
Psychological Determinants of COVID-19 Vaccine Acceptance among Healthcare Workers in Kuwait: A Cross-Sectional Study Using the 5C and Vaccine Conspiracy Beliefs Scales



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Overview of the Questionnaire Items
2.3. Major Measures in the Study
2.3.1. Willingness to Accept COVID-19 Vaccination
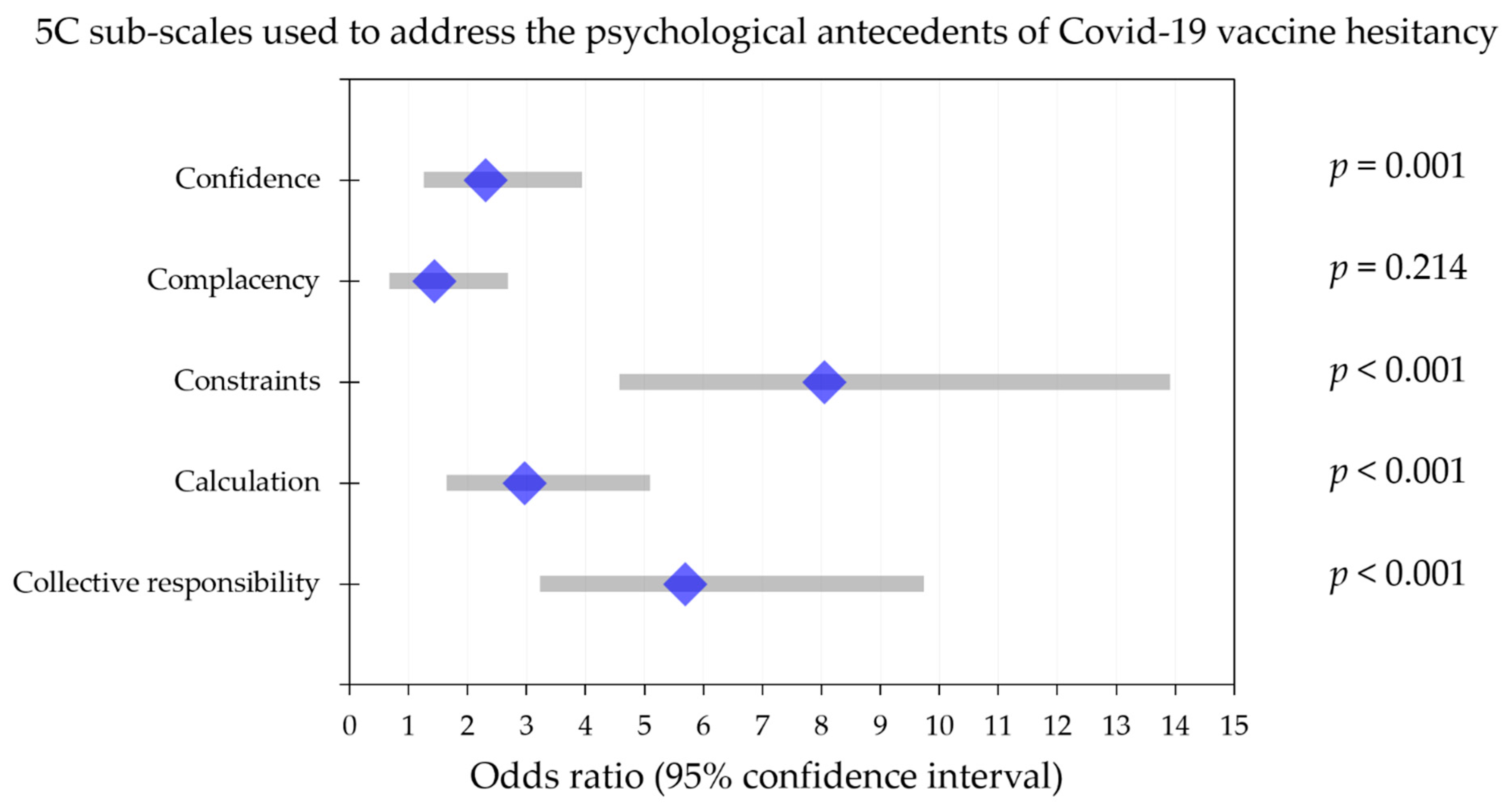
2.3.2. The Role of Psychological Antecedents and Conspiracy Beliefs in COVID-19 Vaccine Rejection/Hesitancy
