Triage of Patients Suspected of COVID-19 in Chronic Hemodialysis: Eosinophil Count Differentiates Low and High Suspicion of COVID-19

 , , and
, , and 
Abstract
1. Introduction
2. Methods
2.1. Setting
2.2. Participants
2.3. Data Source/Measurement
2.3.1. Epidemiological and Clinical Data
2.3.2. Laboratory Procedures
2.3.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
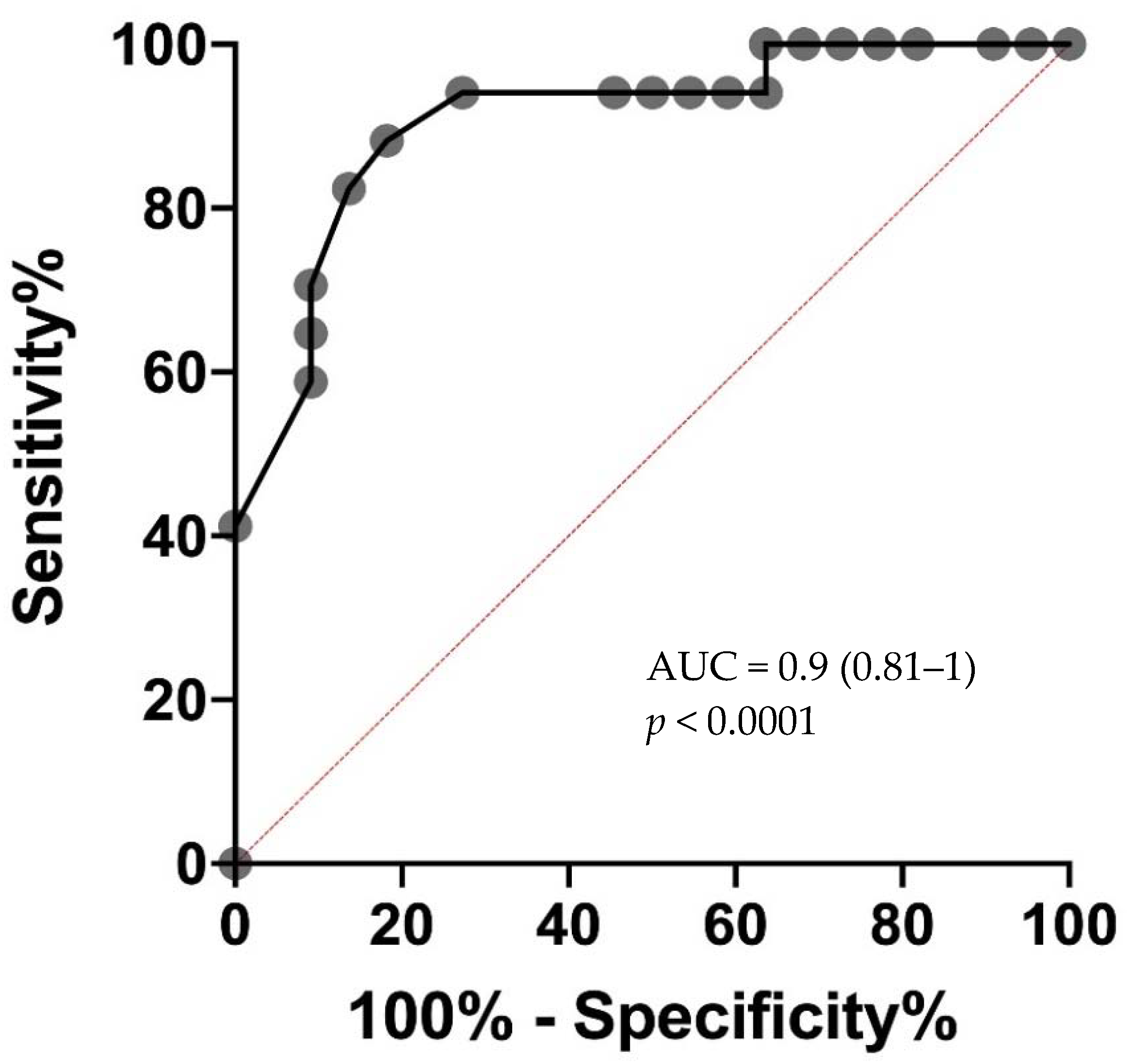
3.2. Diagnostic Accuracy of Eosinopenia
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ACEI | Angiotensin-converting enzyme inhibitors |
| APHM | Assistance Publique–Hôpitaux de Marseille |
| ARB | Angiotensin receptor blockers |
| BMI | Body mass index |
| CBC | Complete blood count |
| COVID-19 | Coronavirus Disease-19 |
| CRP | C-reactive protein |
| CT | Chest computed tomography |
| IQR | Interquartile range |
| NSAIDs | Non-steroidal anti-inflammatory drugs |
| SARS-CoV-2 | Severe acute respiratory syndrome related-coronavirus 2 |
| ROC AUC | Receiver operating characteristic area under curve |
| RNA | Ribonucleic acid |
| RT-PCR | Real-time reverse-transcriptase polymerase chain reaction |
References
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Cheng, Y.; Luo, R.; Wang, K.; Zhang, M.; Wang, Z.; Dong, L.; Li, J.; Yao, Y.; Ge, S.; Xu, G. Kidney disease is associated with in-hospital death of patients with COVID-19. Kidney Int. 2020, 97, 829–838. [Google Scholar] [CrossRef] [PubMed]
- Burgner, A.; Ikizler, T.A.; Dwyer, J.P. COVID-19 and the Inpatient Dialysis Unit: Managing Resources During Contingency Planning Pre-Crisis. Clin. J. Am. Soc. Nephrol. 2020, 15, 720–722. [Google Scholar] [CrossRef] [PubMed]
- Basile, C.; Combe, C.; Pizzarelli, F.; Covic, A.; Davenport, A.; Kanbay, M.; Kirmizis, D.; Schneditz, D.; van der Sande, F.; Mitra, S. Recommendations for the prevention, mitigation and containment of the emerging SARS-CoV-2 (COVID-19) pandemic in haemodialysis centres. Nephrol. Dial. Transplant. 2020, 35, 737–741. [Google Scholar] [CrossRef] [PubMed]
