
Exploring Psychological Factors for COVID-19 Vaccination Intention in Taiwan



Abstract
:1. Introduction
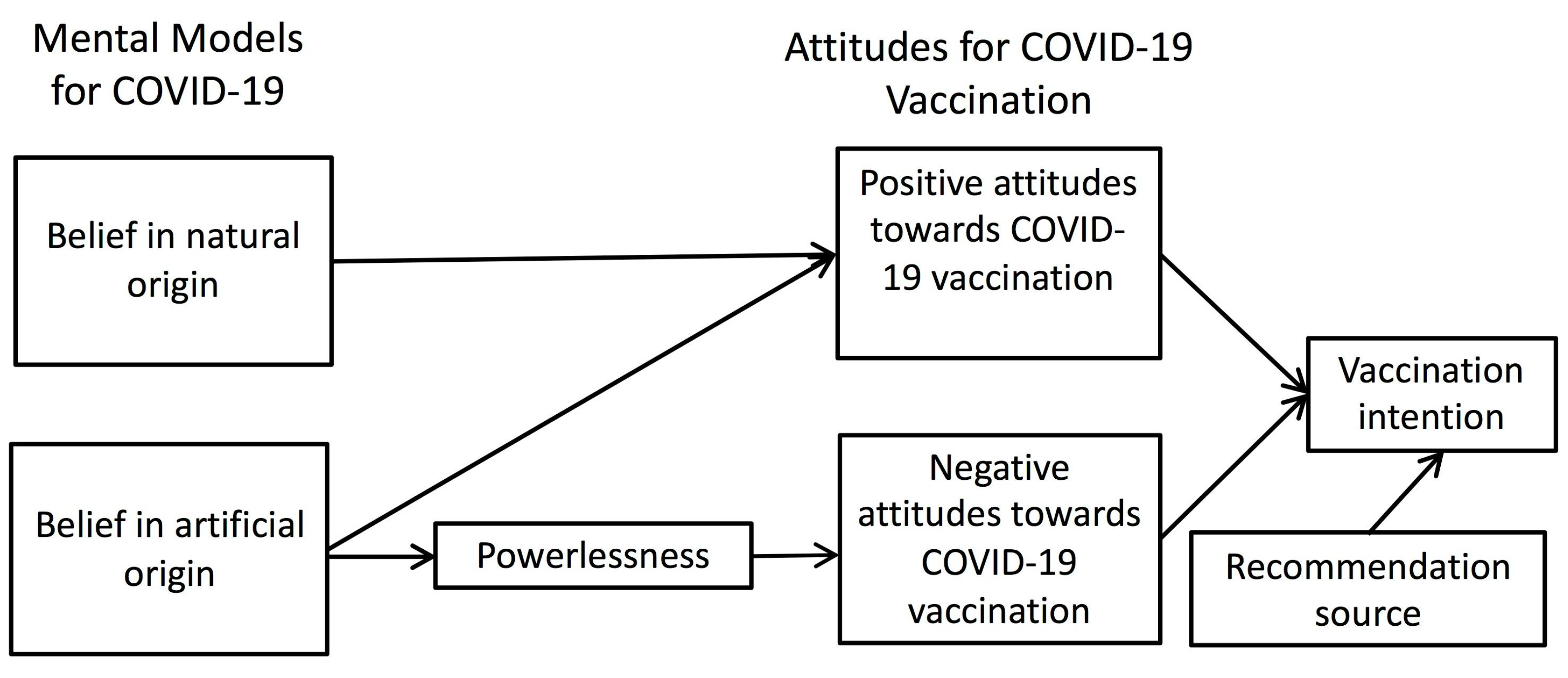
1.1. Mental Models for COVID-19
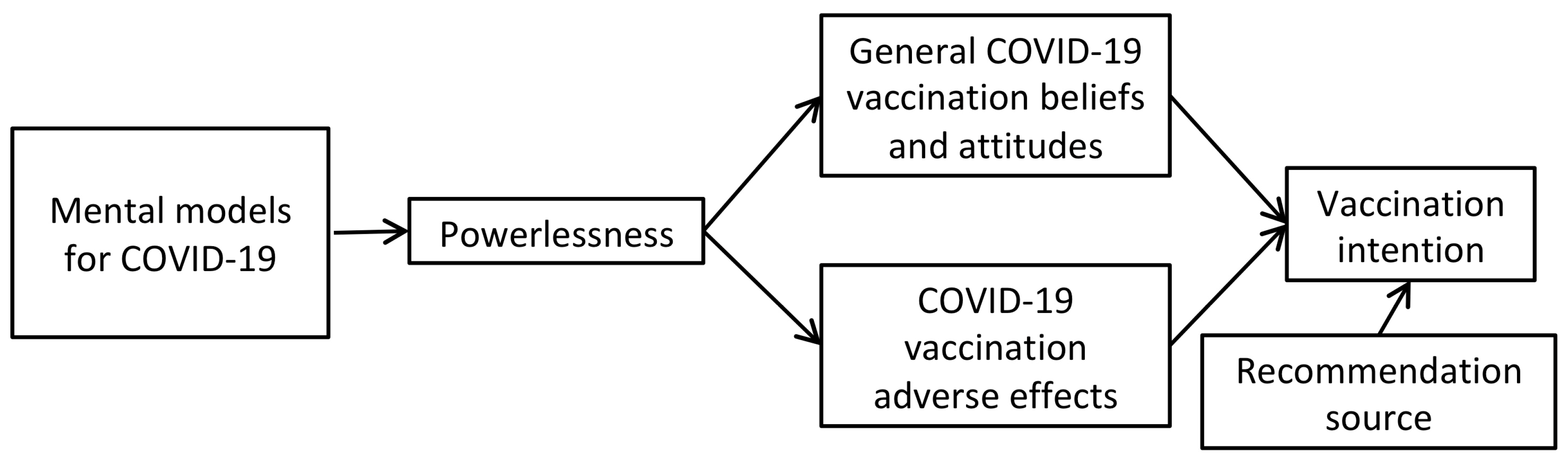
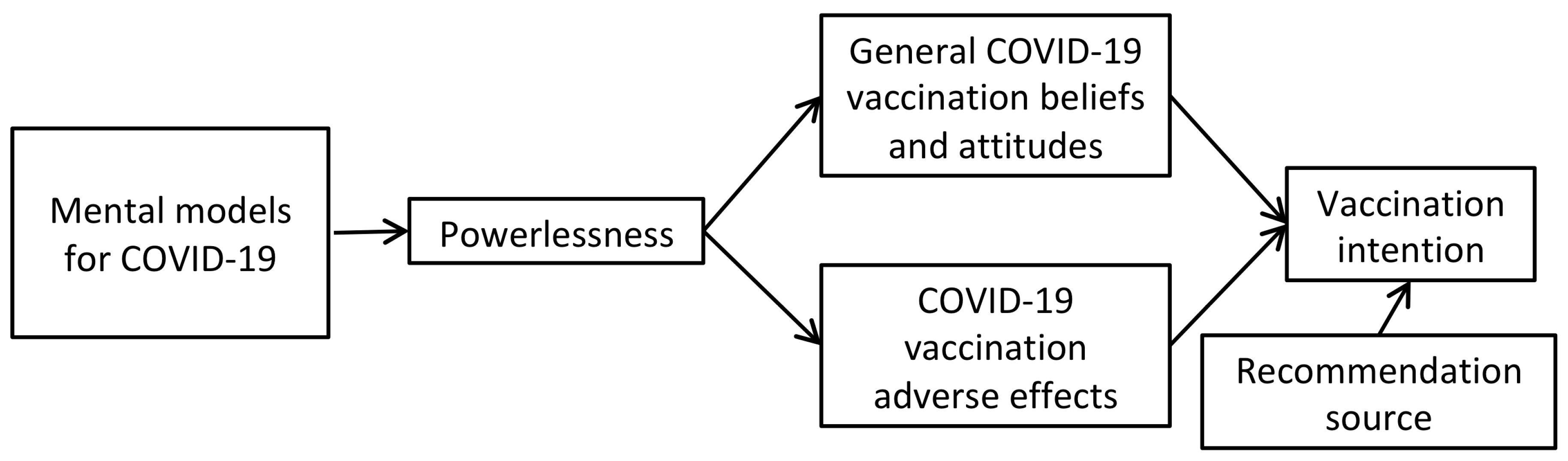
1.2. Aims and Hypothesis
2. Materials and Methods
2.1. Participants
2.2. Materials
3. Results
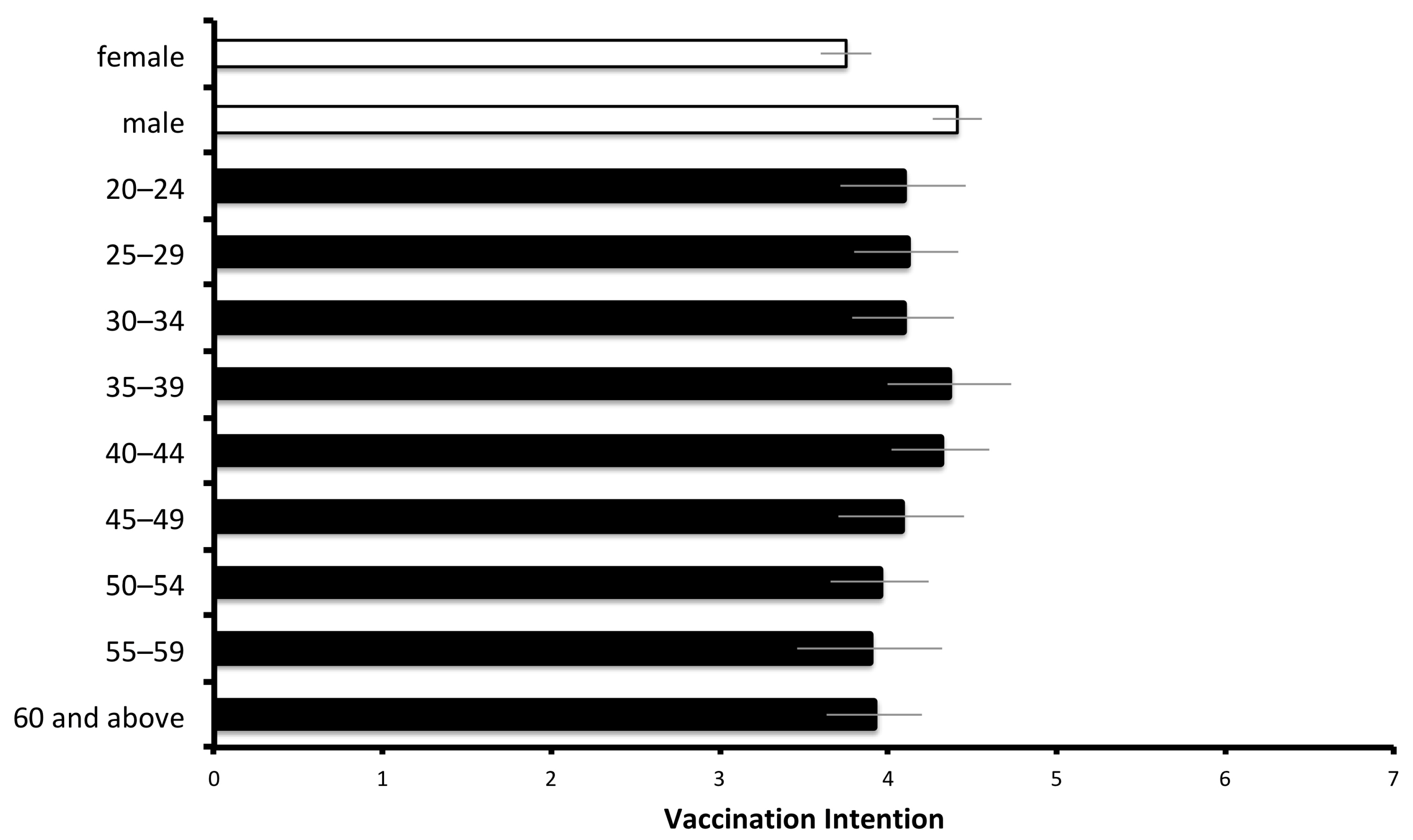
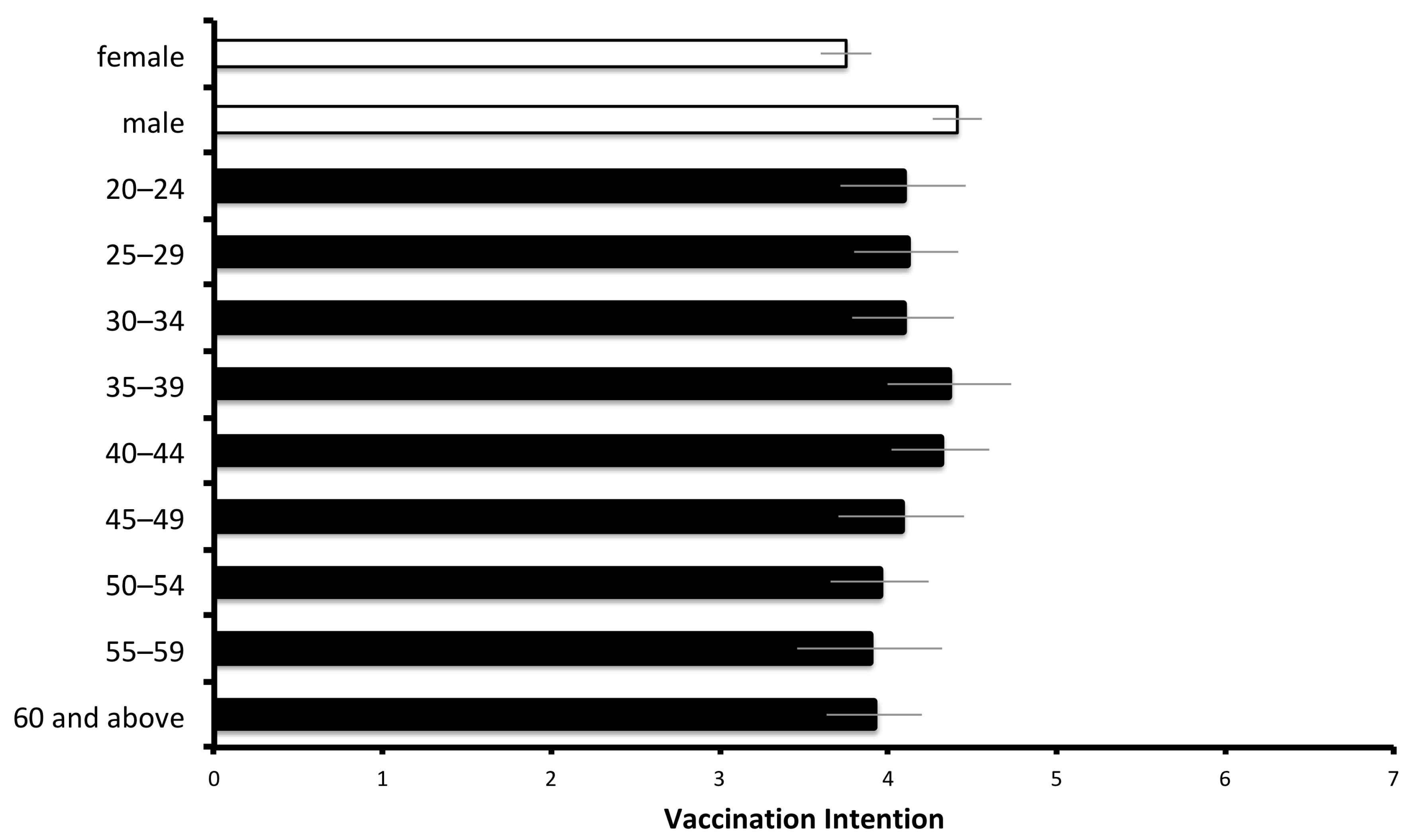
3.1. Demographic Factors
3.2. Recommendation Source
3.3. Attitudes toward Vaccination
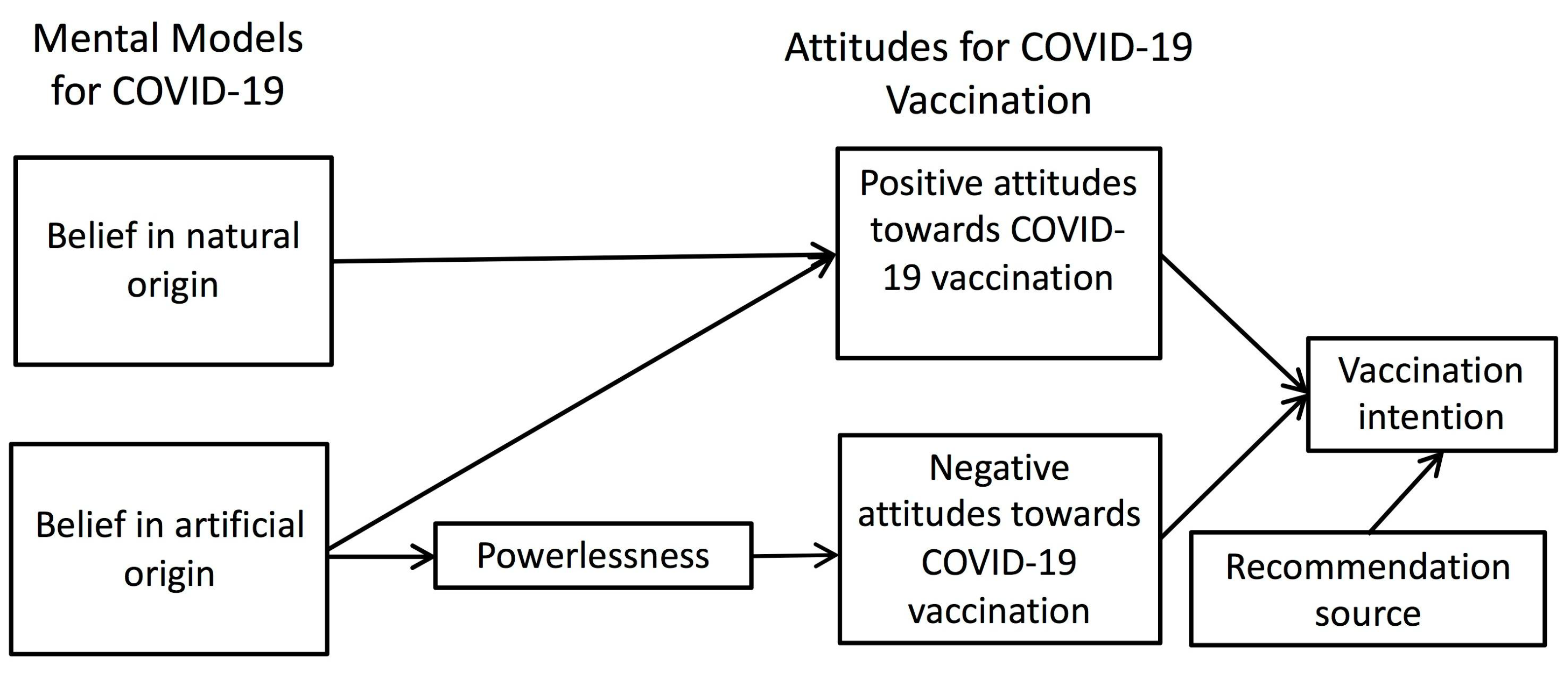
3.4. Mental Models for COVID-19
3.5. Mediation Analysis
4. Discussion
4.1. Demographic Factors of Vaccination Intention
4.2. Recommendation Source
4.3. Mental Models
4.4. Research Limitations and Practical Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dyer, O. Covid-19: Variants are spreading in countries with low vaccination rates. Br. Med J. 2021, 373, n1359. [Google Scholar] [CrossRef] [PubMed]
