
Attitudes of Medical Students toward COVID-19 Vaccination: Who Is Willing to Receive a Third Dose of the Vaccine?


Abstract
:1. Introduction
2. Methods
2.1. Participants and Measures
2.2. Ethics
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. COVID-19 Dashboard. Available online: https://covid19.who.int/ (accessed on 8 October 2021).
- Azuma, K.; Nojiri, T.; Kawashima, M.; Hanai, A.; Ayaki, M.; Tsubota, K.; TRF-Japan Study Group. Possible favorable lifestyle changes owing to the coronavirus disease 2019 (COVID-19) pandemic among middle-aged Japanese women: An ancillary survey of the TRF-Japan study using the original “Taberhythm” smartphone app. PLoS ONE 2021, 16, e0248935. [Google Scholar] [CrossRef]
- Murayama, H.; Okubo, R.; Tabuchi, T. Increase in Social Isolation during the COVID-19 Pandemic and Its Association with Mental Health: Findings from the JACSIS 2020 Study. Int. J. Environ. Res. Public Health 2021, 18, 8238. [Google Scholar] [CrossRef]
- Nagasu, M.; Muto, K.; Yamamoto, I. Impacts of anxiety and socioeconomic factors on mental health in the early phases of the COVID-19 pandemic in the general population in Japan: A web-based survey. PLoS ONE 2021, 16, e0247705. [Google Scholar] [CrossRef]
- Tezuka, M.; Nagata, T.; Saeki, K.; Tsuboi, Y.; Fukutani, N. Association between Abrupt Change to Teleworking and Physical Symptoms During the Coronavirus Disease 2019 (COVID-19) Emergency Declaration in Japan. J. Occup. Environ. Med. 2021, in press. [Google Scholar] [CrossRef]
- Ministry of Health, Labour and Welfare: Notice on COVID-19 Vaccination. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000121431_00218.html (accessed on 14 September 2021). (In Japanese)
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. C4591001 Clinical Trial Group. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Harries, A.J.; Lee, C.; Jones, L.; Rodriguez, R.M.; Davis, J.A.; Boysen-Osborn, M.; Kashima, K.J.; Krane, N.K.; Rae, G.; Kman, N.; et al. Effects of the COVID-19 pandemic on medical students: A multicenter quantitative study. BMC Med. Educ. 2021, 21, 14. [Google Scholar] [CrossRef]
