
Carbapenem-Resistant Klebsiella pneumoniae Infections in ICU COVID-19 Patients—A Scoping Review

 ,
, 
 ,
,  and
and 
Abstract
:1. Introduction
1.1. Resistance in Klebsiella pneumoniae
1.2. Co-Infections in Patients with COVID-19
1.3. Objective
2. Methods
2.1. Study Design
2.2. Definition of Scoping Review
2.3. Search Strategy
2.4. Study Selection
2.5. Selection Process
2.6. Data Extraction
3. Results
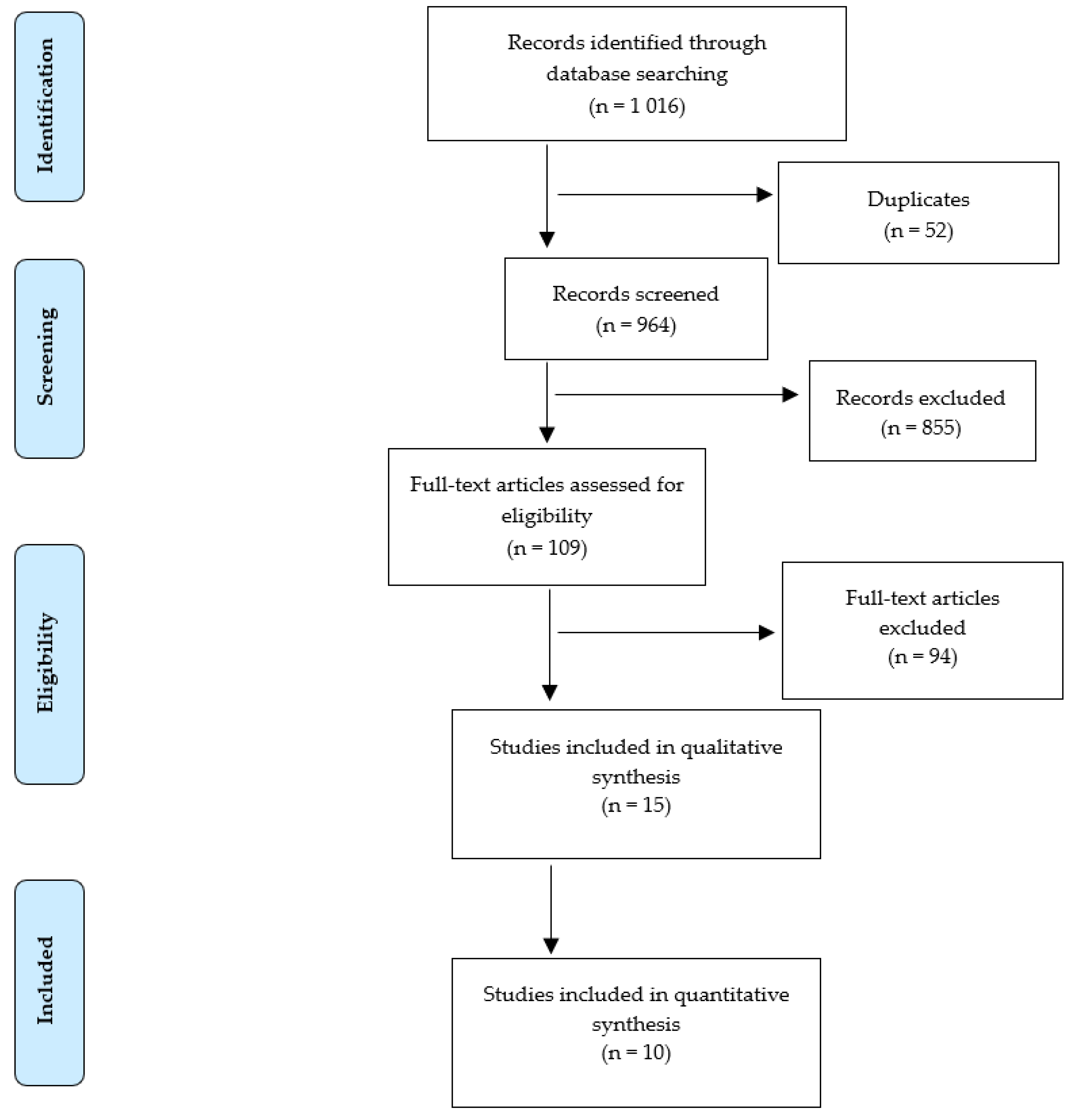
3.1. Results of the Scoping Review
3.2. Demographic and Social Data
3.3. Characteristics of the Study Population
4. Discussion
5. A Limitation of Scoping Review
6. Conclusions
7. Implications for Practice
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Carvalhaes, C.G.; Cayô, R.; Gales, A.C. Klebsiella pneumoniae Carbapenemase-Producing Klebsiella pneumoniae in the Intensive Care Unit: A Real Challenge to Physicians, Scientific Community, and Society. Shock 2013, 39, 32–37. [Google Scholar] [CrossRef]
- Logan, L.K.; Weinstein, R.A. The Epidemiology of Carbapenem-Resistant Enterobacteriaceae: The Impact and Evolution of a Global Menace. J. Infect. Dis. 2017, 215, S28–S36. [Google Scholar] [CrossRef] [Green Version]
- Martin, R.M.; Bachman, M.A. Colonization, Infection, and the Accessory Genome of Klebsiella pneumoniae. Front. Cell. Infect. Microbiol. 2018, 8, 4. [Google Scholar] [CrossRef] [Green Version]
- Alves, A.; Sucena, I.; Ribeiro, C.; Silva, E.; Shiang, T.; Vanzeller, M. Factors associated with colonization and infection by Carbapenem Resistant Enterobacteriaceae. Eur. Respir. J. 2018, 52, PA4702. [Google Scholar] [CrossRef]
- Sievert, D.M.; Ricks, P.; Edwards, J.R.; Schneider, A.; Patel, J.; Srinivasan, A.; Kallen, A.; Limbago, B.; Fridkin, S. Antimicrobial-resistant pathogens associated with healthcare-associated infections: Summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2009–2010. Infect. Control Hosp. Epidemiol. 2013, 34, 1–14. [Google Scholar] [CrossRef]
- Kotb, S.; Lyman, M.; Ismail, G.; El Fattah, M.A.; Girgis, S.A.; Etman, A.; Hafez, S.; El-Kholy, J.; Zaki, M.E.S.; Rashed, H.-A.G.; et al. Epidemiology of Carbapenem-resistant Enterobacteriaceae in Egyptian intensive care units using National Healthcare–associated Infections Surveillance Data, 2011–2017. Antimicrob. Resist. Infect. Control 2020, 9, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Yuling, Z.; Zhao, Y.; Liu, C.; Chen, Z.; Zhou, D. Molecular pathogenesis of Klebsiella pneumoniae. Future Microbiol. 2014, 9, 1071–1081. [Google Scholar] [CrossRef]
- Czekaj, T.; Ciszewski, M. Klebsiella pneumoniae NDM—New emerging superbacteria. Med. Rodz. 2015, 1, 23–27. [Google Scholar]