2.3.3. Dichotomous Classification of the 5C Subscales for Multinomial Regression Analysis
2.3.4. COVID-19 Vaccine Hesitancy in Relation to VCBS
2.4. Ethical Permission
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Study Participants
3.2. An Overall High Rate for Acceptance of COVID-19 Vaccination among HCWs in Kuwait
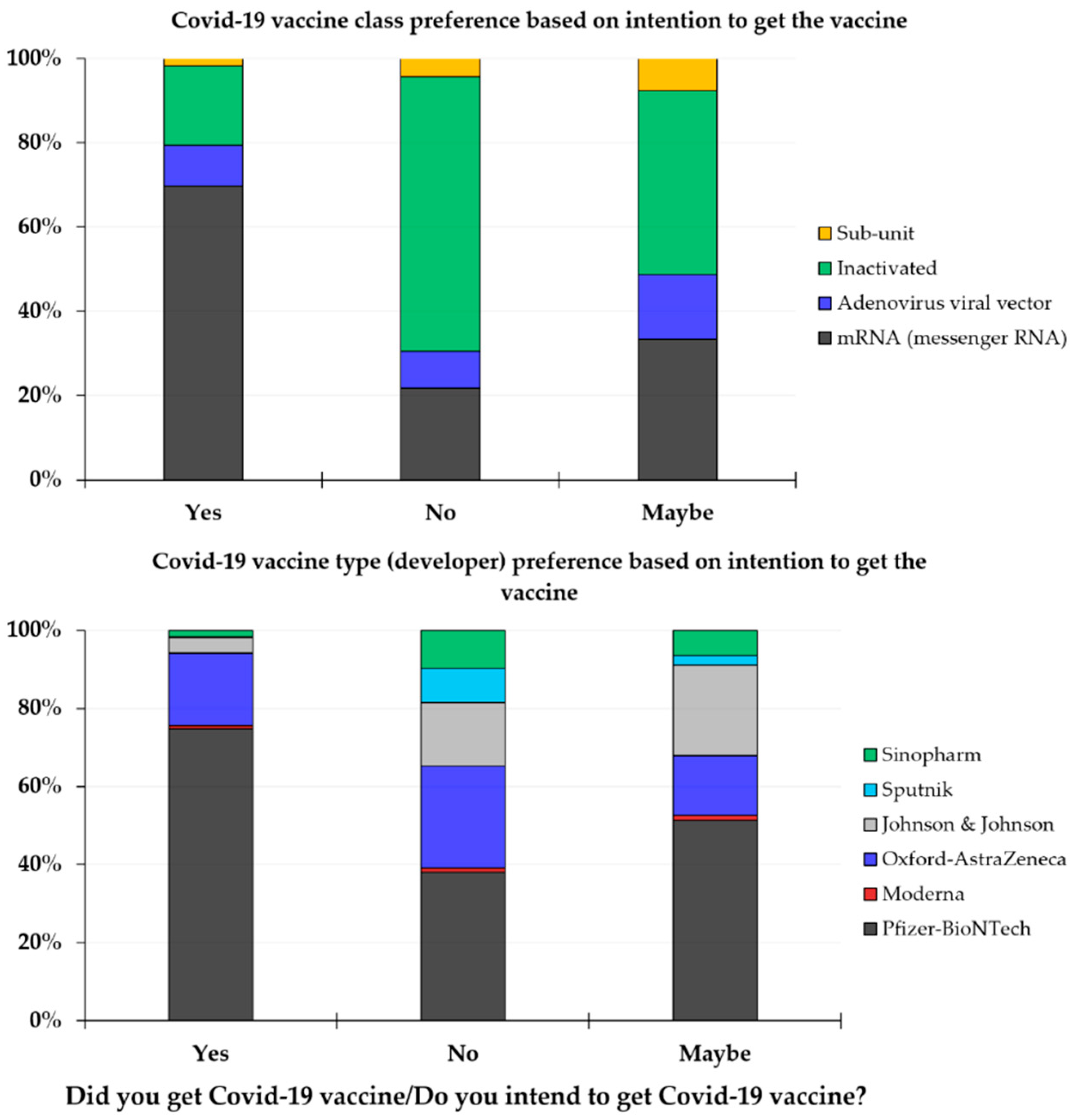
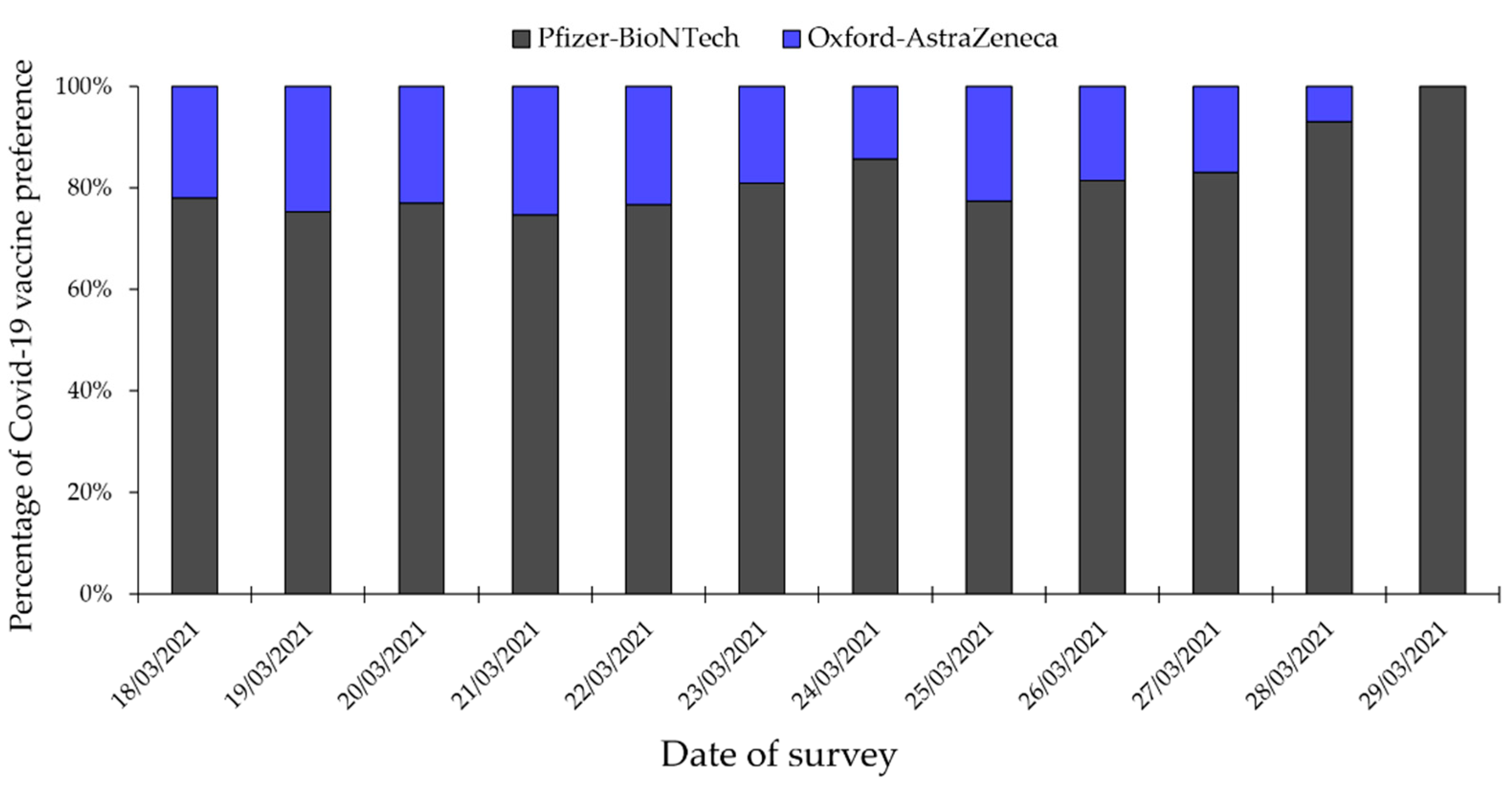
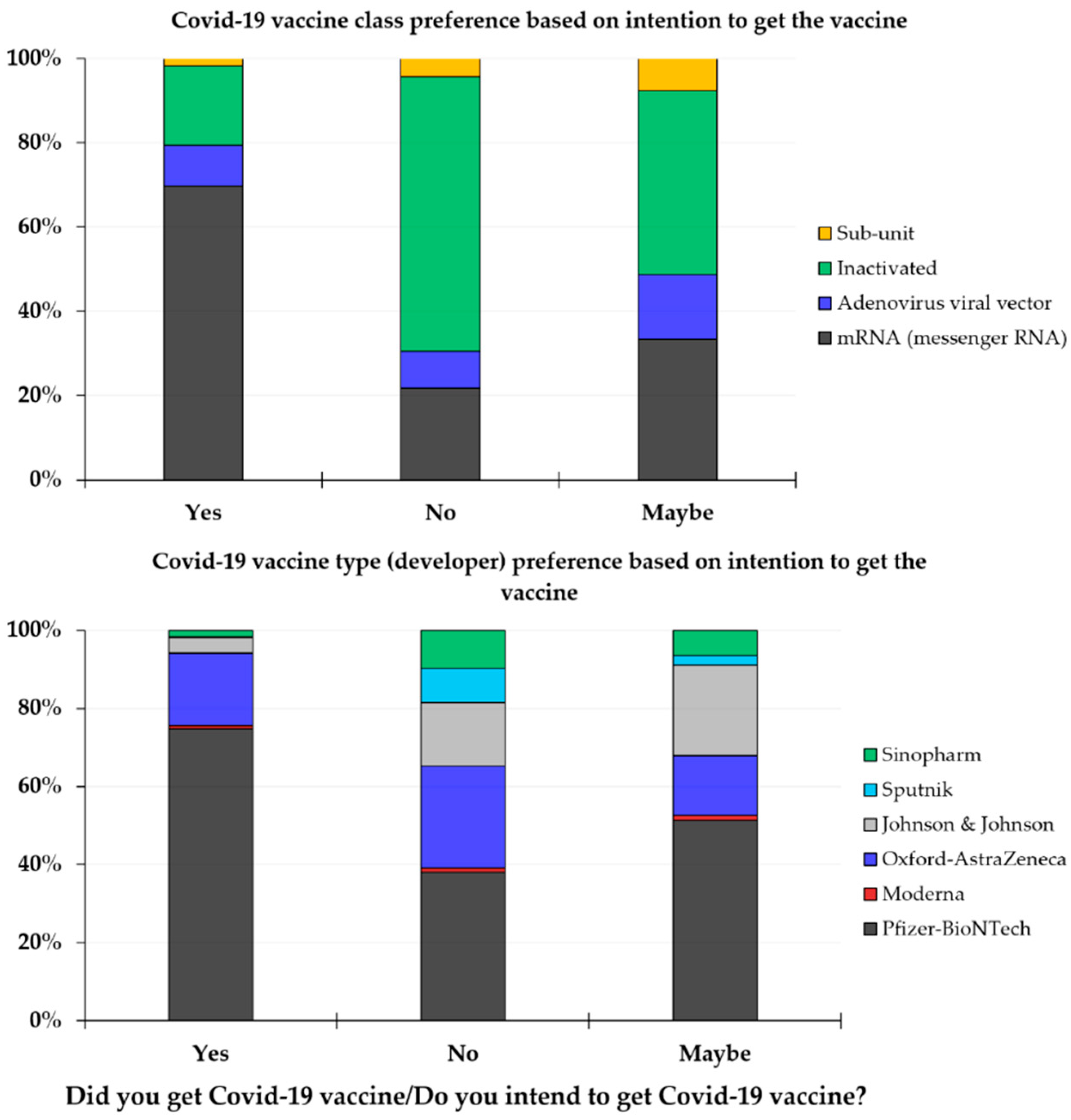
