
Association between Elevated TGA-IgA Titers and Older Age at Diagnosis with Absence of HBV Seroconversion in Celiac Children

 ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
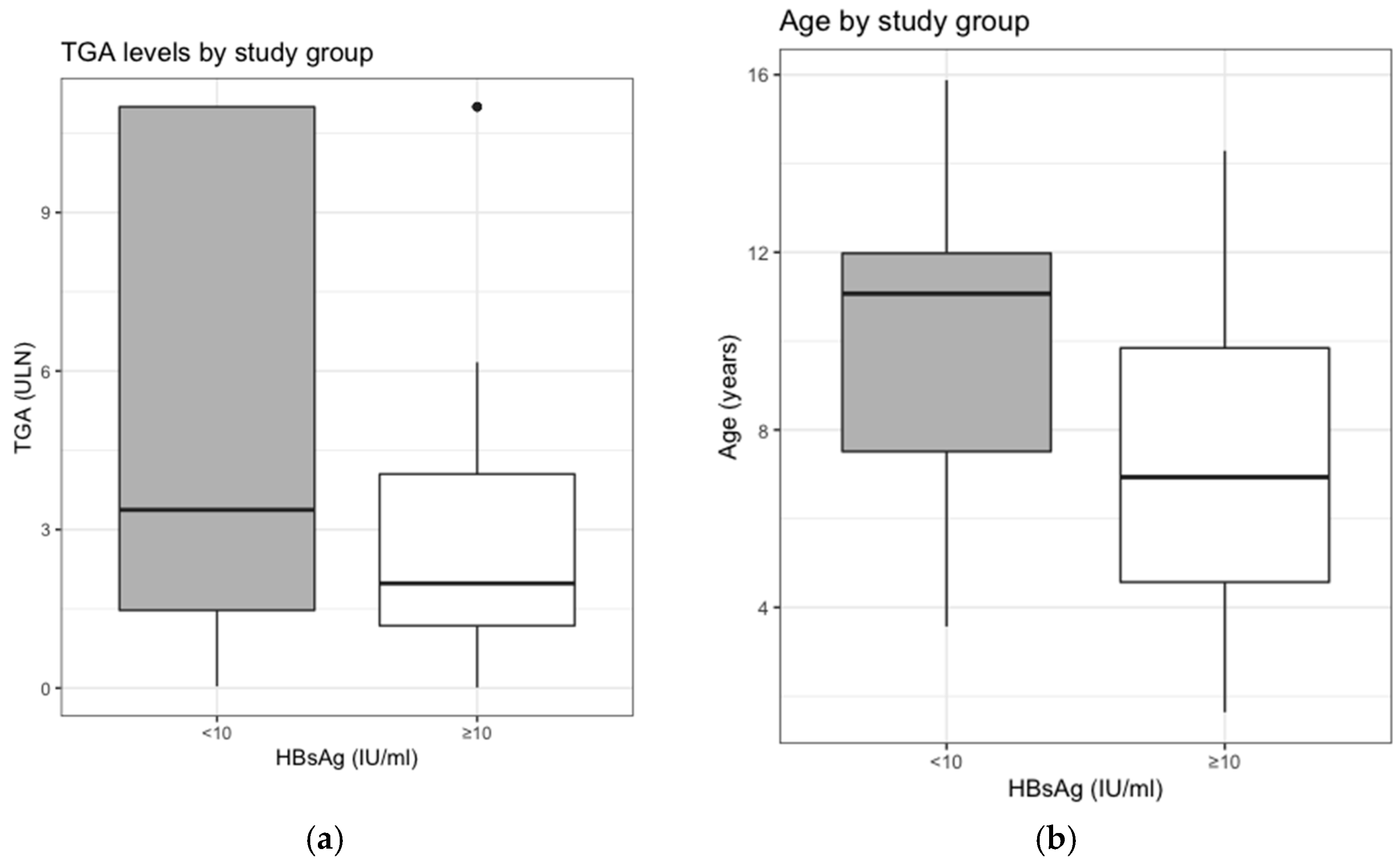
3.1. Mean TGA-IgA and Serologic Response to the Vaccination
3.2. Clinical Presentation and Serologic Response to the Vaccination
3.3. Median Age and Serologic Response to the Vaccination
3.4. Regression Analysis on the Response to the Vaccine
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ludvigsson, J.F.; Leffler, D.A.; Bai, J.C.; Biagi, F.; Fasano, A.; Green, P.H.; Hadjivassiliou, M.; Kaukinen, K.; Kelly, C.P.; Leonard, J.N.; et al. The Oslo definitions for coeliac disease and related terms. Gut 2013, 62, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Green, P.H.; Krishnareddy, S.; Lebwohl, B. Clinical manifestations of celiac disease. Digit. Dis. 2015, 33, 137–140. [Google Scholar] [CrossRef] [PubMed]
- Trovato, C.M.; Raucci, U.; Valitutti, F.; Montuori, M.; Villa, M.P.; Cucchiara, S.; Parisi, P. Neuropsychiatric manifestations in celiac disease. Epilepsy Behav. 2019, 99, 106393. [Google Scholar] [CrossRef]
- Lundin, K.E.; Wijmenga, C. Coeliac disease and autoimmune disease-genetic overlap and screening. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 507–515. [Google Scholar] [CrossRef]
- Popp, A.; Maki, M. Changing pattern of childhood celiac disease epidemiology: Contributing factors. Front. Pediatr. 2019, 7, 357. [Google Scholar] [CrossRef] [PubMed]
- Husby, S.; Koletzko, S.; Korponay-Szabo, I.R.; Mearin, M.L.; Phillips, A.; Shamir, R.; Troncone, R.; Giersiepen, K.; Branski, D.; Catassi, C.; et al. European society for pediatric gastroenterology, hepatology, and nutrition guidelines for the diagnosis of coeliac disease. J. Pediatr. Gastroenterol. Nutr. 2012, 54, 136–160. [Google Scholar] [CrossRef] [PubMed]
- Husby, S.; Koletzko, S.; Korponay-Szabo, I.; Kurppa, K.; Mearin, M.L.; Ribes-Koninckx, C.; Shamir, R.; Troncone, R.; Auricchio, R.; Castillejo, G.; et al. European society paediatric gastroenterology, hepatology and nutrition guidelines for diagnosing coeliac disease 2020. J. Pediatr. Gastroenterol. Nutr. 2020, 70, 141–156. [Google Scholar] [CrossRef]
- Valitutti, F.; Trovato, C.M.; Montuori, M.; Cucchiara, S. Pediatric celiac disease: Follow-up in the spotlight. Adv. Nutr. 2017, 8, 356–361. [Google Scholar] [CrossRef]
- Tiberti, C.; Montuori, M.; Panimolle, F.; Trovato, C.M.; Anania, C.; Valitutti, F.; Vestri, A.R.; Lenzi, A.; Cucchiara, S.; Morano, S. Screening for type 1 diabetes-, thyroid-, gastric-, and adrenal-specific humoral autoimmunity in 529 children and adolescents with celiac disease at diagnosis identifies as positive one in every nine patients. Diabetes Care 2017, 40, e10–e11. [Google Scholar] [CrossRef] [PubMed]