- Xu, L.; Sun, X.; Ma, X. Systematic review and meta-analysis of mortality of patients infected with carbapenem-resistant Klebsiella pneumoniae. Ann. Clin. Microbiol. Antimicrob. 2017, 16, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Reyes, J.; Aguilar, A.C.; Caicedo, A. Carbapenem-Resistant Klebsiella pneumoniae: Microbiology Key Points for Clinical Practice. Int. J. Gen. Med. 2019, 12, 437–446. [Google Scholar] [CrossRef] [Green Version]
- Nordmann, P.; Dortet, L.; Poirel, L. Carbapenem resistance in Enterobacteriaceae: Here is the storm! Trends Mol. Med. 2012, 18, 263–272. [Google Scholar] [CrossRef]
- Molton, J.S.; Tambyah, P.A.; Ang, B.S.P.; Ling, M.L.; Fisher, D.A. The Global Spread of Healthcare-Associated Multidrug-Resistant Bacteria: A Perspective from Asia. Clin. Infect. Dis. 2013, 56, 1310–1318. [Google Scholar] [CrossRef] [PubMed]
- McConville, T.H.; Sullivan, S.B.; Gomez-Simmonds, A.; Whittier, S.; Uhlemann, A.-C. Carbapenem-resistant Enterobacteriaceae colonization (CRE) and subsequent risk of infection and 90-day mortality in critically ill patients, an observational study. PLoS ONE 2017, 12, e0186195. [Google Scholar] [CrossRef]
- Kang, J.S.; Yi, J.; Ko, M.K.; Lee, S.O.; Lee, J.E.; Kim, K.-H. Prevalence and Risk Factors of Carbapenem-resistant Enterobacteriaceae Acquisition in an Emergency Intensive Care Unit in a Tertiary Hospital in Korea: A Case-Control Study. J. Korean Med. Sci. 2019, 34, e140. [Google Scholar] [CrossRef] [PubMed]
- Kumarasamy, K.K.; Toleman, M.A.; Walsh, T.R.; Bagaria, J.; Butt, F.; Balakrishnan, R.; Chaudhary, U.; Doumith, M.; Giske, C.G.; Irfan, S.; et al. Emergence of a new antibiotic resistance mechanism in India, Pakistan, and the UK: A molecular, biological, and epidemiological study. Lancet Infect. Dis. 2010, 10, 597–602. [Google Scholar] [CrossRef]
- Ludwig, S.; Zarbock, A. Coronaviruses and SARS-CoV-2: A Brief Overview. Anesth Analg. 2020, 20. [Google Scholar] [CrossRef]
- Rawson, T.M.; Moore, L.S.P.; Zhu, N.; Ranganathan, N.; Skolimowska, K.; Gilchrist, M.; Satta, G.; Cooke, G.; Holmes, A. Bacterial and Fungal Coinfection in Individuals with Coronavirus: A Rapid Review to Support COVID-19 Antimicrobial Prescribing. Clin. Infect. Dis. 2020, 71, 2459–2468. [Google Scholar] [CrossRef]
- Phelan, A.L.; Katz, R.; Gostin, L.O. The Novel Coronavirus Originating in Wuhan, China: Challenges for Global Health Governance. JAMA 2020, 323, 709. [Google Scholar] [CrossRef] [Green Version]
- Bengoechea, J.A.; Bamford, C.G. SARS-CoV-2, bacterial coinfections, and AMR: The deadly trio in COVID-19? EMBO Mol. Med. 2020, 12, e12560. [Google Scholar] [CrossRef]
- Bogossian, E.G.; Taccone, F.S.; Izzi, A.; Yin, N.; Garufi, A.; Hublet, S.; Njimi, H.; Ego, A.; Gorham, J.; Byl, B.; et al. The Acquisition of Multidrug-Resistant Bacteria in Patients Admitted to COVID-19 Intensive Care Units: A Monocentric Retrospective Case Control Study. Microorganisms 2020, 8, 1821. [Google Scholar] [CrossRef] [PubMed]
