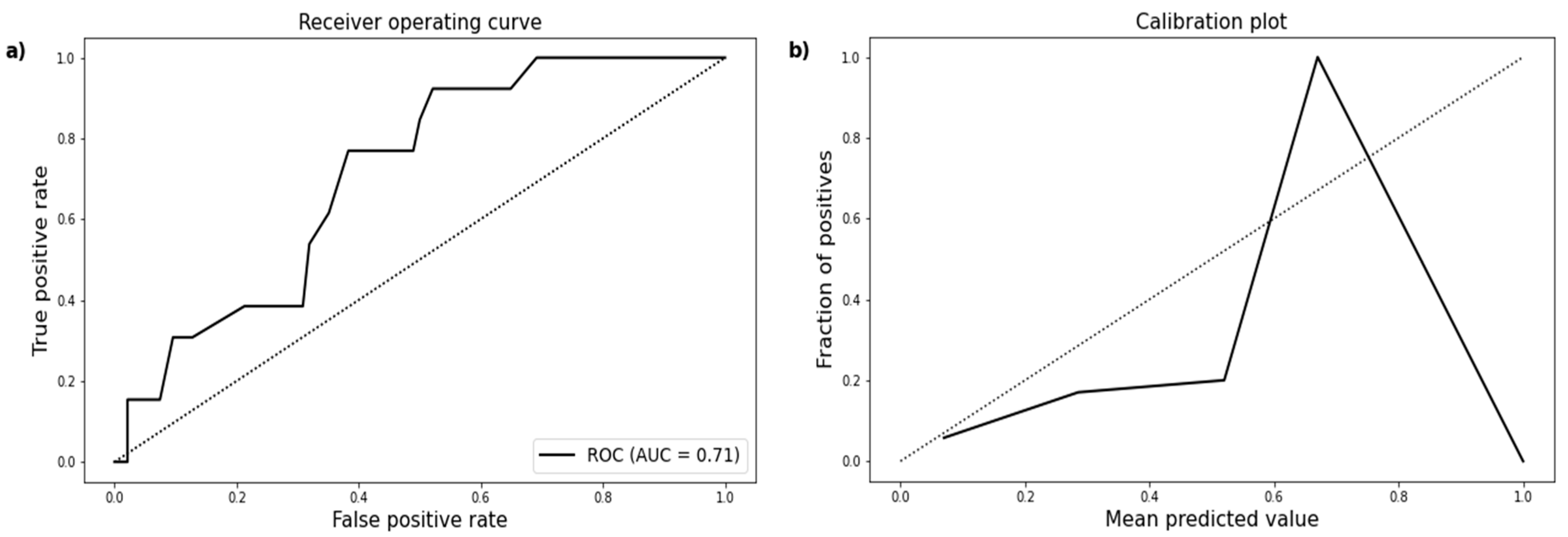
| Sepsis by WATSON | 0.71 (95% CI 0.58–0.83) | X2 = 12.14, p = 0.14 | 0.12 |
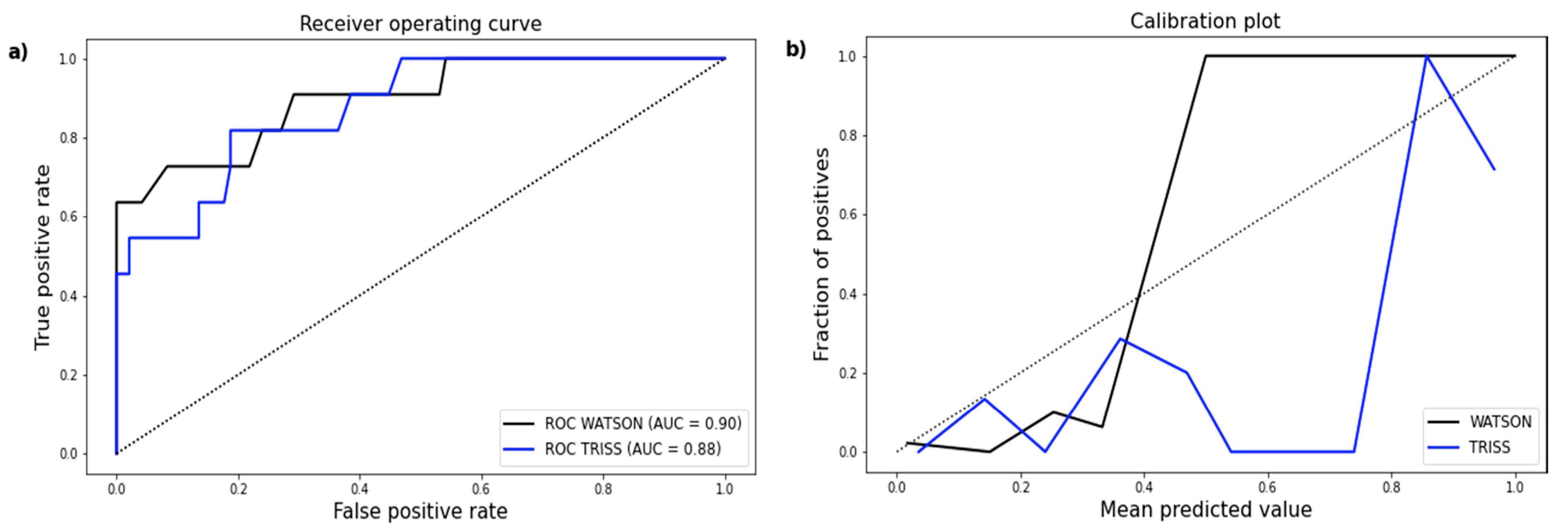
| Early Death by WATSON | 0.90 (95% CI 0.79–0.99) | X2 = 8.19, p = 0.42 | 0.06 |
| Early Death by TRISS | 0.88 (95% CI 0.77–0.97) | X2 = 31.93, p < 0.05 | 0.11 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Niggli, C.; Pape, H.-C.; Niggli, P.; Mica, L. Validation of a Visual-Based Analytics Tool for Outcome Prediction in Polytrauma Patients (WATSON Trauma Pathway Explorer) and Comparison with the Predictive Values of TRISS. J. Clin. Med. 2021, 10, 2115. https://doi.org/10.3390/jcm10102115
Niggli C, Pape H-C, Niggli P, Mica L. Validation of a Visual-Based Analytics Tool for Outcome Prediction in Polytrauma Patients (WATSON Trauma Pathway Explorer) and Comparison with the Predictive Values of TRISS. Journal of Clinical Medicine. 2021; 10(10):2115. https://doi.org/10.3390/jcm10102115
Chicago/Turabian StyleNiggli, Cédric, Hans-Christoph Pape, Philipp Niggli, and Ladislav Mica. 2021. "Validation of a Visual-Based Analytics Tool for Outcome Prediction in Polytrauma Patients (WATSON Trauma Pathway Explorer) and Comparison with the Predictive Values of TRISS" Journal of Clinical Medicine 10, no. 10: 2115. https://doi.org/10.3390/jcm10102115
APA StyleNiggli, C., Pape, H.-C., Niggli, P., & Mica, L. (2021). Validation of a Visual-Based Analytics Tool for Outcome Prediction in Polytrauma Patients (WATSON Trauma Pathway Explorer) and Comparison with the Predictive Values of TRISS. Journal of Clinical Medicine, 10(10), 2115. https://doi.org/10.3390/jcm10102115