
Association of Influenza Vaccination and Prognosis in Patients Testing Positive to SARS-CoV-2 Swab Test: A Large-Scale Italian Multi-Database Cohort Study

 , , ,
, , ,  , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
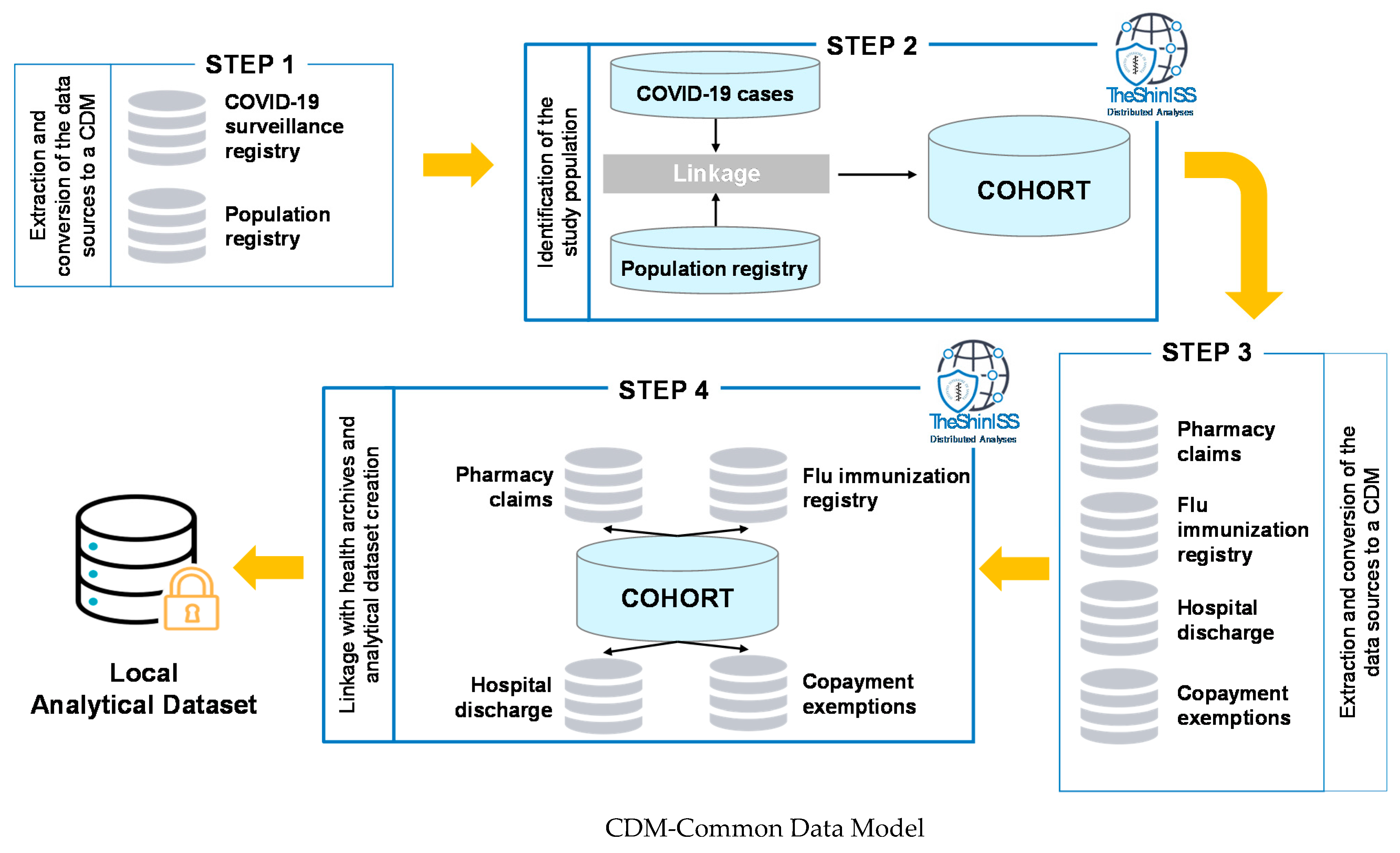
2.1. Setting and Study Design