3.3. A Majority of HCWs in Kuwait Preferred Messenger RNA-Based and Pfizer-BioNTech Vaccines
3.4. The Conspiratorial Belief Regarding SARS-CoV-2 Origin and Anti-Vaccination Altogether Were Associated with COVID-19 Vaccine Hesitancy
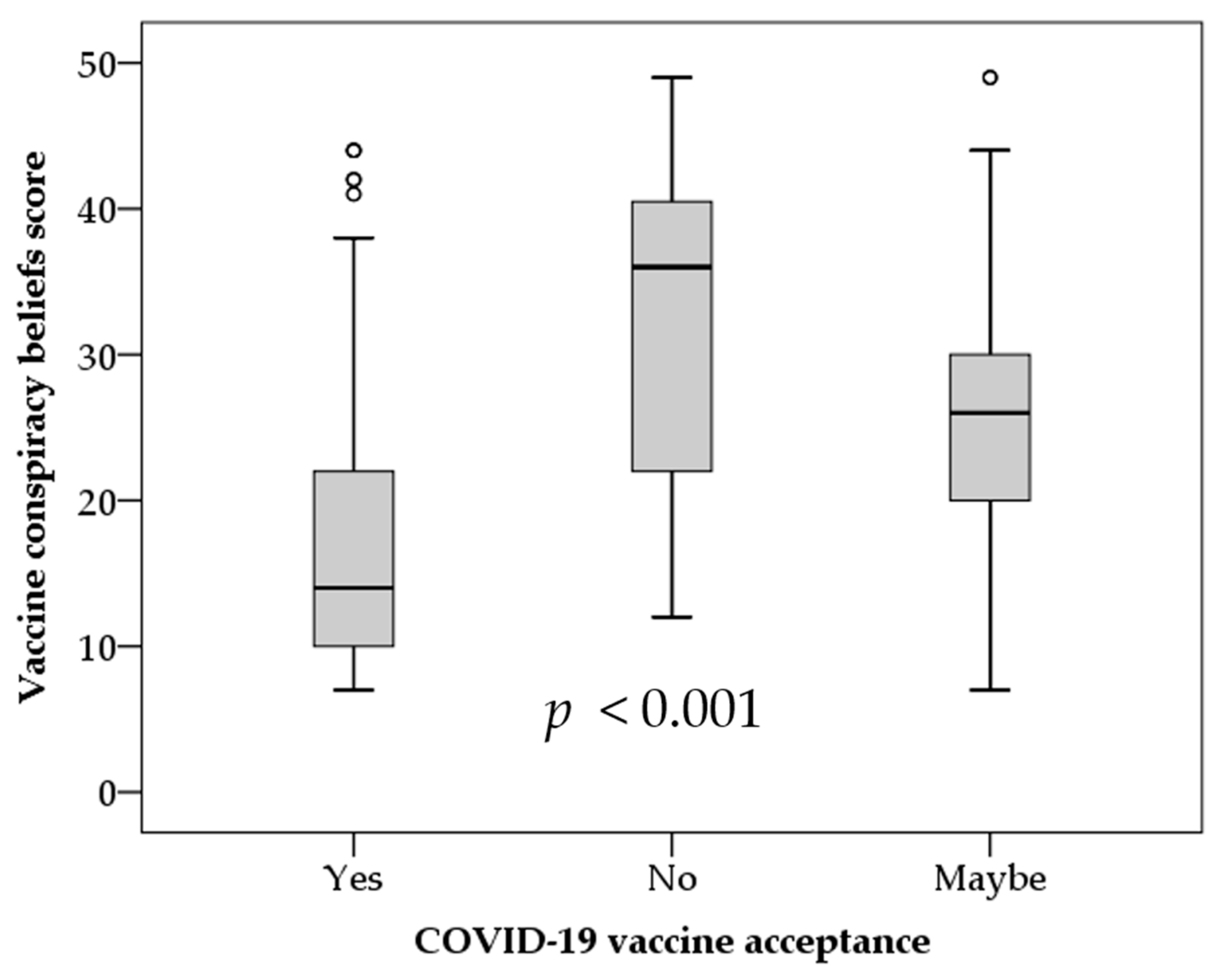
3.5. COVID-19 Vaccine Conspiracy Beliefs Were Associated with a Significantly Lower Intent to Receive COVID-19 Vaccination among HCWs in Kuwait
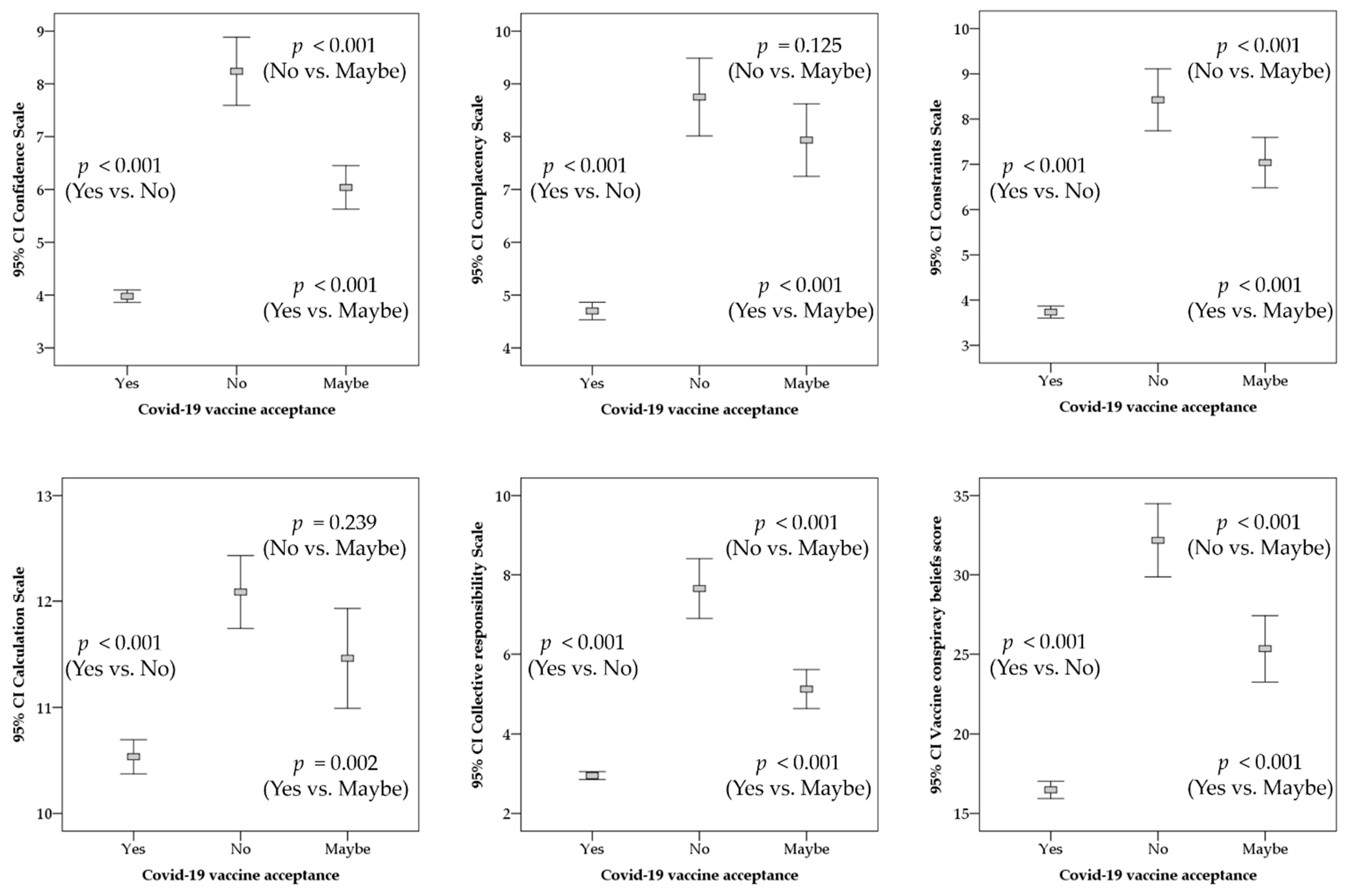
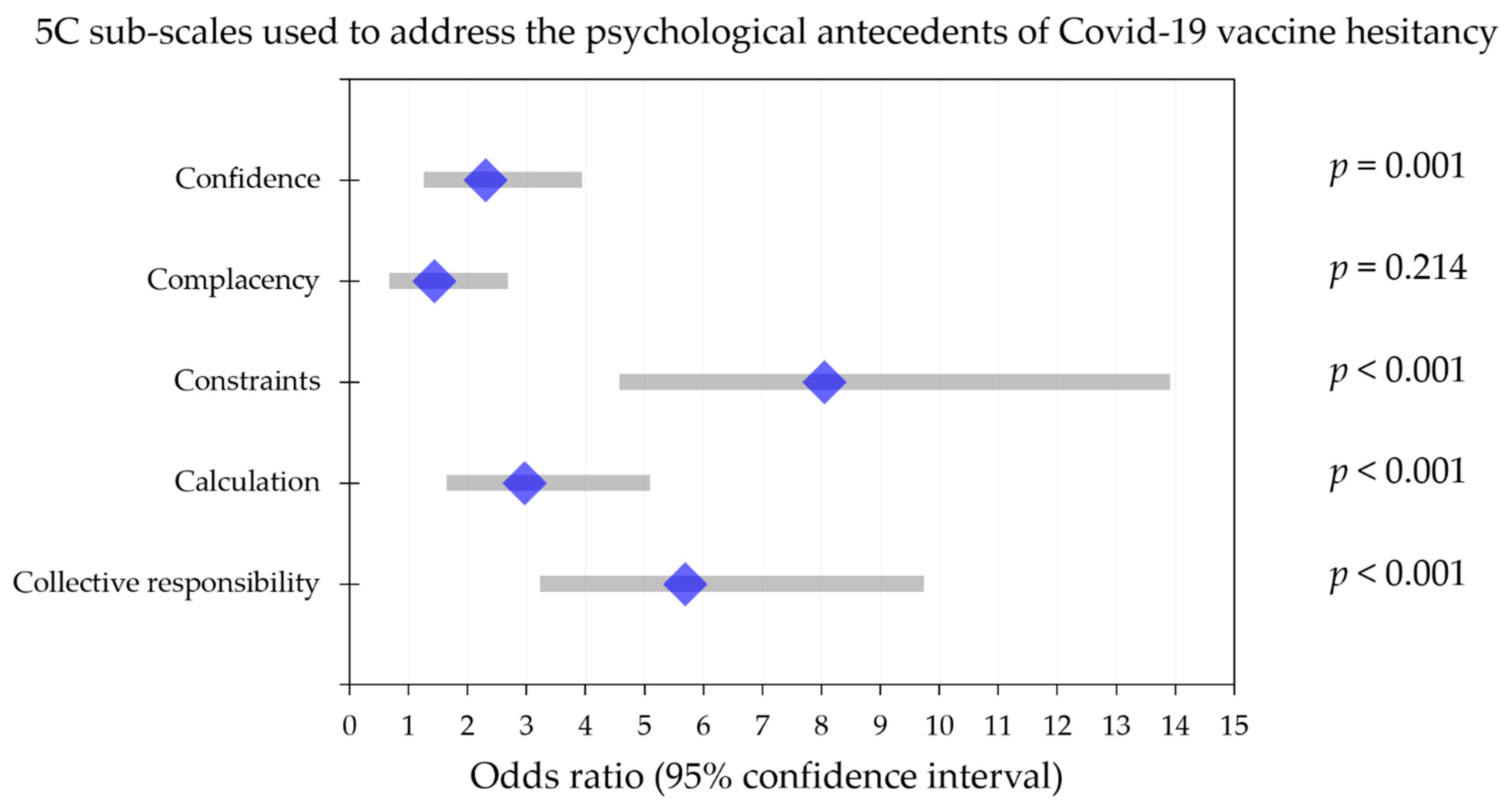
