Newly Developed Pediatric Membrane Oxygenator that Suppresses Excessive Pressure Drop in Cardiopulmonary Bypass and Extracorporeal Membrane Oxygenation (ECMO)


Abstract
1. Introduction
2. Material and Methods
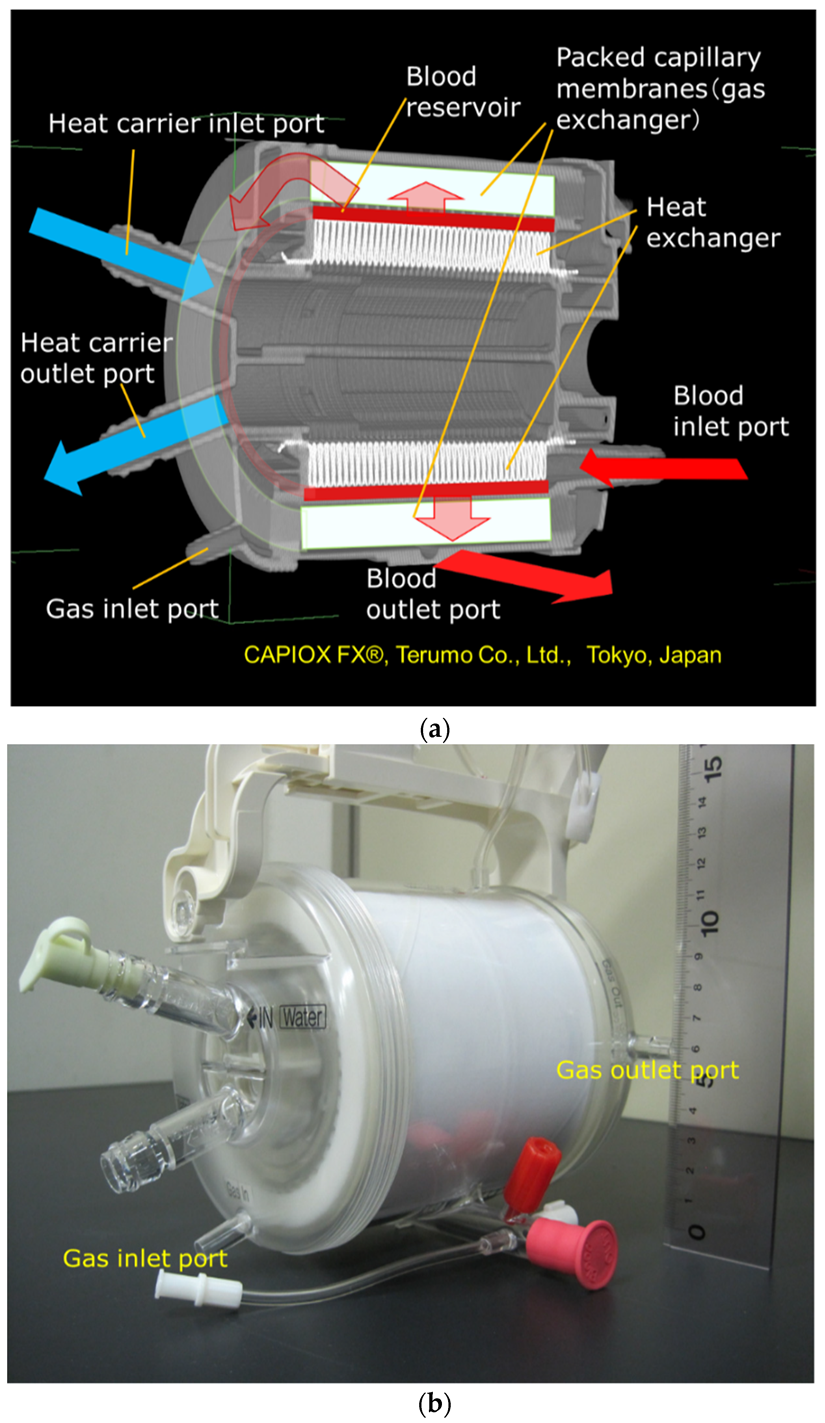
2.1. Hollow Fiber Membrane Oxygenators
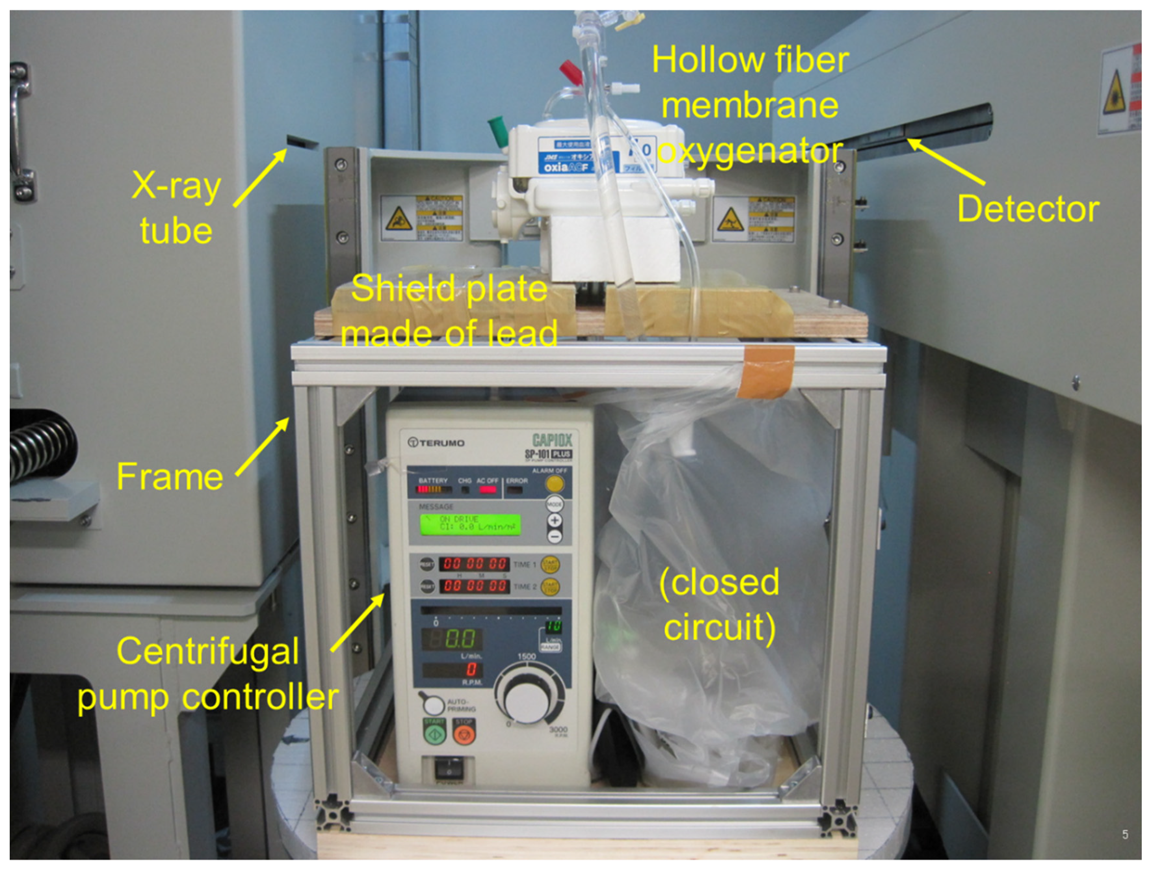
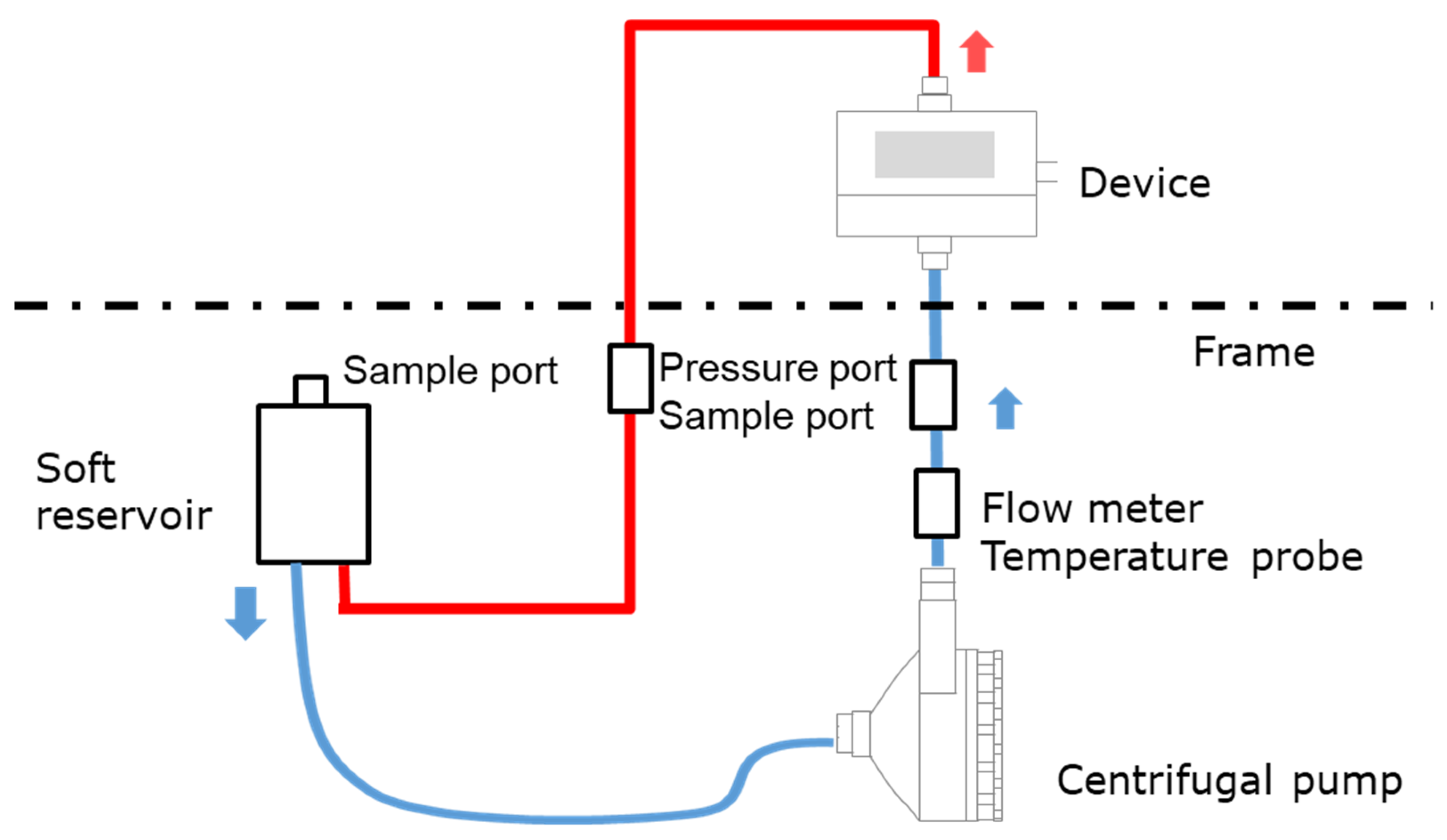
2.2. Imaging a Membrane Oxygenator Inside During Fluid Perfusion Using High-Power X-Ray CT
- (1)