- Sethuraman, N.; Jeremiah, S.S.; Ryo, A. Interpreting Diagnostic Tests for SARS-CoV-2. JAMA 2020, 323, 2249–2251. [Google Scholar] [CrossRef] [PubMed]
- Long, C.; Xu, H.; Shen, Q.; Zhang, X.; Fan, B.; Wang, C.; Zeng, B.; Li, Z.; Li, X.; Li, H. Diagnosis of the Coronavirus disease (COVID-19): rRT-PCR or CT? Eur. J. Radiol. 2020, 126, 108961. [Google Scholar] [CrossRef]
- Bataille, S.; Pedinielli, N.; Bergougnioux, J.-P. Could ferritin help the screening for COVID-19 in hemodialysis patients? Kidney Int. 2020, 98, 235–236. [Google Scholar] [CrossRef] [PubMed]
- Thomas, A.; Silver, S.A.; Perl, J.; Freeman, M.; Slater, J.J.; Nash, D.M.; Vinegar, M.; McArthur, E.; Garg, A.X.; Harel, Z.; et al. The Frequency of Routine Blood Sampling and Patient Outcomes Among Maintenance Hemodialysis Recipients. Am. J. Kidney Dis. 2020, 75, 471–479. [Google Scholar] [CrossRef] [PubMed]
- Lano, G.; Braconnier, A.; Bataille, S.; Cavaille, G.; Moussi-Frances, J.; Gondouin, B.; Bindi, P.; Nakhla, M.; Mansour, J.; Halin, P.; et al. Risk factors for severity of COVID-19 in chronic dialysis patients from a multicentre French cohort. Clin. Kidney J. 2020, 13, 878–888. [Google Scholar] [CrossRef]
- Corman, V.M.; Landt, O.; Kaiser, M.; Molenkamp, R.; Meijer, A.; Chu, D.K.W.; Bleicker, T.; Brünink, S.; Schneider, J.; Schmidt, M.L.; et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Eurosurveillance 2020, 25, 2000045. [Google Scholar] [CrossRef] [PubMed]