3.6. The 5C Psychological Determinants for COVID-19 Vaccination
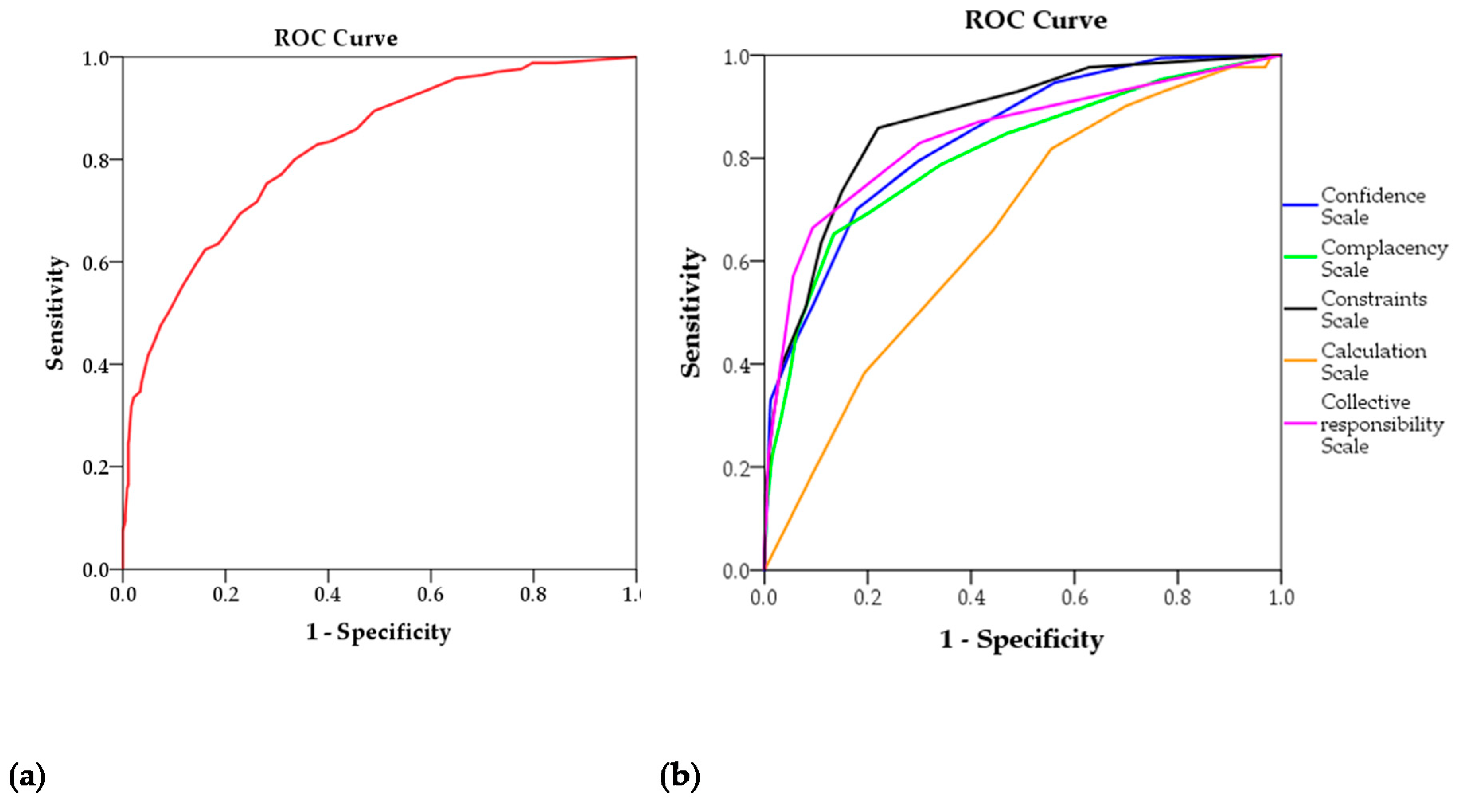
3.7. ROC Analysis of the 5C Subscales and the VCBS Scale
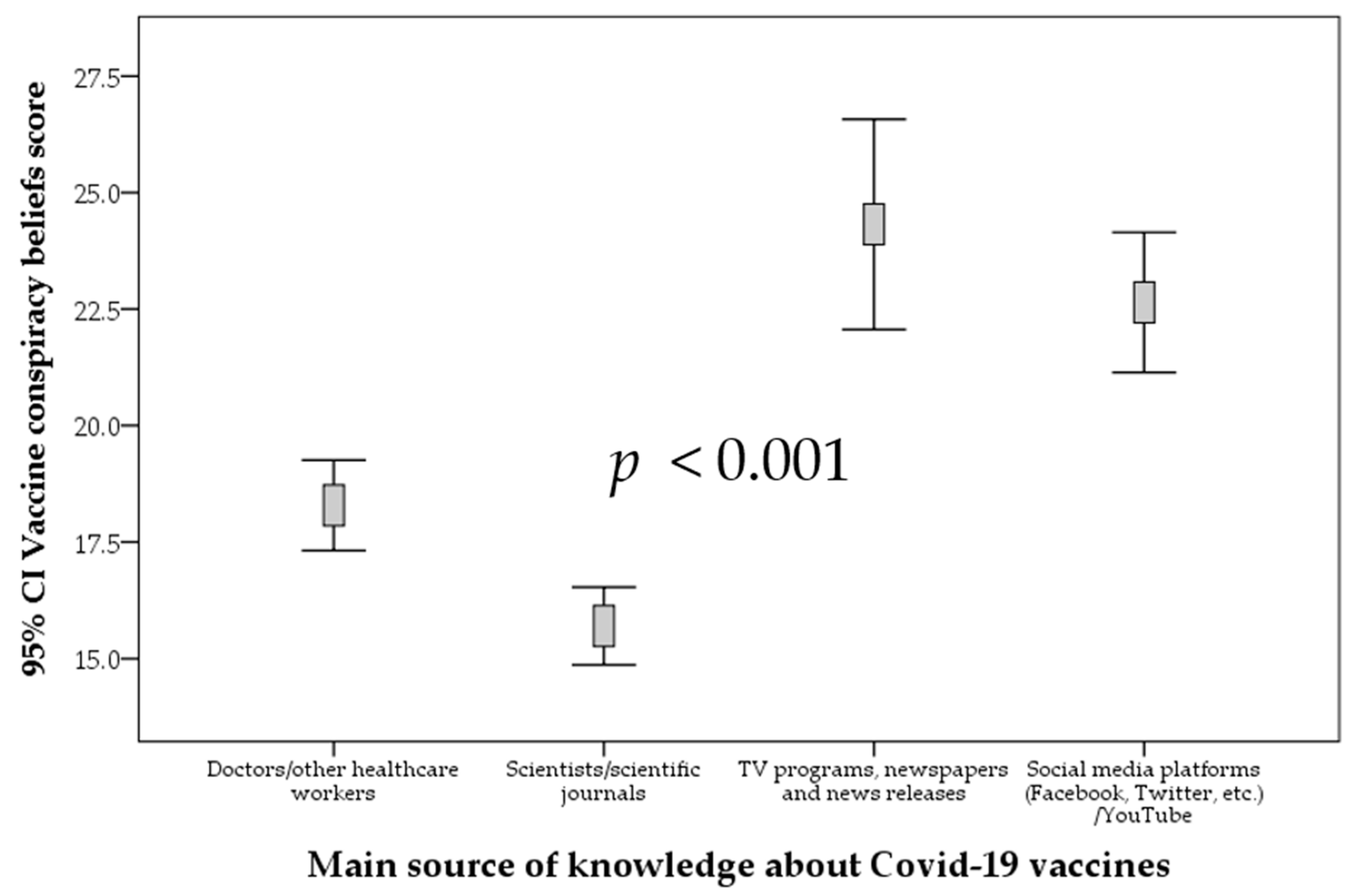
3.8. Sources of Knowledge about COVID-19 Vaccines and Its Relation to Vaccine Acceptance
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The World Health Organization (WHO). Ten Threats to Global Health in 2019. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 12 April 2021).