- A test solution that can be used for X-ray CT imaging (high specific gravity of particles).
- (2)
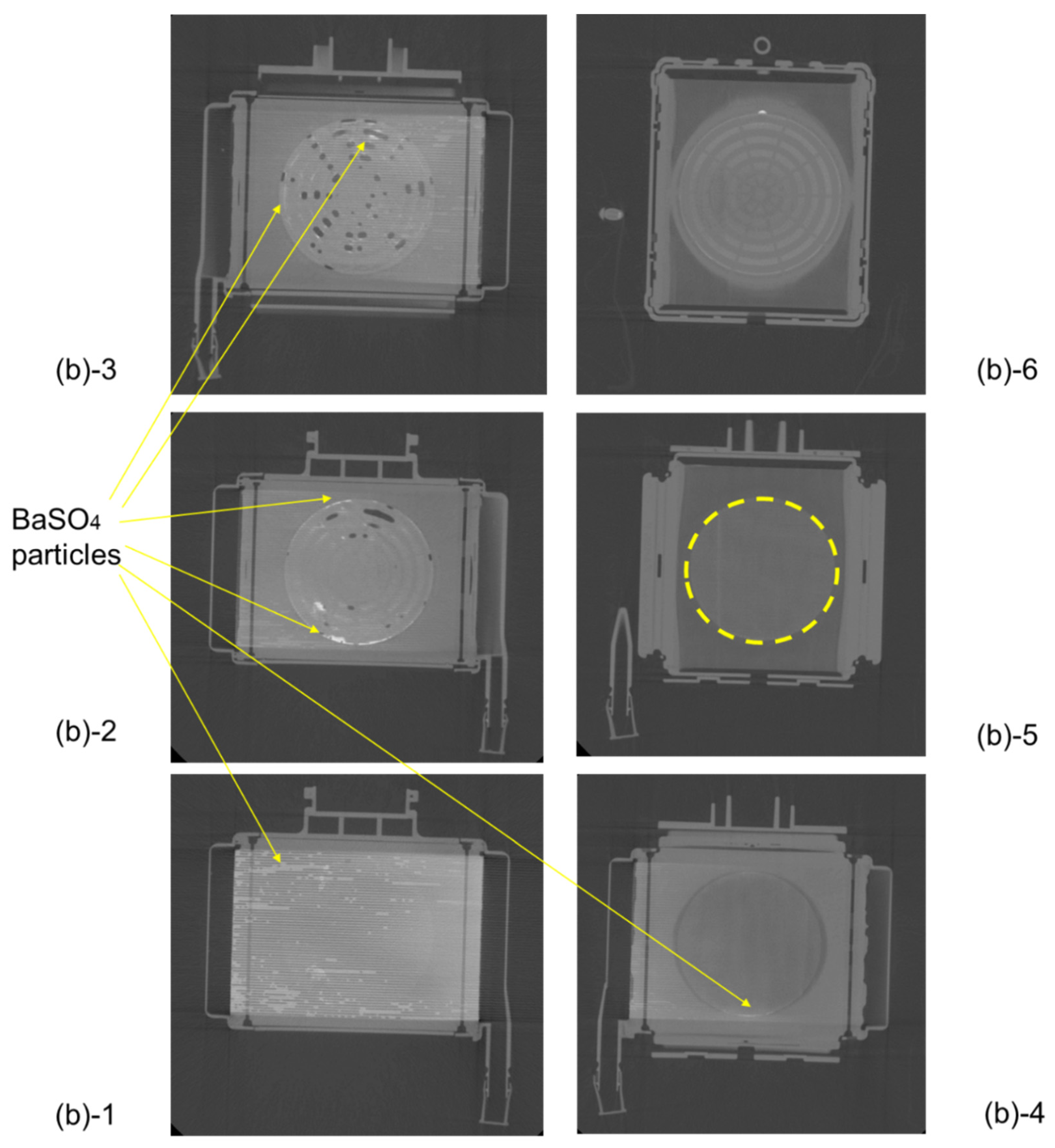
- It can localize in the region of the blood flow channel where it is expected to stay easily in between the hollow fibers (the red blood cell diameter is 8 µm as a guide, and since the BaSO4 particles do not deform during fluid perfusion, 5 µm particle was used as the BaSO4 particle size which is slightly smaller than 8 µm).