- Lucia, V.C.; Kelekar, A.; Afonso, N.M. COVID-19 vaccine hesitancy among medical students. J. Public Health 2021, 43, 445–449. [Google Scholar] [CrossRef]
- Saied, S.M.; Saied, E.M.; Kabbash, I.A.; Abdo, S.A.E. Vaccine hesitancy: Beliefs and barriers associated with COVID-19 vaccination among Egyptian medical students. J. Med. Virol. 2021, 93, 4280–4291. [Google Scholar] [CrossRef] [PubMed]
- Herzog, R.; Álvarez-Pasquin, M.J.; Díaz, C.; Del Barrio, J.L.; Estrada, J.M.; Gil, Á. Are healthcare workers’ intentions to vaccinate related to their knowledge, beliefs and attitudes? A systematic review. BMC Public Health 2013, 13, 154. [Google Scholar] [CrossRef] [Green Version]
- Reiter, P.L.; Pennell, M.L.; Katz, M.L. Acceptability of a COVID-19 vaccine among adults in the United States: How many people would get vaccinated? Vaccine 2020, 38, 6500–6507. [Google Scholar] [CrossRef] [PubMed]
- The Lancet Infectious Diseases. COVID-19 vaccine equity and booster doses. Lancet. Infect. Dis. 2021, 21, 1193. [Google Scholar] [CrossRef]
- Bar-On, Y.M.; Goldberg, Y.; Mandel, M.; Bodenheimer, O.; Freedman, L.; Kalkstein, N.; Mizrahi, B.; Alroy-Preis, S.; Ash, N.; Milo, R.; et al. Protection of BNT162b2 Vaccine Booster against Covid-19 in Israel. N. Engl. J. Med. 2021, in press. [Google Scholar] [CrossRef]
- Kamar, N.; Abravanel, F.; Marion, O.; Couat, C.; Izopet, J.; Del Bello, A. Three Doses of an mRNA Covid-19 Vaccine in Solid-Organ Transplant Recipients. N. Engl. J. Med. 2021, 385, 661–662. [Google Scholar] [CrossRef]
- Yue, L.; Xie, T.; Yang, T.; Zhou, J.; Chen, H.; Zhu, H.; Li, H.; Xiang, H.; Wang, J.; Yang, H.; et al. A third booster dose may be necessary to mitigate neutralizing antibody fading after inoculation with two doses of an inactivated SARS-CoV-2 vaccine. J. Med. Virol. 2021, in press. [Google Scholar] [CrossRef]
- Zhang, J.; He, Q.; An, C.; Mao, Q.; Gao, F.; Bian, L.; Wu, X.; Wang, Q.; Liu, P.; Song, L.; et al. Boosting with heterologous vaccines effectively improves protective immune responses of the inactivated SARS-CoV-2 vaccine. Emerg. Microbes. Infect. 2021, 10, 1598–1608. [Google Scholar] [CrossRef]