- Wiysonge, C.S.; Ndwandwe, D.; Ryan, J.; Jaca, A.; Batoure, O.; Anya, B.M.; Cooper, S. Vaccine hesitancy in the era of COVID-19: Could lessons from the past help in divining the future? Hum. Vaccines Immunother. 2021, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Dror, A.A.; Eisenbach, N.; Taiber, S.; Morozov, N.G.; Mizrachi, M.; Zigron, A.; Srouji, S.; Sela, E. Vaccine hesitancy: The next challenge in the fight against COVID-19. Eur. J. Epidemiol. 2020, 35, 775–779. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.; Tu, P.; Beitsch, L.M. Confidence and Receptivity for COVID-19 Vaccines: A Rapid Systematic Review. Vaccines 2020, 9. [Google Scholar] [CrossRef] [PubMed]
- Wouters, O.J.; Shadlen, K.C.; Salcher-Konrad, M.; Pollard, A.J.; Larson, H.J.; Teerawattananon, Y.; Jit, M. Challenges in ensuring global access to COVID-19 vaccines: Production, affordability, allocation, and deployment. Lancet 2021, 397, 1023–1034. [Google Scholar] [CrossRef]
- Dagan, N.; Barda, N.; Kepten, E.; Miron, O.; Perchik, S.; Katz, M.A.; Hernan, M.A.; Lipsitch, M.; Reis, B.; Balicer, R.D. BNT162b2 mRNA Covid-19 Vaccine in a Nationwide Mass Vaccination Setting. N. Engl. J. Med. 2021, 384, 1412–1423. [Google Scholar] [CrossRef]
- Baraniuk, C. Covid-19: How the UK vaccine rollout delivered success, so far. BMJ 2021, 372, n421. [Google Scholar] [CrossRef]
- Omer, S.B.; Salmon, D.A.; Orenstein, W.A.; deHart, M.P.; Halsey, N. Vaccine refusal, mandatory immunization, and the risks of vaccine-preventable diseases. N. Engl. J. Med. 2009, 360, 1981–1988. [Google Scholar] [CrossRef]
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int. J. Surg. 2020, 78, 185–193. [Google Scholar] [CrossRef]
- Mukaetova-Ladinska, E.B.; Kronenberg, G. Psychological and neuropsychiatric implications of COVID-19. Eur. Arch. Psychiatry Clin. Neurosci. 2021, 271, 235–248. [Google Scholar] [CrossRef]
- Carvalho, T.; Krammer, F.; Iwasaki, A. The first 12 months of COVID-19: A timeline of immunological insights. Nat. Rev. Immunol. 2021, 21, 245–256. [Google Scholar] [CrossRef]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Rawat, K.; Kumari, P.; Saha, L. COVID-19 vaccine: A recent update in pipeline vaccines, their design and development strategies. Eur. J. Pharmacol. 2021, 892, 173751. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Perez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Xia, S.; Zhang, Y.; Wang, Y.; Wang, H.; Yang, Y.; Gao, G.F.; Tan, W.; Wu, G.; Xu, M.; Lou, Z.; et al. Safety and immunogenicity of an inactivated SARS-CoV-2 vaccine, BBIBP-CorV: A randomised, double-blind, placebo-controlled, phase 1/2 trial. Lancet Infect. Dis. 2021, 21, 39–51. [Google Scholar] [CrossRef]
- Ledford, H. J&J’s One-Shot COVID Vaccine Offers Hope for Faster Protection. Available online: https://www.nature.com/articles/d41586-021-00119-7 (accessed on 6 May 2021).
- Baraniuk, C. Covid-19: What do we know about Sputnik V and other Russian vaccines? BMJ 2021, 372, n743. [Google Scholar] [CrossRef]
- MacDonald, N.E.; SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Dube, E.; Laberge, C.; Guay, M.; Bramadat, P.; Roy, R.; Bettinger, J. Vaccine hesitancy: An overview. Hum. Vaccines Immunother. 2013, 9, 1763–1773. [Google Scholar] [CrossRef]
- Peretti-Watel, P.; Larson, H.J.; Ward, J.K.; Schulz, W.S.; Verger, P. Vaccine hesitancy: Clarifying a theoretical framework for an ambiguous notion. PLoS Curr. 2015, 7. [Google Scholar] [CrossRef]
- Murphy, J.; Vallieres, F.; Bentall, R.P.; Shevlin, M.; McBride, O.; Hartman, T.K.; McKay, R.; Bennett, K.; Mason, L.; Gibson-Miller, J.; et al. Psychological characteristics associated with COVID-19 vaccine hesitancy and resistance in Ireland and the United Kingdom. Nat. Commun. 2021, 12, 29. [Google Scholar] [CrossRef]
- Salali, G.D.; Uysal, M.S. COVID-19 vaccine hesitancy is associated with beliefs on the origin of the novel coronavirus in the UK and Turkey. Psychol. Med. 2020, 1–3. [Google Scholar] [CrossRef]
- Jolley, D.; Douglas, K.M. The effects of anti-vaccine conspiracy theories on vaccination intentions. PLoS ONE 2014, 9, e89177. [Google Scholar] [CrossRef]
- Barello, S.; Palamenghi, L.; Graffigna, G. Looking inside the ‘black box’ of vaccine hesitancy: Unlocking the effect of psychological attitudes and beliefs on COVID-19 vaccine acceptance and implications for public health communication. Psychol. Med. 2021, 1–2. [Google Scholar] [CrossRef]
- Ball, P.; Maxmen, A. The epic battle against coronavirus misinformation and conspiracy theories. Nature 2020, 581, 371–374. [Google Scholar] [CrossRef]
- Sallam, M.; Dababseh, D.; Yaseen, A.; Al-Haidar, A.; Taim, D.; Eid, H.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. COVID-19 misinformation: Mere harmless delusions or much more? A knowledge and attitude cross-sectional study among the general public residing in Jordan. PLoS ONE 2020, 15, e0243264. [Google Scholar] [CrossRef]
- Sallam, M.; Dababseh, D.; Eid, H.; Al-Mahzoum, K.; Al-Haidar, A.; Taim, D.; Yaseen, A.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. High Rates of COVID-19 Vaccine Hesitancy and Its Association with Conspiracy Beliefs: A Study in Jordan and Kuwait among Other Arab Countries. Vaccines (Basel) 2021, 9. [Google Scholar] [CrossRef]
- Hornsey, M.J.; Harris, E.A.; Fielding, K.S. The psychological roots of anti-vaccination attitudes: A 24-nation investigation. Health Psychol. 2018, 37, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Yaqub, O.; Castle-Clarke, S.; Sevdalis, N.; Chataway, J. Attitudes to vaccination: A critical review. Soc. Sci. Med. 2014, 112, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Betsch, C.; Böhm, R.; Chapman, G.B. Using behavioral insights to increase vaccination policy effectiveness. Policy Insights Behav. Brain Sci. 2015, 2, 61–73. [Google Scholar] [CrossRef]
- Betsch, C.; Bach Habersaat, K.; Deshevoi, S.; Heinemeier, D.; Briko, N.; Kostenko, N.; Kocik, J.; Bohm, R.; Zettler, I.; Wiysonge, C.S.; et al. Sample study protocol for adapting and translating the 5C scale to assess the psychological antecedents of vaccination. BMJ Open 2020, 10, e034869. [Google Scholar] [CrossRef] [Green Version]
- Shapiro, G.K.; Holding, A.; Perez, S.; Amsel, R.; Rosberger, Z. Validation of the vaccine conspiracy beliefs scale. Papillomavirus Res. 2016, 2, 167–172. [Google Scholar] [CrossRef] [Green Version]
- Betsch, C.; Schmid, P.; Heinemeier, D.; Korn, L.; Holtmann, C.; Bohm, R. Beyond confidence: Development of a measure assessing the 5C psychological antecedents of vaccination. PLoS ONE 2018, 13, e0208601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freeman, D.; Waite, F.; Rosebrock, L.; Petit, A.; Causier, C.; East, A.; Jenner, L.; Teale, A.-L.; Carr, L.; Mulhall, S. Coronavirus conspiracy beliefs, mistrust, and compliance with government guidelines in England. Psychol. Med. 2020, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Mohanty, A.; Kabi, A.; Mohanty, A.P. Health problems in healthcare workers: A review. J. Fam. Med. Prim. Care 2019, 8, 2568–2572. [Google Scholar] [CrossRef]
- Wheeler, M.; Buttenheim, A.M. Parental vaccine concerns, information source, and choice of alternative immunization schedules. Hum. Vaccines Immunother. 2013, 9, 1782–1789. [Google Scholar] [CrossRef] [Green Version]
- Sallam, M. COVID-19 Vaccine Hesitancy Worldwide: A Concise Systematic Review of Vaccine Acceptance Rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef] [PubMed]
- Statista. Estimated Population in Kuwait from 2012 to 2019, by Citizenship Status. Available online: https://www.statista.com/statistics/645790/kuwait-population-by-citizenship-status/#:~:text=Population%20in%20Kuwait%20by%20citizenship%202012%2D2019&text=Non%2DKuwaiti%20residents%20accounted%20for,was%20at%20about%20three%20million (accessed on 30 April 2021).