- (3)
- On the other hand, during the X-ray CT imaging, there should be no flow channel blockage that would prevent the test solution from flowing.
2.3. High-Power X-Ray Computed Tomography (CT)
2.4. Oxygen and Carbon Dioxide Transfer Rates, Pressure Drop of Blood Flow Channel
3. Results
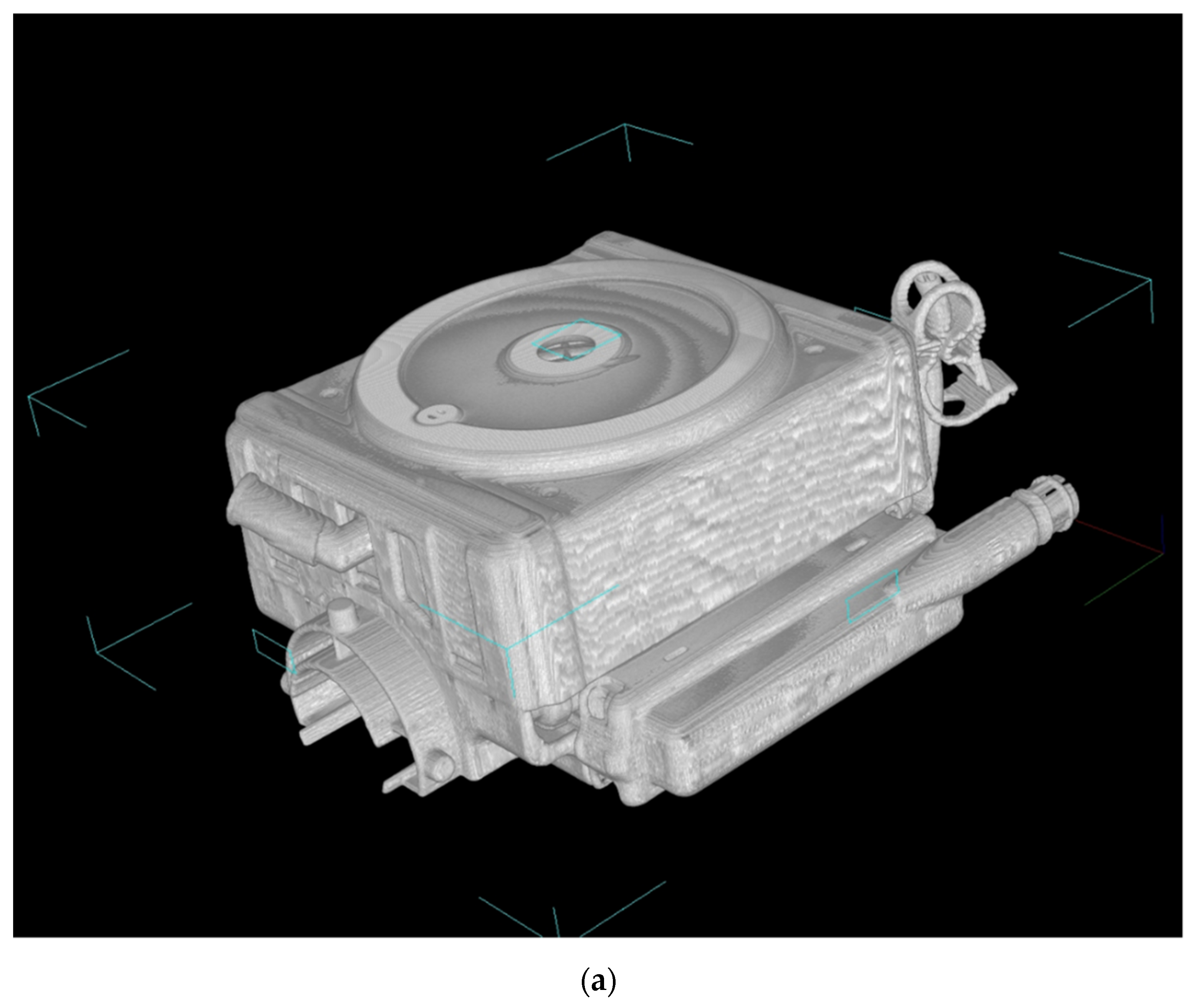
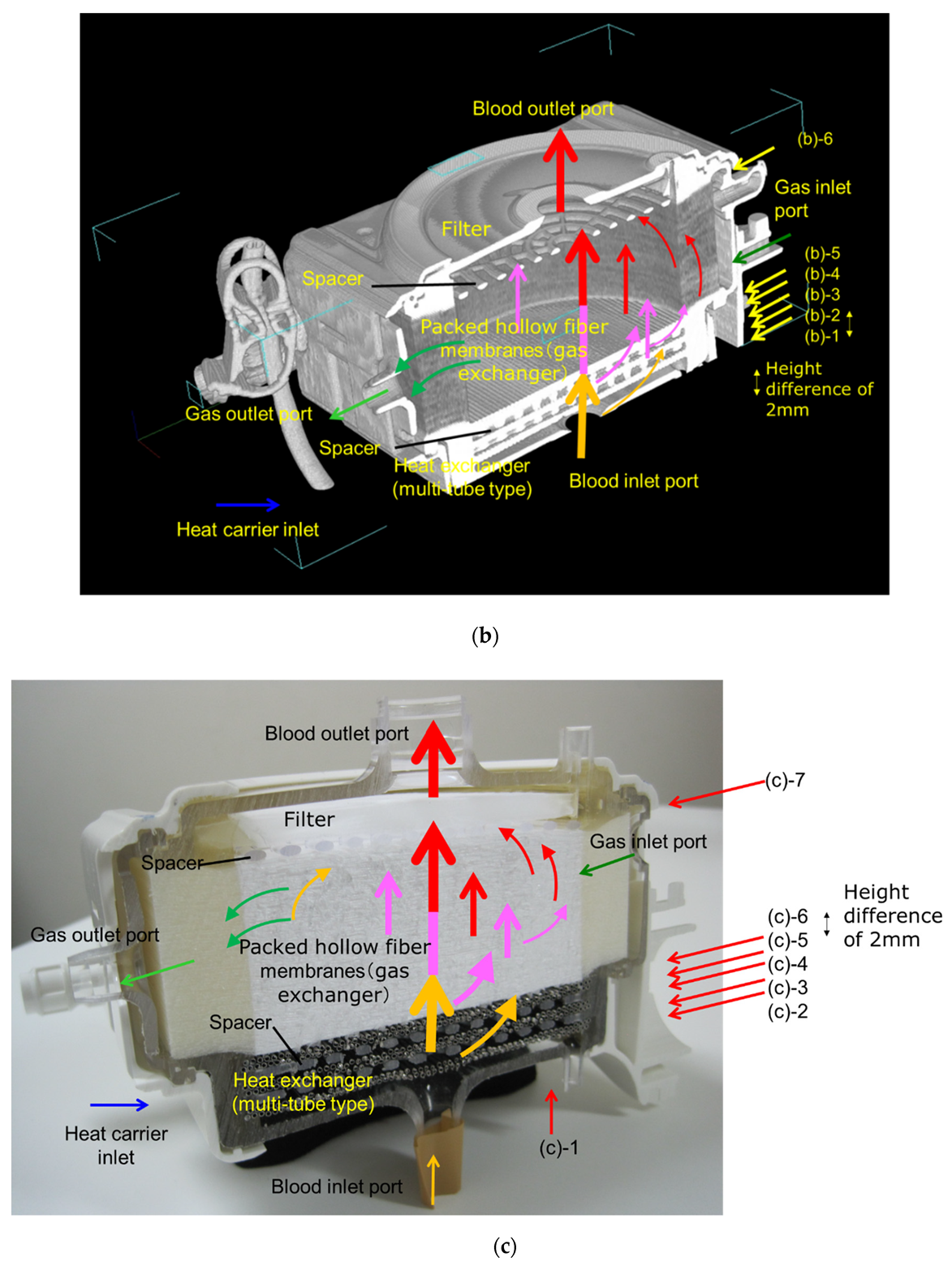
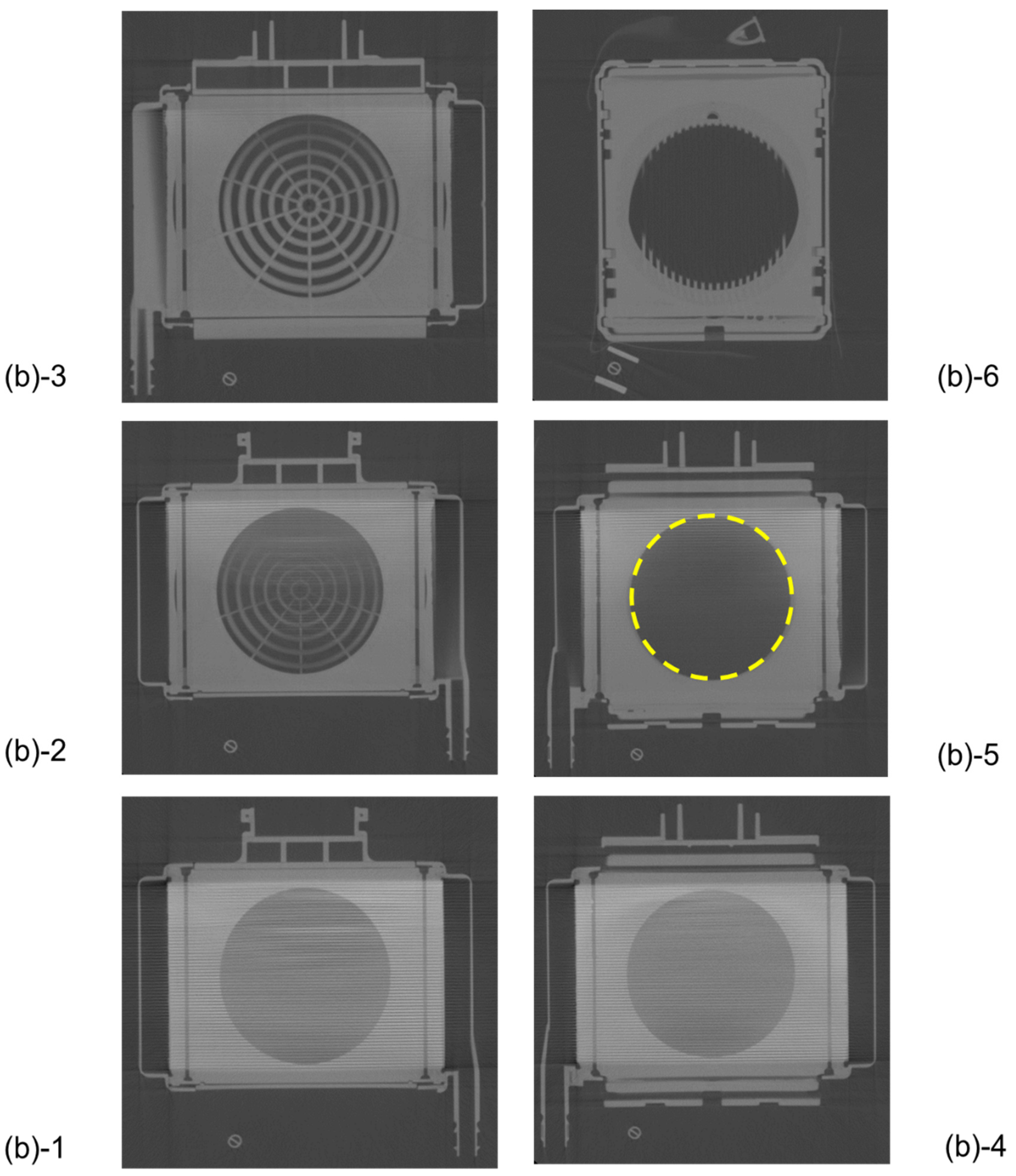
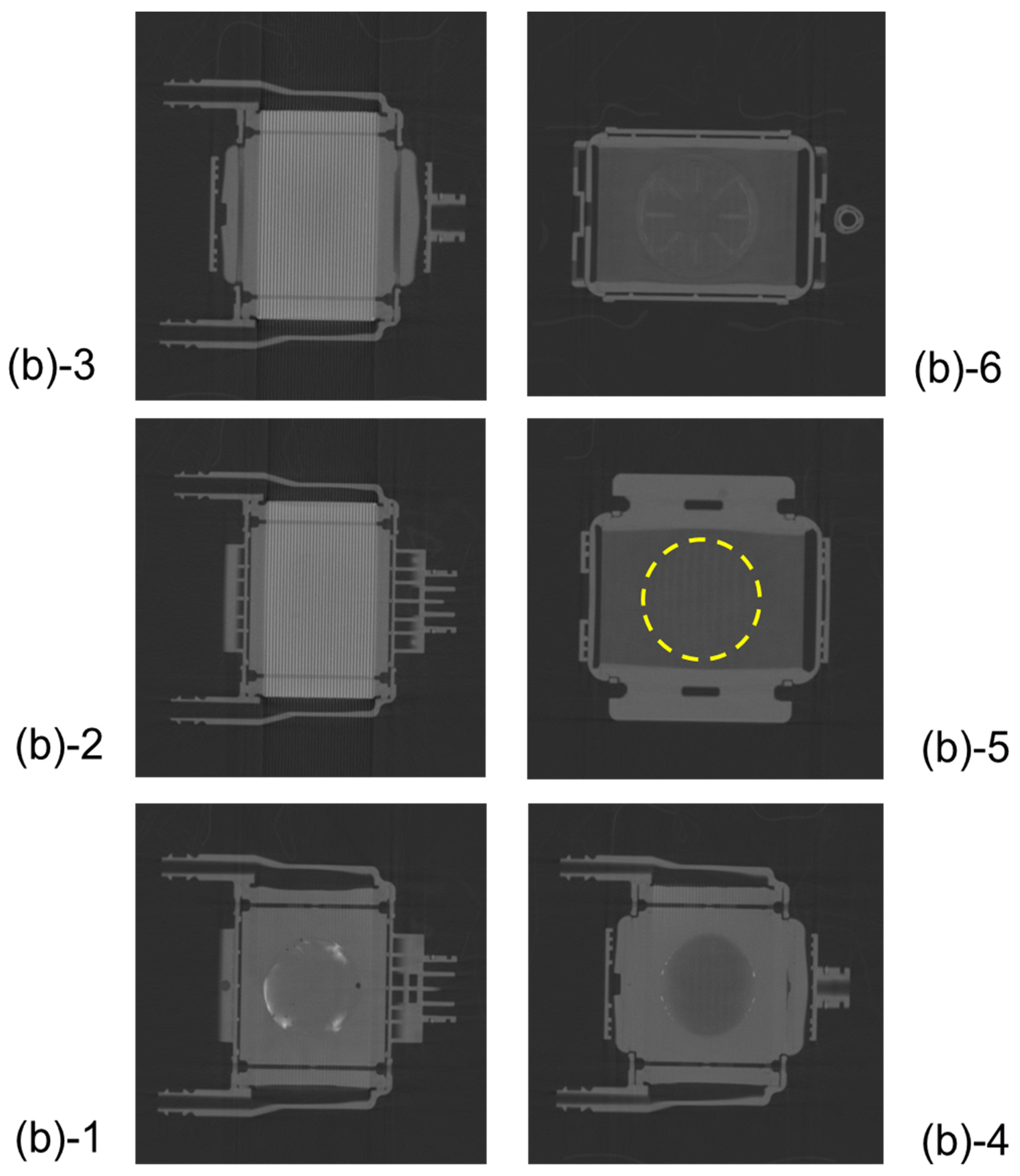
3.1. Non-Destructive Visualization of a Hollow Fiber Membrane Oxygenator Using High-Power X-Ray Computed Tomography