2.2. Data Sources
2.3. Exposure, Outcomes, and Confounders
2.4. Statistical Analysis
3. Results
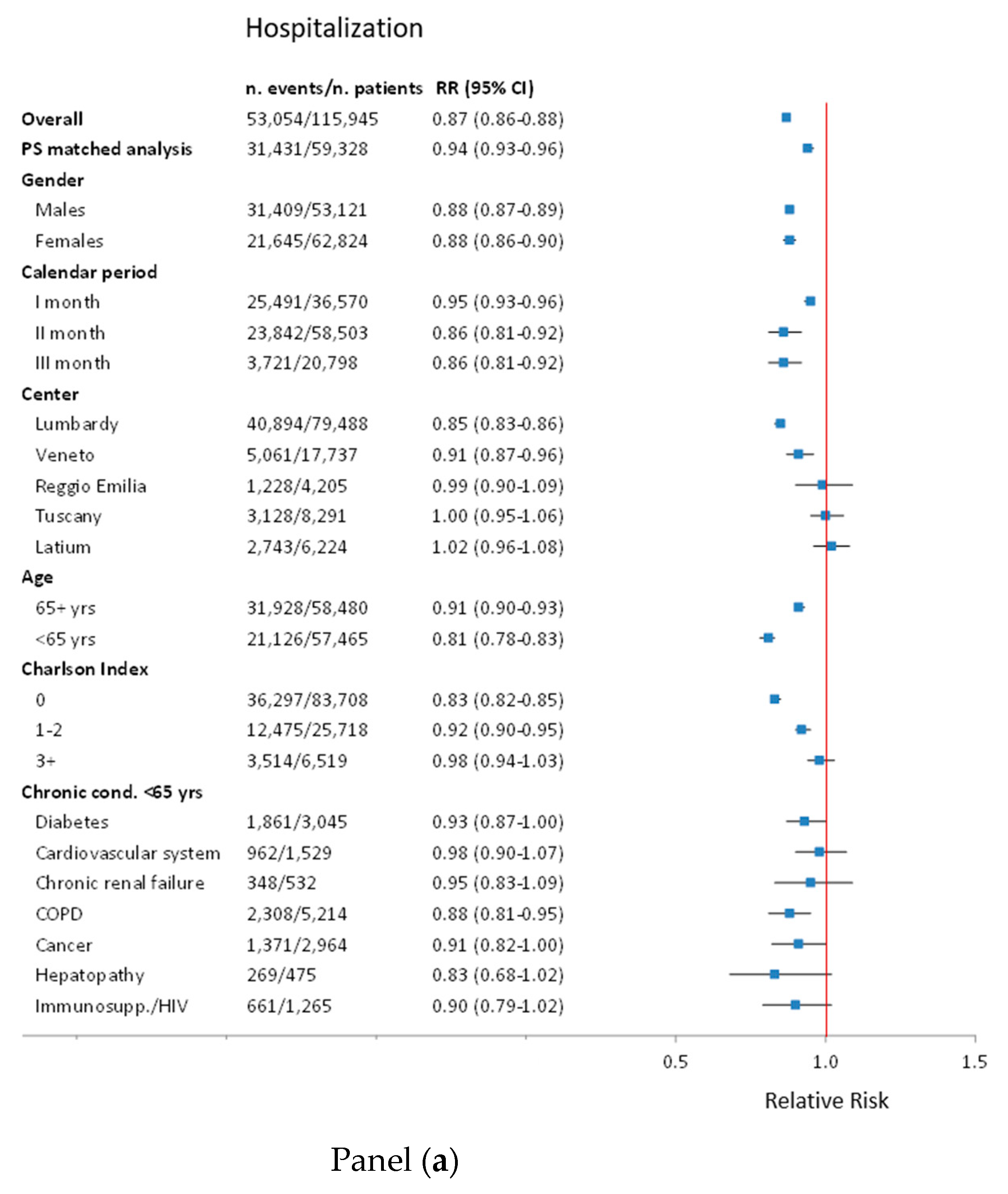
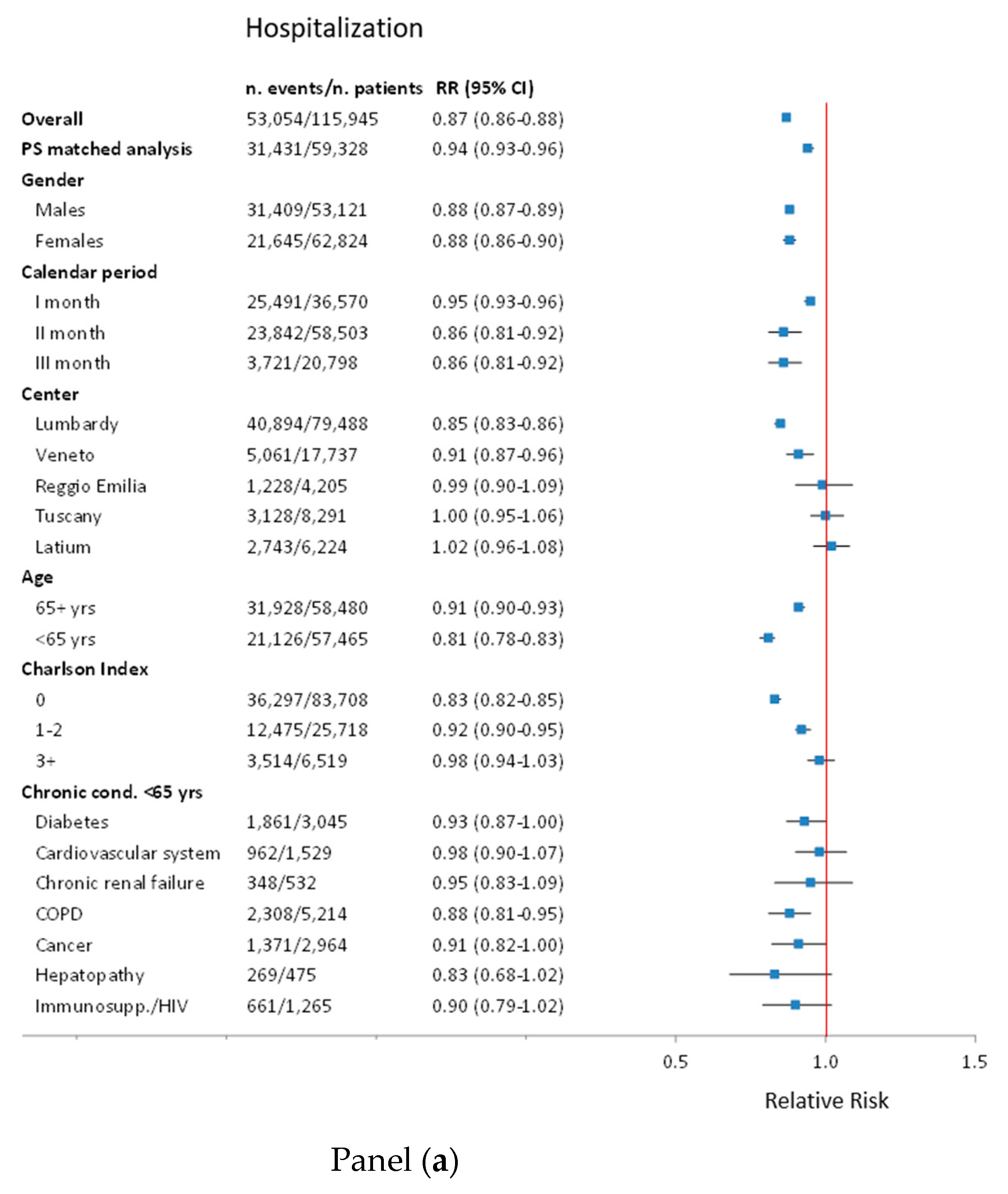
3.1. Risk of Hospitalisation
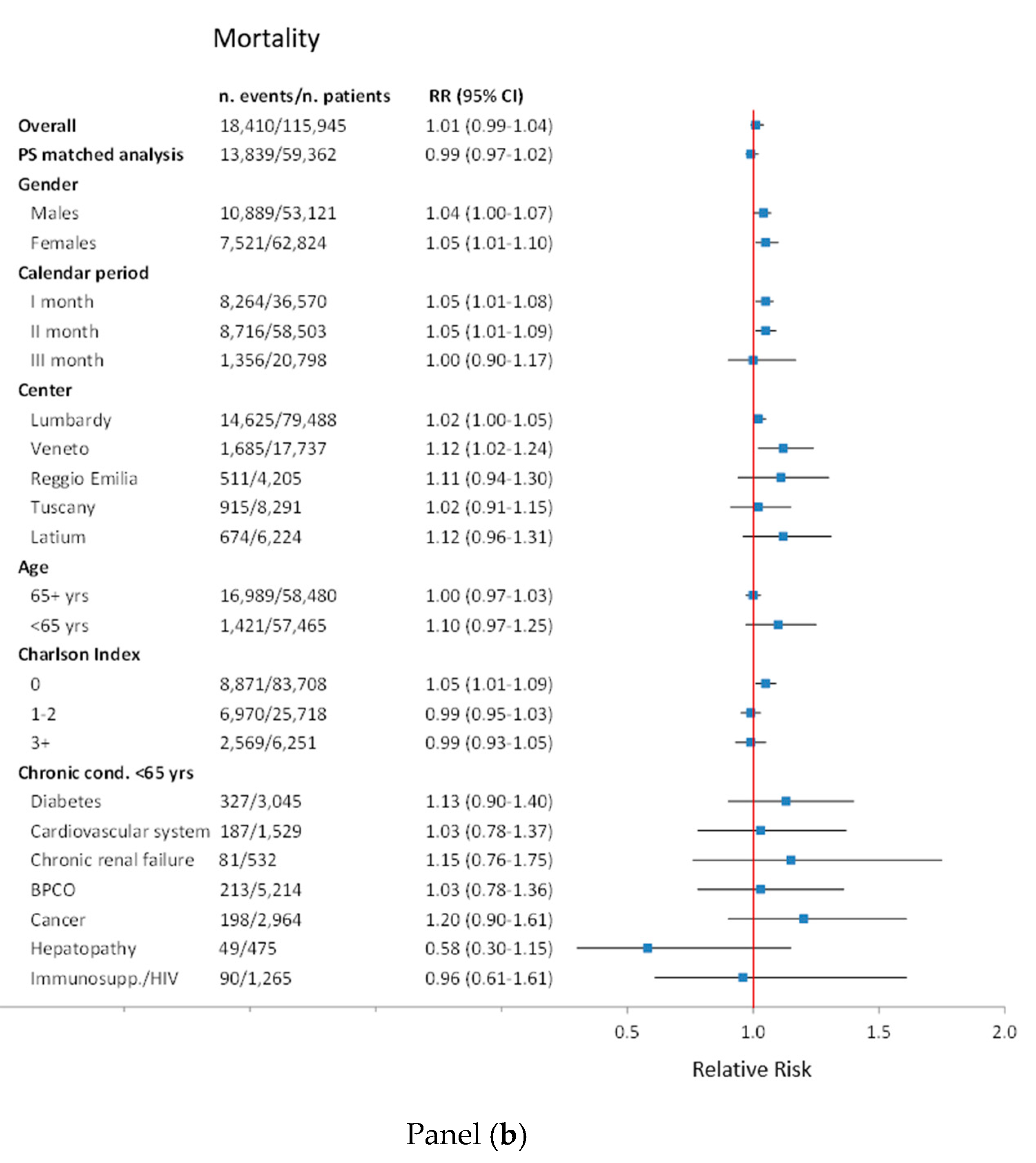
3.2. Risk of Death and ICU Plus Death Composite Outcome
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Naming the Coronavirus Disease (COVID-19) and the Virus That Causes It. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/naming-the-coronavirus-disease-(covid-2019)-and-the-virus-that-causes-it (accessed on 17 June 2021).
- World Health Organization. Archived: WHO Timeline—COVID-19. Available online: https://www.who.int/news/item/27-04-2020-who-timeline---covid-19 (accessed on 17 June 2021).
- European Centre for Disease Prevention and Control. COVID-19. Available online: https://https://www.ecdc.europa.eu/en/covid-19 (accessed on 17 June 2021).