- Soares, P.; Rocha, J.V.; Moniz, M.; Gama, A.; Laires, P.A.; Pedro, A.R.; Dias, S.; Leite, A.; Nunes, C. Factors associated with COVID-19 vaccine hesitancy. Vaccines 2021, 9, 300. [Google Scholar] [CrossRef]
- Wang, J.; Jing, R.; Lai, X.; Zhang, H.; Lyu, Y.; Knoll, M.D.; Fang, H. Acceptance of COVID-19 vaccination during the COVID-19 Pandemic in China. Vaccines 2020, 8, 482. [Google Scholar] [CrossRef]
- Harapan, H.; Wagner, A.L.; Yufika, A.; Winardi, W.; Anwar, S.; Gan, A.K.; Setiawan, A.M.; Rajamoorthy, Y.; Sofyan, H.; Mudatsir, M. Acceptance of a COVID-19 vaccine in southeast Asia: A cross-sectional study in Indonesia. Front. Public Health 2020, 8, 381. [Google Scholar] [CrossRef]
- Murphy, J.; Vallières, F.; Bentall, R.P.; Shevlin, M.; McBride, O.; Hartman, T.K.; McKay, R.; Bennett, K.; Mason, L.; Gibson-Miller, J. Psychological characteristics associated with COVID-19 vaccine hesitancy and resistance in Ireland and the United Kingdom. Nat. Commun. 2021, 12, 1–15. [Google Scholar] [CrossRef]