- Moledina, S.M.; Maini, A.A.; Gargan, A.; Harland, W.; Jenney, H.; Phillips, G.; Thomas, K.; Chauhan, D.; Fertleman, M. Clinical Characteristics and Predictors of Mortality in Patients with COVID-19 Infection Outside Intensive Care. Int. J. Gen. Med. 2020, 13, 1157–1165. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Leung, V.; Westwood, D.; MacFadden, D.R.; Soucy, J.P.J.; Daneman, N. Bacterial co-infection and secondary infection in patients with COVID-19: A living rapid review and meta-analysis. Clin. Microbiol. Infect. 2020, 26, 1622–1629. [Google Scholar] [CrossRef]
- Zhu, X.; Ge, Y.; Wu, T.; Zhao, K.; Chen, Y.; Wu, B.; Zhu, F.; Zhu, B.; Cui, L. Co-infection with respiratory pathogens among COVID-2019 cases. Virus Res. 2020, 285, 198005. [Google Scholar] [CrossRef]
- Ruan, Q.; Yang, K.; Wang, W.; Jiang, L.; Song, J. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensiv. Care Med. 2020, 46, 846–848. [Google Scholar] [CrossRef] [Green Version]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [Green Version]
- The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 5 February 2021).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; for the PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Karruli, A.; Boccia, F.; Gagliardi, M.; Patauner, F.; Ursi, M.P.; Sommese, P.; De Rosa, R.; Murino, P.; Ruocco, G.; Corcione, A.; et al. Multidrug-Resistant Infections and Outcome of Critically Ill Patients with Coronavirus Disease 2019: A Single Center Experience. Microb. Drug Resist. 2021. [Google Scholar] [CrossRef]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Xia, J.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir. Med. 2020, 8, 475–481, Erratum in Lancet Respir Med. 2020, 8, e26. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Wang, J.; Yang, Y.; Cai, P.; Cao, J.; Cai, X.; Zhang, Y. Etiology and antimicrobial resistance of secondary bacterial infections in patients hospitalized with COVID-19 in Wuhan, China: A retrospective analysis. Antimicrob. Resist. Infect. Control 2020, 9, 153. [Google Scholar] [CrossRef] [PubMed]
- Ramadan, H.K.-A.; Mahmoud, M.; Aburahma, M.Z.; Elkhawaga, A.; El-Mokhtar, M.; Sayed, I.M.; Hosni, A.; Hassany, S.M.; Medhat, M. Predictors of Severity and Co-Infection Resistance Profile in COVID-19 Patients: First Report from Upper Egypt. Infect. Drug Resist. 2020, 13, 3409–3422. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Simmonds, A.; Annavajhala, M.K.; McConville, T.H.; Dietz, D.; Shoucri, S.M.; Laracy, J.C.; Rozenberg, F.D.; Nelson, B.; Greendyke, W.G.; Furuya, E.Y.; et al. Carbapenemase-producing Enterobacterales causing secondary infections during the COVID-19 crisis at a New York City hospital. J. Antimicrob. Chemother. 2021, 76, 380–384. [Google Scholar] [CrossRef] [PubMed]