- Kita, H. Eosinophils: Multifaceted biological properties and roles in health and disease: Immunobiology of eosinophils. Immunol. Rev. 2011, 242, 161–177. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Ding, X.; Xia, G.; Chen, H.G.; Chen, F.; Geng, Z.; Xu, L.; Lei, S.; Pan, A.; Wang, L.; et al. Eosinopenia and elevated C-reactive protein facilitate triage of COVID-19 patients in fever clinic: A retrospective case-control study. EClinicalMedicine 2020, 23, 100375. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.-J.; Ni, Z.-Y.; Hu, Y.; Liang, W.-H.; Ou, C.-Q.; He, J.-X.; Liu, L.; Shan, H.; Lei, C.-L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Qarni, B.; Osman, M.A.; Levin, A.; Feehally, J.; Harris, D.; Jindal, K.; Olanrewaju, T.O.; Samimi, A.; Olah, M.E.; Braam, B.; et al. Kidney care in low- and middle-income countries. Clin. Nephrol. 2019, 93, 21–30. [Google Scholar] [CrossRef]
- El Nahas, A.M.; Bello, A.K. Chronic kidney disease: The global challenge. Lancet 2005, 365, 331–340. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable a | Total n = 37 | Negative COVID n = 21 | Positive COVID n = 16 | p Value |
|---|---|---|---|---|
| Male | 24 (64.9) | 12 (57.2) | 12 (75) | 0.31 |
| Age (years) | 72 (54.5–79) | 72 (48–83.5) | 71 (55–80.9) | 0.79 |
| Weight (kg) | 63.5 (57.5–70.6) | 64.5 (58–69.3) | 63.5 (55.6–81.8) | 0.32 |
| BMI (kg/m2) | 23.3 (20.6–24.6) | 23.7 (20.8–24.5) | 23.3 (19.8–25.7) | 0.92 |
| Nephropathy: | - | |||
| Glomerular | 11 (29.7) | 5 (23.8) | 6 (37.5) | |
| Vascular | 8 (21.6) | 5 (23.8) | 3 (18.6) | |
| Tubular | 8 (21.6) | 7 (33.3) | 1 (6.3) | |
| Genetic | 2 (5.5) | 1 (4.8) | 1 (6.3) | |
| Not determined | 8 (21.6) | 3 (14.3) | 5 (31.3) | |
| Vascular access: | ||||
| Fistula | 26 (70.3) | 15 (71.4) | 11 (68.8) | 1 |
| Central catheter | 11 (29.7) | 6 (28.6) | 5 (31.2) | |
| Immunosuppression | 11 (29.6) | 7 (33.3) | 4 (28.6) | 1 |
| History of graft kidney | 7 (18.9) | 4 (19.1) | 3 (20) | 1 |
| Comorbidities | ||||
| Hypertension | 32 (86.5) | 19 (90.5) | 13 (81.3) | 0.63 |
| Congestive heart failure | 6 (12.5) | 4 (19.5) | 2 (12.5) | 0.68 |