- Our World in Data. Kuwait: Coronavirus Pandemic Country Profile. Available online: https://ourworldindata.org/coronavirus/country/kuwait (accessed on 30 April 2021).
- COVID19 Vaccine Tracker. Kuwait: 2 Vaccines Approved for Use in Kuwait. Available online: https://covid19.trackvaccines.org/country/kuwait/ (accessed on 6 May 2021).
- Salman, A.; Fakhraldeen, S.A.; Chun, S.; Jamil, K.; Gasana, J.; Al-Hunayan, A. Enhancing Research and Development in the Health Sciences as a Strategy to Establish a Knowledge-Based Economy in the State of Kuwait: A Call for Action. Healthcare 2020, 8, 264. [Google Scholar] [CrossRef] [PubMed]
- Checkmarket. Sample Size Calculator. Available online: https://www.checkmarket.com/ (accessed on 10 January 2021).
- Sallam, M.; Dababseh, D.; Eid, H.; Hasan, H.; Taim, D.; Al-Mahzoum, K.; Al-Haidar, A.; Yaseen, A.; Ababneh, N.A.; Assaf, A.; et al. Low COVID-19 Vaccine Acceptance Is Correlated with Conspiracy Beliefs among University Students in Jordan. Int. J. Environ. Res. Public Health 2021, 18. [Google Scholar] [CrossRef]
- Nguyen, L.H.; Drew, D.A.; Graham, M.S.; Joshi, A.D.; Guo, C.-G.; Ma, W.; Mehta, R.S.; Warner, E.T.; Sikavi, D.R.; Lo, C.-H. Risk of COVID-19 among front-line health-care workers and the general community: A prospective cohort study. Lancet Public Health 2020, 5, e475–e483. [Google Scholar] [CrossRef]
- AlAwadhi, E.; Zein, D.; Mallallah, F.; Bin Haider, N.; Hossain, A. Monitoring COVID-19 Vaccine Acceptance in Kuwait During the Pandemic: Results from a National Serial Study. Risk Manag. Healthc Policy 2021, 14, 1413–1429. [Google Scholar] [CrossRef]
- Alqudeimat, Y.; Alenezi, D.; AlHajri, B.; Alfouzan, H.; Almokhaizeem, Z.; Altamimi, S.; Almansouri, W.; Alzalzalah, S.; Ziyab, A.H. Acceptance of a COVID-19 Vaccine and Its Related Determinants among the General Adult Population in Kuwait. Med. Princ. Pract. 2021. [Google Scholar] [CrossRef]
- Fares, S.; Elmnyer, M.M.; Mohamed, S.S.; Elsayed, R. COVID-19 Vaccination Perception and Attitude among Healthcare Workers in Egypt. J. Prim. Care Community Health 2021, 12. [Google Scholar] [CrossRef]
- Wang, K.; Wong, E.L.Y.; Ho, K.F.; Cheung, A.W.L.; Chan, E.Y.Y.; Yeoh, E.K.; Wong, S.Y.S. Intention of nurses to accept coronavirus disease 2019 vaccination and change of intention to accept seasonal influenza vaccination during the coronavirus disease 2019 pandemic: A cross-sectional survey. Vaccine 2020, 38, 7049–7056. [Google Scholar] [CrossRef]
- Biswas, N.; Mustapha, T.; Khubchandani, J.; Price, J.H. The Nature and Extent of COVID-19 Vaccination Hesitancy in Healthcare Workers. J. Community Health 2021, 1–8. [Google Scholar] [CrossRef]
- Kwok, K.O.; Li, K.-K.; Wei, W.I.; Tang, A.; Wong, S.Y.S.; Lee, S.S. Influenza vaccine uptake, COVID-19 vaccination intention and vaccine hesitancy among nurses: A survey. Int. J. Nurs. Stud. 2021, 114, 103854. [Google Scholar] [CrossRef]
- Iacobucci, G. Covid-19: Single Dose of Pfizer and Oxford Vaccines Cuts Risk of Hospital Admission by 80% in over 80s, Data Suggest. BMJ 2021, 372, n612. [Google Scholar] [CrossRef]
- Szmyd, B.; Karuga, F.F.; Bartoszek, A.; Staniecka, K.; Siwecka, N.; Bartoszek, A.; Błaszczyk, M.; Radek, M. Attitude and Behaviors towards SARS-CoV-2 Vaccination among Healthcare Workers: A Cross-Sectional Study from Poland. Vaccines 2021, 9, 218. [Google Scholar] [CrossRef]
- Dzieciolowska, S.; Hamel, D.; Gadio, S.; Dionne, M.; Gagnon, D.; Robitaille, L.; Cook, E.; Caron, I.; Talib, A.; Parkes, L.; et al. Covid-19 Vaccine Acceptance, Hesitancy and Refusal among Canadian Healthcare Workers: A Multicenter Survey. Am. J. Infect. Control. 2021. [Google Scholar] [CrossRef]
- Paris, C.; Bénézit, F.; Geslin, M.; Polard, E.; Baldeyrou, M.; Turmel, V.; Tadié, É.; Garlantezec, R.; Tattevin, P. COVID-19 vaccine hesitancy among healthcare workers. Infect. Dis. Now 2021, S2666. [Google Scholar] [CrossRef]
- Papagiannis, D.; Rachiotis, G.; Malli, F.; Papathanasiou, I.V.; Kotsiou, O.; Fradelos, E.C.; Giannakopoulos, K.; Gourgoulianis, K.I. Acceptability of COVID-19 Vaccination among Greek Health Professionals. Vaccines 2021, 9, 200. [Google Scholar] [CrossRef]
- Nohl, A.; Afflerbach, C.; Lurz, C.; Brune, B.; Ohmann, T.; Weichert, V.; Zeiger, S.; Dudda, M. Acceptance of COVID-19 Vaccination among Front-Line Health Care Workers: A Nationwide Survey of Emergency Medical Services Personnel from Germany. Vaccines 2021, 9. [Google Scholar] [CrossRef]
- Spinewine, A.; Pétein, C.; Evrard, P.; Vastrade, C.; Laurent, C.; Delaere, B.; Henrard, S. Attitudes towards COVID-19 Vaccination among Hospital Staff—Understanding What Matters to Hesitant People. Vaccines 2021, 9, 469. [Google Scholar] [CrossRef]
- Qattan, A.M.N.; Alshareef, N.; Alsharqi, O.; Al Rahahleh, N.; Chirwa, G.C.; Al-Hanawi, M.K. Acceptability of a COVID-19 Vaccine Among Healthcare Workers in the Kingdom of Saudi Arabia. Front. Med. 2021, 8, 644300. [Google Scholar] [CrossRef]
- Detoc, M.; Bruel, S.; Frappe, P.; Tardy, B.; Botelho-Nevers, E.; Gagneux-Brunon, A. Intention to participate in a COVID-19 vaccine clinical trial and to get vaccinated against COVID-19 in France during the pandemic. Vaccine 2020, 38, 7002–7006. [Google Scholar] [CrossRef]
- Khubchandani, J.; Sharma, S.; Price, J.H.; Wiblishauser, M.J.; Sharma, M.; Webb, F.J. COVID-19 Vaccination Hesitancy in the United States: A Rapid National Assessment. J. Community Health 2021, 46, 270–277. [Google Scholar] [CrossRef] [PubMed]
