The Severity of Diabetic Retinopathy Is an Independent Factor for the Progression of Diabetic Nephropathy



 ,
, 
Abstract
1. Introduction
2. Materials and Methods
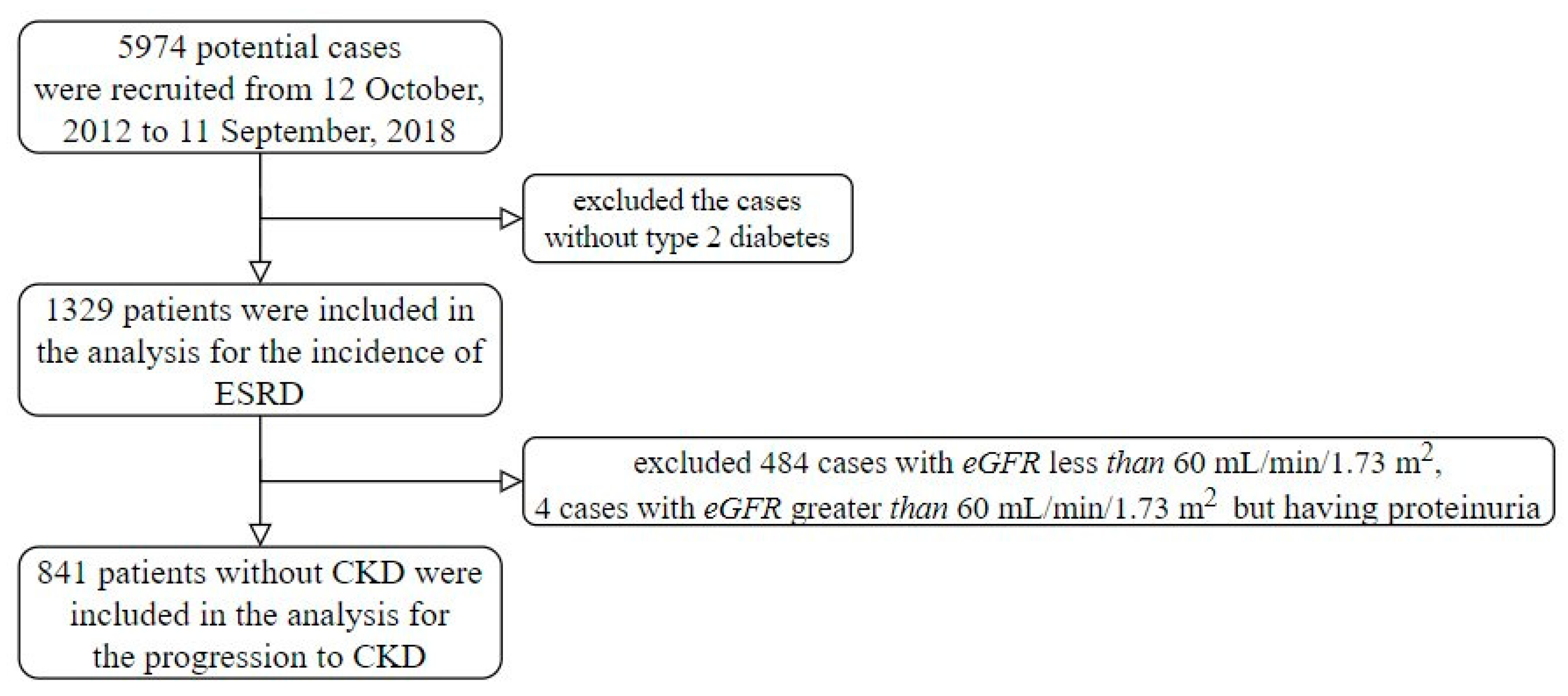
2.1. Population
2.2. Measurements and Variables
2.3. Deep Learning Model for Grading Diabetic Retinopathy
2.4. Statistical Analysis and Model Performance Assessment
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- The Diabetes Control and Complications (DCCT) Research Group. Effect of intensive therapy on the development and progression of diabetic nephropathy in the diabetes control and complications trial. Kidney Int. 1995, 47, 1703–1720. [Google Scholar] [CrossRef] [PubMed]
- Turner, R.C.; Holman, R.R.; Stratton, I.M.; Cull, C.A.; Matthews, D.R.; Manley, S.E.; Frighi, V.; Wright, A.D.; Neil, A.; Kohner, E.; et al. Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). Lancet 1998, 352, 854–865. [Google Scholar]
- Mathiesen, E.; Rønn, B.; Storm, B.; Foght, H.; Deckert, T. The natural course of microalbuminuria in insulin-dependent diabetes: A 10-year prospective study. Diabet. Med. 1995, 12, 482–487. [Google Scholar] [CrossRef] [PubMed]
- Hung, C.-C.; Lin, H.Y.-H.; Hwang, D.-Y.; Kuo, I.-C.; Chiu, Y.-W.; Lim, L.-M.; Hwang, S.-J.; Chen, H.-C. Diabetic retinopathy and clinical parameters favoring the presence of diabetic nephropathy could predict renal outcome in patients with diabetic kidney disease. Sci. Rep. 2017, 7, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Jiang, G.; Luk, A.O.Y.; Tam, C.H.T.; Xie, F.; Carstensen, B.; Lau, E.S.H.; Lim, C.K.P.; Lee, H.M.; Ng, A.C.W.; Ng, M.C.Y.; et al. Progression of diabetic kidney disease and trajectory of kidney function decline in Chinese patients with type 2 diabetes. Kidney Int. 2019, 95, 178–187. [Google Scholar] [CrossRef]
- Park, H.C.; Lee, Y.-K.; Cho, A.; Hoon Han, C.; Noh, J.-W.; Shin, Y.J.; Bae, S.H.; Kim, H. Diabetic retinopathy is a prognostic factor for progression of chronic kidney disease in the patients with type 2 diabetes mellitus. PLoS ONE 2019, 14, e0220506. [Google Scholar] [CrossRef]
- Rodriguez-Poncelas, A.; Mundet-Tuduri, X.; Miravet-Jimenez, S.; Casellas, A.; Barrot-De la Puente, J.F.; Franch-Nadal, J.; Coll-de Tuero, G. Chronic kidney disease and diabetic retinopathy in patients with type 2 diabetes. PLoS ONE 2016, 11, e0149448. [Google Scholar] [CrossRef]