| Coronary heart disease | 7 (18.9) | 2 (9.5) | 5 (31.2) | 0.2 |
| Peripheral vascular disease | 7 (18.9) | 3 (14.3) | 4 (25) | 0.44 |
| Cardiac arrhythmia | 12 (32.4) | 8 (40) | 4 (25) | 0.48 |
| Chronic respiratory disease | 4 (10.8) | 3 (14.3) | 1 (6.3) | 0.62 |
| Diabetes | 11 (30.6) | 7 (35) | 4 (25) | 0.72 |
| Cancer | 4 (10.8) | 1 (4.8) | 3 (18.8) | 0.3 |
| Smoker | 5 (13.9) | 4 (19.5) | 1 (6.3) | 0.35 |
| Medication: | ||||
| ACE inhibitors | 6 (16.2) | 2 (9.5) | 4 (25) | 0.17 |
| ARBs | 5 (13.5) | 3 (14.3) | 2 (12.5) | 1 |
| Beta blocker | 12 (32.4) | 6 (28.6) | 6 (37.5) | 0.73 |
| Calcium channel blockers | 10 (27.0) | 6 (28.6) | 4 (25) | 1 |
| Diuretic | 1 (2.7) | 0 | 1 (6.3) | 0.43 |
| Aspirin | 12 (32.4) | 7 (33.3) | 5 (31.3) | 1 |
| Clopidogrel | 3 (8.1) | 2 (9.5) | 1 (6.3) | 1 |
| VK | 9 (24.3) | 6 (28.6) | 3 (18.8) | 0.7 |
| Statin drug | 5 (13.5) | 1 (4.8) | 4 (25) | 0.14 |
| Steroids | 0 | 0 | 0 | - |
| ASEs | 27 (73) | 17 (61.9) | 10 (38.1) | 0.38 |
| March biological values | ||||
| Leukocyte (G/L) | 5.9 (4.6–6.5) | 5.8 (4.6–7.9) | 5.9 (4.7–6.2) | 0.54 |
| Neutrophil (G/L) | 3.6 (2.8–4.6) | 3.6 (3.1–5.3) | 3.6 (2.4–4.2) | 0.44 |
| Lymphocyte (G/L) | 1 (0.75–1.45) | 1 (0.6–1.2) | 1.2 (0.9–1.6) | 0.16 |
| Monocyte (G/L) | 0.6 (0.4–0.8) | 0.6 (0.45–0.9) | 0.5 (0.4–0.7) | 0.29 |
| Eosinophil (G/L) | 0.17 (0.01–0.33) | 0.17 (0.1–0.3) | 0.18 (0.11–0.35) | 0.44 |
| Platelet (G/L) | 189 (143–249) | 198 (149–258) | 179 (138–235) | 0.71 |
| Hemoglobin (g/dL) | 11.2 (10.4–11.6) | 11.2 (10–11.6) | 11.2 (10.6–11.8) | 0.78 |
| CRP (mg/L) | 4.7 (1.35–8.45) | 6.2 (2.8–9.9) | 2.3 (0.7–38.8) | 0.95 |
| Albumin (g/L) | 39.3 (37.2–42) | 39 (37.2–42) | 39.8 (37.2–42.3) | 0.47 |
| Potassium (mmol/L) | 4.5 (4.1–5.3) | 4.3 (4–5) | 5.1 (4.1–5.7) | 0.2 |
| Variables a | Negative COVID | Positive COVID | p Value |