- Tiberti, C.; Montuori, M.; Trovato, C.M.; Panimolle, F.; Filardi, T.; Valitutti, F.; Lenzi, A.; Cucchiara, S.; Morano, S. Gluten-free diet impact on dynamics of pancreatic islet-specific autoimmunity detected at celiac disease diagnosis. Pediatr. Diabetes 2020, 21, 774–780. [Google Scholar] [CrossRef] [PubMed]
- Lionetti, E.; Gatti, S.; Galeazzi, T.; Caporelli, N.; Francavilla, R.; Cucchiara, S.; Roggero, P.; Malamisura, B.; Iacono, G.; Tomarchio, S.; et al. Safety of oats in children with celiac disease: A double-blind, randomized, placebo-controlled trial. J. Pediatr. 2018, 194, 116–122.e2. [Google Scholar] [CrossRef] [PubMed]
- Valitutti, F.; Iorfida, D.; Anania, C.; Trovato, C.M.; Montuori, M.; Cucchiara, S.; Catassi, C. Cereal consumption among subjects with celiac disease: A snapshot for nutritional considerations. Nutrients 2017, 9, 396. [Google Scholar] [CrossRef] [PubMed]
- Trovato, C.M.; Montuori, M.; Oliva, S.; Cucchiara, S.; Cignarelli, A.; Sansone, A. Assessment of public perceptions and concerns of celiac disease: A Twitter-based sentiment analysis study. Dig. Liver Dis. 2020, 52, 464–466. [Google Scholar] [CrossRef] [PubMed]
- Saco, T.V.; Strauss, A.T.; Ledford, D.K. Hepatitis B vaccine nonresponders: Possible mechanisms and solutions. Ann. Allergy Asthma Immunol. 2018, 121, 320–327. [Google Scholar] [CrossRef] [PubMed]
- Opri, R.; Veneri, D.; Mengoli, C.; Zanoni, G. Immune response to hepatitis B vaccine in patients with celiac disease: A systematic review and meta-analysis. Hum. Vaccines Immunother. 2015, 11, 2800–2805. [Google Scholar] [CrossRef] [PubMed]
- Mormile, R. Hepatitis B vaccine non response: A predictor of latent autoimmunity? Med. Hypotheses 2017, 104, 45–47. [Google Scholar] [CrossRef] [PubMed]
- Inoue, T.; Tanaka, Y. Cross-protection of hepatitis B vaccination among different genotypes. Vaccines 2020, 8, 456. [Google Scholar] [CrossRef]
- Anania, C.; Olivero, F.; Spagnolo, A.; Chiesa, C.; Pacifico, L. Immune response to vaccines in children with celiac disease. World J. Gastroenterol. 2017, 23, 3205–3213. [Google Scholar] [CrossRef]
- Zingone, F.; Capone, P.; Tortora, R.; Rispo, A.; Morisco, F.; Caporaso, N.; Imperatore, N.; De Stefano, G.; Iovino, P.; Ciacci, C. Role of gluten intake at the time of hepatitis B virus vaccination in the immune response of celiac patients. Clin. Vaccine Immunol. 2013, 20, 660–662. [Google Scholar] [CrossRef]
- Zingone, F.; Morisco, F.; Zanetti, A.; Romano, L.; Portella, G.; Capone, P.; Andreozzi, P.; Tortora, R.; Ciacci, C. Long-term antibody persistence and immune memory to hepatitis B virus in adult celiac patients vaccinated as adolescents. Vaccine 2011, 29, 1005–1008. [Google Scholar] [CrossRef]