- Yoda, T.; Katsuyama, H. Willingness to receive COVID-19 vaccination in Japan. Vaccines 2021, 9, 48. [Google Scholar] [CrossRef] [PubMed]
- Sherman, S.M.; Smith, L.E.; Sim, J.; Amlôt, R.; Cutts, M.; Dasch, H.; Rubin, G.J.; Sevdalis, N. COVID-19 vaccination intention in the UK: Results from the COVID-19 vaccination acceptability study (CoVAccS), a nationally representative cross-sectional survey. Hum. Vaccines Immunother. 2020, 17, 1612–1621. [Google Scholar] [CrossRef] [PubMed]
- Williams, L.; Flowers, P.; McLeod, J.; Young, D.; Rollins, L. Social patterning and stability of intention to accept a COVID-19 vaccine in Scotland: Will those most at risk accept a vaccine? Vaccines 2021, 9, 17. [Google Scholar] [CrossRef] [PubMed]
- Reiter, P.L.; Pennell, M.L.; Katz, M.L. Acceptability of a COVID-19 vaccine among adults in the United States: How many people would get vaccinated? Vaccine 2020, 38, 6500–6507. [Google Scholar] [CrossRef]
- Janz, N.K.; Becker, M.H. The health belief model: A decade later. Health Educ. Q. 1984, 11, 1–47. [Google Scholar] [CrossRef] [Green Version]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Rogers, R.W.; Prentice-Dunn, S. Protection motivation theory. In Handbook of Health Behavior Research 1: Personal and Social Determinants; Gochman, D.S., Ed.; Plenum Press: New York, NY, USA, 1997; pp. 113–132. [Google Scholar]
- Johnson-Laird, P.N. Mental Models: Towards a Cognitive Science of Language, Inference, and Consciousness; Harvard University Press: Cambridge, MA, USA, 1983; 528p. [Google Scholar]
- Johnson-Laird, P.N. Mental models and human reasoning. Proc. Natl. Acad. Sci. USA 2010, 107, 18243–18250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson-Laird, P.N. Inference with mental models. In The Oxford Handbook of Thinking and Reasoning; Holyoak, K.J., Morrison, R.G., Eds.; Oxford University Press: Oxford, UK, 2012; pp. 134–145. [Google Scholar]