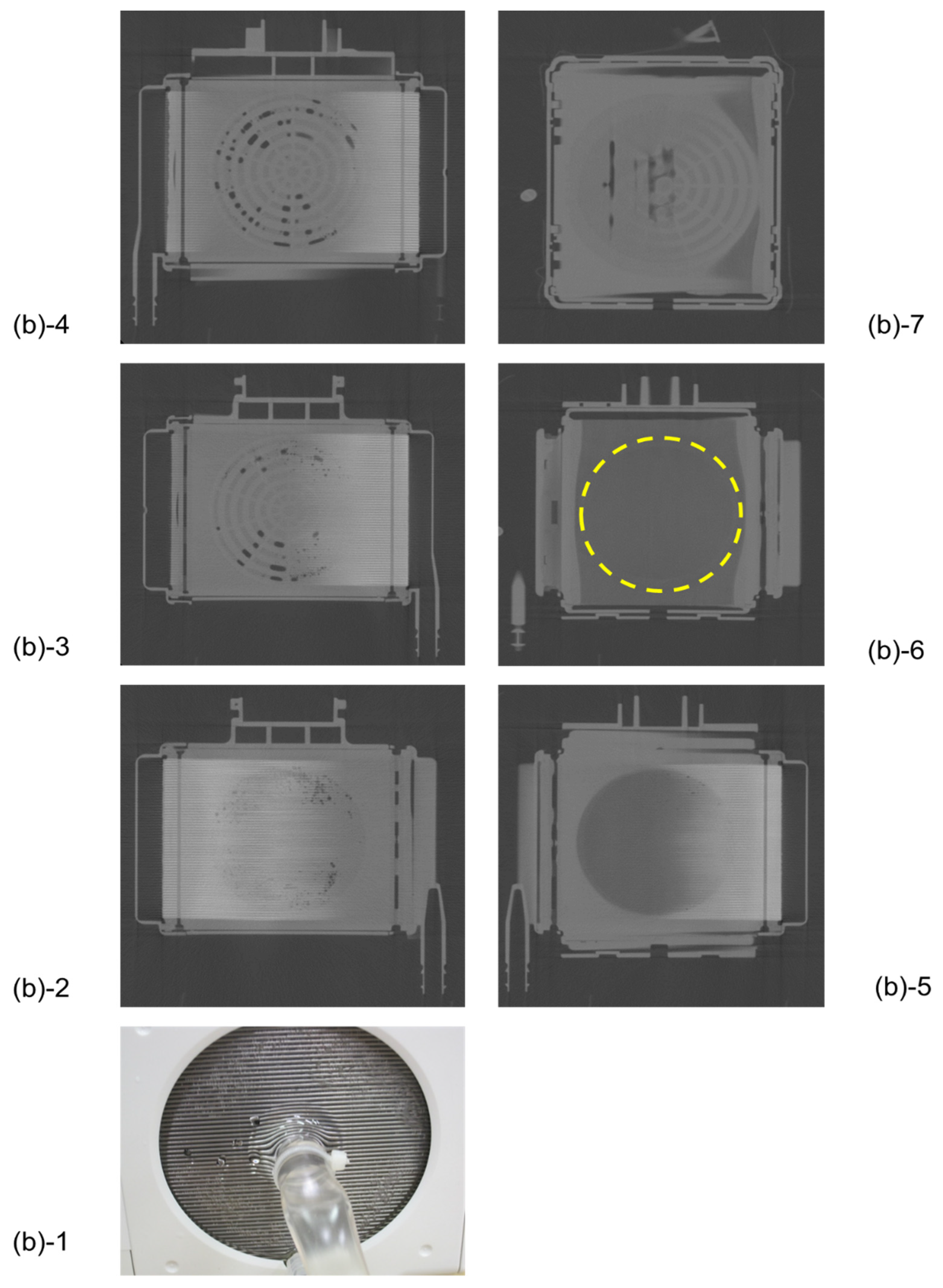
3.2. Non-Destructive Visualization in a Hollow Fiber Membrane Oxygenator during RO Water and X-Ray Contrast Agent Perfusion
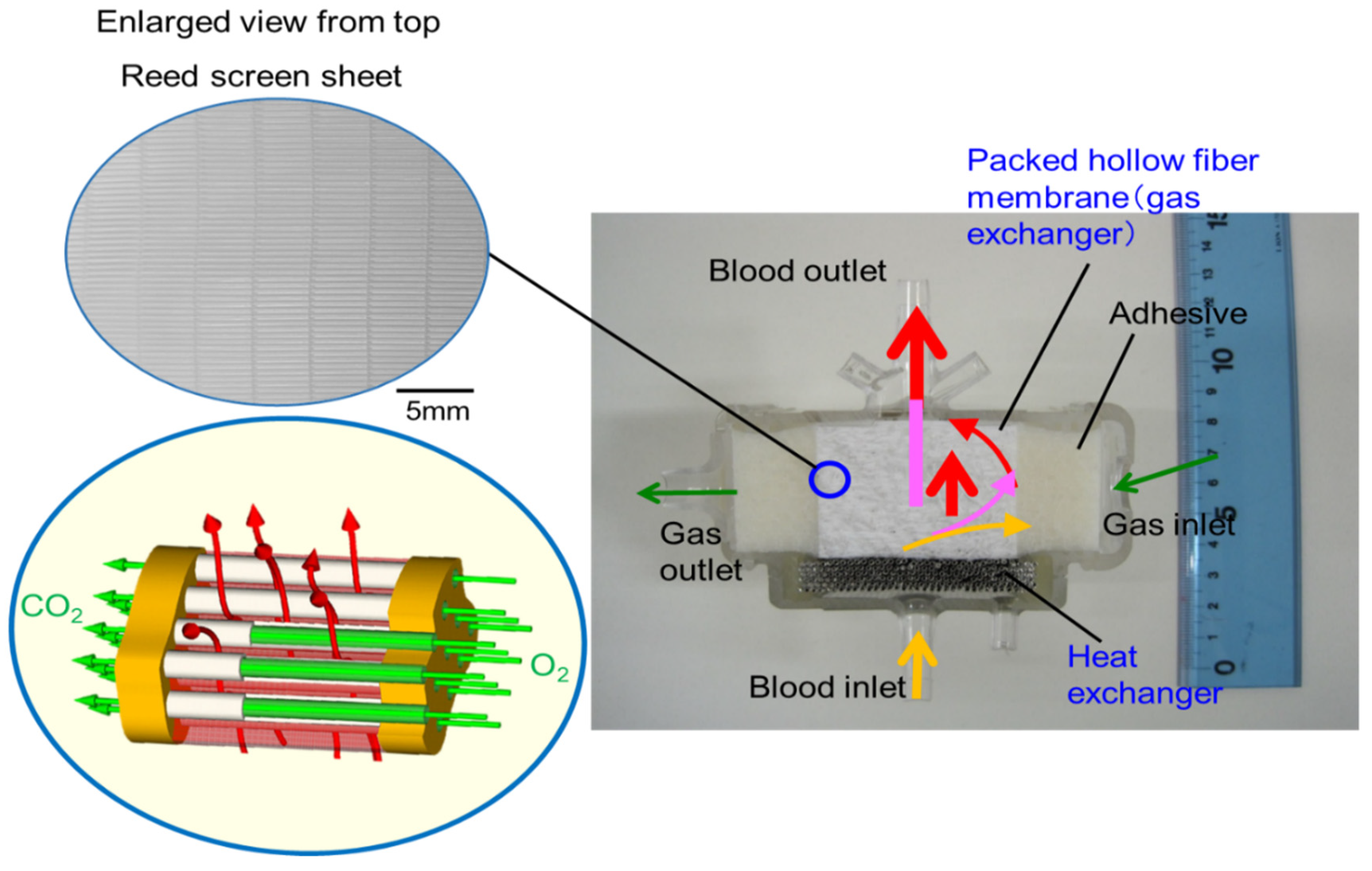
3.3. Design Concept of the Newly Developed Pediatric Membrane Oxygenator
3.4. Non-Destructive Visualization of the Newly-Developed Membrane Oxygenator during Fluid Perfusion
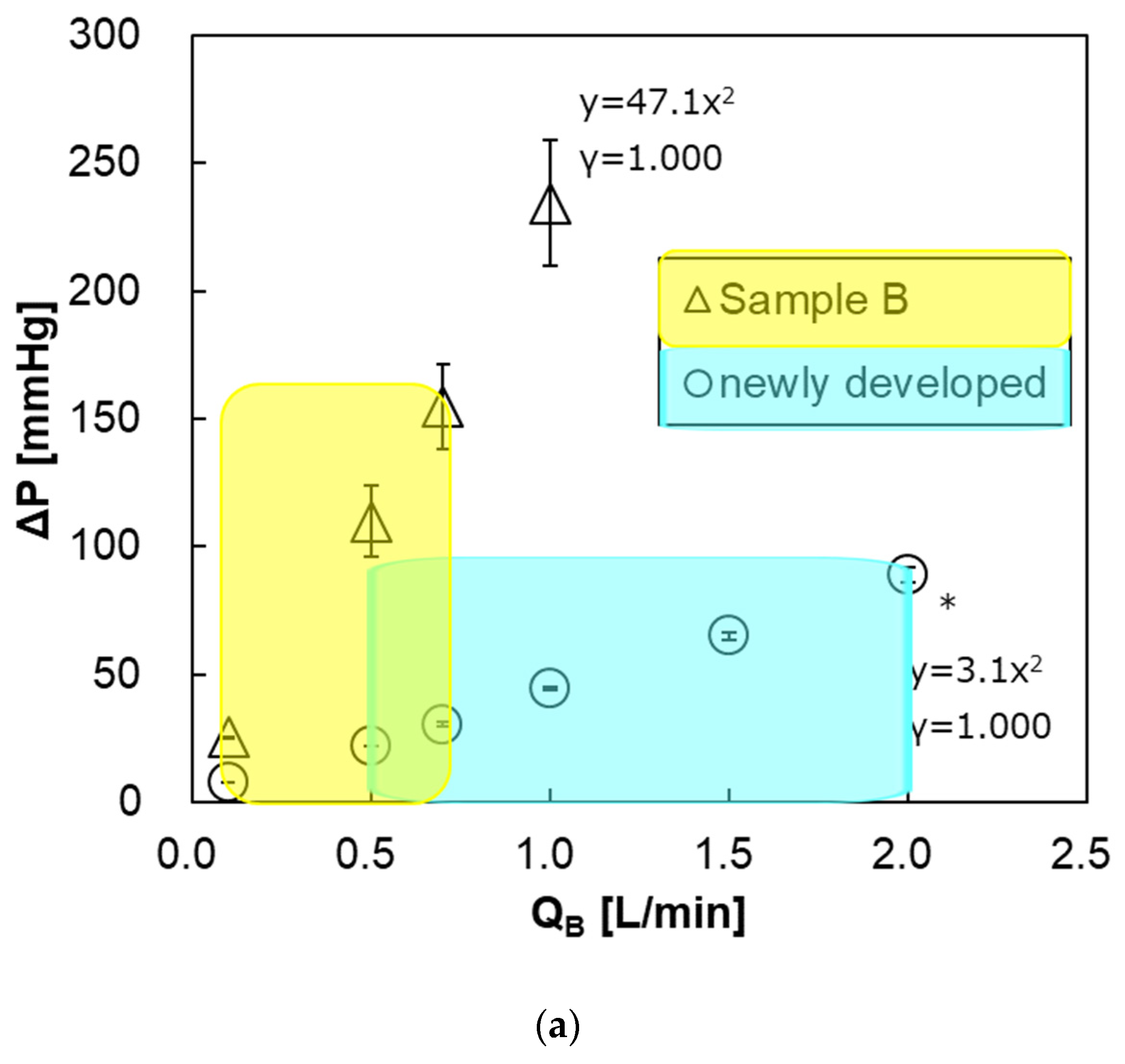
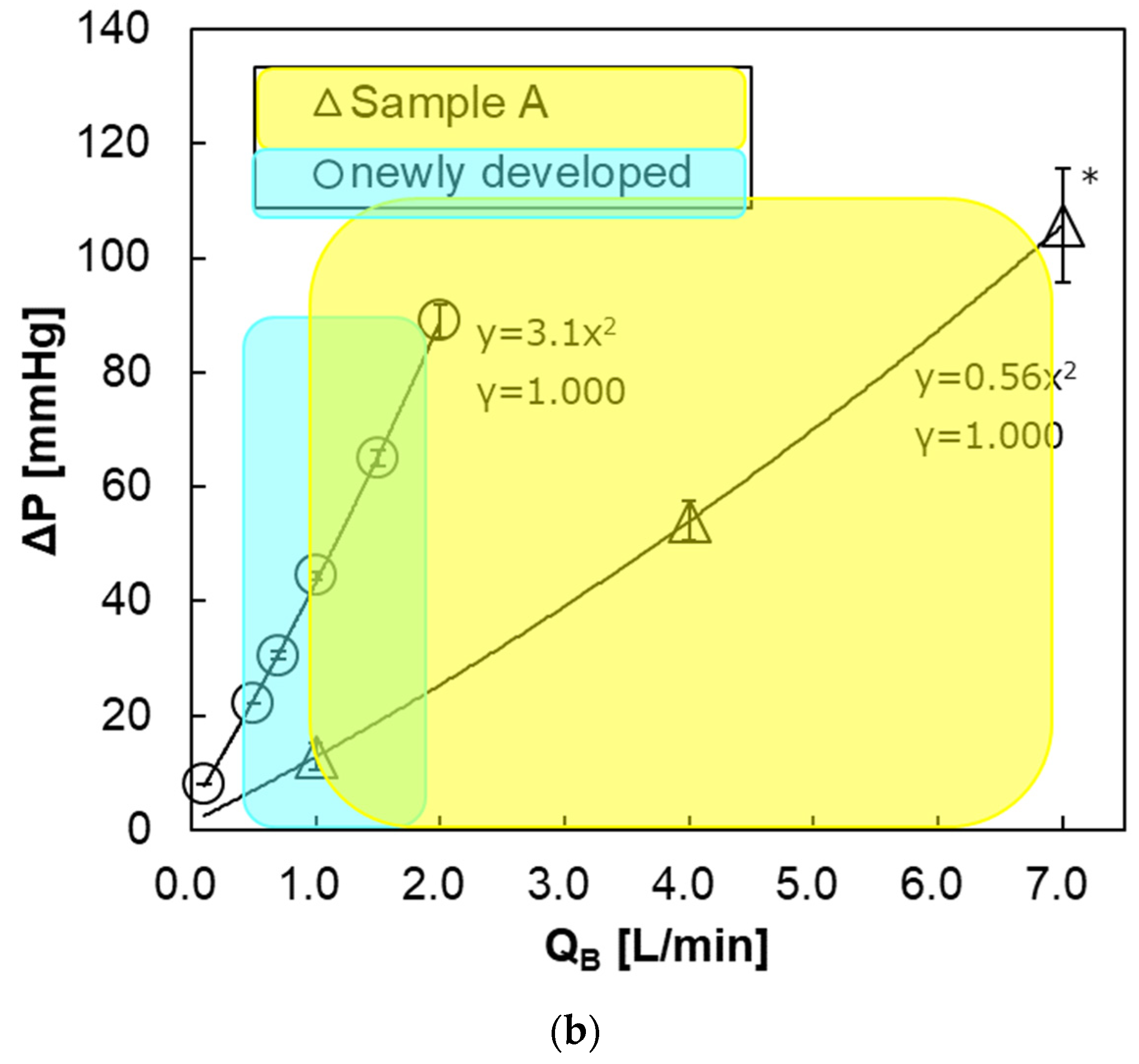
3.5. Pressure Drop of Blood Flow Channel
3.6. Determination of Oxygen and Carbon Dioxide Transfer Rates
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| CaCO2 | arterial carbon dioxide content (mL/dL) |
| CvCO2 | venous carbon dioxide content (mL/dL) |
| FiO2 | inspired oxygen fractional concentration (%) |
| KCO2 | carbon dioxide transfer rate (mL/min) |
| KO2 | oxygen transfer rate (mL/min) |
| Hb | hemoglobin concentration (g/dL) |
| P | pressure (mmHg) |
| ΔP | pressure drop (mmHg) |
| PaO2 | arterial partial pressure (mmHg) |
| PvO2 | venous partial pressure (mmHg) |
| QB | flow rate of blood side (mL/min) |
| SaO2 | arterial oxygen saturation (%) |
| SvO2 | venous oxygen saturation (%) |
| TaCO2 | arterial carbon dioxide content (mmol/dL) |
| TvCO2 | venous carbon dioxide content (mmol/dL) |
| V | flow rate of gas side (mL/min) |
| Greek letters | |
| a | artery |
| B | blood |
| i | inlet |
| o | outlet |
| v | vein |
References
- Japanese ECMOnet for COVID-19. Available online: https://www.jaam.jp/info/COVID-19.html (accessed on 1 August 2020).