- Jabri, B.; Sollid, L.M. Tissue-mediated control of immunopathology in coeliac disease. Nat. Rev. Immunol. 2009, 9, 858–870. [Google Scholar] [CrossRef] [PubMed]
- Vitaliti, G.; Pratico, A.D.; Cimino, C.; Di Dio, G.; Lionetti, E.; La Rosa, M.; Leonardi, S. Hepatitis B vaccine in celiac disease: Yesterday, today and tomorrow. World J. Gastroenterol. 2013, 19, 838–845. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.K.; Nie, J.J.; Li, J.; Zhuang, H. The effect of HLA on immunological response to hepatitis B vaccine in healthy people: A meta-analysis. Vaccine 2013, 31, 4355–4361. [Google Scholar] [CrossRef] [PubMed]
- Martinetti, M.; De Silvestri, A.; Belloni, C.; Pasi, A.; Tinelli, C.; Pistorio, A.; Salvaneschi, L.; Rondini, G.; Avanzini, M.A.; Cuccia, M. Humoral response to recombinant hepatitis B virus vaccine at birth: Role of HLA and beyond. Clin. Immunol. 2000, 97, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Tang, J.; Song, W.; Lobashevsky, E.; Wilson, C.M.; Kaslow, R.A. HLA and cytokine gene polymorphisms are independently associated with responses to hepatitis B vaccination. Hepatology 2004, 39, 978–988. [Google Scholar] [CrossRef] [PubMed]
- Godkin, A.; Davenport, M.; Hill, A.V. Molecular analysis of HLA class II associations with hepatitis B virus clearance and vaccine nonresponsiveness. Hepatology 2005, 41, 1383–1390. [Google Scholar] [CrossRef]
- Thio, C.L.; Thomas, D.L.; Karacki, P.; Gao, X.; Marti, D.; Kaslow, R.A.; Goedert, J.J.; Hilgartner, M.; Strathdee, S.A.; Duggal, P.; et al. Comprehensive analysis of class I and class II HLA antigens and chronic hepatitis B virus infection. J. Virol. 2003, 77, 12083–12087. [Google Scholar] [CrossRef]
- Silvestri, F.; Tromba, V.; Mazzotta, I.; Costantino, F. How diabetes type 1 affects immune response to hepatitis B virus vaccine in pediatric population? Evaluation of a booster dose in unresponsive subjects with type 1 diabetes. Minerva Pediatr. 2019. [Google Scholar] [CrossRef]
- Watts, A.; Bennett, W.E.; Molleston, J.P.; Gupta, S.K.; Croffie, J.M.; Waseem, S.; McFerron, B.A.; Steiner, S.J.; Kumar, S.; Vanderpool, C.P.; et al. Incidence of low seroimmunity to hepatitis B virus in children with inflammatory bowel disease. J. Pediatr. Gastroenterol. Nutr. 2017, 65, 551–554. [Google Scholar] [CrossRef]
- Green, P.H. Celiac disease: How many biopsies for diagnosis? Gastrointest. Endosc. 2008, 67, 1088–1090. [Google Scholar] [CrossRef]
- Oberhuber, G.; Granditsch, G.; Vogelsang, H. The histopathology of coeliac disease: Time for a standardized report scheme for pathologists. Eur. J. Gastroenterol. Hepatol. 1999, 11, 1185–1194. [Google Scholar] [CrossRef] [PubMed]
- Ertekin, V.; Tosun, M.S.; Selimoglu, M.A. Is there need for a new hepatitis B vaccine schedule for children with celiac disease? Hepat. Mon. 2011, 11, 634–637. [Google Scholar] [CrossRef] [PubMed]