- Chumakov, K.; Benn, C.S.; Aaby, P.; Kottilil, S.; Gallo, R. Can Existing Live Vaccines Prevent COVID-19? Science 2020, 368, 1187–1188. [Google Scholar] [CrossRef] [PubMed]
- Jehi, L.; Ji, X.; Milinovich, A.; Erzurum, S.; Rubin, B.P.; Gordon, S.; Young, J.B.; Kattan, M.W. Individualizing Risk Prediction for Positive Coronavirus Disease 2019 Testing. Chest 2020, 158, 1364–1375. [Google Scholar] [CrossRef] [PubMed]
- Sultana, J.; Mazzaglia, G.; Luxi, N.; Cancellieri, A.; Capuano, A.; Ferrajolo, C.; de Waure, C.; Ferlazzo, G.; Trifirò, G. Potential Effects of Vaccinations on the Prevention of COVID-19: Rationale, Clinical Evidence, Risks, and Public Health Considerations. Expert Rev. Vaccines 2020, 19, 919–936. [Google Scholar] [CrossRef] [PubMed]
- Hui, K.P.Y.; Cheung, M.-C.; Perera, R.A.P.M.; Ng, K.-C.; Bui, C.H.T.; Ho, J.C.W.; Ng, M.M.T.; Kuok, D.I.T.; Shih, K.C.; Tsao, S.-W.; et al. Tropism, Replication Competence, and Innate Immune Responses of the Coronavirus SARS-CoV-2 in Human Respiratory Tract and Conjunctiva: An Analysis in Ex-Vivo and in-Vitro Cultures. Lancet Respir. Med. 2020, 8, 687–695. [Google Scholar] [CrossRef]
- Zanettini, C.; Omar, M.; Dinalankara, W.; Imada, E.L.; Colantuoni, E.; Parmigiani, G.; Marchionni, L. Influenza Vaccination and COVID19 Mortality in the USA. medRxiv 2020. [Google Scholar] [CrossRef]
- Marín-Hernández, D.; Schwartz, R.E.; Nixon, D.F. Epidemiological Evidence for Association between Higher Influenza Vaccine Uptake in the Elderly and Lower COVID-19 Deaths in Italy. J. Med. Virol. 2020, 93, 64–65. [Google Scholar] [CrossRef] [PubMed]
- Amato, M.; Werba, J.P.; Frigerio, B.; Coggi, D.; Sansaro, D.; Ravani, A.; Ferrante, P.; Veglia, F.; Tremoli, E.; Baldassarre, D. Relationship between Influenza Vaccination Coverage Rate and COVID-19 Outbreak: An Italian Ecological Study. Vaccines 2020, 8, 535. [Google Scholar] [CrossRef] [PubMed]
- Arokiaraj, M.C. Considering Interim Interventions to Control COVID-19 Associated Morbidity and Mortality—Perspectives. Front. Public Health 2020, 8, 444. [Google Scholar] [CrossRef]
- Fink, G.; Orlova-Fink, N.; Schindler, T.; Grisi, S.; Ferrer, A.P.; Daubenberger, C.; Brentani, A. Inactivated Trivalent Influenza Vaccine Is Associated with Lower Mortality among Covid-19 Patients in Brazil. MedRxiv 2020. [Google Scholar] [CrossRef]
- Ragni, P.; Marino, M.; Formisano, D.; Bisaccia, E.; Scaltriti, S.; Bedeschi, E.; Grilli, R. Association between Exposure to Influenza Vaccination and COVID-19 Diagnosis and Outcomes. Vaccines 2020, 8, 675. [Google Scholar] [CrossRef] [PubMed]
- Green, I.; Ashkenazi, S.; Merzon, E.; Vinker, S.; Golan-Cohen, A. The Association of Previous Influenza Vaccination and Coronavirus Disease-2019. Hum. Vaccines Immunother. 2020, 17, 1–7. [Google Scholar] [CrossRef]
- Benchimol, E.I.; Smeeth, L.; Guttmann, A.; Harron, K.; Moher, D.; Petersen, I.; Sørensen, H.T.; von Elm, E.; Langan, S.M.; Committee, R.W. The REporting of Studies Conducted Using Observational Routinely-Collected Health Data (RECORD) Statement. PLoS Med. 2015, 12, e1001885. [Google Scholar] [CrossRef] [PubMed]
- Istituto Nazionale di Statistica. Geo DEMO. Demography in Figures. Available online: http://demo.istat.it/index_e.php (accessed on 17 June 2021).