- Douglas, K.M.; Sutton, R.M. Does it take one to know one? Endorsement of conspiracy theories is influenced by personal willingness to conspire. Br. J. Soc. Psychol. 2011, 50, 544–552. [Google Scholar] [CrossRef] [Green Version]
- Goertzel, T. Belief in conspiracy theories. Political Psychol. 1994, 15, 731–742. [Google Scholar] [CrossRef]
- McCauley, C.; Jacques, S. The popularity of conspiracy theories of presidential assassination: A Bayesian analysis. J. Personal. Soc. Psychol. 1979, 37, 637. [Google Scholar] [CrossRef]
- Swami, V.; Coles, R. The truth is out there: Belief in conspiracy theories. Psychologist 2010, 23, 560–563. [Google Scholar]
- Wood, M.J.; Douglas, K.M.; Sutton, R.M. Dead and alive: Beliefs in contradictory conspiracy theories. Soc. Psychol. Personal. Sci. 2012, 3, 767–773. [Google Scholar] [CrossRef] [Green Version]
- Biddlestone, M.; Green, R.; Douglas, K.M. Cultural orientation, power, belief in conspiracy theories, and intentions to reduce the spread of COVID-19. Br. J. Soc. Psychol. 2020, 59, 663–673. [Google Scholar] [CrossRef] [PubMed]
- Bertin, P.; Nera, K.; Delouvée, S. Conspiracy beliefs, rejection of vaccination, and support for hydroxychloroquine: A conceptual replication-extension in the COVID-19 pandemic context. Front. Psychol. 2020, 11, 2471. [Google Scholar] [CrossRef]
- Freeman, D.; Loe, B.S.; Chadwick, A.; Vaccari, C.; Waite, F.; Rosebrock, L.; Jenner, L.; Petit, A.; Lewandowsky, S.; Vanderslott, S. COVID-19 vaccine hesitancy in the UK: The Oxford coronavirus explanations, attitudes, and narratives survey (Oceans) II. Psychol. Med. Available online: https://www.cambridge.org/core/journals/psychological-medicine/article/covid19-vaccine-hesitancy-in-the-uk-the-oxford-coronavirus-explanations-attitudes-and-narratives-survey-oceans-ii/C30FDB5C3D87123F28E351FDAAD5351A (accessed on 8 July 2021).