- Filippelli, M.; Garozzo, M.T.; Capizzi, A.; Spina, M.; Manti, S.; Tardino, L.; Salpietro, C.; Leonardi, S. Immune response to hepatitis B virus vaccine in celiac subjects at diagnosis. World J. Hepatol. 2016, 8, 1105–1109. [Google Scholar] [CrossRef] [PubMed]
- Trovato, C.M.; Albanese, C.V.; Leoni, S.; Celletti, I.; Valitutti, F.; Cavallini, C.; Montuori, M.; Barbato, M.; Catalano, C.; Cucchiara, S. Lack of clinical predictors for low mineral density in children with celiac disease. J. Pediatr. Gastroenterol. Nutr. 2014, 59, 799–802. [Google Scholar] [CrossRef]
- Leonardi, S.; Spina, M.; Spicuzza, L.; Rotolo, N.; La Rosa, M. Hepatitis B vaccination failure in celiac disease: Is there a need to reassess current immunization strategies? Vaccine 2009, 27, 6030–6033. [Google Scholar] [CrossRef]
- Zifman, E.; Zevit, N.; Heshin-Bekenstein, M.; Turner, D.; Shamir, R.; Silbermintz, A. Effect of a gluten free diet on hepatitis B surface antibody concentration in previously immunized pediatric celiac patients. Pediatr. Gastroenterol. Hepatol. Nutr. 2020, 23, 132–136. [Google Scholar] [CrossRef]
- Zanoni, G.; Contreas, G.; Valletta, E.; Gabrielli, O.; Mengoli, C.; Veneri, D. Normal or defective immune response to hepatitis B vaccine in patients with diabetes and celiac disease. Hum. Vaccines Immunother. 2015, 11, 58–62. [Google Scholar] [CrossRef]
- Wainwright, R.B.; Bulkow, L.R.; Parkinson, A.J.; Zanis, C.; McMahon, B.J. Protection provided by hepatitis B vaccine in a Yupik Eskimo population—Results of a 10-year study. J. Infect. Dis. 1997, 175, 674–677. [Google Scholar] [CrossRef]
- Heshin-Bekenstein, M.; Turner, D.; Shamir, R.; Bar-Meir, M.; Dagan, R.; Zevit, N.; Silbermintz, A. Hepatitis B Virus revaccination with standard versus pre-S vaccine in previously immunized patients with celiac disease. J. Pediatr. Gastroenterol. Nutr. 2015, 61, 400–403. [Google Scholar] [CrossRef]
- Rousseff, T.; Claeys, T.; Vande Vijver, E.; Moes, N.; Vande Velde, S.; Schelstraete, P.; De Bruyne, R.; Van Winckel, M.; Van Biervliet, S. Hepatitis B virus vaccination and revaccination response in children diagnosed with coeliac disease: A multicentre prospective study. Acta Gastroenterol. Belg. 2019, 82, 27–30. [Google Scholar]
- Nemes, E.; Lefler, E.; Szegedi, L.; Kapitany, A.; Kovacs, J.B.; Balogh, M.; Szabados, K.; Tumpek, J.; Sipka, S.; Korponay-Szabo, I.R. Gluten intake interferes with the humoral immune response to recombinant hepatitis B vaccine in patients with celiac disease. Pediatrics 2008, 121, e1570–e1576. [Google Scholar] [CrossRef] [PubMed]
- Passanisi, S.; Dipasquale, V.; Romano, C. Vaccinations and immune response in celiac disease. Vaccines 2020, 8, 278. [Google Scholar] [CrossRef] [PubMed]