- Ohshimo, S.; Shime, N.; Nakagawa, S.; Nishida, O.; Takeda, S.; Committee of the Japan ECMO Project. Comparison of extracorporeal membrane oxygenation outcome for influenza-associated acute respiratory failure in Japan between 2009 and 2016. J. Intensive Care 2018, 6, 38. [Google Scholar] [CrossRef] [PubMed]
- Peek, G.J.; Mugford, M.; Tiruvoipati, R.; Wilson, A.; Allen, E.; Thalanany, M.M.; Hibbert, C.L.; Truesdale, A.; Clemens, F.; Cooper, N.; et al. Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): A multicentre randomised controlled trial. Lancet 2009, 374, 1351–1363. [Google Scholar] [CrossRef]
- Blomback, M.; Kronlund, P.; Aberg, B.; Fatah, K.; Hansson, L.O.; Egberg, N.; Moor, E.; Carlsson, K. Channelologic fibrin formation and cold-induced clotting of membrane oxygenators during cardiopulmonary bypass. J. Cardiothorac. Vasc. Anesth. 1995, 9, 34–43. [Google Scholar] [CrossRef]
- Eugene, A.H., II. Chapter 5: Circuitry and Cannulation Techniques. In Cardiopulmonary Bypass Principles and Practice, 3rd ed.; Gravlee, G.P., Davis, R.F., Stammers, A.H., Ungerleider, R.M., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2008; pp. 63–113. [Google Scholar]
- Fisher, A.R.; Baker, M.; Buffin, M.; Campbell, P.; Hansbro, S.; Kennington, S.; Lilley, A.; Whitehorne, M. Normal and abnormal trans-oxygenator pressure gradients during cardiopulmonary bypass. Perfusion 2003, 18, 25–30. [Google Scholar] [CrossRef]
- Myers, G.J.; Weighell, P.R.; McCloskey, B.J.; Holt, A.M.; McTeer, S.; Maxwell, S.L. A multicenter investigation into the occurrence of high-pressure excursions. J. Extra Corpor. Technol. 2003, 35, 127–132. [Google Scholar]
- Ündar, A.; Owens, W.R.; McGarry, M.C.; Surprise, D.L.; Kilpack, V.D.; Mueller, M.W.; McKenzie, E.D.; Fraser, J.C.D. Comparison of hollow-fiber membrane oxygenators in terms of pressure drop of the membranes during normothermic and hypothermic cardiopulmonary bypass in neonates. Perfusion 2005, 20, 135–138. [Google Scholar] [CrossRef]
- Izumi, R. To reduce complications in pediatric extracorporeal circulation. Jpn. J. Extra Corpor. Technol. 2019, 46, 274. (In Japanese) [Google Scholar]
- Iwaki, S.; Tani, S.; Yoshida, Y.; Taka, H. Why do the excessive pressure drops in pediatric membrane oxygenator not decrease? Jpn. J. Extra Corpor. Technol. 2019, 46, 283. (In Japanese) [Google Scholar]
- Sakai, K.; Yanagisawa, M.; Hosoya, N.; Ohmura, T.; Sakagami, M.; Kuwano, K.; Nakanishi, H. Comparison of oxygenation and flow characteristics of inside and outside blood flow membrane oxygenators. Artif Organs Today 1993, 3, 57–80. [Google Scholar]
- Matsuda, N.; Sakai, K. Blood flow and oxygen transfer rate of an outside blood flow membrane oxygenator. J. Membr. Sci. 2000, 170, 153–158. [Google Scholar] [CrossRef]
- Matsuda, N.; Sakai, K.; Yamamoto, K.-I.; Iwasaki, H. Effects of hollow fiber packing fraction on blood flow pattern and gas transfer rate of an intravascular oxygenator (IVOX). J. Membr. Sci. 2000, 179, 231–241. [Google Scholar] [CrossRef]
- Funakubo, A.; Taga, I.; McGillicuddy, J.W.; Fukui, Y.; Hirschl, R.B.; Bartlett, R.H. Flow vectorial analysis in an artificial implantable lung. ASAIO J. 2003, 49, 383–387. [Google Scholar] [PubMed]
- Catapano, G. Turbulent flow technique for the estimation of oxygen diffusive permeability of membranes for the oxygenation of blood and other cell suspensions. J. Membr. Sci. 2004, 230, 131–139. [Google Scholar] [CrossRef]
- Zhang, J.; Nolan, T.D.; Zhang, T.; Griffith, B.P.; Wu, Z.J. Characterization of membrane blood oxygenation devices using computational fluid dynamics. J. Membr. Sci. 2007, 288, 268–279. [Google Scholar] [CrossRef]
- Tabesh, H.; Amoabediny, G.; Poorkhalil, A.; Khachab, A.; Kashefi, A.; Mottaghy, K. A theoretical model for evaluation of the design of a hollow-fiber membrane oxygenator. J. Artif. Organs 2012, 15, 347–356. [Google Scholar] [CrossRef]
- Hirano, A.; Yamamoto, K.-I.; Matsuda, M.; Inoue, M.; Nagao, S.; Kuwana, K.; Kamiya, M.; Sakai, K. Flow Uniformity in Oxygenators with Different Outlet Port Design. ASAIO J. 2009, 55, 209–212. [Google Scholar] [CrossRef] [PubMed]
- ISO5636-5(2013), Paper and Board – Determination of Air Permeance (Medium Range)—Part 5: Gurley Method; ISO Technical Committee: Geneva, Switzerlnd, 2013.