- García-Meniño, I.; Forcelledo, L.; Rosete, Y.; García-Prieto, E.; Escudero, D.; Fernández, J. Spread of OXA-48-producing Klebsiella pneumoniae among COVID-19-infected patients: The storm after the storm. J. Infect. Public Health 2021, 14, 50–52. [Google Scholar] [CrossRef]
- Montrucchio, G.; Corcione, S.; Sales, G.; Curtoni, A.; De Rosa, F.; Brazzi, L. Carbapenem-resistant Klebsiella pneumoniae in ICU-admitted COVID-19 patients: Keep an eye on the ball. J. Glob. Antimicrob. Resist. 2020, 23, 398–400. [Google Scholar] [CrossRef]
- Arcari, G.; Raponi, G.; Sacco, F.; Bibbolino, G.; Di Lella, F.M.; Alessandri, F.; Coletti, M.; Trancassini, M.; Deales, A.; Pugliese, F.; et al. Klebsiella pneumoniae infections in COVID-19 patients: A 2-month retrospective analysis in an Italian hospital. Int. J. Antimicrob. Agents 2021, 57, 106245. [Google Scholar] [CrossRef]
- Magnasco, L.; Mikulska, M.; Giacobbe, D.; Taramasso, L.; Vena, A.; Dentone, C.; Dettori, S.; Tutino, S.; Labate, L.; Di Pilato, V.; et al. Spread of Carbapenem-Resistant Gram-Negatives and Candida auris During the COVID-19 Pandemic in Critically Ill Patients: One Step Back in Antimicrobial Stewardship? Microorganisms 2021, 9, 95. [Google Scholar] [CrossRef]
- Arteaga-Livias, K.; Pinzas-Acosta, K.; Perez-Abad, L.; Panduro-Correa, V.; Rabaan, A.A.; Pecho-Silva, S.; Dámaso-Mata, B. A multidrug-resistant Klebsiella pneumoniae outbreak in a Peruvian hospital: Another threat from the COVID-19 pandemic. Infect. Control Hosp. Epidemiol. 2021, 1–2. [Google Scholar] [CrossRef]
- Tiri, B.; Sensi, E.; Marsiliani, V.; Cantarini, M.; Priante, G.; Vernelli, C.; Martella, L.A.; Costantini, M.; Mariottini, A.; Andreani, P.; et al. Antimicrobial Stewardship Program, COVID-19, and Infection Control: Spread of Carbapenem-Resistant Klebsiella pneumoniae Colonization in ICU COVID-19 Patients. What Did Not Work? J. Clin. Med. 2020, 9, 2744. [Google Scholar] [CrossRef]
- Belvisi, V.; Del Borgo, C.; Vita, S.; Redaelli, P.; Dolce, P.; Pacella, D.; Kertusha, B.; Carraro, A.; Marocco, R.; De Masi, M.; et al. Impact of SARS CoV-2 pandemic on carbapenemase-producing Klebsiella pneumoniae prevention and control programme: Convergent or divergent action? J. Hosp. Infect. 2021, 109, 29–31. [Google Scholar] [CrossRef]
- Soriano, M.C.; Vaquero, C.; Ortiz-Fernández, A.; Caballero, A.; Blandino-Ortiz, A.; de Pablo, R. Low incidence of co-infection, but high incidence of ICU-acquired infections in critically ill patients with COVID-19. J. Infect. 2021, 82, e20–e21. [Google Scholar] [CrossRef]
