
Cumulative Fluid Balance during Extracorporeal Membrane Oxygenation and Mortality in Patients with Acute Respiratory Distress Syndrome

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
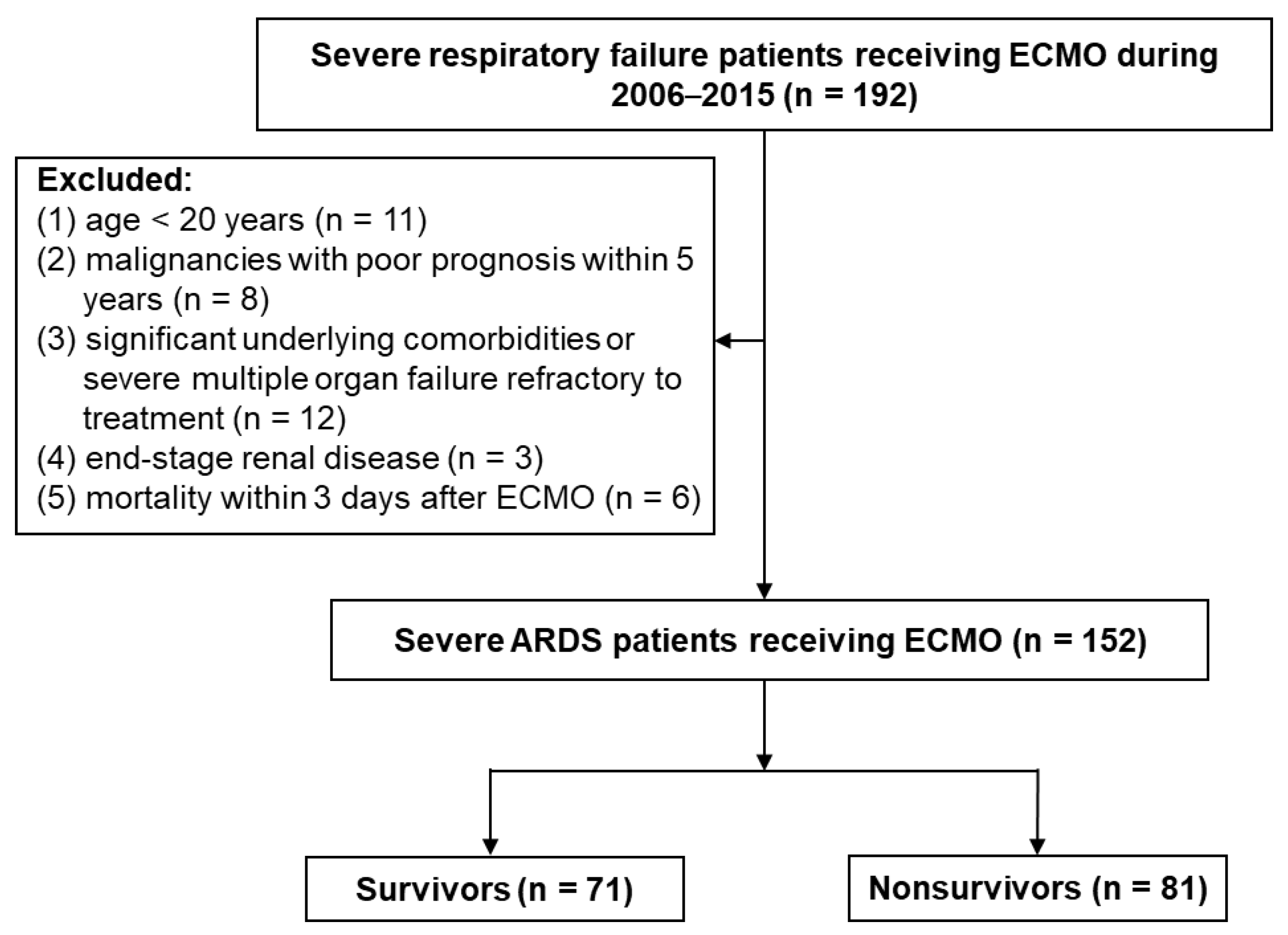
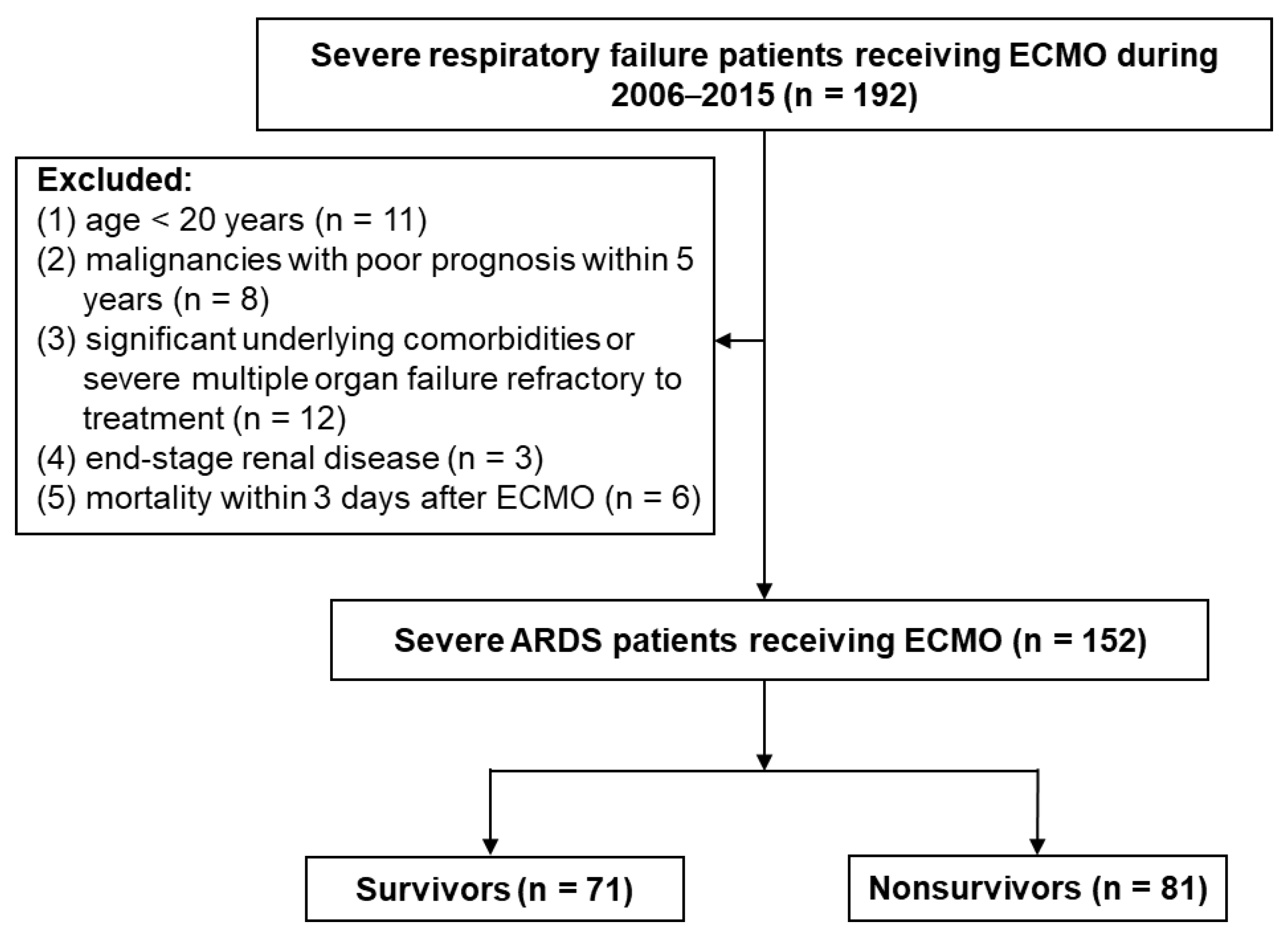
2.1. Study Design and Patients
2.2. Definitions
2.3. Data Collection
2.4. ECMO Systems
2.5. Statistical Analysis
3. Results
3.1. Patients
3.2. Comparison of Survivors and Nonsurvivors
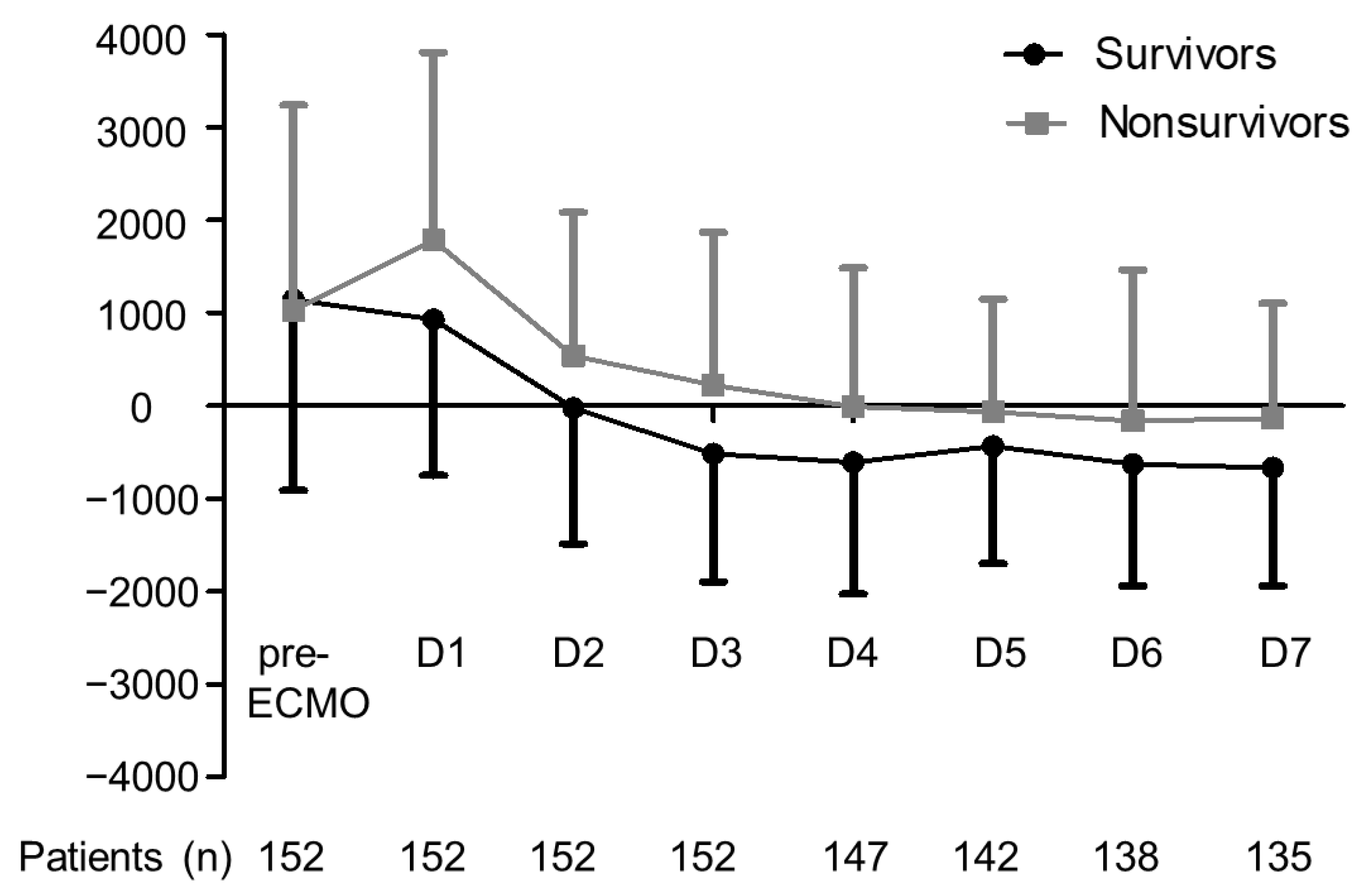
3.3. Comparisons of Cumulative Fluid Balance at 3 Days after ECMO
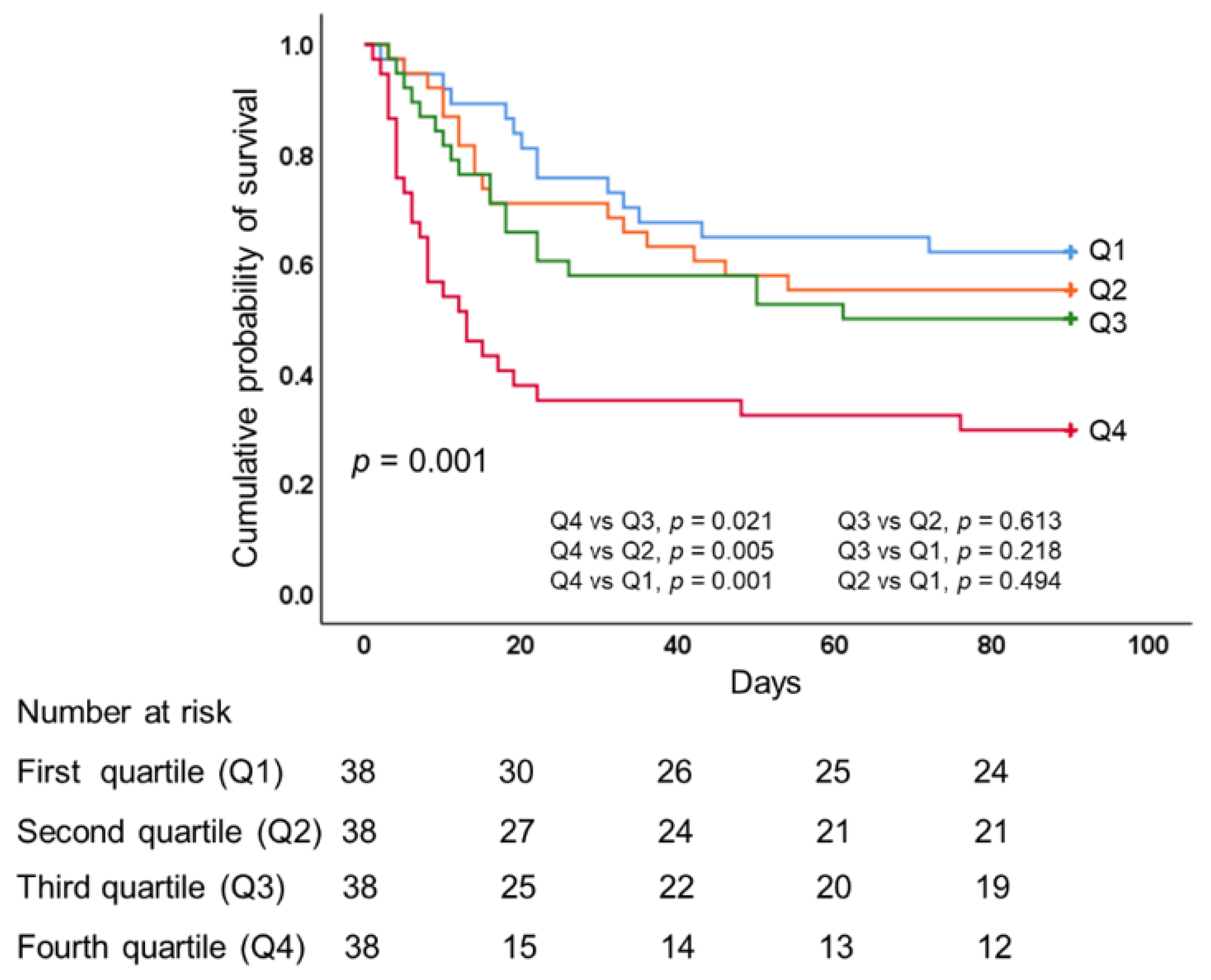
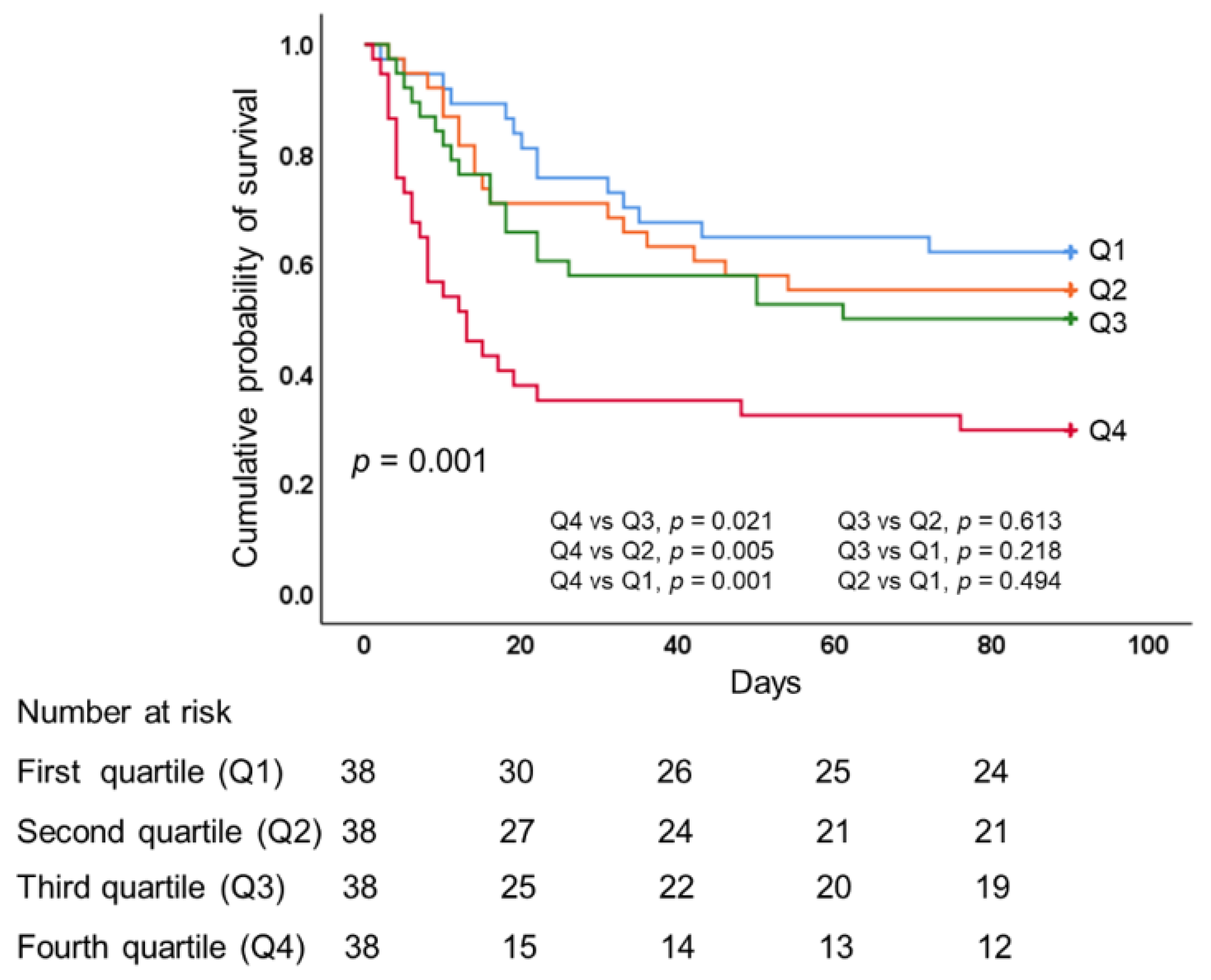
3.4. Outcomes
3.5. Factors Associated with Hospital Mortality