- Lin, H.-T.; Zheng, C.-M.; Wu, Y.-C.; Chang, Y.-H.; Chen, J.-T.; Liang, C.-M.; Chang, T.-J.; Zheng, J.-Q.; Tai, M.-C.; Lin, Y.-F. Diabetic retinopathy as a risk factor for chronic kidney disease progression: A multicenter case–control study in Taiwan. Nutrients 2019, 11, 509. [Google Scholar] [CrossRef]
- Yamanouchi, M.; Mori, M.; Hoshino, J.; Kinowaki, K.; Fujii, T.; Ohashi, K.; Furuichi, K.; Wada, T.; Ubara, Y. Retinopathy progression and the risk of end-stage kidney disease: Results from a longitudinal Japanese cohort of 232 patients with type 2 diabetes and biopsy-proven diabetic kidney disease. BMJ Open Diabetes Res. Care 2019, 7, e000726. [Google Scholar] [CrossRef]
- Wong, T.Y.; Sun, J.; Kawasaki, R.; Ruamviboonsuk, P.; Gupta, N.; Lansingh, V.C.; Maia, M.; Mathenge, W.; Moreker, S.; Muqit, M.M.K.; et al. Guidelines on diabetic eye care: The international council of ophthalmology recommendations for screening, follow-up, referral, and treatment based on resource settings. Ophthalmology 2018, 125, 1608–1622. [Google Scholar] [CrossRef]
- Hogg, R.J.; Furth, S.; Lemley, K.V.; Portman, R.; Schwartz, G.J.; Coresh, J.; Balk, E.; Lau, J.; Levin, A.; Kausz, A.T.; et al. National kidney foundation’s kidney disease outcomes quality initiative clinical practice guidelines for chronic kidney disease in children and adolescents: Evaluation, classification, and stratification. Pediatrics 2003, 111, 1416–1421. [Google Scholar] [CrossRef] [PubMed]
- SStevens, P.E.; Levin, A. Evaluation and management of chronic kidney disease: Synopsis of the kidney disease: Improving global outcomes 2012 clinical practice guideline. Ann. Intern. Med. 2013, 158, 825–830. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.kaggle.com/c/diabetic-retinopathy-detection (accessed on 12 June 2020).
- Hu, J.; Shen, L.; Sun, G. Squeeze-and-excitation networks. In Proceedings of the IEEE Conference on Computer Vision And Pattern Recognition, Salt Lake City, UT, USA, 18–23 June 2018; pp. 7132–7141. [Google Scholar]
- Simpson, A.J. Over-sampling in a deep neural network. arXiv 2015, arXiv:1502.03648. [Google Scholar]
- LLin, C.; Hsu, C.J.; Lou, Y.S.; Yeh, S.J.; Lee, C.C.; Su, S.L.; Chen, H.C. Artificial intelligence learning semantics via external resources for classifying diagnosis codes in discharge notes. J. Med. Internet Res. 2017, 19, e380. [Google Scholar] [CrossRef] [PubMed]
- Gross, S.; Wilber, M. Training and Investigating Residual Nets. Facebook AI Research, CA. 2016. Available online: http://torch.ch/blog/2016/02/04/resnets.html (accessed on 12 June 2020).