- Mahmoudi, H. Bacterial co-infections and antibiotic resistance in patients with COVID-19. GMS Hyg. Infect. Control 2020, 15. [Google Scholar] [CrossRef]
- Hughes, S.; Troise, O.; Donaldson, H.; Mughal, N.; Moore, L. Bacterial and fungal coinfection among hospitalized patients with COVID-19: A retrospective cohort study in a UK secondary-care setting. Clin. Microbiol. Infect. 2020, 26, 1395–1399. [Google Scholar] [CrossRef] [PubMed]
- Norton, A. Many COVID-19 Patients Given Useless Antibiotics, Study Finds; Isle of Man; Medical Xpress: Bradford, UK, 4 August 2020; Available online: https://medicalxpress.com/news/2020-08-covid-patients-useless-antibiotics.html (accessed on 15 February 2021).
- Getahun, H.; Smith, I.; Trivedi, K.; Paulin, S.; Balkhy, H.H. Tackling antimicrobial resistance in the COVID-19 pandemic. Bull. World Health Organ. 2020, 98, 442. [Google Scholar] [CrossRef]
- Chedid, M.; Waked, R.; Haddad, E.; Chetata, N.; Saliba, G.; Choucair, J. Antibiotics in treatment of COVID-19 complications: A review of frequency, indications, and efficacy. J. Infect. Public Health 2021, 14, 570–576. [Google Scholar] [CrossRef]
- Pelfrene, E.; Botgros, R.; Cavaleri, M. Antimicrobial multidrug resistance in the era of COVID-19: A forgotten plight? Antimicrob. Resist. Infect. Control 2021, 10, 21. [Google Scholar] [CrossRef] [PubMed]
- Baiou, A.; Elbuzidi, A.A.; Bakdach, D.; Zaqout, A.; Alarbi, K.M.; Bintaher, A.A.; Ali, M.M.B.; Elarabi, A.M.; Ali, G.A.M.; Daghfal, J.; et al. Clinical characteristics and risk factors for the isolation of multi-drug-resistant Gram-negative bacteria from critically ill patients with COVID-19. J. Hosp. Infect. 2021, 110, 165–171. [Google Scholar] [CrossRef]


{kind=link}
| Inclusion Criteria | Exclusion Criteria | |
|---|---|---|
| Years considered/Time period | All evidence published in the last 2 years, period 2019–2021 | |
| Setting | Healthcare settings for COVID-19 patients | Other healthcare settings |
| Type of study design/references | Observational studies, cases report, letters to the editor | Descriptive studies, single-case report |
| Participants | Positive COVID-19 patients | Negative COVID-19 patients |
| Interventions | Interventions to detect CRKP infection | Studies without a clearly described intervention |
| Outcome measures | Patient outcomes, culture outcomes | General outcome of co-infections in COVID-19 patients (without specification) |
| Language | English | Other lenguage |
| Databases | MEDLINE (PubMed), Cochrane Library | Other databases |
| Key words | Carbapenem-resistance, Klebsiella pneumoniae, COVID-19 | |
| Additional search terms, with which the central search terms were combined | COVID-19, co-infections, Intensive Care Units Klebsiella pneumoniae, Carbapenem-Resistant Enterobacteriaceae, COVID-19 COVID-19, CRKP, ICU |