- Istituto Superiore di Sanità. Epidemia COVID-19—Aggiornamento Nazionale 14 Maggio 2020. Available online: https://www.epicentro.iss.it/coronavirus/bollettino/Bollettino-sorveglianza-integrata-COVID-19_14-maggio-2020.pdf (accessed on 17 June 2021).
- Massari, M.; Spila Alegiani, S.; Da Cas, R.; Menniti Ippolito, F. “TheShinISS”: An Open-Source Tool for Conducting Distributed Analyses within Pharmacoepidemiological Multi-Database Studies. Boll. Epidemiol. Naz. 2020, 1, 39–45. [Google Scholar]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A New Method of Classifying Prognostic Comorbidity in Longitudinal Studies: Development and Validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- World Health Organization. COVID-19 Clinical Management: Living Guidance. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-clinical-2021-1 (accessed on 17 June 2021).
- World Health Organization. International Guidelines For Certificationa and Classification (Coding) Of Covid-19 as Cause of Death. Available online: https://cdn.who.int/media/docs/default-source/classification/icd/covid-19/guidelines-cause-of-death-covid-19-20200420-en.pdf?sfvrsn=35fdd864_2 (accessed on 17 June 2021).
- Martínez-Baz, I.; Trobajo-Sanmartín, C.; Arregui, I.; Navascués, A.; Adelantado, M.; Indurain, J.; Fresán, U.; Ezpeleta, C.; Castilla, J. Influenza Vaccination and Risk of SARS-CoV-2 Infection in a Cohort of Health Workers. Vaccines 2020, 8, 611. [Google Scholar] [CrossRef] [PubMed]
- Del Riccio, M.; Lorini, C.; Bonaccorsi, G.; Paget, J.; Caini, S. The Association between Influenza Vaccination and the Risk of SARS-CoV-2 Infection, Severe Illness, and Death: A Systematic Review of the Literature. Int. J. Environ. Res. Public Health 2020, 17, 7870. [Google Scholar] [CrossRef]
- Christenson, B.; Hedlund, J.; Lundbergh, P.; Örtqvist, Å. Additive Preventive Effect of Influenza and Pneumococcal Vaccines in Elderly Persons. Eur. Respir. J. 2004, 23, 363–368. [Google Scholar] [CrossRef] [PubMed]
- Escobar, L.E.; Molina-Cruz, A.; Barillas-Mury, C. BCG Vaccine Protection From Severe Coronavirus Disease 2019 (COVID19). Proc. Natl. Acad. Sci. USA 2020, 117, 17720–17726. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| COVID-19 Cases (%) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Region | Population a ≥18 yrs b | Cumulative Incidence (Range between Provinces) c | ICU d Occupation at the Peak c | Positive Tests c | Vaccination Coverage >64 yrs b | Vaccination Coverage ≤64 yrs b | Hospitalised | ICU d | Case Fatality Rate (30 Days) |
| Lombardy | 8,461,634 | 0.84 (0.38–1.76) | 100.0 | 24.9 | 55.2 | 12.1 | 51.5 | 2.6 | 18.4 |
| Veneto | 4,128,295 | 0.39 (0.19–0.54) | 43.2 | 6.9 | 63.0 | 11.7 | 28.5 | 4.3 | 9.5 |
| Reggio Emilia | 440,869 | 0.92 | 65.0 e | 27.7 | 59.9 | 14.2 | 29.2 | - | 12.2 |
| Tuscany | 3,169,250 | 0.27 (0.16–0.54) | 64.1 | 6.7 | 54.6 | 13.2 | 37.7 | 4.3 | 11.0 |