3.6. Comparisons of VV-ECMO- and VA-ECMO-Supported ARDS Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brodie, D.; Bacchetta, M. Extracorporeal membrane oxygenation for ARDS in adults. N. Engl. J. Med. 2011, 365, 1905–1914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giani, M.; Redaelli, S.; Siragusa, A.; Fumagalli, B.; Rona, R.; Foti, G. Extracorporeal Gas Exchange for Acute Respiratory Distress Syndrome: Open Questions, Controversies and Future Directions. Membranes 2021, 11, 172. [Google Scholar] [CrossRef]
- Abrams, D.; Brodie, D. Extracorporeal Membrane Oxygenation for Adult Respiratory Failure: 2017 Update. Chest 2017, 152, 639–649. [Google Scholar] [CrossRef] [PubMed]
- Combes, A.; Pesenti, A.; Ranieri, V.M. Fifty Years of Research in ARDS. Is Extracorporeal Circulation the Future of Acute Respiratory Distress Syndrome Management? Am. J. Respir Crit. Care Med. 2017, 195, 1161–1170. [Google Scholar] [CrossRef] [PubMed]
- Gattinoni, L.; Vassalli, F.; Romitti, F.; Vasques, F.; Pasticci, I.; Duscio, E.; Quintel, M. Extracorporeal gas exchange: When to start and how to end? Crit. Care 2019, 23 (Suppl. S1), 203. [Google Scholar] [CrossRef] [Green Version]
- Ficial, B.; Vasques, F.; Zhang, J.; Whebell, S.; Slattery, M.; Lamas, T.; Daly, K.; Agnew, N.; Camporota, L. Physiological Basis of Extracorporeal Membrane Oxygenation and Extracorporeal Carbon Dioxide Removal in Respiratory Failure. Membranes 2021, 11, 225. [Google Scholar] [CrossRef]
- Extracorporeal Life Support Organization. Available online: https://www.elso.org/Resources/Guidelines.aspx (accessed on 6 June 2021).