|---|---|---|---|
| Leukocyte (G/L) | 7.4 (4.9–10.4) | 4.1 (3.3–7.1) | 0.0072 |
| Neutrophil (G/L) | 5.1 (3.3–8.1) | 2.7 (2.2–5.6) | 0.021 |
| Lymphocyte (G/L) | 0.85 (0.57–1.22) | 0.8 (0.55–1.05) | 0.29 |
| Monocyte (G/L) | 0.80 (0.47–0.92) | 0.5 (0.3–0.8) | 0.099 |
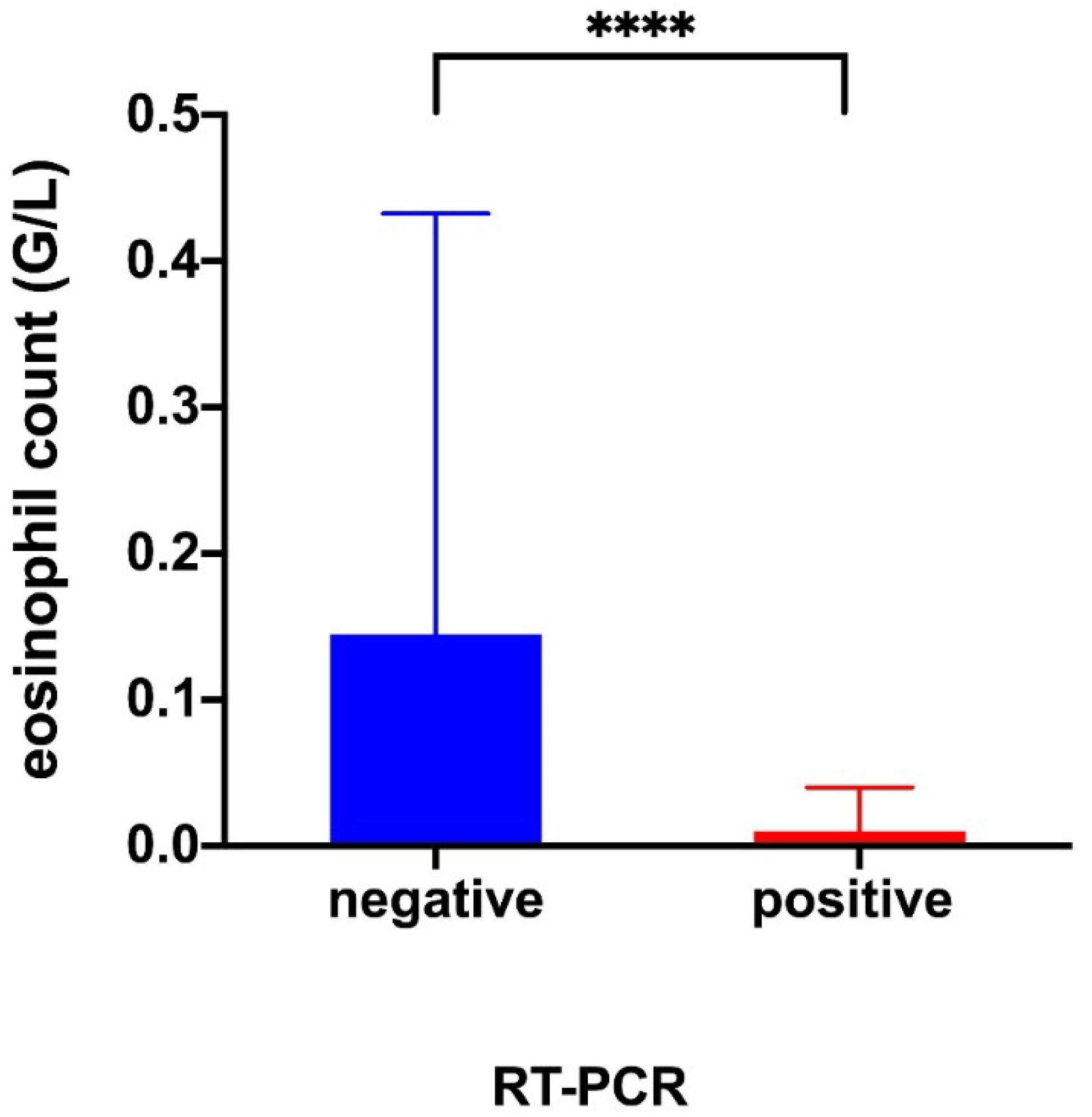
| Eosinophil (G/L) | 0.15 (0.06–0.43) | 0.01 (0–0.04) | 0.0003 |
| Platelet (G/L) | 201 (152–255) | 162 (118–185) | 0.077 |
| Hemoglobin (g/dL) | 11.1 (10.5–11.6) | 11.2 (10.4–12.4) | 0.81 |
| CRP (mg/L) | 13 (3.3–65.5) | 34.2 (15.9–72.8) | 0.57 |
| Albumin (g/L) | 40.5 (36.1–42.4) | 37.6 (34.2–41.5) | 0.24 |
| Potassium (mmol/L) | 4.6 (4.15–5.55) | 4.8 (4.1–5.1) | 0.32 |
| Variable a | Negative RT-PCR | p Value | Positive RT-PCR | p Value | ||
|---|---|---|---|---|---|---|
| Monthly Assessment | Suspicion Day | Monthly Assessment | Suspicion Day | |||
| Leukocyte (G/L) | 5.8 (4.6–7.9) | 7.4 (4.9–10.4) | 0.09 | 5.9 (4.7–6.2) | 4.1 (3.3–7.1) | 0.16 |
| Neutrophil (G/L) | 3.6 (3.1–5.3) | 5.1 (3.3–8.1) | 0.008 | 3.6 (2.4–4.2) | 2.7 (2.2–5.6) | 0.84 |
| Lymphocyte (G/L) | 1 (0.6–1.2) | 0.85 (0.57–1.22) | 0.30 | 1.2 (0.9–1.6) | 0.8 (0.55–1.05) | 0.001 |
| Monocyte (G/L) | 0.6 (0.45–0.9) | 0.8 (0.47–0.92) | 0.48 | 0.5 (0.4–0.7) | 0.5 (0.3–0.8) | 0.82 |
| Eosinophil (G/L) | 0.17 (0.1–0.3) | 0.15 (0.06–0.43) | 0.23 | 0.18 (0.11–0.35) | 0.01 (0–0.04) | <0.0001 |
| Platelet (G/L) | 198 (149–258) | 201 (152–255) | 0.64 | 179 (138–235) | 162 (118–185) | 0.004 |
| Hemoglobin (g/dL) | 11.2 (10–11.6) | 11.1 (10.5–11.6) | 0.24 | 11.2 (10.6–11.8) | 11.2 (10.4–12.4) | 0.71 |
| CRP (mg/L) | 6.2 (2.8–9.9) | 13 (3.3–65.5) | 0.02 | 2.3 (0.7–38.8) | 34.2 (15.9–72.8) | 0.001 |
| Albumin (g/L) | 39 (37.2–4) | 40.5 (36.1–42.4) | 0.38 | 39.8 (37.2–42.3) | 37.6 (34.2–41.5) | 0.07 |