- Krause, P.R.; Fleming, T.R.; Peto, R.; Longini, I.M.; Figueroa, J.P.; Sterne, J.A.C.; Cravioto, A.; Rees, H.; Higgins, J.P.T.; Boutron, I.; et al. Considerations in boosting COVID-19 vaccine immune responses. Lancet 2021, 398, 1377–1380. [Google Scholar] [CrossRef]
- Mahase, E. Covid-19: Third vaccine dose boosts immune response but may not be needed, say researchers. BMJ 2021, 373, n1659. [Google Scholar] [CrossRef] [PubMed]
- Robinson, E.; Jones, A.; Lesser, I.; Daly, M. International estimates of intended uptake and refusal of COVID-19 vaccines: A rapid systematic review and meta-analysis of large nationally representative samples. Vaccine 2021, 39, 2024–2034. [Google Scholar] [CrossRef] [PubMed]
- Bălan, A.; Bejan, I.; Bonciu, S.; Eni, C.E.; Ruță, S. Romanian Medical Students’ Attitude towards and Perceived Knowledge on COVID-19 Vaccination. Vaccines 2021, 9, 854. [Google Scholar] [CrossRef]
- Talarek, E.; Warzecha, J.; Banasiuk, M.; Banaszkiewicz, A. Influenza Vaccination Coverage and Intention to Receive Hypothetical Ebola and COVID-19 Vaccines among Medical Students. Vaccines 2021, 9, 709. [Google Scholar] [CrossRef] [PubMed]
- Kanyike, A.M.; Olum, R.; Kajjimu, J.; Ojilong, D.; Akech, G.M.; Nassozi, D.R.; Agira, D.; Wamala, N.K.; Asiimwe, A.; Matovu, D.; et al. Acceptance of the coronavirus disease-2019 vaccine among medical students in Uganda. Trop. Med. Health 2021, 49, 37. [Google Scholar] [CrossRef]
- Petravić, L.; Arh, R.; Gabrovec, T.; Jazbec, L.; Rupčić, N.; Starešinič, N.; Zorman, L.; Pretnar, A.; Srakar, A.; Zwitter, M.; et al. Factors Affecting Attitudes towards COVID-19 Vaccination: An Online Survey in Slovenia. Vaccines 2021, 9, 247. [Google Scholar] [CrossRef]
- Pastorino, R.; Villani, L.; Mariani, M.; Ricciardi, W.; Graffigna, G.; Boccia, S. Impact of COVID-19 Pandemic on Flu and COVID-19 Vaccination Intentions among University Students. Vaccines 2021, 9, 70. [Google Scholar] [CrossRef]
- Szmyd, B.; Bartoszek, A.; Karuga, F.F.; Staniecka, K.; Błaszczyk, M.; Radek, M. Medical Students and SARS-CoV-2 Vaccination: Attitude and Behaviors. Vaccines 2021, 9, 128. [Google Scholar] [CrossRef] [PubMed]