- Filippelli, M.; Lionetti, E.; Pulvirenti, A.; Gennaro, A.; Lanzafame, A.; Marseglia, G.L.; Salpietro, C.; Rosa, M.L.; Leonardi, S. New approaches in hepatitis B vaccination for celiac disease. Immunotherapy 2014, 6, 945–952. [Google Scholar] [CrossRef] [PubMed]
- Filippelli, M.; Lionetti, E.; Gennaro, A.; Lanzafame, A.; Arrigo, T.; Salpietro, C.; La Rosa, M.; Leonardi, S. Hepatitis B vaccine by intradermal route in non responder patients: An update. World J. Gastroenterol. 2014, 20, 10383–10394. [Google Scholar] [CrossRef] [PubMed]
- Papadopoli, R.; De Sarro, C.; Torti, C.; Pileggi, C.; Pavia, M. Is there any opportunity to provide an hbv vaccine booster dose before anti-Hbs titer vanishes? Vaccines 2020, 8, 227. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Group A (anti HBs Ab > 10 mIU/mL) | Group B (anti HBs Ab < 10 mIU/mL) | p | |
|---|---|---|---|
| Number | 56 | 40 | |
| Female | 36 | 26 | |
| Male | 20 | 14 | |
| Median Age | 6.93 (IQR: 4.57–9.84) | 11.1 (IQR: 7.51–11.98) | <0.001 |
| TGA-IgA mean | 3.10 ± 2.90 | 5.10 ± 4.26 | 0.012 |
| TGA-IgA <10 ULN | 51 | 28 | |
| TGA-IgA >10 ULN | 5 | 12 | |
| Symptomatic children | 49 | 33 | n.s |
| Asymptomatic children | 7 | 7 | n.s |
| β | Std. Error | OR [95% CI] | p | |
|---|---|---|---|---|
| TGA titers (high vs. low) | −1.67 | 0.73 | 0.19 [0.04–0.81] | 0.023 |
| Symptoms (yes vs. no) | −0.96 | 0.75 | 0.38 [0.09–1.70] | 0.20 |
| Age (years) | −0.33 | 0.09 | 0.72 [0.60–0.86] | 0.0002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trovato, C.M.; Montuori, M.; Sansone, A.; Morelli, A.; Russo, G.; Pietropaoli, N.; Oliva, S. Association between Elevated TGA-IgA Titers and Older Age at Diagnosis with Absence of HBV Seroconversion in Celiac Children. Vaccines 2021, 9, 101. https://doi.org/10.3390/vaccines9020101
Trovato CM, Montuori M, Sansone A, Morelli A, Russo G, Pietropaoli N, Oliva S. Association between Elevated TGA-IgA Titers and Older Age at Diagnosis with Absence of HBV Seroconversion in Celiac Children. Vaccines. 2021; 9(2):101. https://doi.org/10.3390/vaccines9020101
Chicago/Turabian StyleTrovato, Chiara Maria, Monica Montuori, Andrea Sansone, Annalisa Morelli, Giusy Russo, Nicoletta Pietropaoli, and Salvatore Oliva. 2021. "Association between Elevated TGA-IgA Titers and Older Age at Diagnosis with Absence of HBV Seroconversion in Celiac Children" Vaccines 9, no. 2: 101. https://doi.org/10.3390/vaccines9020101
APA StyleTrovato, C. M., Montuori, M., Sansone, A., Morelli, A., Russo, G., Pietropaoli, N., & Oliva, S. (2021). Association between Elevated TGA-IgA Titers and Older Age at Diagnosis with Absence of HBV Seroconversion in Celiac Children. Vaccines, 9(2), 101. https://doi.org/10.3390/vaccines9020101