- He, F.; Xia, X.; Wu, X.; Yu, X.; Huang, F. Diabetic Retinopathy in Predicting Diabetic Nephropathy in Patients with Type 2 Diabetes and Renal Disease: A Meta-Analysis; Springer: Berlin, Germany, 2013. [Google Scholar]
- El-Asrar, A.M.A.; Al-Rubeaan, K.A.; Al-Amro, S.A.; Moharram, O.A.; Kangave, D. Retinopathy as a predictor of other diabetic complications. Int. Ophthalmol. 2001, 24, 1–11. [Google Scholar] [CrossRef]
- Sasso, F.C.; Pafundi, P.C.; Gelso, A.; Bono, V.; Costagliola, C.; Marfella, R.; Sardu, C.; Rinaldi, L.; Galiero, R.; Acierno, C.J.N.; et al. Relationship between albuminuric CKD and diabetic retinopathy in a real-world setting of type 2 diabetes: Findings from no blind study. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 923–930. [Google Scholar] [CrossRef]
- Jadawji, C.; Crasto, W.; Gillies, C.; Kar, D.; Davies, M.J.; Khunti, K.; Seidu, S. Prevalence and progression of diabetic nephropathy in South Asian, white European and African Caribbean people with type 2 diabetes: A systematic review and meta-analysis. Diabetes Obes. Metab. 2019, 21, 658–673. [Google Scholar] [CrossRef]
- Wei, L.; Xiao, Y.; Li, L.; Xiong, X.; Han, Y.; Zhu, X.; Sun, L. The Susceptibility genes in diabetic nephropathy. Kidney Dis. 2018, 4, 226–237. [Google Scholar] [CrossRef]
- Bello, N.A.; Pfeffer, M.A.; Skali, H.; McGill, J.B.; Rossert, J.; Olson, K.A.; Weinrauch, L.; Cooper, M.E.; de Zeeuw, D.; Rossing, P.; et al. Retinopathy and clinical outcomes in patients with type 2 diabetes mellitus, chronic kidney disease, and anemia. BMJ Open Diabetes Res. Care 2014, 2, e000011. [Google Scholar] [CrossRef]
- Penno, G.; Solini, A.; Zoppini, G.; Orsi, E.; Zerbini, G.; Trevisan, R.; Gruden, G.; Cavalot, F.; Laviola, L.; Morano, S.; et al. Rate and determinants of association between advanced retinopathy and chronic kidney disease in patients with type 2 diabetes: The Renal Insufficiency And Cardiovascular Events (RIACE) Italian multicenter study. Diabetes Care 2012, 35, 2317–2323. [Google Scholar] [CrossRef]
- Cooper, M.E. Pathogenesis, prevention, and treatment of diabetic nephropathy. Lancet 1998, 352, 213–219. [Google Scholar] [CrossRef]
- Gross, J.L.; De Azevedo, M.J.; Silveiro, S.P.; Canani, L.H.; Caramori, M.L.; Zelmanovitz, T. Diabetic nephropathy: Diagnosis, prevention, and treatment. Diabetes Care 2005, 28, 164–176. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Ortega, M.; Rodrigues-Diez, R.R.; Lavoz, C.; Rayego-Mateos, S. Special Issue “Diabetic Nephropathy: Diagnosis, Prevention and Treatment”; Multidisciplinary Digital Publishing Institute: Basel, Switzerland, 2020. [Google Scholar]
- Bello, A.K.; Alrukhaimi, M.; Ashuntantang, G.E.; Bellorin-Font, E.; Gharbi, M.B.; Braam, B.; Feehally, J.; Harris, D.C.; Jha, V.; Jindal, K.; et al. Global overview of health systems oversight and financing for kidney care. Kidney Int. Suppl. 2018, 8, 41–51. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Initial Grades of Diabetic Nephropathy | ||||||