| Latium | 4,933,338 | 0.13 (0.09–0.25) | 24.0 | 4.5 | 60.1 | 12.4 | 44.1 | 4.0 | 10.8 |
| Age <65 Years | Age 65+ Years | |||||
|---|---|---|---|---|---|---|
| Total Case (N.) | Vaccinated Cases (%) | p | Total Case (N.) | Vaccinated Cases (%) | p | |
| COVID-19 diagnosed cases | 57,465 | 7008 (12.2%) | 58,480 | 33,094 (56.6%) | ||
| Centre | ||||||
| Lombardy | 36,760 | 4428 (12.0%) | 0.003 | 42,728 | 23,604 (55.2%) | <0.001 |
| Veneto | 10,059 | 1180 (11.7%) | 7678 | 4835 (63.0%) | ||
| Tuscany | 4673 | 618 (13.2%) | 3618 | 1980 (54.7%) | ||
| Reggio Emilia | 2268 | 322 (14.2%) | 1937 | 1160 (59.9%) | ||
| Latium | 3705 | 460 (12.4%) | 2519 | 1515 (60.1%) | ||
| Gender | ||||||
| Females | 31,051 | 3845 (12.4%) | 0.14 | 31,773 | 18,683 (58.8%) | <0.001 |
| Males | 26,414 | 3163 (12.0%) | 26,707 | 14,411 (54.0%) | ||
| Age, year | ||||||
| 18–49 | 27,358 | 2566 (9.4%) | <0.001 | |||
| 50–64 | 30,107 | 4442 (14.8%) | ||||
| 65–74 | 16,522 | 7125 (43.1%) | <0.001 | |||
| 75–84 | 21,349 | 12,400 (58.1%) | ||||
| 85+ | 20,609 | 13,569 (65.8%) | ||||
| Charlson index | ||||||
| 0 | 52,225 | 5749 (11.0%) | <0.001 | 31,483 | 16,922 (53.7%) | <0.001 |
| 1–2 | 4786 | 1102 (23.0%) | 20,932 | 12,479 (59.6%) | ||
| ≥3 | 454 | 157 (34.6%) | 6065 | 3693 (60.9%) | ||
| N. of hospitalizations (last 2 years) | ||||||
| 0 | 48,463 | 5512 (11.4%) | <0.001 | 38,185 | 21,505 (56.3%) | 0.022 |
| 1 | 6375 | 946 (14.8%) | 10,671 | 6167 (57.8%) | ||
| ≥2 | 2627 | 550 (20.9%) | 9624 | 5422 (56.3%) | ||
| Comorbidities | ||||||
| Cerebrovascular diseases | 900 | 250 (27.8%) | <0.001 | 9814 | 6016 (61.3%) | <0.001 |
| Artery cardiac disease | 1529 | 377 (24.7%) | <0.001 | 14,271 | 8731 (61.2%) | <0.001 |
| Hypertension | 12,841 | 2173 (16.9%) | <0.001 | 38,248 | 21,664 (56.6%) | 0.73 |
| Hepatopathy | 475 | 110 (23.2%) | <0.001 | 1065 | 602 (56.5%) | 0.97 |
| Chronic kidney failure | 532 | 152 (28.6%) | <0.001 | 3436 | 1972 (57.4%) | 0.33 |
| Diabetes mellitus | 3045 | 699 (23.0%) | <0.001 | 12,078 | 7041 (58.3%) | <0.001 |
| Chronic pulmonary disease | 906 | 294 (32.5%) | <0.001 | 5908 | 3614 (61.2%) | <0.001 |
| Neoplasms | 2964 | 541 (18.3%) | <0.001 | 9081 | 5202 (57.3%) | 0.15 |
| Dementia | 88 | 44 (50.0%) | <0.001 | 5117 | 3287 (64.2%) | <0.001 |
| Rheumatic diseases | 416 | 93 (22.4%) | <0.001 | 1029 | 604 (58.7%) | 0.17 |
| Prior drug use a | ||||||
| Antiacid drugs | 9080 | 1551 (17.1%) | <0.001 | 23,474 | 13,385 (57.0%) | 0.086 |
| Lipid modifying agents | 4791 | 1003 (20.9%) | <0.001 | 16,963 | 9633 (56.8%) | 0.54 |
| Anticoagulants | 2962 | 484 (16.3%) | <0.001 | 11,402 | 6471 (56.8%) | 0.70 |
| Platelet aggregation inhibitors | 2306 | 593 (25.7%) | <0.001 | 15,112 | 8824 (58.4%) | <0.001 |
| Antiarrhythmics, class I and III | 434 | 87 (20.0%) | <0.001 | 2927 | 1682 (57.5%) | 0.33 |