- Sakr, Y.; Rubatto Birri, P.N.; Kotfis, K.; Nanchal, R.; Shah, B.; Kluge, S.; Schroeder, M.E.; Marshall, J.C.; Vincent, J.L. Intensive Care Over Nations Investigators. Higher Fluid Balance Increases the Risk of Death From Sepsis: Results From a Large International Audit. Crit. Care Med. 2017, 45, 386–394. [Google Scholar] [CrossRef]
- Messmer, A.S.; Zingg, C.; Müller, M.; Gerber, J.L.; Schefold, J.C.; Pfortmueller, C.A. Fluid Overload and Mortality in Adult Critical Care Patients-A Systematic Review and Meta-Analysis of Observational Studies. Crit. Care Med. 2020, 48, 1862–1870. [Google Scholar] [CrossRef]
- Neyra, J.A.; Li, X.; Canepa-Escaro, F.; Adams-Huet, B.; Toto, R.D.; Yee, J.; Hedayati, S.S. Acute Kidney Injury in Critical Illness Study Group. Cumulative Fluid Balance and Mortality in Septic Patients with or Without Acute Kidney Injury and Chronic Kidney Disease. Crit. Care Med. 2016, 44, 1891–1900. [Google Scholar] [CrossRef]
- Silversides, J.A.; Fitzgerald, E.; Manickavasagam, U.S.; Lapinsky, S.E.; Nisenbaum, R.; Hemmings, N.; Nutt, C.; Trinder, T.J.; Pogson, D.G.; Fan, E. Role of Active Deresuscitation After Resuscitation (RADAR) Investigators. Deresuscitation of Patients With Iatrogenic Fluid Overload Is Associated With Reduced Mortality in Critical Illness. Crit. Care Med. 2018, 46, 1600–1607. [Google Scholar] [CrossRef]
- Zhang, J.; Crichton, S.; Dixon, A.; Seylanova, N.; Peng, Z.Y.; Ostermann, M. Cumulative fluid accumulation is associated with the development of acute kidney injury and non-recovery of renal function: A retrospective analysis. Crit. Care 2019, 23, 392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vignon, P.; Evrard, B.; Asfar, P.; Busana, M.; Calfee, C.S.; Coppola, S.; Demiselle, J.; Geri, G.; Jozwiak, M.; Martin, G.S.; et al. Fluid administration and monitoring in ARDS: Which management? Intensive Care Med. 2020, 46, 2252–2264. [Google Scholar] [CrossRef] [PubMed]
- National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network; Wiedemann, H.P.; Wheeler, A.P.; Bernard, G.R.; Thompson, B.T.; Hayden, D.; deBoisblanc, B.; Connors, A.F., Jr.; Hite, R.D.; Harabin, A.L. Comparison of two fluid-management strategies in acute lung injury. N. Engl. J. Med. 2006, 354, 2564–2575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silversides, J.A.; Major, E.; Ferguson, A.J.; Mann, E.E.; McAuley, D.F.; Marshall, J.C.; Blackwood, B.; Fan, E. Conservative fluid management or deresuscitation for patients with sepsis or acute respiratory distress syndrome following the resuscitation phase of critical illness: A systematic review and meta-analysis. Intensive Care Med. 2017, 43, 155–170. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, M.; Bailey, M.; Kelly, J.; Hodgson, C.; Cooper, D.J.; Scheinkestel, C.; Pellegrino, V.; Bellomo, R.; Pilcher, D. Impact of fluid balance on outcome of adult patients treated with extracorporeal membrane oxygenation. Intensive Care Med. 2014, 40, 1256–1266. [Google Scholar] [CrossRef]
- Kim, H.; Paek, J.H.; Song, J.H.; Lee, H.; Jhee, J.H.; Park, S.; Yun, H.R.; Kee, Y.K.; Han, S.H.; Yoo, T.H.; et al. Permissive fluid volume in adult patients undergoing extracorporeal membrane oxygenation treatment. Crit. Care 2018, 22, 270. [Google Scholar] [CrossRef] [Green Version]
- Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute respiratory distress syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar]
- Chiu, L.C.; Lin, S.W.; Chuang, L.P.; Li, H.H.; Liu, P.H.; Tsai, F.C.; Chang, C.H.; Hung, C.Y.; Lee, C.S.; Leu, S.W.; et al. Mechanical power during extracorporeal membrane oxygenation and hospital mortality in patients with acute respiratory distress syndrome. Crit. Care 2021, 25, 13. [Google Scholar] [CrossRef]
- Kellum, J.A.; Lameire, N. KDIGO AKI Guideline Work Group. Diagnosis, evaluation, and management of acute kidney injury: A KDIGO summary (Part 1). Crit. Care 2013, 17, 204. [Google Scholar] [CrossRef] [Green Version]
- Millar, J.E.; Fanning, J.P.; McDonald, C.I.; McAuley, D.F.; Fraser, J.F. The inflammatory response to extracorporeal membrane oxygenation (ECMO): A review of the pathophysiology. Crit. Care 2016, 20, 387. [Google Scholar] [CrossRef] [Green Version]
- Thompson, B.T.; Chambers, R.C.; Liu, K.D. Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2017, 377, 562–572. [Google Scholar] [CrossRef] [PubMed]