| First Author, Year | Study Design | Selection | Comparability | Outcome | Total Scores |
|---|---|---|---|---|---|
| Karruli A. et al. 2019 [30] | Retrospective study | ** | ** | ** | 6 |
| Yang X. et al. 2020 [31] | Retrospective study | *** | ** | * | 6 |
| Li J. et al. 2020 [32] | Retrospective study | *** | * | ** | 6 |
| Ramadan, H.K.A et al. 2020 [33] | Prospective study | *** | ** | ** | 7 |
| Gomez-Simmonds, A. et al. 2020 [34] | Retrospective study | **** | ** | *** | 8 |
| García–Menioño, I. et al. 2021 [35] | Retrospective study | *** | ** | *** | 8 |
| Montrucchioa, G. et al. 2020 [36] | Retrospective study | *** | ** | *** | 8 |
| Arcari, G. et al. 2021 [37] | Retrospective study | ** | ** | *** | 7 |
| Magnasco, L. et al. 2021 [38] | Retrospective study | *** | * | *** | 7 |
| Arteaga-Livias, K. et al. 2021 [39] | Prospective study | *** | ** | ** | 7 |
| First Author, Year | (1) Question and Inclusion | (2) Protocol | (3) Study Design | (4) Comprehensive Search | (5) Study Selection | (6) Data Extraction | (7) Excluded Studies Justification | (8) Included Studies Details | (9) Risk of Bias (RoB) | (10) Funding Sources | (11) Statistical Methods | (12) RoB on Meta-Analysis | (13) RoB in Individual Studies | (14) Explanation for Heterogeneity | (15) Publication Bias | (16) Conflict of Interest |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Karruli A. et al. 2019 [30] | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | No | Yes | Yes | Yes | No |
| Yang X. et al. 2020 [31] | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | No | Yes | Yes | Yes | No |
| Li J. et al. 2020 [32] | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | No | Yes | Yes | Yes | No |
| Ramadan, H.K.A. et al. 2020 [33] | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | No |
| Gomez-Simmonds, A. et al. 2020 [34] | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | N/a | N/a | Yes | Yes | No | No |
| García—Menioño, I., et al. 2020 [35] | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | N/a | N/a | Yes | Yes | No | No |
| Montrucchioa, G. et al. 2020 [36] | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | N/a | N/a | Yes | Yes | No | No |
| Arcari, G., et al. 2021 [37] | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | N/a | N/a | Yes | Yes | No | No |
| Magnasco, L. et al. 2021 [38] | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | No | Yes | Yes | Yes | No |
| Arteaga-Livias, K. et al. 2021 [39] | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | N/a | N/a | Yes | Yes | No | No |
| Total, N (%) | 10 (100%) | 0 (0%) | 10 (100%) | 10 (100%) | 10 (100%) | 10 (100%) | 10 (100%) | 10 (100%) | 10 (100%) | 3 (27%) | 5 (50%) | 1 (9%) | 10 (100%) | 10 (100%) | 5 (45%) | 0 (0%) |