- Pivetti, M.; Melotti, G.; Bonomo, M.; Hakoköngäs, E. Conspiracy beliefs and acceptance of COVID-vaccine: An exploratory study in Italy. Soc. Sci. 2021, 10, 108. [Google Scholar] [CrossRef]
- Roozenbeek, J.; Schneider, C.R.; Dryhurst, S.; Kerr, J.; Freeman, A.L.; Recchia, G.; Van Der Bles, A.M.; Van Der Linden, S. Susceptibility to misinformation about COVID-19 around the world. R. Soc. Open Sci. 2020, 7, 201199. [Google Scholar] [CrossRef]
- Jolley, D.; Douglas, K.M. The social consequences of conspiracism: Exposure to conspiracy theories decreases intentions to engage in politics and to reduce one’s carbon footprint. Br. J. Psychol. 2014, 105, 35–56. [Google Scholar] [CrossRef]
- Bogart, L.M.; Thorburn, S. Relationship of African Americans’ sociodemographic characteristics to belief in conspiracies about HIV/AIDS and birth control. J. Natl. Med Assoc. 2006, 98, 1144. [Google Scholar]
- Soveri, A.; Karlsson, L.C.; Antfolk, J.; Lindfelt, M.; Lewandowsky, S. Unwillingness to engage in behaviors that protect against COVID-19: The role of conspiracy beliefs, trust, and endorsement of complementary and alternative medicine. BMC Public Health 2021, 21, 1–12. [Google Scholar] [CrossRef]
- National Development Council. 2019 Digital Opportunity Survey for Individuals and Households. Available online: https://www.ndc.gov.tw/en/News2.aspx?n=78871F8A656B4BA5&sms=A2B4856EC48AD4BB (accessed on 7 July 2021).
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford publications: New York, NY, USA, 2017; 507p. [Google Scholar]
- Moran, K.R.; Del Valle, S.Y. A meta-analysis of the association between gender and protective behaviors in response to respiratory epidemics and pandemics. PLoS ONE 2016, 11, e0164541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baumgaertner, B.; Ridenhour, B.J.; Justwan, F.; Carlisle, J.E.; Miller, C.R. Risk of disease and willingness to vaccinate in the United States: A population-based survey. PLoS Med. 2020, 17, e1003354. [Google Scholar] [CrossRef] [PubMed]
- Bish, A.; Yardley, L.; Nicoll, A.; Michie, S. Factors associated with uptake of vaccination against pandemic influenza: A systematic review. Vaccine 2011, 29, 6472–6484. [Google Scholar] [CrossRef] [PubMed]
- Brien, S.; Kwong, J.C.; Buckeridge, D.L. The determinants of 2009 pandemic A/H1N1 influenza vaccination: A systematic review. Vaccine 2012, 30, 1255–1264. [Google Scholar] [CrossRef]
- Neumann-Böhme, S.; Varghese, N.E.; Sabat, I.; Barros, P.P.; Brouwer, W.; van Exel, J.; Schreyögg, J.; Stargardt, T. Once we have it, will we use it? A European survey on willingness to be vaccinated against COVID-19. Eur. J. Health Econ. 2020, 21, 977–982. [Google Scholar] [CrossRef]
- Joseph, J.G.; Montgomery, S.B.; Emmons, C.-A.; Kessler, R.C.; Ostrow, D.G.; Wortman, C.B.; O’Brien, K.; Eller, M.; Eshleman, S. Magnitude and determinants of behavioral risk reduction: Longitudinal analysis of a cohort at risk for AIDS. Psychol. Health 1987, 1, 73–95. [Google Scholar]
- Jolley, D.; Douglas, K.M. The effects of anti-vaccine conspiracy theories on vaccination intentions. PLoS ONE 2014, 9, e89177. [Google Scholar] [CrossRef] [PubMed]
- Randolph, H.E.; Barreiro, L.B. Herd immunity: Understanding COVID-19. Immunity 2020, 52, 737–741. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.M.; May, R.M. Vaccination and herd immunity to infectious diseases. Nature 1985, 318, 323–329. [Google Scholar] [CrossRef]
- Mathieu, E.; Ritchie, H.; Ortiz-Ospina, E.; Roser, M.; Hasell, J.; Appel, C.; Giattino, C.; Rodés-Guirao, L. A global database of COVID-19 vaccinations. Nat. Hum. Behav. Available online: https://www.nature.com/articles/s41562-021-01122-8#citeas (accessed on 8 July 2021).