|---|---|---|---|---|---|---|
| Stage 1 (n = 400) | Stage 2 (n = 445) | Stage 3 (n = 294) | Stage 4 (n = 103) | Stage 5 (n = 87) | p-Value # | |
| Basic characteristics | ||||||
| DR severity | <0.001 | |||||
| No DR | 175 (43.8%) | 193 (43.4%) | 93 (31.6%) | 21 (20.4%) | 21 (24.1%) | |
| Mild NPDR | 73 (18.2%) | 69 (15.5%) | 56 (19.0%) | 25 (24.3%) | 20 (23.0%) | |
| Moderate NPDR | 106 (26.5%) | 114 (25.6%) | 94 (32.0%) | 36 (35.0%) | 28 (32.2%) | |
| Severe NPDR | 39 (9.8%) | 59 (13.3%) | 42 (14.3%) | 16 (15.5%) | 14 (16.1%) | |
| PDR | 7 (1.8%) | 10 (2.2%) | 9 (3.1%) | 5 (4.9%) | 4 (4.6%) | |
| Gender | 0.222 | |||||
| Female | 171 (42.8%) | 222 (49.9%) | 147 (50.0%) | 46 (44.7%) | 40 (46.0%) | |
| Male | 229 (57.2%) | 223 (50.1%) | 147 (50.0%) | 57 (55.3%) | 47 (54.0%) | |
| Age (years) | 57.58 ± 12.88 | 65.92 ± 11.29 | 67.12 ± 12.45 | 65.01 ± 11.71 | 60.91 ± 12.05 | <0.001 |
| Height (cm) | 162.48 ± 9.05 | 161.84 ± 8.77 | 161.94 ± 8.60 | 162.24 ± 8.59 | 163.25 ± 8.73 | 0.625 |
| Weight (kg) | 69.05 ± 15.04 | 66.27 ± 13.09 | 67.62 ± 14.27 | 67.20 ± 12.73 | 67.24 ± 13.01 | 0.076 |
| Body mass index | 26.06 ± 4.97 | 25.20 ± 4.01 | 25.74 ± 4.97 | 25.47 ± 3.96 | 25.21 ± 4.31 | 0.074 |
| SBP (mmHg) | 138.75 ± 21.51 | 141.20 ± 21.45 | 141.94 ± 22.83 | 138.43 ± 23.45 | 141.99 ± 22.58 | 0.235 |
| DBP (mmHg) | 80.56 ± 12.52 | 79.36 ± 12.55 | 78.20 ± 12.59 | 77.19 ± 11.43 | 77.95 ± 13.46 | 0.039 |
| Comorbidity | ||||||
| Hypertension | 120 (30.0%) | 166 (37.3%) | 137 (46.6%) | 53 (51.5%) | 48 (55.2%) | <0.001 |
| lipidemia | 128 (32.0%) | 132 (29.7%) | 87 (29.6%) | 33 (32.0%) | 30 (34.5%) | 0.850 |
| Ischemic heart disease | 81 (20.2%) | 95 (21.3%) | 77 (26.2%) | 25 (24.3%) | 33 (37.9%) | 0.005 |
| Heart failure | 41 (10.2%) | 40 (9.0%) | 31 (10.5%) | 8 (7.8%) | 11 (12.6%) | 0.760 |
| COPD | 7 (1.8%) | 7 (1.6%) | 12 (4.1%) | 4 (3.9%) | 1 (1.1%) | 0.128 |
| Stroke | 66 (13.1%) | 25 (10.3%) | 52 (13.8%) | 23 (13.5%) | 5 (14.3%) | 0.734 |
| Diabetic neuropathy | 38 (9.5%) | 35 (7.9%) | 23 (7.8%) | 12 (11.7%) | 7 (8.0%) | 0.703 |
| Laboratory test | ||||||
| HbA1c (%) | 8.21 ± 2.07 | 7.80 ± 1.85 | 8.19 ± 2.10 | 7.78 ± 1.78 | 7.95 ± 2.05 | 0.014 |
| Last Glu AC (mg/dL) | 149.85 ± 56.80 | 145.87 ± 58.83 | 149.61 ± 58.06 | 150.43 ± 68.97 | 140.93 ± 51.79 | 0.617 |
| Triglyceride (mg/dL) | 151.19 ± 126.72 | 153.36 ± 139.92 | 160.72 ± 93.66 | 175.69 ± 89.07 | 172.44 ± 119.66 | 0.251 |
| Total Cholesterol (mg/dL) | 171.80 ± 39.92 | 170.43 ± 38.57 | 169.38 ± 46.76 | 179.24 ± 52.56 | 174.89 ± 61.73 | 0.321 |
| LDL Cholesterol (mg/dL) | 102.95 ± 33.15 | 100.64 ± 31.83 | 98.45 ± 36.81 | 98.70 ± 37.67 | 97.39 ± 47.30 | 0.416 |