| Potassium (mmol/L) | 4.3 (4–5) | 4.6 (4.15–5.6) | 0.16 | 5.1 (4.1–5.7) | 4.8 (4.1–5.1) | 0.27 |
| Effect Size | Value | 95% CI |
|---|---|---|
| Sensitivity | 0.82 | 0.59 to 0.94 |
| Specificity | 0.86 | 0.67 to 0.95 |
| Positive Predictive Value | 0.82 | 0.59 to 0.94 |
| Negative Predictive Value | 0.86 | 0.67 to 0.95 |
| Likelihood Ratio | 6.04 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vial, R.; Gully, M.; Bobot, M.; Scarfoglière, V.; Brunet, P.; Bouchouareb, D.; Duval, A.; Zino, H.-o.; Faraut, J.; Jehel, O.; et al. Triage of Patients Suspected of COVID-19 in Chronic Hemodialysis: Eosinophil Count Differentiates Low and High Suspicion of COVID-19. J. Clin. Med. 2021, 10, 4. https://doi.org/10.3390/jcm10010004
Vial R, Gully M, Bobot M, Scarfoglière V, Brunet P, Bouchouareb D, Duval A, Zino H-o, Faraut J, Jehel O, et al. Triage of Patients Suspected of COVID-19 in Chronic Hemodialysis: Eosinophil Count Differentiates Low and High Suspicion of COVID-19. Journal of Clinical Medicine. 2021; 10(1):4. https://doi.org/10.3390/jcm10010004
Chicago/Turabian StyleVial, Romain, Marion Gully, Mickael Bobot, Violaine Scarfoglière, Philippe Brunet, Dammar Bouchouareb, Ariane Duval, He-oh Zino, Julien Faraut, Océane Jehel, and et al. 2021. "Triage of Patients Suspected of COVID-19 in Chronic Hemodialysis: Eosinophil Count Differentiates Low and High Suspicion of COVID-19" Journal of Clinical Medicine 10, no. 1: 4. https://doi.org/10.3390/jcm10010004
APA StyleVial, R., Gully, M., Bobot, M., Scarfoglière, V., Brunet, P., Bouchouareb, D., Duval, A., Zino, H.-o., Faraut, J., Jehel, O., Berdad-Haddad, Y., Burtey, S., Jarrot, P.-A., Lano, G., & Robert, T. (2021). Triage of Patients Suspected of COVID-19 in Chronic Hemodialysis: Eosinophil Count Differentiates Low and High Suspicion of COVID-19. Journal of Clinical Medicine, 10(1), 4. https://doi.org/10.3390/jcm10010004