{kind=link}
{kind=link}
{kind=link}
| Construct | Items | Factor Loading |
|---|---|---|
| Positive attitudes toward COVID-19 vaccines (variance explained: 38%) | A coronavirus vaccination should be mandatory for everyone who is able to have it. | 0.68 |
| If I get a coronavirus vaccination, I will be protected against coronavirus. | 0.77 | |
| If I don’t get a coronavirus vaccination and end up getting coronavirus, I would regret not getting the vaccination. | 0.72 | |
| Other people like me will get a coronavirus vaccination. | 0.84 | |
| My family would approve of my having a coronavirus vaccination. | 0.80 | |
| My friends would approve of my having a coronavirus vaccination. | 0.77 | |
| A coronavirus vaccine will allow us to get back to ‘normal’. | 0.82 | |
| Negative attitudes toward COVID-19 vaccines | I would be worried about experiencing side-effects from a coronavirus vaccination. | 0.74 |
| (variance explained: 17%) | I might regret getting a coronavirus vaccination if I later experienced side-effects from the vaccination. | 0.75 |
| A coronavirus vaccination will be too new for me to be confident about getting vaccinated. | 0.75 | |
| Belief of vaccine-induced infection (variance explained: 4%) | A coronavirus vaccination could give me coronavirus. | 0.39 |
| Independent Variable | Outcome Variable | r2 | β | Statistical Tests |
|---|---|---|---|---|
| Positive attitudes | Vaccination intention | 0.67 | 0.77 | t (1097) = 42.56, p < 0.001 |
| Negative attitudes | −0.12 | t (1097) = −6.56, p < 0.001 | ||
| Belief in natural origin | Positive attitudes | 0.05 | 0.14 | t (1097) = 4.64, p < 0.001 |
| Belief in artificial origin | 0.21 | t (1097) = 7.14, p < 0.001 | ||
| Belief in natural origin | Negative attitudes | 0.004 | n.s. | n.s. |
| Belief in artificial origin | 0.07 | t (1098) = 2.16, p = 0.03) | ||
| Powerlessness | Positive attitudes | 0.002 | 0.05 | n.s. |
| Powerlessness | Negative attitudes | 0.03 | 0.18 | t (1098) = 6.04, p < 0.001 |
| Independent Variable | Outcome Variable | Notes | Statistical Test |
|---|---|---|---|
| Belief in artificial origin | Powerlessness | t (1098) = 5.33, p < 0.001 | |
| Powerlessness | Negative attitudes | t (1097) = 5.76, p < 0.001 | |
| Belief in artificial origin | Negative attitudes | Total effect | t (1098) = 2.16, p = 0.03 |
| Belief in artificial origin | Negative attitudes | Indirect effect | 95% CI 0.01–0.04 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lo, S.-Y.; Li, S.-C.S.; Wu, T.-Y. Exploring Psychological Factors for COVID-19 Vaccination Intention in Taiwan. Vaccines 2021, 9, 764. https://doi.org/10.3390/vaccines9070764
Lo S-Y, Li S-CS, Wu T-Y. Exploring Psychological Factors for COVID-19 Vaccination Intention in Taiwan. Vaccines. 2021; 9(7):764. https://doi.org/10.3390/vaccines9070764
Chicago/Turabian StyleLo, Shih-Yu, Shu-Chu Sarrina Li, and Tai-Yee Wu. 2021. "Exploring Psychological Factors for COVID-19 Vaccination Intention in Taiwan" Vaccines 9, no. 7: 764. https://doi.org/10.3390/vaccines9070764
APA StyleLo, S.-Y., Li, S.-C. S., & Wu, T.-Y. (2021). Exploring Psychological Factors for COVID-19 Vaccination Intention in Taiwan. Vaccines, 9(7), 764. https://doi.org/10.3390/vaccines9070764