| HDL Cholesterol (mg/dL) | 47.44 ± 13.33 | 46.77 ± 13.41 | 45.33 ± 11.83 | 45.00 ± 12.62 | 46.05 ± 13.61 | 0.192 |
| Creatinine (mg/dL) | 0.69 ± 0.14 | 0.93 ± 0.16 | 1.43 ± 0.30 | 2.83 ± 0.68 | 7.26 ± 2.81 | <0.001 |
| Uric Acid (mg/dL) | 5.50 ± 1.47 | 5.85 ± 1.58 | 6.64 ± 1.93 | 7.24 ± 1.87 | 7.24 ± 2.51 | <0.001 |
| Hemoglobin (g/dL) | 13.24 ± 1.76 | 13.03 ± 1.79 | 12.17 ± 1.88 | 10.62 ± 1.88 | 10.21 ± 1.51 | <0.001 |
| Albumin (g/dL) | 3.88 ± 0.61 | 3.89 ± 0.57 | 3.79 ± 0.57 | 3.63 ± 0.57 | 3.47 ± 0.60 | <0.001 |
| Result | ||||||
| ESRD event | 4 (1.0%) | 3 (0.7%) | 22 (7.5%) | 23 (22.3%) | 17 (19.5%) | <0.001 |
| Time to ESRD (years) | 1.90 ± 1.53 | 2.05 ± 1.60 | 2.10 ± 1.53 | 1.83 ± 1.49 | 1.68 ± 1.29 | 0.080 |
| Initial Grades of Diabetic Retinopathy | ||||||
|---|---|---|---|---|---|---|
| No DR (n = 503) | Mild NPDR (n = 243) | Moderate NPDR (n = 378) | Severe NPDR (n = 170) | PDR (n = 35) | p-Value # | |
| Basic characteristics | ||||||
| Body mass index | 25.47 ± 4.27 | 25.89 ± 5.24 | 25.27 ± 4.28 | 26.18 ± 4.97 | 26.19 ± 4.22 | 0.152 |
| SBP (mmHg) | 138.85 ± 20.27 | 142.08 ± 22.72 | 141.37 ± 22.84 | 139.75 ± 22.69 | 146.14 ± 27.50 | 0.127 |
| DBP (mmHg) | 78.89 ± 12.26 | 78.33 ± 11.62 | 79.90 ± 13.04 | 79.54 ± 13.01 | 80.57 ± 15.44 | 0.527 |
| Comorbidity | ||||||
| lipidemia | 144 (28.6%) | 71 (29.2%) | 120 (31.7%) | 58 (34.1%) | 17 (48.6%) | 0.107 |
| Ischemic heart disease | 116 (23.1%) | 56 (23.0%) | 87 (23.0%) | 47 (27.6%) | 5 (14.3%) | 0.491 |
| Heart failure | 49 (9.7%) | 20 (8.2%) | 41 (10.8%) | 20 (11.8%) | 1 (2.9%) | 0.466 |
| COPD | 18 (3.6%) | 5 (2.1%) | 4 (1.1%) | 2 (1.2%) | 2 (5.7%) | 0.051 |
| Stroke | 54 (13.5%) | 48 (10.8%) | 42 (14.3%) | 18 (17.5%) | 9 (10.3%) | 0.305 |
| Diabetic neuropathy | 29 (5.8%) | 26 (10.7%) | 39 (10.3%) | 15 (8.8%) | 6 (17.1%) | 0.018 |
| Laboratory test | ||||||
| HbA1c (%) | 7.69 ± 1.89 | 8.03 ± 1.86 | 8.29 ± 2.01 | 8.39 ± 2.27 | 7.88 ± 1.91 | <0.001 |
| Last Glu AC (mg/dL) | 143.29 ± 56.77 | 147.54 ± 55.95 | 151.82 ± 58.95 | 154.43 ± 65.91 | 143.43 ± 52.26 | 0.127 |
| Triglyceride (mg/dL) | 151.11 ± 111.56 | 155.49 ± 91.32 | 161.08 ± 129.90 | 170.54 ± 167.13 | 154.26 ± 106.63 | 0.444 |
| Total Cholesterol (mg/dL) | 170.58 ± 40.67 | 170.15 ± 45.89 | 172.11 ± 43.82 | 174.39 ± 48.75 | 176.74 ± 50.41 | 0.780 |
| LDL Cholesterol (mg/dL) | 99.70 ± 32.53 | 101.10 ± 37.07 | 99.40 ± 34.29 | 102.86 ± 38.61 | 107.66 ± 43.68 | 0.568 |
| HDL Cholesterol (mg/dL) | 47.31 ± 13.67 | 46.10 ± 12.27 | 45.98 ± 12.74 | 45.12 ± 12.60 | 48.71 ± 13.01 | 0.223 |
| Creatinine (mg/dL) | 1.28 ± 1.52 | 1.71 ± 2.09 | 1.63 ± 1.78 | 1.69 ± 1.68 | 2.15 ± 2.93 | 0.001 |
| Uric Acid (mg/dL) | 5.80 ± 1.67 | 6.16 ± 1.79 | 6.35 ± 2.04 | 6.33 ± 1.77 | 6.80 ± 1.55 | <0.001 |
| Hemoglobin (g/dL) | 12.96 ± 1.85 | 12.53 ± 1.99 | 12.20 ± 2.12 | 12.23 ± 2.10 | 11.38 ± 1.94 | <0.001 |