- Rosental, H.; Shmueli, L. Integrating Health Behavior Theories to Predict COVID-19 Vaccine Acceptance: Differences between Medical Students and Nursing Students. Vaccines 2021, 9, 783. [Google Scholar] [CrossRef] [PubMed]
- Kelekar, A.K.; Lucia, V.C.; Afonso, N.M.; Mascarenhas, A.K. COVID-19 vaccine acceptance and hesitancy among dental and medical students. J. Am. Dent. Assoc. 2021, 152, 596–603. [Google Scholar] [CrossRef]
- Okubo, R.; Yoshioka, T.; Ohfuji, S.; Matsuo, T.; Tabuchi, T. COVID-19 Vaccine Hesitancy and Its Associated Factors in Japan. Vaccines 2021, 9, 662. [Google Scholar] [CrossRef]
- Xu, B.; Gao, X.; Zhang, X.; Hu, Y.; Yang, H.; Zhou, Y.H. Real-World Acceptance of COVID-19 Vaccines among Healthcare Workers in Perinatal Medicine in China. Vaccines 2021, 9, 704. [Google Scholar] [CrossRef] [PubMed]
- Graupensperger, S.; Abdallah, D.A.; Lee, C.M. Social norms and vaccine uptake: College students’ COVID vaccination intentions, attitudes, and estimated peer norms and comparisons with influenza vaccine. Vaccine 2021, 39, 2060–2067. [Google Scholar] [CrossRef]
- Sovicova, M.; Zibolenova, J.; Svihrova, V.; Hudeckova, H. Odds Ratio Estimation of Medical Students’ Attitudes towards COVID-19 Vaccination. Int. J. Environ. Res. Public Health. 2021, 18, 6815. [Google Scholar] [CrossRef]
- Sakai, H.; Shimizu, M.; Yoshimura, T.; Hato, E. Psychological Reactance to Mobility Restrictions Due to the COVID-19 Pandemic: A Japanese Population Study. Front. Psychol. 2021, 12, 655022. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Strongly | Srtongly | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Agree | (n) | Agree | (n) | Disagree | (n) | Disagree | (n) | ||
| Q1 | In principle, I approve of vaccinations. | 51.2% | (254) | 47.2% | (234) | 1.2% | (6) | 0.4% | (2) |
| Q2 | I have a fear of needles/shots. | 5.0% | (25) | 24.8% | (123) | 40.3% | (200) | 29.8% | (148) |
| Q3 | If I get COVID-19, I will develop severe symptoms. | 3.0% | (15) | 27.6% | (137) | 61.9% | (307) | 7.5% | (37) |