- Gadoth, A.; Halbrook, M.; Martin-Blais, R.; Gray, A.; Tobin, N.H.; Ferbas, K.G.; Aldrovandi, G.M.; Rimoin, A.W. Cross-sectional Assessment of COVID-19 vaccine acceptance among health care workers in Los Angeles. Ann. Intern. Med. 2021, 174, 882–885. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B. Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- Wise, J. Covid-19: European Countries Suspend Use of Oxford-AstraZeneca Vaccine after Reports of Blood Clots. BMJ 2021, 372, n699. [Google Scholar] [CrossRef]
- Pottegård, A.; Lund, L.C.; Karlstad, Ø.; Dahl, J.; Andersen, M.; Hallas, J.; Lidegaard, Ø.; Tapia, G.; Gulseth, H.L.; Ruiz, P.L.-D. Arterial events, venous thromboembolism, thrombocytopenia, and bleeding after vaccination with Oxford-AstraZeneca ChAdOx1-S in Denmark and Norway: Population based cohort study. BMJ 2021, 373, n1114. [Google Scholar] [CrossRef]
- Chirumbolo, S. Vaccination hesitancy and the “myth” on mRNA-based vaccines in Italy in the COVID-19 era: Does urgency meet major safety criteria? J. Med Virol. 2021, 93, 4049–4053. [Google Scholar] [CrossRef]
- Anand, P.; Stahel, V.P. The safety of Covid-19 mRNA vaccines: A review. Patient Saf. Surg. 2021, 15, 20. [Google Scholar] [CrossRef]
- Ghazy, R.M.; Abd ElHafeez, S.; Shaaban, R.; Elbarazi, I.; Abdou, M.S.; Ramadan, A.; Kheirallah, K.A. Determining the Cutoff Points of the 5C Scale for Assessment of COVID-19 Vaccines Psychological Antecedents among the Arab Population: A Multinational Study. J. Prim. Care Community Health 2021, 12, 21501327211018568. [Google Scholar] [CrossRef]
- Puci, M.V.; Nosari, G.; Loi, F.; Puci, G.V.; Montomoli, C.; Ferraro, O.E. Risk Perception and Worries among Health Care Workers in the COVID-19 Pandemic: Findings from an Italian Survey. Healthcare 2020, 8, 535. [Google Scholar] [CrossRef]
- Abolfotouh, M.A.; Almutairi, A.F.; BaniMustafa, A.A.; Hussein, M.A. Perception and attitude of healthcare workers in Saudi Arabia with regard to Covid-19 pandemic and potential associated predictors. BMC Infect. Dis. 2020, 20, 719. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2021, 27, 225–228. [Google Scholar] [CrossRef]
- Dini, G.; Toletone, A.; Sticchi, L.; Orsi, A.; Bragazzi, N.L.; Durando, P. Influenza vaccination in healthcare workers: A comprehensive critical appraisal of the literature. Hum. Vaccines Immunother. 2018, 14, 772–789. [Google Scholar] [CrossRef] [Green Version]
- Karlsson, L.C.; Lewandowsky, S.; Antfolk, J.; Salo, P.; Lindfelt, M.; Oksanen, T.; Kivimäki, M.; Soveri, A. The association between vaccination confidence, vaccination behavior, and willingness to recommend vaccines among Finnish healthcare workers. PLoS ONE 2019, 14, e0224330. [Google Scholar] [CrossRef]
- Sallam, M.; Dababseh, D.; Yaseen, A.; Al-Haidar, A.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. Conspiracy Beliefs Are Associated with Lower Knowledge and Higher Anxiety Levels Regarding COVID-19 among Students at the University of Jordan. Int. J. Environ. Res. Public Health 2020, 17. [Google Scholar] [CrossRef]
- Trafimow, D. A Frequentist Alternative to Significance Testing, p-Values, and Confidence Intervals. Econometrics 2019, 7, 26. [Google Scholar] [CrossRef] [Green Version]
- Trafimow, D.; Earp, B.D. Null hypothesis significance testing and Type I error: The domain problem. New Ideas Psychol. 2017, 45, 19–27. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Feature | N 3 (%) |
|---|---|---|
| Mean age (SD 1) | 33.6 (9.7) | |
| Sex | Male | 393 (38.6) |
| Female | 626 (61.4) | |
| Nationality | Kuwaiti | 765 (75.1) |
| Non-Kuwaiti | 221 (21.7) | |
| Stateless/unknown | 33 (3.2) | |
| Occupation | Physician | 292 (28.7) |
| Dentist | 170 (16.7) | |
| Pharmacist | 206 (20.2) | |
| Nurse | 127 (12.5) | |
| Laboratory technician | 80 (7.9) | |
| Other 2 | 144 (14.1) | |
| Educational level | Undergraduate degree | 662 (65.0) |
| Postgraduate degree | 357 (35.0) | |
| Workplace | Public | 915 (89.8) |
| Private | 104 (10.2) | |
| History of chronic disease | Yes | 182 (17.9) |
| No | 837 (82.1) | |
| Experience of COVID-19 in self or family | Yes | 523 (51.3) |
| No | 496 (48.7) |
| Characteristic | Feature | Occupation N 2 (%) | p Value 4 | |||||
|---|---|---|---|---|---|---|---|---|
| Physician | Dentist | Pharmacist | Nurse | Laboratory Technician | Other 3 | |||
| Age | Mean (SD 1) | 36 (11.0) | 31 (7.1) | 34 (8.4) | 33 (9.2) | 35 (10.7) | 32 (10.1) | 0.001 |
| Sex | Male | 150 (51.4) | 101 (59.4) | 45 (21.8) | 33 (26.0) | 25 (31.3) | 39 (27.1) | <0.001 |
| Female | 142 (48.6) | 69 (40.6) | 161 (78.2) | 94 (74.0) | 55 (68.8) | 105 (72.9) | ||
| Nationality | Kuwaiti | 229 (78.4) | 148 (87.1) | 188 (91.3) | 33 (26.0) | 51 (63.7) | 116 (80.6) | <0.001 |
| Non-Kuwaiti | 56 (19.2) | 17 (10.0) | 16 (7.8) | 88 (69.3) | 22 (27.5) | 22 (15.3) | ||
| Stateless/unknown | 7 (2.4) | 5 (2.9) | 2 (1.0) | 6 (4.7) | 7 (8.8) | 6 (4.2) | ||
| Educational level | Undergraduate degree | 116 (39.7) | 105 (61.8) | 141 (68.4) | 120 (94.5) | 66 (82.5) | 114 (79.2) | <0.001 |
| Postgraduate degree | 176 (60.3) | 65 (38.2) | 65 (31.6) | 7 (5.5) | 14 (17.5) | 30 (20.8) | ||
| Workplace | Public | 276 (94.5) | 152 (89.4) | 175 (85.0) | 112 (88.2) | 77 (96.3) | 123 (85.4) | 0.002 |
| Private | 16 (5.5) | 18 (10.6) | 31 (15.0) | 15 (11.8) | 3 (3.8) | 21 (14.6) | ||
| Variable | Feature | Did You Get COVID-19 Vaccine/Do You Intend to Get COVID-19 Vaccine? N 3 (%) | p Value 4 | ||
|---|---|---|---|---|---|
| Yes | No | Maybe | |||
| Mean age (SD 1) | 33.9 (9.9) | 31.8 (8.7) | 32.2 (8.1) | 0.208 | |
| Sex | Male | 359 (91.3) | 15 (3.8) | 19 (4.8) | <0.001 *** |
| Female | 490 (78.3) | 77 (12.3) | 59 (9.4) | ||
| Nationality | Kuwaiti | 651 (85.1) | 65 (8.5) | 49 (6.4) | 0.031 * |