| Albumin (g/dL) | 3.89 ± 0.54 | 3.82 ± 0.57 | 3.77 ± 0.64 | 3.74 ± 0.63 | 3.66 ± 0.64 | 0.004 |
| Result | ||||||
| ESRD event | 11 (2.2%) | 11 (4.5%) | 34 (9.0%) | 9 (5.3%) | 4 (11.4%) | <0.001 |
| Time to ESRD (years) | 2.22 ± 1.65 | 2.01 ± 1.50 | 1.60 ± 1.36 | 2.06 ± 1.51 | 1.82 ± 1.53 | <0.001 |
| Crude-HR (95% CI) | p-Value | Adj-HR (95% CI) | p-Value # | |
|---|---|---|---|---|
| Initial DR grade | <0.001 | 0.103 | ||
| No DR | 1.00 | 1.00 | ||
| Mild NPDR | 2.35 (1.01–5.43) | 0.046 | 1.51 (0.63–3.62) | 0.355 |
| Moderate NPDR | 5.96 (2.99–11.89) | <0.001 | 2.63 (1.25–5.50) | 0.010 |
| Severe NPDR | 2.79 (1.16–6.75) | 0.023 | 1.58 (0.62–3.99) | 0.335 |
| PDR | 6.98 (2.22–21.94) | 0.001 | 1.87 (0.56–6.19) | 0.308 |
| Initial CKD grade | <0.001 | <0.001 | ||
| 1 | 1.00 | 1.00 | ||
| 2 | 0.42 (0.08–2.31) | 0.321 | 0.67 (0.12–3.69) | 0.642 |
| 3 | 8.27 (2.67–25.62) | <0.001 | 13.87 (4.42–43.54) | <0.001 |
| 4 | 27.37 (8.83–84.86) | <0.001 | 39.10 (12.54–121.88) | <0.001 |
| 5 | 30.27 (9.54–96.09) | <0.001 | 32.87 (10.36–104.21) | <0.001 |
| Gender | 0.252 | 0.956 | ||
| Female | 1.00 | 1.00 | ||
| Male | 1.33 (0.81–2.19) | 0.252 | 1.01 (0.61–1.67) | 0.956 |
| age | 0.62 (0.51–0.76) | <0.001 | 0.55 (0.44–0.70) | <0.001 |
| height | 1.18 (0.92–1.51) | 0.184 | 0.96 (0.71–1.30) | 0.804 |
| weight | 0.95 (0.74–1.21) | 0.669 | 0.88 (0.50–1.57) | 0.676 |
| Body mass index | 0.86 (0.67–1.11) | 0.254 | 0.85 (0.65–1.11) | 0.230 |
| SBP | 0.91 (0.72–1.15) | 0.439 | 0.91 (0.73–1.12) | 0.359 |
| DBP | 0.98 (0.77–1.25) | 0.877 | 0.88 (0.68–1.13) | 0.311 |
| Comorbidity | ||||
| Hypertension | 2.68 (1.62–4.41) | <0.001 | 1.59 (0.95–2.66) | 0.075 |
| lipidemia | 1.33 (0.82–2.18) | 0.249 | 1.16 (0.70–1.92) | 0.568 |
| Ischemic heart disease | 2.10 (1.29–3.41) | 0.003 | 1.79 (1.08–2.97) | 0.025 |
| Stroke | 1.44 (0.73–2.82) | 0.293 | 1.46 (0.73–2.92) | 0.287 |
| Diabetic neuropathy | 1.71 (0.89–3.28) | 0.106 | 1.35 (0.67–2.70) | 0.401 |
| Heart failure | 2.18 (1.19–4.01) | 0.012 | 1.91 (1.01–3.60) | 0.047 |
| Laboratory test | ||||
| HbA1c | 1.07 (0.86–1.33) | 0.567 | 1.00 (0.79–1.27) | 0.995 |
| Glu AC | 1.06 (0.87–1.31) | 0.555 | 0.90 (0.76–1.08) | 0.266 |
| triglyceride | 1.01 (0.95–1.06) | 0.784 | 0.97 (0.91–1.03) | 0.343 |
| total Cholesterol | 1.12 (0.98–1.29) | 0.099 | 1.15 (0.94–1.41) | 0.174 |
| LDL Cholesterol | 1.51 (1.26–1.82) | <0.001 | 1.23 (1.02–1.50) | 0.033 |
| HDL Cholesterol | 0.95 (0.74–1.21) | 0.653 | 0.83 (0.65–1.05) | 0.119 |
| Creatinine | 1.54 (1.38–1.72) | <0.001 | 0.76 (0.52–1.12) | 0.163 |
| Hemoglobin | 0.38 (0.30–0.49) | <0.001 | 0.75 (0.56–1.00) | 0.049 |
| Initial Grades of Diabetic Retinopathy | ||||||
|---|---|---|---|---|---|---|
| No DR (n = 368) | Mild NPDR (n = 141) | Moderate NPDR (n = 218) | Severe NPDR (n = 97) | PDR (n = 17) | p-Value # | |
| Basic characteristics | ||||||
| Gender | 0.393 | |||||