- Malbrain, M.L.N.G.; Van Regenmortel, N.; Saugel, B.; De Tavernier, B.; Van Gaal, P.J.; Joannes-Boyau, O.; Teboul, J.L.; Rice, T.W.; Mythen, M.; Monnet, X. Principles of fluid management and stewardship in septic shock: It is time to consider the four D’s and the four phases of fluid therapy. Ann. Intensive Care 2018, 8, 66. [Google Scholar] [CrossRef] [PubMed]
- Haneya, A.; Diez, C.; Philipp, A.; Bein, T.; Mueller, T.; Schmid, C.; Lubnow, M. Impact of Acute Kidney Injury on Outcome in Patients With Severe Acute Respiratory Failure Receiving Extracorporeal Membrane Oxygenation. Crit. Care Med. 2015, 43, 1898–1906. [Google Scholar] [CrossRef]
- Ostermann, M.; Connor, M., Jr.; Kashani, K. Continuous renal replacement therapy during extracorporeal membrane oxygenation: Why, when and how? Curr. Opin. Crit. Care 2018, 24, 493–503. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.; Pham, T.; Arcadipane, A.; Agerstrand, C.; Ohshimo, S.; Pellegrino, V.; Vuylsteke, A.; Guervilly, C.; McGuinness, S.; Pierard, S.; et al. Mechanical Ventilation Management during Extracorporeal Membrane Oxygenation for Acute Respiratory Distress Syndrome. An International Multicenter Prospective Cohort. Am. J. Respir. Crit. Care Med. 2019, 200, 1002–1012. [Google Scholar] [CrossRef] [PubMed]
- Ostermann, M.; Straaten, H.M.; Forni, L.G. Fluid overload and acute kidney injury: Cause or consequence? Crit. Care 2015, 19, 443. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| Variables | All | Survivors | Nonsurvivors | p | |
|---|---|---|---|---|---|
| (n = 152) | (n = 71) | (n = 81) | |||
| Age (years) | 50.3 ± 16.4 | 46.0 ± 16.5 | 54.1 ± 15.4 | 0.002 | |
| Male (gender) | 103 (67.8%) | 48 (67.6%) | 55 (67.9%) | 0.969 | |
| Body mass index (kg/m2) | 25.8 ± 5.3 | 26.0 ± 5.8 | 25.6 ± 4.7 | 0.631 | |
| ARDS etiologies | |||||
| Pulmonary cause | 118 (78%) | 59 (83%) | 59 (73%) | 0.130 | |
| Extrapulmonary cause | 34 (22%) | 12 (17%) | 22 (27%) | 0.130 | |
| Diabetes mellitus | 40 (26%) | 23 (32%) | 17 (21%) | 0.111 | |
| Chronic liver disease | 21 (14%) | 6 (9%) | 15 (19%) | 0.073 | |
| Immunocompromised status | 40 (26%) | 11 (16%) | 29 (36%) | 0.005 | |
| Chronic kidney disease | 17 (11.2%) | 8 (11.2%) | 9 (11.1%) | 0.976 | |
| SOFA score before ECMO | 10.8 ± 3.2 | 10.3 ± 3.1 | 11.3 ± 3.2 | 0.067 | |
| Lung injury score before ECMO | 3.4 ± 0.4 | 3.4 ± 0.4 | 3.3 ± 0.4 | 0.106 | |
| PaO2/FiO2 (mmHg) before ECMO | 63 (52–88) | 64 (53–80) | 63 (52–107) | 0.168 | |
| ECMO VA mode | 24 (15.8%) | 6 (8.5%) | 18 (22.2%) | 0.020 | |
| ECMO blood flow rate (L/min) at day 1 | 3.4 ± 0.7 | 3.3 ± 0.8 | 3.5 ± 0.7 | 0.079 | |
| ECMO blood flow rate (L/min) at day 3 | 3.8 ± 0.8 | 3.7 ± 1.0 | 3.9 ± 0.7 | 0.269 | |
| SOFA score from day 1 to day 3 on ECMO | 9.6 ± 2.3 | 8.8 ± 1.9 | 10.4 ± 2.4 | <0.001 | |
| PaO2/FiO2 (mmHg) from day 1 to day 3 on ECMO | 178 (131–240) | 200 (146–247) | 165 (124–211) | 0.588 | |
| Ventilator settings from day 1 to day 3 on ECMO | |||||
| Mechanical power (J/min) | 12.1 ± 6.2 | 10.9 ± 4.3 | 13.1 ± 7.4 | 0.022 | |
| Tidal volume (mL/kg PBW) | 6.0 ± 2.2 | 6.1 ± 2.0 | 6.0 ± 2.4 | 0.914 | |
| PEEP (cm H2O) | 12.0 ± 3.3 | 12.3 ± 3.2 | 11.7 ± 3.3 | 0.202 | |
| Peak inspiratory pressure (cm H2O) | 31.7 ± 5.6 | 30.6 ± 5.1 | 32.8 ± 5.9 | 0.018 | |
| Mean airway pressure (cm H2O) | 17.7 ± 4.0 | 17.4± 3.6 | 17.9 ± 4.3 | 0.406 | |
| Dynamic compliance (mL/cm H2O) | 19.2 ± 8.1 | 21.1 ± 7.7 | 17.4 ± 8.1 | 0.006 | |
| Fluid balance, mL | |||||
| Before ECMO 24 h | 923 (−258 to 2125) | 1027 (−287 to 2341) | 795 (−193 to 1781) | 0.751 | |
| First 24 h | 1327 (57 to 2800) | 846 (−160 to 2095) | 1688 (219 to 3668) | 0.006 | |
| Cumulative 3 days | 1190 (−873 to 3935) | 277 (−1798 to 2384) | 1927 (−100 to 5266) | <0.001 | |
| Total fluid input, mL | |||||
| Before ECMO 24 h | 3007 (2255–4117) | 2772 (2281–3924) | 3437 (2255–4304) | 0.597 | |
| First 24 h | 4774 (3545–5926) | 4065 (3118–5441) | 5213 (4010–6010) | 0.083 | |
| Cumulative 3 days | 13,013 (9996–17,095) | 12,675 (10,039–15,056) | 13,374 (9871–17,626) | 0.841 | |
| Urine output, mL | |||||
| Before ECMO 24 h | 1500 (550–2380) | 1585 (700–2750) | 1350 (475–2093) | 0.054 | |
| First 24 h | 1318 (396–2536) | 1642 (750–2705) | 950 (183–2438) | 0.055 | |
| Cumulative 3 days | 4890 (1375–8758) | 6853 (1731–9779) | 3760 (681–7530) | 0.042 | |