- Fukuda, M.; Izumi, R. Analysis of fluid flow in a membrane oxygenator device non-destructively. Patent 045272, 31 August 2017. [Google Scholar]
- Ministry of Health, Labour and Welfare. Chapter II Controlled Areas; Exposure Dose Limits and Measurements (Indications of Controlled Areas) Article 3, Regulation on Prevention of Ionizing Radiation Hazards, Ministry of Labour Order No. 41; Ministry of Health, Labour and Welfare: Tokyo, Japan, 1972. [Google Scholar]
- ISO 7199. Third Edition: 2016 Cardiovascular Implants and Artificial Organs—Blood-Gas Exchangers (Oxygenators); International Organization for Standardization: London, UK, 2016; pp. 11–15. [Google Scholar]
- Galletti, P.M.; Richardson, P.D.; Snider, M.T.; Friedman, L.I. A standardized method for defining the overall gas transfer performance of membrane oxygenators. ASAIO J. 1972, 18, 359–368. [Google Scholar] [CrossRef]
- Evseev, A.K.; Zhuravel, S.V.; Alentiev, A.Y.; Goroncharovskaya, I.V.; Petrikov, S.S. Membranes in Extracorporeal Blood Oxygenation Technology. Membr. Technol. 2019, 1, 201–211. [Google Scholar] [CrossRef]
- Meyns, B.; Vercaemst, L.; Vandezande, E.; Bollen, H.; Vlasselaers, D. Plasma Leakage of Oxygenators in ECMO Depends on the Type of Oxygenator and on Patient Variables. Int. J. Artif. Organs 2005, 28, 30–34. [Google Scholar] [CrossRef]
- Fournier, R.L. Chapter 9: Extracorporeal devices. In Basic Transport Phenomena in Biomedical Engineering, 4th ed.; Fournier, R.L., Ed.; CRC Press: Boca Raton, FL, USA, 2017; pp. 451–514. [Google Scholar]
- Hagiwara, K.; Innami, K.; Yokoyama, K.; Kitoh, H.; Nogawa, A.; Muramoto, T.; Tatebe, K.; Seita, Y.; Fukasawa, H. An approach to the microporous hollow fiber for the ECMO oxygenator—Micopore characterization of the gas exchange performance, plasma leakage, and hydrophilization of the inner surface of fibers. Jpn. J. Artif. Organs 1992, 21, 720–726. [Google Scholar]
- Yamamoto, K.-I.; Hayama, M.; Matsuda, M.; Yakushiji, T.; Fukuda, M.; Miyasaka, T.; Sakai, K. Evaluation of asymmetrical structure dialysis membrane by tortuous capillary pore diffusion model. J. Membr. Sci. 2007, 287, 88–93. [Google Scholar] [CrossRef]
- Yamazaki, K.; Matsuda, M.; Yamamoto, K.-I.; Yakushiji, T.; Sakai, K. Internal and surface structure characterization of cellulose triacetate hollow-fiber dialysis membranes. J. Membr. Sci. 2011, 368, 34–40. [Google Scholar] [CrossRef]
- Fukuda, M.; Saomoto, H.; Mori, T.; Yoshimoto, H.; Kusumi, R.; Sakai, K. Impact of three-dimensional tortuous pore structure on polyethersulfone membrane morphology and mass transfer properties from a manufacturing perspective. J. Artif. Organs 2020, 23, 171–179. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, M.; Yoshimoto, H.; Saomoto, H.; Sakai, K. Validity of Three-Dimensional Tortuous Pore Structure and Fouling of Hemoconcentration Capillary Membrane Using the Tortuous Pore Diffusion Model and Scanning Probe Microscopy. Membranes 2020, 10, 315. [Google Scholar] [CrossRef] [PubMed]



















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample (Product) | Commercially Available Membrane Oxygenator Sample A | Newly Developed Pediatric Membrane Oxygenator Prototype | Commercially Available Membrane Oxygenator 1) Kids D100 Sample B | Commercially Available Membrane Oxygenator CAPIOX® FX05 Sample C |
|---|---|---|---|---|
| Manufacturer | JMS Co., Ltd., Japan | ― | LivaNova Co., Ltd., Sorin Group, Italy | Terumo Co., Ltd., Japan |
| Membrane area [m2] 2) | 1.7 | 0.39 | 0.22 | 0.5 |
| Material of hollow fiber membrane Pore structure 3) | Polypropylene (PP), asymmetric pore structure | Polypropylene (PP), asymmetric pore structure | Polypropylene (PP) | Polypropylene (PP) |
| Inner diameter of lumen [µm] (n = 30) | 238 ± 5 | 238 ± 5 | 233 ± 14 | 195 ± 8 |
| Membrane thickness [µm] (n = 30) | 35 ± 1 | 35 ± 1 | 34 ± 1 | 57 ± 6 |
| Number of hollow fibers [-] | 19,500 | 9000 | - | - |
| Length of hollow fiber [mm] | 90 | 45 | - | - |
| Air permeability 4) [sec] | 35.1 ± 1.4 | 33.8 ± 0.4 | - | - |
| Antithromboge-nic material coating for blood flow channel | Poly(2-methacryloyloxyethyl phosphoryl choline) (PMPC) | Poly(2-methacryloyloxyethyl phosphoryl choline) (PMPC) | poly(2-methacryloyloxyethyl phosphoryl choline) (PMPC) | poly(hydoroxyethylmetharylate) (PHEMA) |
| Priming volume [mL] | 245 | 37 | 31 | 43 |
| Range of blood flow rate (Max QB) [L/min] | 1.0–7.0 (7.0) | 0.5–2.0 (2.0) | 0.1–0.7 (0.7) | −1.5 (1.5) |
| Calculated retention time [s] 5) | 2.1 | 1.1 | 2.6 | 1.7 |
| Sample (Product) | Commercially Available Membrane Oxygenator Sample A | Newly Developed Pediatric Membrane Oxygenator Prototype | Commercially Available MEMBRANE Oxygenator Kids D100 Sample B |
|---|---|---|---|
| Maximum oxygen transfer rate [mL/min, STP] | 433 (Max QB = 7 L/min) | 116 (Max QB = 2 L/min) | 43 (Max QB = 0.7 L/min) |
| Maximum carbon dioxide transfer rate [mL/min, STP] (V/Q = 1.0) | 355 | 98 | 38 |
| Pressure drop of the blood flow channel [mmHg] | 106 (Max QB = 7 L/min) | 89 (Max QB = 2 L/min) | 155 (Max QB = 0.7 L/min) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fukuda, M.; Tokumine, A.; Noda, K.; Sakai, K. Newly Developed Pediatric Membrane Oxygenator that Suppresses Excessive Pressure Drop in Cardiopulmonary Bypass and Extracorporeal Membrane Oxygenation (ECMO). Membranes 2020, 10, 362. https://doi.org/10.3390/membranes10110362
Fukuda M, Tokumine A, Noda K, Sakai K. Newly Developed Pediatric Membrane Oxygenator that Suppresses Excessive Pressure Drop in Cardiopulmonary Bypass and Extracorporeal Membrane Oxygenation (ECMO). Membranes. 2020; 10(11):362. https://doi.org/10.3390/membranes10110362
Chicago/Turabian StyleFukuda, Makoto, Asako Tokumine, Kyohei Noda, and Kiyotaka Sakai. 2020. "Newly Developed Pediatric Membrane Oxygenator that Suppresses Excessive Pressure Drop in Cardiopulmonary Bypass and Extracorporeal Membrane Oxygenation (ECMO)" Membranes 10, no. 11: 362. https://doi.org/10.3390/membranes10110362
APA StyleFukuda, M., Tokumine, A., Noda, K., & Sakai, K. (2020). Newly Developed Pediatric Membrane Oxygenator that Suppresses Excessive Pressure Drop in Cardiopulmonary Bypass and Extracorporeal Membrane Oxygenation (ECMO). Membranes, 10(11), 362. https://doi.org/10.3390/membranes10110362