| Antibiotics | 18,583 | 2485 (13.4%) | <0.001 | 21,226 | 11,927 (56.2%) | 0.14 |
| Anti HIV b drugs | 316 | 74 (23.4%) | <0.001 | 264 | 128 (48.5%) | 0.008 |
| Anti-Parkinsonian drugs | 116 | 40 (34.5%) | <0.001 | 1778 | 1099 (61.8%) | <0.001 |
| Antiepileptics | 2119 | 585 (27.6%) | <0.001 | 4857 | 2752 (56.7%) | 0.92 |
| Antipsychotics | 1175 | 401 (34.1%) | <0.001 | 4621 | 2718 (58.8%) | 0.001 |
| Antidepressants | 3794 | 667 (17.6%) | <0.001 | 9822 | 5840 (59.5%) | <0.001 |
| Corticosteroids for systemic use | 5347 | 845 (15.8%) | <0.001 | 7194 | 4024 (55.9%) | 0.23 |
| DMARDs c | 987 | 212 (21.5%) | <0.001 | 1183 | 602 (50.9%) | <0.001 |
| Recent drug use d | ||||||
| NSAIDs e | 2234 | 329 (14.7%) | <0.001 | 3582 | 2006 (56.0%) | 0.46 |
| n. of Events/n. of Subjects | RR a unadj (95% CI b) | RR adj (95% CI) | ||
|---|---|---|---|---|
| Vaccinated | Not Vaccinated | |||
| Type of event | ||||
| Hospitalisation | 19,104/40,102 | 33,950/75,843 | 1.06 (1.05–1.08) | 0.87 (0.86–0.88) |
| Deaths COVID19 | 10,212/40,102 | 8198/75,843 | 2.36 (2.29–2.42) | 1.04 (1.01–1.06) |
| ICU c/Deaths COVID19 d | 10,366/38,620 | 9238/73,120 | 2.12 (2.07–2.18) | 1.01 (0.99–1.04) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Massari, M.; Spila-Alegiani, S.; Fabiani, M.; Belleudi, V.; Trifirò, G.; Kirchmayer, U.; Poggi, F.R.; Mancuso, P.; Menniti-Ippolito, F.; Gini, R.; et al. Association of Influenza Vaccination and Prognosis in Patients Testing Positive to SARS-CoV-2 Swab Test: A Large-Scale Italian Multi-Database Cohort Study. Vaccines 2021, 9, 716. https://doi.org/10.3390/vaccines9070716
Massari M, Spila-Alegiani S, Fabiani M, Belleudi V, Trifirò G, Kirchmayer U, Poggi FR, Mancuso P, Menniti-Ippolito F, Gini R, et al. Association of Influenza Vaccination and Prognosis in Patients Testing Positive to SARS-CoV-2 Swab Test: A Large-Scale Italian Multi-Database Cohort Study. Vaccines. 2021; 9(7):716. https://doi.org/10.3390/vaccines9070716
Chicago/Turabian StyleMassari, Marco, Stefania Spila-Alegiani, Massimo Fabiani, Valeria Belleudi, Gianluca Trifirò, Ursula Kirchmayer, Francesca Romana Poggi, Pamela Mancuso, Francesca Menniti-Ippolito, Rosa Gini, and et al. 2021. "Association of Influenza Vaccination and Prognosis in Patients Testing Positive to SARS-CoV-2 Swab Test: A Large-Scale Italian Multi-Database Cohort Study" Vaccines 9, no. 7: 716. https://doi.org/10.3390/vaccines9070716
APA StyleMassari, M., Spila-Alegiani, S., Fabiani, M., Belleudi, V., Trifirò, G., Kirchmayer, U., Poggi, F. R., Mancuso, P., Menniti-Ippolito, F., Gini, R., Bartolini, C., Leoni, O., Ercolanoni, M., Da-Re, F., Guzzinati, S., Luxi, N., Riccardo, F., & Giorgi-Rossi, P. (2021). Association of Influenza Vaccination and Prognosis in Patients Testing Positive to SARS-CoV-2 Swab Test: A Large-Scale Italian Multi-Database Cohort Study. Vaccines, 9(7), 716. https://doi.org/10.3390/vaccines9070716