| Blood product transfusions, mL | |||||
| Red blood cell | 505 (390–1120) | 520 (395–1075) | 430 (385–1180) | 0.803 | |
| Fresh frozen plasma | 560 (280–1120) | 490 (280–1100) | 590 (280–1120) | 0.800 | |
| Platelet concentrate | 250 (130–560) | 230 (125–550) | 325 (198–573) | 0.721 | |
| Hemoglobin (g/dL) | |||||
| Before ECMO | 10.7 ± 2.4 | 11.5 ± 2.4 | 10.0 ± 2.3 | 0.008 | |
| Day 1 | 10.7 ± 2.9 | 11.4 ± 3.4 | 9.9 ± 2.1 | 0.004 | |
| Day 3 | 10.2 ± 1.6 | 10.2 ± 1.8 | 10.1 ± 1.3 | 0.881 | |
| Serum creatinine (mg/dL) | |||||
| Before ECMO | 2.0 ± 2.1 | 2.0 ± 2.4 | 2.0 ± 1.9 | 0.946 | |
| Day 1 | 2.1 ± 1.8 | 2.1 ± 1.9 | 2.1 ± 1.8 | 0.782 | |
| Day 3 | 2.0 ± 1.5 | 1.8 ± 1.7 | 2.1 ± 1.3 | 0.343 | |
| AKI during ECMO (n) | |||||
| Stage 1 | 62 (40.8%) | 29 (40.8%) | 33 (40.7%) | 0.990 | |
| Stage 2 | 31 (20.4%) | 10 (14.1%) | 21 (25.9%) | 0.071 | |
| Stage 3 | 20 (13.2%) | 7 (9.9%) | 13 (16%) | 0.260 | |
| Diuretics (n) | 106 (69.7%) | 52 (73.2%) | 54 (66.7%) | 0.379 | |
| Inotropes (n) | 133 (87.5%) | 53 (74.6%) | 80 (98.8%) | <0.001 | |
| RRT (n) | 88 (58%) | 30 (42%) | 58 (72%) | <0.001 | |
| RRT initiation prior to ECMO (n) | 15 (9.9%) | 4 (5.6%) | 11 (13.6%) | 0.112 | |
| Time from RRT to ECMO (days) | 5 (2–18) | 2 (1–2) | 11 (5–20) | 0.002 | |
| RRT initiation during ECMO (n) | 73 (48%) | 26 (36.7%) | 47 (58%) | 0.008 | |
| Time from ECMO to RRT (days) | 1 (0–3) | 0 (0–1) | 1 (0–5) | 0.004 | |
| Duration of ECMO (days) | 9 (6–15) | 9 (5–13) | 11 (6–16) | 0.089 | |
| Duration of RRT (days) | 13 (4–30) | 16 (5–34) | 11 (4–28) | 0.163 | |
| Variables | First Quartile | Second Quartile | Third Quartile | Fourth Quartile | p | |
|---|---|---|---|---|---|---|
| (n = 38) | (n = 38) | (n = 38) | (n = 38) | |||
| Age (years) | 48.1 ± 16.9 | 51.0 ± 15.7 | 46.3 ± 16.0 | 55.3 ± 16.1 | 0.088 | |
| Male (gender) | 27 (71.1%) | 28 (73.7%) | 27 (71.1%) | 21 (55.3%) | 0.347 | |
| Body mass index (kg/m2) | 26.7 ± 6.6 | 26.4 ± 4.1 | 26.3 ± 5.3 | 23.8 ± 4.5 | 0.110 | |
| SOFA score before ECMO | 9.9 ± 3.3 | 11.6 ± 2.7 | 10.9 ± 3.2 | 10.8 ± 3.3 | 0.153 | |
| PaO2/FiO2 (mmHg) before ECMO | 58 (52–96) | 68 (56–87) | 57 (48–86) | 64 (54–95) | 0.998 | |
| ECMO VA mode | 6 (15.8%) | 7 (18.4%) | 5 (13.2%) | 6 (15.8%) | 0.941 | |
| ECMO blood flow rate (L/min) at day 1 | 3.4 ± 0.8 | 3.6 ± 0.6 | 3.3 ± 0.6 | 3.4 ± 0.8 | 0.570 | |
| ECMO blood flow rate (L/min) at day 3 | 3.9 ± 0.8 | 4.1 ± 0.4 | 3.8 ± 1.1 | 3.7 ± 0.8 | 0.776 | |
| SOFA score from day 1 to day 3 on ECMO | 9.0 ± 2.3 | 9.1 ± 2.0 | 9.6 ± 2.5 | 10.5 ± 2.2 | 0.041 | |
| PaO2/FiO2 (mmHg) from day 1 to day 3 on ECMO | 167 (127–275) | 160 (127–241) | 192 (154–231) | 169 (130–222) | 0.696 | |
| Ventilator settings from day 1 to day 3 on ECMO | ||||||
| Mechanical power (J/min) | 12.3 ± 6.0 | 13.0 ± 6.2 | 11 ± 4.7 | 12.1 ± 7.9 | 0.589 | |
| Tidal volume (mL/kg PBW) | 6.7 ± 2.6 | 6.0 ± 2.1 | 5.9 ± 1.7 | 5.5 ± 2.3 | 0.135 | |
| PEEP (cm H2O) | 11.9 ± 3.2 | 11.7 ± 3.5 | 12.4 ± 3.3 | 12 ± 3.1 | 0.839 | |
| Peak inspiratory pressure (cm H2O) | 30.5 ± 5.0 | 31.8 ± 5.7 | 31.8 ± 4.8 | 33.6 ± 6.2 | 0.101 | |
| Mean airway pressure (cm H2O) | 16.7 ± 3.8 | 17.5 ± 4.5 | 17.5 ± 3.4 | 19.0 ± 4.1 | 0.088 | |
| Dynamic compliance (mL/cm H2O) | 22.1 ± 7.8 | 19.6 ± 8.2 | 19.3 ± 7.5 | 15.6 ± 7.1 | 0.005 | |
| Fluid balance, mL | ||||||
| Before ECMO 24 h | 494 (−440 to 1537) | 363 (−324 to 1484) | 1102 (221 to 2244) | 1242 (−28 to 3118) | 0.024 | |
| First 24 h | −376 (−1327 to 267) | 645 (57 to 2035) | 1539 (595 to 2427) | 3646 (2407 to 4379) | <0.001 | |
| Cumulative 3 days | −2158 (−3844 to −1644) | 223 (−486 to 713) | 2179 (1797to 2914) | 5995 (4556 to 8128) | <0.001 | |
| Total fluid input, mL | ||||||
| Before ECMO 24 h | 2760 (1856–3970) | 3700 (2745–4227) | 3025 (2230–4330) | 2980 (1870–4836) | 0.405 | |
| First 24 h | 4065 (3158–5213) | 4047 (3350–5673) | 4696 (3545–5499) | 5795 (4800–7351) | 0.095 | |
| Cumulative 3 days | 12,023 (9405–15,900) | 12,899 (9598–15,057) | 12,774 (10,088–16,847) | 14,654 (11,365–18,983) | 0.717 | |
| Urine output, mL | ||||||
| Before ECMO 24 h | 2300 (1008–3565) | 1215 (450–2343) | 1458 (753–2103) | 1050 (326–2038) | 0.001 | |
| First 24 h | 2770 (1135–3695) | 1000 (300–2180) | 1690 (838–2466) | 635 (85–1360) | <0.001 | |
| Cumulative 3 days | 8900 (6853–12459) | 4492 (1439–9201) | 5285 (2788–7475) | 1417 (255–4530) | <0.001 | |