| Female | 182 (49.5%) | 64 (45.4%) | 94 (43.1%) | 41 (42.3%) | 10 (58.8%) | |
| Male | 186 (50.5%) | 77 (54.6%) | 124 (56.9%) | 56 (57.7%) | 7 (41.2%) | |
| Age (years) | 64.06 ± 13.90 | 61.69 ± 13.41 | 60.54 ± 10.28 | 58.58 ± 11.67 | 58.33 ± 10.10 | <0.001# |
| Height (cm) | 161.63 ± 8.85 | 162.10 ± 9.88 | 162.42 ± 8.37 | 163.57 ± 8.82 | 161.79 ± 9.63 | 0.298# |
| Weight (kg) | 66.80 ± 13.83 | 68.17 ± 13.78 | 67.42 ± 13.71 | 70.05 ± 15.96 | 68.61 ± 17.14 | 0.451# |
| Body mass index | 25.45 ± 4.17 | 26.01 ± 5.65 | 25.43 ± 4.11 | 26.03 ± 4.92 | 25.86 ± 4.17 | 0.915# |
| SBP (mmHg) | 138.25 ± 19.87 | 141.94 ± 22.66 | 141.49 ± 21.90 | 138.48 ± 22.54 | 152.76 ± 28.80 | 0.082# |
| DBP (mmHg) | 79.24 ± 12.37 | 79.92 ± 11.04 | 80.76 ± 12.60 | 79.70 ± 13.97 | 85.12 ± 18.14 | 0.418# |
| Comorbidity | ||||||
| Hypertension | 119 (32.3%) | 51 (36.2%) | 72 (33.0%) | 35 (36.1%) | 6 (35.3%) | 0.910 |
| lipidemia | 100 (27.2%) | 38 (27.0%) | 75 (34.4%) | 35 (36.1%) | 9 (52.9%) | 0.044 |
| Ischemic heart disease | 74 (20.1%) | 34 (24.1%) | 47 (21.6%) | 19 (19.6%) | 1 (5.9%) | 0.501 |
| Heart failure | 31 (8.4%) | 9 (6.4%) | 26 (11.9%) | 12 (12.4%) | 1 (5.9%) | 0.31 |
| COPD | 10 (2.7%) | 2 (1.4%) | 2 (0.9%) | 0 (0.0%) | 0 (0.0%) | 0.372 |
| Stroke | 48 (13.0%) | 17 (12.1%) | 24 (11.0%) | 11 (11.3%) | 1 (5.9%) | 0.937 |
| Diabetic neuropathy | 23 (6.2%) | 17 (12.1%) | 21 (9.6%) | 9 (9.3%) | 2 (11.8%) | 0.185 |
| Laboratory test | ||||||
| HbA1c (%) | 7.72 ± 1.92 | 7.99 ± 1.97 | 8.24 ± 1.79 | 8.54 ± 2.36 | 7.78 ± 1.97 | <0.001 |
| Last Glu AC (mg/dL) | 144.12 ± 57.86 | 148.18 ± 53.03 | 150.22 ± 54.92 | 159.10 ± 71.30 | 123.53 ± 38.11 | 0.039 |
| Triglyceride (mg/dL) | 146.60 ± 118.68 | 150.05 ± 86.88 | 156.59 ± 153.53 | 170.53 ± 194.11 | 140.65 ± 69.66 | 0.776 |
| Total Cholesterol (mg/dL) | 171.83 ± 36.93 | 170.57 ± 41.43 | 169.39 ± 40.84 | 171.63 ± 40.85 | 177.59 ± 34.86 | 0.676 |
| LDL Cholesterol (mg/dL) | 101.95 ± 30.79 | 103.56 ± 36.36 | 98.59 ± 31.45 | 103.44 ± 33.64 | 115.35 ± 38.22 | 0.398 |
| HDL Cholesterol (mg/dL) | 48.18 ± 13.97 | 46.12 ± 11.95 | 46.82 ± 13.57 | 44.25 ± 11.60 | 50.82 ± 12.79 | 0.083 |
| Uric Acid (mg/dL) | 5.56 ± 1.46 | 5.64 ± 1.43 | 5.70 ± 1.65 | 6.03 ± 1.63 | 6.08 ± 1.38 | 0.118 |
| Hemoglobin (g/dL) | 13.28 ± 1.66 | 13.35 ± 1.75 | 12.91 ± 1.87 | 13.08 ± 1.77 | 11.41 ± 2.13 | 0.001 |
| Albumin (g/dL) | 3.91 ± 0.55 | 3.90 ± 0.58 | 3.85 ± 0.64 | 3.87 ± 0.59 | 3.82 ± 0.63 | 0.895 |
| Result | ||||||
| CKD event | 5 (1.4%) | 5 (3.5%) | 11 (5.0%) | 7 (7.2%) | 1 (5.9%) | 0.012 |
| Time to CKD (years) | 2.19 ± 1.65 | 2.05 ± 1.58 | 1.58 ± 1.38 | 2.19 ± 1.53 | 1.47 ± 1.15 | <0.001 |
| Crude-HR (95% CI) | p-Value | Adj-HR (95% CI) | p-Value # | |
|---|---|---|---|---|
| Initial DR grade | 0.004 | 0.012 | ||
| No DR | 1.00 | 1.00 | ||
| Mild NPDR | 3.46 (0.92–12.98) | 0.066 | 3.38 (0.90–12.71) | 0.072 |