| Non-Kuwaiti | 172 (77.8) | 22 (10.0) | 27 (12.2) | ||
| Stateless/unknown | 26 (78.8) | 5 (15.2) | 2 (6.1) | ||
| Occupation | Physician | 264 (90.4) | 13 (4.5) | 15 (5.1) | <0.001 *** |
| Dentist | 155 (91.2) | 5 (2.9) | 10 (5.9) | ||
| Pharmacist | 165 (80.1) | 26 (12.6) | 15 (7.3) | ||
| Nurse | 89 (70.1) | 22 (17.3) | 16 (12.6) | ||
| Laboratory technician | 61 (76.3) | 11 (13.8) | 8 (10.0) | ||
| Other 2 | 115 (79.9) | 15 (10.4) | 14 (9.7) | ||
| Educational level | Undergraduate degree | 530 (80.1) | 71 (10.7) | 61 (9.2) | 0.001 ** |
| Postgraduate degree | 319 (89.4) | 21 (5.9) | 17 (4.8) | ||
| Workplace | Public | 773 (84.5) | 80 (8.7) | 62 (6.8) | 0.004 ** |
| Private | 76 (73.1) | 12 (11.5) | 16 (15.4) | ||
| History of chronic disease | Yes | 147 (80.8) | 24 (13.2) | 11 (6.0) | 0.075 |
| No | 702 (83.9) | 68 (8.1) | 67 (8.0) | ||
| Experience of COVID-19 in self or family | Yes | 434 (83.0) | 51 (9.8) | 38 (7.3) | 0.654 |
| No | 415 (83.7) | 41 (8.3) | 40 (8.1) | ||
| Variable | Feature | COVID-19 Vaccine Class N 3 (%) | p Value 4 | |||
|---|---|---|---|---|---|---|
| mRNA 2 | Viral Vector | Sub-unit | Inactivated | |||
| Sex | Male | 278 (70.7) | 31 (7.9) | 3 (0.8) | 81 (20.6) | <0.001 *** |
| Female | 360 (57.5) | 72 (11.5) | 22 (3.5) | 172 (27.5) | ||
| Nationality | Kuwaiti | 486 (63.5) | 83 (10.8) | 21 (2.7) | 175 (22.9) | 0.084 |
| Non-Kuwaiti | 129 (58.4) | 20 (9.0) | 4 (1.8) | 68 (30.8) | ||
| Stateless/unknown | 23 (69.7) | 0 | 0 | 10 (30.3) | ||
| Occupation | Physician | 216 (74.0) | 17 (5.8) | 2 (0.7) | 57 (19.5) | <0.001 *** |
| Dentist | 125 (73.5) | 13 (7.6) | 1 (0.6) | 31 (18.2) | ||
| Pharmacist | 120 (58.3) | 40 (19.4) | 3 (1.5) | 43 (20.9) | ||
| Nurse | 57 (44.9) | 13 (10.2) | 6 (4.7) | 51 (40.2) | ||
| Laboratory technician | 43 (53.8) | 6 (7.5) | 4 (5.0) | 27 (33.8) | ||
| Other 1 | 77 (53.5) | 14 (9.7) | 9 (6.3) | 44 (30.6) | ||
| Educational level | Undergraduate degree | 399 (60.3) | 72 (10.9) | 19 (2.9) | 172 (26.0) | 0.164 |
| Postgraduate degree | 239 (66.9) | 31 (8.7) | 6 (1.7) | 81 (22.7) | ||
| Workplace | Public | 575 (62.8) | 94 (10.3) | 22 (2.4) | 224 (24.5) | 0.839 |
| Private | 63 (60.6) | 9 (8.7) | 3 (2.9) | 29 (27.9) | ||
| History of chronic disease | Yes | 118 (64.8) | 18 (9.9) | 4 (2.2) | 42 (23.1) | 0.915 |
| No | 520 (62.1) | 85 (10.2) | 21 (2.5) | 211 (25.2) | ||
| Experience of COVID-19 in self or family | Yes | 340 (65.0) | 52 (9.9) | 11 (2.1) | 120 (22.9) | 0.378 |
| No | 298 (60.1) | 51 (10.3) | 14 (2.8) | 133 (26.8) | ||
| Variable | Feature | COVID-19 Vaccine Type (Developer) N 2 (%) | p Value 3 | |||||
|---|---|---|---|---|---|---|---|---|
| Pfizer-BioNTech | Sinopharm | Oxford-AstraZeneca | Sputnik | Moderna | Johnson & Johnson | |||
| Sex | Male | 298 (75.8) | 11 (2.8) | 58 (14.8) | 4 (1.0) | 2 (0.5) | 20 (5.1) | 0.027 * |
| Female | 412 (65.8) | 17 (2.7) | 135 (21.6) | 9 (1.4) | 7 (1.1) | 46 (7.3) | ||
| Nationality | Kuwaiti | 544 (71.1) | 14 (1.8) | 141 (18.4) | 11 (1.4) | 7 (0.9) | 48 (6.3) | 0.024 * |
| Non-Kuwaiti | 138 (62.4) | 14 (6.3) | 48 (21.7) | 2 (0.9) | 2 (0.9) | 17 (7.7) | ||
| Stateless/unknown | 28 (84.8) | 0 | 4 (12.1) | 0 | 0 | 1 (3.0) | ||
| Occupation | Physician | 224 (76.7) | 7 (2.4) | 43 (14.7) | 3 (1.0) | 3 (1.0) | 12 (4.1) | <0.001 *** |
| Dentist | 144 (84.7) | 2 (1.2) | 16 (9.4) | 0 | 1 (0.6) | 7 (4.1) | ||
| Pharmacist | 125 (60.7) | 4 (1.9) | 54 (26.2) | 1 (0.5) | 0 | 22 (10.7) | ||
| Nurse | 72 (56.7) | 5 (3.9) | 38 (29.9) | 2 (1.6) | 1 (0.8) | 9 (7.1) | ||
| Laboratory technician | 52 (65.0) | 3 (3.8) | 14 (17.5) | 3 (3.8) | 1 (1.3) | 7 (8.8) | ||
| Other 1 | 93 (64.6) | 7 (4.9) | 28 (19.4) | 4 (2.8) | 3 (2.1) | 9 (6.3) | ||
| Educational level | Undergraduate degree | 443 (66.9) | 20 (3.0) | 139 (21.0) | 9 (1.4) | 6 (0.9) | 45 (6.8) | 0.205 |
| Postgraduate degree | 267 (74.8) | 8 (2.2) | 54 (15.1) | 4 (1.1) | 3 (0.8) | 21 (5.9) | ||
| Workplace | Public | 645 (70.5) | 22 (2.4) | 173 (18.9) | 13 (1.4) | 9 (1.0) | 53 (5.8) | 0.018 * |
| Private | 65 (62.5) | 6 (5.8) | 20 (19.2) | 0 | 0 | 13 (12.5) | ||
| History of chronic disease | Yes | 120 (65.9) | 7 (3.8) | 41 (22.5) | 3 (1.6) | 3 (1.6) | 8 (4.4) | 0.295 |
| No | 590 (70.5) | 21 (2.5) | 152 (18.2) | 10 (1.2) | 6 (0.7) | 58 (6.9) | ||
| Experience of COVID-19 in self or family | Yes | 364 (69.6) | 13 (2.5) | 97 (18.5) | 3 (0.6) | 4 (0.8) | 42 (8.0) | 0.122 |
| No | 346 (69.8) | 15 (3.0) | 96 (19.4) | 10 (2.0) | 5 (1.0) | 24 (4.8) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Sanafi, M.; Sallam, M. Psychological Determinants of COVID-19 Vaccine Acceptance among Healthcare Workers in Kuwait: A Cross-Sectional Study Using the 5C and Vaccine Conspiracy Beliefs Scales. Vaccines 2021, 9, 701. https://doi.org/10.3390/vaccines9070701
Al-Sanafi M, Sallam M. Psychological Determinants of COVID-19 Vaccine Acceptance among Healthcare Workers in Kuwait: A Cross-Sectional Study Using the 5C and Vaccine Conspiracy Beliefs Scales. Vaccines. 2021; 9(7):701. https://doi.org/10.3390/vaccines9070701
Chicago/Turabian StyleAl-Sanafi, Mariam, and Malik Sallam. 2021. "Psychological Determinants of COVID-19 Vaccine Acceptance among Healthcare Workers in Kuwait: A Cross-Sectional Study Using the 5C and Vaccine Conspiracy Beliefs Scales" Vaccines 9, no. 7: 701. https://doi.org/10.3390/vaccines9070701
APA StyleAl-Sanafi, M., & Sallam, M. (2021). Psychological Determinants of COVID-19 Vaccine Acceptance among Healthcare Workers in Kuwait: A Cross-Sectional Study Using the 5C and Vaccine Conspiracy Beliefs Scales. Vaccines, 9(7), 701. https://doi.org/10.3390/vaccines9070701