| Blood product transfusions, mL | ||||||
| Red blood cell | 450 (400–1243) | 420 (370–850) | 460 (384–1085) | 810 (500–1233) | 0.722 | |
| Fresh frozen plasma | 890 (258–1268) | 695 (280–1003) | 525 (290–1120) | 475 (273–1105) | 0.598 | |
| Platelet concentrate | 420 (115–565) | 400 (128–565) | 225 (128–485) | 240 (180–565) | 0.575 | |
| Hemoglobin (g/dL) | ||||||
| Before ECMO | 11.0 ± 2.8 | 10.3 ± 1.8 | 10.7 ± 2.9 | 10.8 ± 2.1 | 0.870 | |
| Day 1 | 10.8 ± 3.2 | 10.5 ± 3.1 | 11.0 ± 3.3 | 10.3 ± 2.0 | 0.782 | |
| Day 3 | 10.6 ± 1.8 | 10.2 ± 1.6 | 10.3 ± 1.6 | 9.6 ± 1.3 | 0.118 | |
| Serum creatinine (mg/dL) | ||||||
| Before ECMO | 1.6 ± 1.6 | 2.3 ± 2.6 | 2.0 ± 2.1 | 2.1 ± 2.1 | 0.622 | |
| Day 1 | 1.8 ± 1.5 | 2.2 ± 1.7 | 2.0 ± 2.1 | 2.4 ± 2.0 | 0.595 | |
| Day 3 | 1.7 ± 1.4 | 2.2 ± 1.6 | 1.9 ± 1.5 | 2.1 ± 1.5 | 0.475 | |
| AKI during ECMO (n) | ||||||
| Stage 1 | 14 (36.8%) | 19 (50%) | 16 (42.1%) | 13 (34.2%) | 0.588 | |
| Stage 2 | 5 (13.2%) | 3 (7.9%) | 10 (26.3%) | 13 (34.2%) | 0.015 | |
| Stage 3 | 4 (10.5%) | 5 (13.2%) | 4 (10.5%) | 7 (18.4%) | 0.697 | |
| Diuretics (n) | 26 (68.4%) | 28 (73.7%) | 26 (68.4%) | 26 (68.4%) | 0.941 | |
| Inotropes (n) | 32 (84.2%) | 31 (81.6%) | 34 (89.5%) | 36 (94.7%) | 0.130 | |
| RRT (n) | 17 (44.7%) | 23 (60.5%) | 20 (52.6%) | 28 (73.7%) | 0.057 | |
| RRT initiation prior to ECMO (n) | 2 (5.3%) | 4 (10.5%) | 4 (10.5%) | 5 (13.2%) | 0.272 | |
| Time from RRT to ECMO (days) | 11(2) | 3 (1-18) | 8 (2–14) | 8 (4–25) | 0.831 | |
| RRT initiation during ECMO (n) | 15 (39.5%) | 19 (50%) | 16 (42.1%) | 23 (60.5%) | 0.124 | |
| Time from ECMO to RRT (days) | 1 (0–10) | 1 (0–9) | 1 (0–4) | 1 (0–2) | 0.147 | |
| Duration of RRT (days) | 13 (4–32) | 15 (7–36) | 12 (6–26) | 11 (4–24) | 0.549 | |
| Hospital mortality, n (%) | 14 (36.8%) | 18 (47.4%) | 21 (55.3%) | 28 (73.7%) | 0.009 | |
| Variables | First Quartile | Second Quartile | Third Quartile | Fourth Quartile | p | |
|---|---|---|---|---|---|---|
| (n = 38) | (n = 38) | (n = 38) | (n = 38) | |||
| Mortality | ||||||
| 28-day hospital mortality, n (%) | 9 (23.7%) | 11 (28.9%) | 16 (42.1%) | 24 (63.2%) | <0.001 | |
| 60-day hospital mortality, n (%) | 13 (34.2%) | 17 (44.7%) | 18 (47.4%) | 25 (65.8%) | 0.002 | |
| 90-day hospital mortality, n (%) | 14 (36.8%) | 17 (44.7%) | 19 (50%) | 26 (68.4%) | 0.001 | |
| Other outcomes | ||||||
| Duration of ECMO (days) | 8 (5–16) | 12 (7–18) | 10 (7–15) | 7 (4–12) | 0.209 | |
| Duration of mechanical ventilator (days) | 25 (11–31) | 27 (14–44) | 22 (15–40) | 18 (10–36) | 0.380 | |
| Length of ICU stay (days) | 27 (13–38) | 29 (16–49) | 27 (18–48) | 18 (10–39) | 0.451 | |
| Length of hospital stay (days) | 41 (27–61) | 49 (23–73) | 40 (22–69) | 28 (11–53) | 0.334 | |
| ECMO-free days at day 28 | 15 (0–22) | 9 (0–19) | 8 (0–19) | 0 (0–14) | 0.082 | |
| Ventilator-free days at day 28 | 0 (0–16) | 0 (0–5) | 0 (0–4) | 0 (0–0) | 0.002 | |
| Ventilator-free days at day 60 | 32 (0–48) | 14 (0–37) | 0 (0–36) | 0 (0–0) | 0.001 | |
| Variables | Adjust HR (95% CI) | p | |
|---|---|---|---|
| Model 1 | |||
| Cumulative fluid balance from day 1 to 3 on ECMO (per 1-L increase) | 1.110 (1.027–1.201) | 0.009 | |
| Model 2 | |||
| Cumulative fluid balance from day 1 to 3 on ECMO | |||
| First quartile | 1.00 (reference) | ||
| Second quartile | 1.200 (0.569–2.531) | 0.632 | |
| Third quartile | 1.675 (0.819–3.425) | 0.158 | |
| Fourth quartile | 2.710 (1.379–5.325) | 0.004 | |
| Variables | VV ECMO | VA ECMO | p | |
|---|---|---|---|---|
| (n = 128) | (n = 24) | |||
| Age (years) | 51.2 ± 16.4 | 45.9 ± 15.2 | 0.147 | |
| Male (gender) | 89 (69.5%) | 14 (58.3%) | 0.281 | |
| Body mass index (kg/m2) | 25.8 ± 5.4 | 25.4 ± 4.3 | 0.754 | |
| ARDS etiologies | ||||
| Pulmonary cause | 103 (80.5%) | 15 (62.5%) | 0.053 | |
| Extrapulmonary cause | 25 (19.5%) | 9 (37.5%) | 0.053 | |
| Diabetes mellitus | 38 (29.7%) | 2 (8.3%) | 0.041 | |
| Chronic liver disease | 19 (14.8%) | 2 (8.3%) | 0.531 | |
| Immunocompromised status | 33 (25.8%) | 7 (29.2%) | 0.730 | |
| Chronic kidney disease | 16 (12.5%) | 1 (4.2%) | 0.313 | |
| SOFA score before ECMO | 10.6 ± 3.1 | 12.2 ± 3.0 | 0.023 | |
| Lung injury score before ECMO | 3.4 ± 0.4 | 3.3 ± 0.5 | 0.384 | |
| PaO2/FiO2 (mmHg) before ECMO | 63 (53–93) | 63 (49–85) | 0.787 | |