| Moderate NPDR | 8.75 (2.74–27.92) | <0.001 | 7.88 (2.43–25.57) | 0.001 |
| Severe NPDR | 5.73 (1.64–20.04) | 0.006 | 5.08 (1.35–19.04) | 0.016 |
| PDR | 14.21 (1.55–130.67) | 0.019 | 11.43 (1.22–107.12) | 0.033 |
| Gender | 0.802 | 0.835 | ||
| Female | 1.00 | 1.00 | ||
| Male | 0.91 (0.42–1.97) | 0.802 | 0.92 (0.42–2.00) | 0.835 |
| age | 0.79 (0.57–1.09) | 0.148 | 0.69 (0.48–1.00) | 0.047 |
| height | 0.80 (0.54–1.18) | 0.263 | 0.69 (0.46–1.04) | 0.077 |
| weight | 0.92 (0.65–1.30) | 0.646 | 0.56 (0.32–0.99) | 0.046 |
| Body mass index | 1.03 (0.71–1.49) | 0.866 | 0.98 (0.67–1.42) | 0.913 |
| SBP | 1.15 (0.81–1.64) | 0.438 | 1.14 (0.81–1.60) | 0.463 |
| DBP | 1.13 (0.79–1.62) | 0.505 | 1.02 (0.70–1.48) | 0.937 |
| Comorbidity | ||||
| Hypertension | 1.51 (0.71–3.22) | 0.286 | 1.42 (0.65–3.12) | 0.381 |
| lipidemia | 1.12 (0.50–2.52) | 0.790 | 1.18 (0.51–2.70) | 0.699 |
| Ischemic heart disease | 0.91 (0.36–2.33) | 0.847 | 1.01 (0.39–2.58) | 0.987 |
| Stroke | 0.48 (0.11–2.11) | 0.332 | 0.73 (0.16–3.23) | 0.674 |
| Diabetic neuropathy | 0.83 (0.24–2.88) | 0.772 | 0.66 (0.16–2.72) | 0.563 |
| Heart failure | 3.45 (1.43–8.29) | 0.006 | 3.47 (1.43–8.40) | 0.006 |
| Laboratory test | ||||
| HbA1c | 1.29 (0.97–1.71) | 0.079 | 1.23 (0.88–1.73) | 0.233 |
| Glu AC | 1.03 (0.75–1.42) | 0.852 | 0.96 (0.67–1.38) | 0.832 |
| triglyceride | 1.04 (0.79–1.38) | 0.765 | 1.04 (0.80–1.37) | 0.754 |
| total Cholesterol | 1.75 (1.17–2.59) | 0.006 | 1.68 (1.10–2.54) | 0.015 |
| LDL Cholesterol | 1.92 (1.32–2.78) | 0.001 | 1.85 (1.24–2.77) | 0.003 |
| HDL Cholesterol | 1.03 (0.71–1.49) | 0.886 | 0.98 (0.66–1.45) | 0.921 |
| Hemoglobin | 0.67 (0.45–1.00) | 0.053 | 0.67 (0.45–1.00) | 0.053 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsing, S.-C.; Lee, C.-C.; Lin, C.; Chen, J.-T.; Chen, Y.-H.; Fang, W.-H. The Severity of Diabetic Retinopathy Is an Independent Factor for the Progression of Diabetic Nephropathy. J. Clin. Med. 2021, 10, 3. https://doi.org/10.3390/jcm10010003
Hsing S-C, Lee C-C, Lin C, Chen J-T, Chen Y-H, Fang W-H. The Severity of Diabetic Retinopathy Is an Independent Factor for the Progression of Diabetic Nephropathy. Journal of Clinical Medicine. 2021; 10(1):3. https://doi.org/10.3390/jcm10010003
Chicago/Turabian StyleHsing, Shi-Chue, Chia-Cheng Lee, Chin Lin, Jiann-Torng Chen, Yi-Hao Chen, and Wen-Hui Fang. 2021. "The Severity of Diabetic Retinopathy Is an Independent Factor for the Progression of Diabetic Nephropathy" Journal of Clinical Medicine 10, no. 1: 3. https://doi.org/10.3390/jcm10010003
APA StyleHsing, S.-C., Lee, C.-C., Lin, C., Chen, J.-T., Chen, Y.-H., & Fang, W.-H. (2021). The Severity of Diabetic Retinopathy Is an Independent Factor for the Progression of Diabetic Nephropathy. Journal of Clinical Medicine, 10(1), 3. https://doi.org/10.3390/jcm10010003