| Q4 | Parents’ opinion affected my decision of whether to receive the COVID-19 vaccine. | 13.1% | (65) | 32.7% | (162) | 29.8% | (148) | 24.4% | (121) |
| Q5 | Friends’ opinion affected my decision of whether to receive the COVID-19 vaccine. | 6.3% | (31) | 33.3% | (165) | 33.1% | (164) | 27.4% | (136) |
| Q6 | News media affected my decision of whether to receive the COVID-19 vaccine. | 4.0% | (20) | 33.1% | (164) | 35.3% | (175) | 27.6% | (137) |
| Q7 | Being free of charge affected my decision of whether to receive the COVID-19 vaccine. | 25.2% | (125) | 34.1% | (169) | 23.4% | (116) | 17.3% | (86) |
| Q8 | In general, the COVID-19 vaccine has apparent side effects. | 22.8% | (113) | 51.4% | (255) | 22.8% | (113) | 3.0% | (15) |
| Q9 | The vaccines provide a high degree of protection against COVID-19. | 11.9% | (59) | 63.7% | (316) | 22.0% | (109) | 2.4% | (12) |
| Q10 | The COVID-19 vaccine was developed too rapidly. | 10.3% | (51) | 35.7% | (177) | 48.2% | (239) | 5.8% | (29) |
| Q11 | I have received sufficient information about COVID-19 vaccination. | 7.3% | (36) | 49.6% | (246) | 38.9% | (193) | 4.2% | (21) |
| Q12 | COVID-19 vaccination is needed for me to travel or go out to eat and drink as in pre-pandemic life. | 44.0% | (218) | 48.8% | (242) | 6.0% | (30) | 1.2% | (6) |
| Q13 | The COVID-19 pandemic will continue for a long time. | 26.2% | (25) | 62.7% | (25) | 10.1% | (25) | 1.0% | (25) |
| Q14 | I have concerns about the sustainability of immunity by the COVID-19 vaccine. | 9.9% | (49) | 57.5% | (285) | 29.0% | (144) | 3.6% | (18) |
| Q15 | I am willing to get the COVID-19 vaccine in the future. | 40.7% | (202) | 50.0% | (248) | 7.7% | (38) | 1.6% | (8) |
| Students’ Willingness to Receive | ||||||
|---|---|---|---|---|---|---|
| Yes | No | |||||
| Age | 21.1 ± 2.4 | 20.8 ± 2.6 | ||||
| Grade | 3.4 ± 1.7 | 3.0 ± 1.6 | ||||
| Sex (male) | 58.9% | (264/450) | 65.2% | (30/46) | ||
| Past history of allergic reaction due to | ||||||
| food | 11.5% | (50/435) | 6.7% | (3/45) | ||
| medication | 5.1% | (22/435) | 2.2% | (1/45) | ||
| animal | 5.5% | (24/436) | 4.4% | (2/46) | ||
| pollen from plants and trees | 25.1% | (109/437) | 20.0% | (9/47) | ||