| ECMO blood flow rate (L/min) at day 1 | 3.4 ± 0.7 | 3.4 ± 0.6 | 0.942 | |
| ECMO blood flow rate (L/min) at day 3 | 3.9 ± 0.8 | 3.8 ± 0.8 | 0.710 | |
| SOFA score from day 1 to day 3 on ECMO | 9.6 ± 2.2 | 9.5 ± 3.0 | 0.862 | |
| PaO2/FiO2 (mmHg) from day 1 to day 3 on ECMO | 180 (135–221) | 160 (106–442) | 0.078 | |
| Ventilator settings from day 1 to day 3 on ECMO | ||||
| Mechanical power (J/min) | 11.5 ± 6.0 | 15.0 ± 6.7 | 0.011 | |
| Tidal volume (mL/kg PBW) | 5.8 ± 2.0 | 7.1 ± 2.7 | 0.014 | |
| PEEP (cm H2O) | 12.3 ± 3.3 | 10.4 ± 2.6 | 0.007 | |
| Peak inspiratory pressure (cm H2O) | 31.3 ± 5.3 | 34.0 ± 7.0 | 0.035 | |
| Mean airway pressure (cm H2O) | 17.8 ± 3.9 | 17.3 ± 4.4 | 0.592 | |
| Dynamic compliance (mL/cm H2O) | 19.2 ± 7.9 | 18.9 ± 9.1 | 0.870 | |
| Fluid balance, mL | ||||
| Before ECMO 24 h | 932 (−148 to 2125) | 904 (−271 to 1996) | 0.919 | |
| First 24 h | 1410 (53 to 2800) | 1084 (78 to 2831) | 0.960 | |
| Cumulative 3 days | 1301 (−873 to 3935) | 833 (−894 to 4012) | 0.953 | |
| Total fluid input, mL | ||||
| Before ECMO 24 h | 2938 (2243–3930) | 4150 (3665–6359) | 0.587 | |
| First 24 h | 4464 (3513–5828) | 5005 (4398–6241) | 0.525 | |
| Cumulative 3 days | 12,899 (9774–16,926) | 13,425 (11,044–18,103) | 0.388 | |
| Urine output, mL | ||||
| Before ECMO 24 h | 1365 (530–2350) | 1857 (975–2721) | 0.408 | |
| First 24 h | 1460 (396–2705) | 826 (168–2264) | 0.316 | |
| Cumulative 3 days | 5385 (1490–8870) | 3750 (1040–7368) | 0.362 | |
| Blood product transfusions, mL | ||||
| Red blood cell | 520 (393–1098) | 420 (385–1306) | 0.634 | |
| Fresh frozen plasma | 560 (285–1110) | 490 (228–1120) | 0.689 | |
| Platelet concentrate | 325 (190–560) | 235 (113–545) | 0.247 | |
| Hemoglobin (g/dL) | ||||
| Before ECMO | 10.7 ± 2.4 | 10.7 ± 2.4 | 0.930 | |
| Day 1 | 10.6 ± 2.9 | 11.0 ± 3.0 | 0.632 | |
| Day 3 | 10.1 ± 1.6 | 10.3 ± 1.4 | 0.700 | |
| Serum creatinine (mg/dL) | ||||
| Before ECMO | 2.0 ± 2.2 | 1.9 ± 1.5 | 0.715 | |
| Day 1 | 2.1 ± 1.9 | 2.0 ± 1.0 | 0.662 | |
| Day 3 | 2.0 ± 1.6 | 1.9 ± 1.0 | 0.928 | |
| AKI during ECMO (n) | ||||
| Stage 1 | 51 (39.8%) | 11 (45.8%) | 0.584 | |
| Stage 2 | 27 (21.1%) | 4 (16.7%) | 0.785 | |
| Stage 3 | 15 (11.7%) | 5 (20.8%) | 0.225 | |
| Diuretics (n) | 91 (71.1%) | 15 (62.5%) | 0.400 | |
| Inotropes (n) | 110 (85.9%) | 23 (95.8%) | 0.311 | |
| RRT (n) | 74 (57.8%) | 14 (58.3%) | 0.962 | |
| RRT initiation prior to ECMO (n) | 13 (10.2%) | 2 (8.3%) | 1.000 | |
| Time from RRT to ECMO (days) | 5 (2–19) | 8 (4) | 0.720 | |
| RRT initiation during ECMO (n) | 61 (47.7%) | 12 (50%) | 0.833 | |
| Time from ECMO to RRT (days) | 1 (0–4) | 0 (0–1) | <0.001 | |
| Duration of ECMO (days) | 10 (6–16) | 8 (4–11) | 0.248 | |
| Duration of RRT (days) | 13 (4–29) | 10 (4–34) | 0.737 | |
| Hospital mortality, n (%) | 63 (49.2%) | 18 (75%) | 0.020 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiu, L.-C.; Chuang, L.-P.; Lin, S.-W.; Chiou, Y.-C.; Li, H.-H.; Chen, Y.-C.; Lin, Y.-J.; Chang, C.-J.; Tsai, F.-C.; Chang, K.-W.; et al. Cumulative Fluid Balance during Extracorporeal Membrane Oxygenation and Mortality in Patients with Acute Respiratory Distress Syndrome. Membranes 2021, 11, 567. https://doi.org/10.3390/membranes11080567
Chiu L-C, Chuang L-P, Lin S-W, Chiou Y-C, Li H-H, Chen Y-C, Lin Y-J, Chang C-J, Tsai F-C, Chang K-W, et al. Cumulative Fluid Balance during Extracorporeal Membrane Oxygenation and Mortality in Patients with Acute Respiratory Distress Syndrome. Membranes. 2021; 11(8):567. https://doi.org/10.3390/membranes11080567
Chicago/Turabian StyleChiu, Li-Chung, Li-Pang Chuang, Shih-Wei Lin, Yu-Ching Chiou, Hsin-Hsien Li, Yung-Chang Chen, Yu-Jr Lin, Chee-Jen Chang, Feng-Chun Tsai, Ko-Wei Chang, and et al. 2021. "Cumulative Fluid Balance during Extracorporeal Membrane Oxygenation and Mortality in Patients with Acute Respiratory Distress Syndrome" Membranes 11, no. 8: 567. https://doi.org/10.3390/membranes11080567
APA StyleChiu, L.-C., Chuang, L.-P., Lin, S.-W., Chiou, Y.-C., Li, H.-H., Chen, Y.-C., Lin, Y.-J., Chang, C.-J., Tsai, F.-C., Chang, K.-W., Hu, H.-C., Huang, C.-C., Leu, S.-W., & Kao, K.-C. (2021). Cumulative Fluid Balance during Extracorporeal Membrane Oxygenation and Mortality in Patients with Acute Respiratory Distress Syndrome. Membranes, 11(8), 567. https://doi.org/10.3390/membranes11080567