| First Author, Year | Sex (%) | Age * [Years] |
|---|---|---|
| Karruli A. et al. 2019 [30] | n/d | n/d |
| Yang X. et al. 2020 [31] | n/d | n/d |
| Li J. et al. 2020 [32] | n/d | n/d |
| Ramadan, H.K.A. et al. 2020 [33] | n/d | n/d |
| Gomez-Simmonds, A. et al. 2020 [34] | 1 F (9) 10 M (91) | 62 (23–74) |
| García–Menioño, I. et al. 2020 [35] | 1 F (14) 6 M (86) | 67 (54–76) |
| Montrucchioa, G. et al. 2020 [36] | 3 F (43) 4 M (57) | 57 (41–71) |
| Arcari, G. et al. 2021 [37] | n/d | n/d |
| Magnasco, L. et al. 2021 [38] | 0 F (0) 2 M (100) | 65 (63,66) |
| Arteaga-Livias, K. et al. 2021 [39] | 0 F (0) 4 M (100) | 56 (45–66) |
| First Author, Year | Country (Region) | Population | Number of Infected Patients (%) | Resistance Gene |
|---|---|---|---|---|
| Karruli A. et al. 2019 [30] | Italy (Napoli) | 32 | n/d | KPC |
| Yang X. et al. 2020 [31] | China (Wuhan) | 52 | 1(2%) | n/d |
| Li J. et al. 2020 [32] | China (Wuhan) | 102 | 32 (31.4%) | n/d |
| Ramadan, H.K.A. et al. 2020 [33] | Egypt (Assiut) | 260 | n/d | KPC, CTX-M, TEM, SHV |
| Gomez-Simmonds, A. et al. 2020 [34] |
United States (New York City) | 3152 | 11(0.35%) | KPC |
| García–Menioño, I. et al. 2020 [35] | Spain (Oviedo, Asturias) | 62 | 3(4.8%) | OXA-48, CTX-M |
| Montrucchioa, G. et al. 2020 [36] | Italy (Turyn) | 35 | 6(17.1%) | KPC |
| Arcari, G. et al. 2021 [37] | Italy (Rome) | 65 | 7(10.8%) | KPC, OXY-48 |
| Magnasco, L. et al. 2021 [38] | Italy (Genoa) | 118 | 2(1.7%) | n/d |
| Arteaga-Livias, K. et al. 2021 [39] | Peru | n/d | 4 | NDM, CTX-M |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mędrzycka-Dąbrowska, W.; Lange, S.; Zorena, K.; Dąbrowski, S.; Ozga, D.; Tomaszek, L. Carbapenem-Resistant Klebsiella pneumoniae Infections in ICU COVID-19 Patients—A Scoping Review. J. Clin. Med. 2021, 10, 2067. https://doi.org/10.3390/jcm10102067
Mędrzycka-Dąbrowska W, Lange S, Zorena K, Dąbrowski S, Ozga D, Tomaszek L. Carbapenem-Resistant Klebsiella pneumoniae Infections in ICU COVID-19 Patients—A Scoping Review. Journal of Clinical Medicine. 2021; 10(10):2067. https://doi.org/10.3390/jcm10102067
Chicago/Turabian StyleMędrzycka-Dąbrowska, Wioletta, Sandra Lange, Katarzyna Zorena, Sebastian Dąbrowski, Dorota Ozga, and Lucyna Tomaszek. 2021. "Carbapenem-Resistant Klebsiella pneumoniae Infections in ICU COVID-19 Patients—A Scoping Review" Journal of Clinical Medicine 10, no. 10: 2067. https://doi.org/10.3390/jcm10102067
APA StyleMędrzycka-Dąbrowska, W., Lange, S., Zorena, K., Dąbrowski, S., Ozga, D., & Tomaszek, L. (2021). Carbapenem-Resistant Klebsiella pneumoniae Infections in ICU COVID-19 Patients—A Scoping Review. Journal of Clinical Medicine, 10(10), 2067. https://doi.org/10.3390/jcm10102067