| house dust mites | 9.9% | (43/438) | 6.7% | (3/45) | ||
| unknown allergen | 3.9% | (17/435) | 4.4% | (2/46) | ||
| Past history of anaphylaxis | 0.5% | (2/435) | 0.0% | (0/435) | ||
| Past history of asthma | 3.4% | (15/435) | 2.2% | (1/45) | ||
| Past history of atopic dermatitis | 2.8% | (12/435) | 0.0% | (0/435) | ||
| Odds Ratio | 95% | CI | Wald Value | p Value | ||
|---|---|---|---|---|---|---|
| Completion of COVID-19 vaccination with a two-dose regimen | ||||||
| Grade | 1.57 | 1.24 | - | 1.98 | 13.71 | <0.001 |
| Q1 | 28.66 | 2.71 | - | 303.45 | 7.77 | 0.005 |
| Q4 | 0.41 | 0.21 | - | 0.83 | 6.24 | 0.013 |
| Q10 | 0.47 | 0.24 | - | 0.91 | 5.05 | 0.025 |
| Q12 | 10.49 | 4.09 | - | 26.89 | 23.94 | <0.001 |
| Willingness to receive the COVID-19 vaccine in future | ||||||
| Q1 | 8.61 | 1.44 | - | 51.55 | 5.56 | 0.018 |
| Q9 | 2.52 | 1.23 | - | 5.18 | 6.32 | 0.012 |
| Q10 | 0.26 | 0.12 | - | 0.55 | 12.25 | <0.001 |
| Q12 | 5.14 | 2.18 | - | 12.09 | 14.02 | <0.001 |
| Q14 | 2.53 | 1.22 | - | 5.28 | 6.15 | 0.013 |
| Odds Ratio | 95% | CI | Wald Value | p Value | ||
|---|---|---|---|---|---|---|
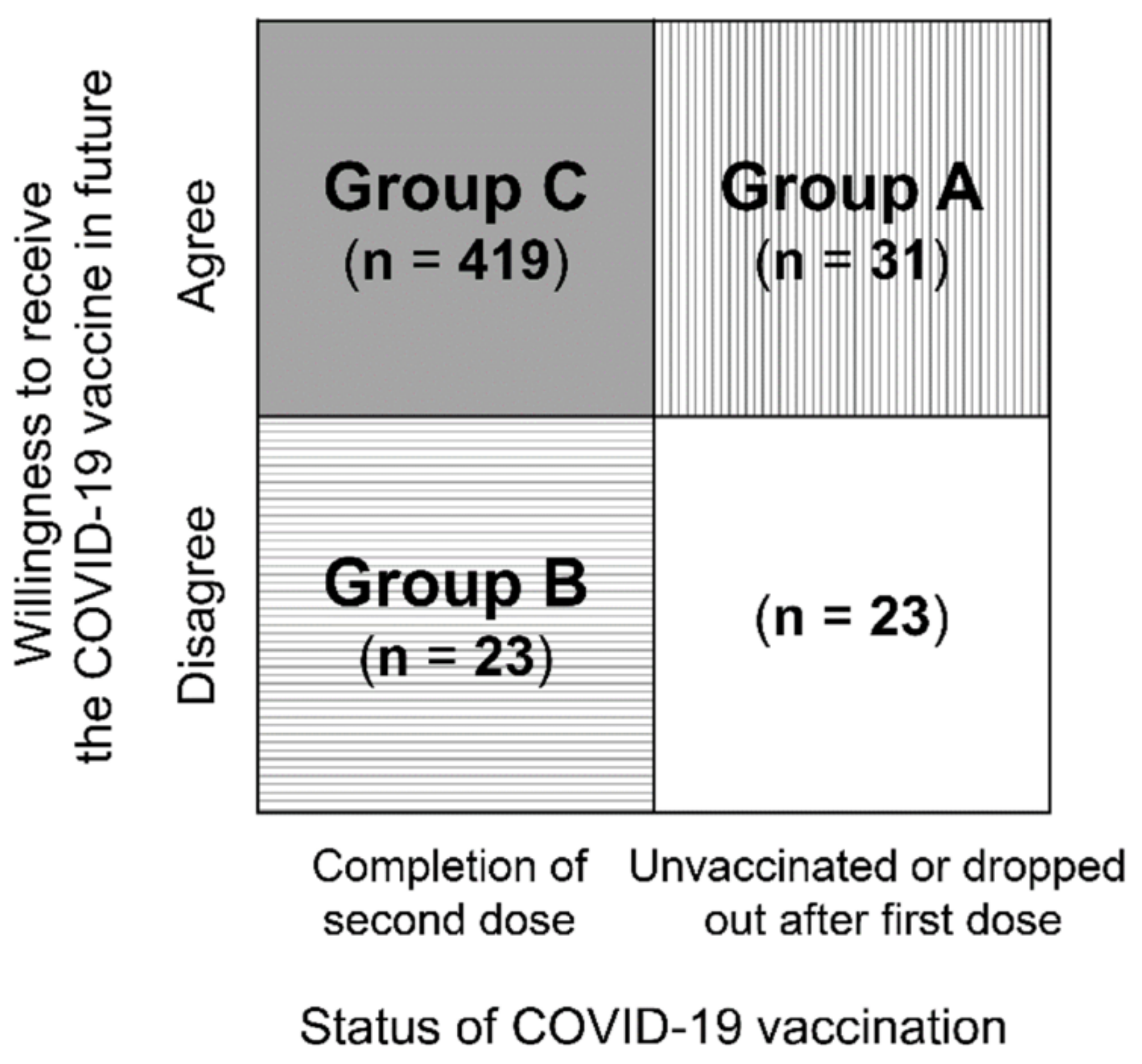
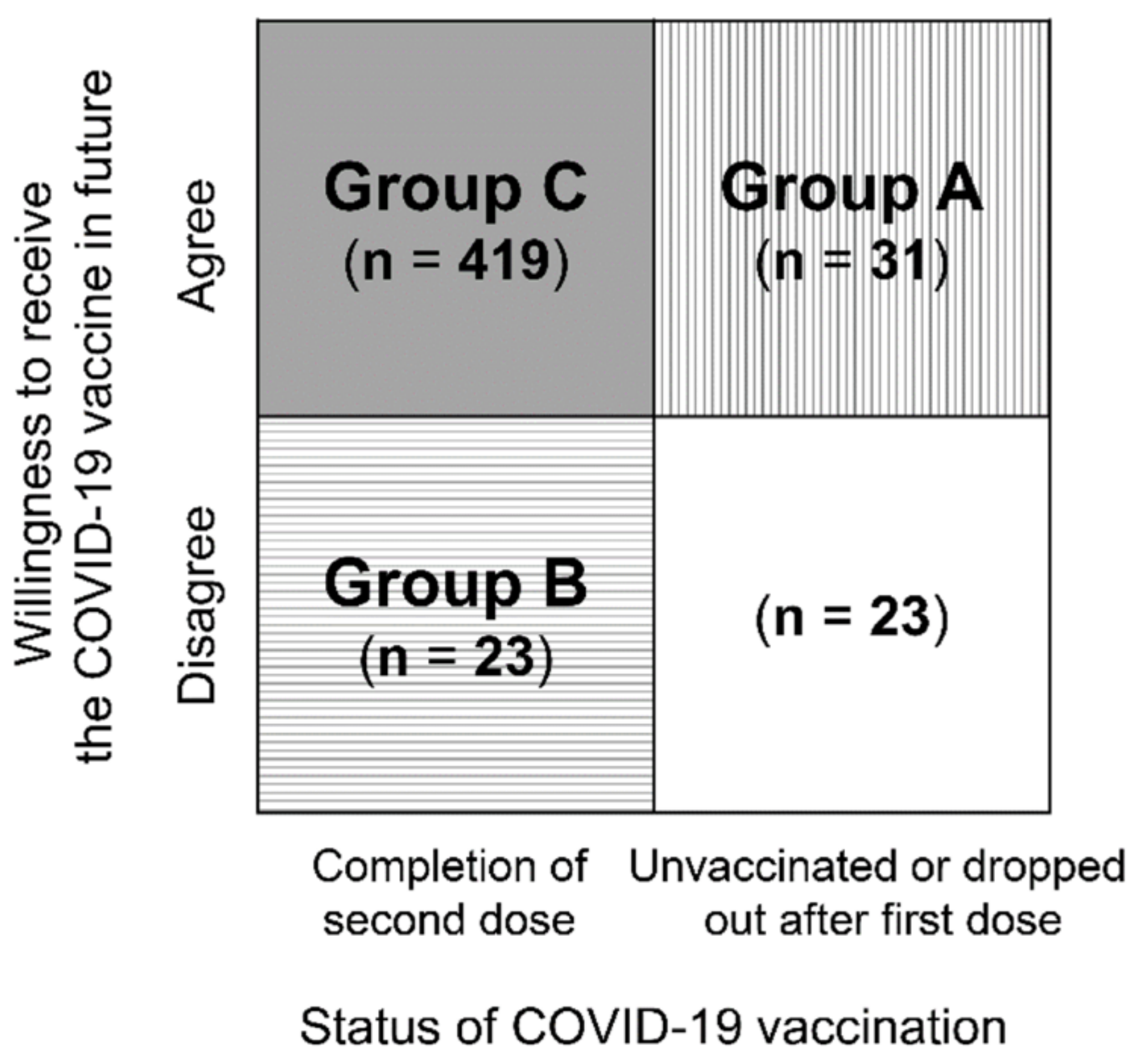
| Group A students who were unvaccinated or dropped out after the first dose of the COVID-19 vaccine but who are willing to receive the vaccine in the future. | ||||||
| Q10 | 4.50 | 1.69 | - | 11.96 | 9.11 | 0.003 |
| Q14 | 0.31 | 0.13 | - | 0.74 | 6.95 | 0.008 |
| Group B students who received a second dose of the COVID-19 vaccine but are not willing to receive the vaccine in the future. | ||||||
| Grade | 0.58 | 0.43 | - | 0.79 | 11.77 | 0.001 |
| Q2 | 3.23 | 1.44 | - | 7.25 | 8.12 | 0.004 |
| Q4 | 2.95 | 1.23 | - | 7.09 | 5.83 | 0.016 |
| Q12 | 0.26 | 0.08 | - | 0.93 | 4.33 | 0.038 |
| Odds Ratio | 95% | CI | Wald Value | p Value | ||
|---|---|---|---|---|---|---|
| Grade | 1.41 | 1.16 | - | 1.70 | 11.93 | 0.001 |
| Q1 | 9.85 | 1.08 | - | 89.83 | 4.11 | 0.043 |
| Q9 | 2.18 | 1.19 | - | 4.01 | 6.29 | 0.012 |
| Q10 | 0.32 | 0.17 | - | 0.57 | 14.61 | <0.001 |
| Q12 | 5.83 | 2.53 | - | 13.43 | 17.18 | <0.001 |
| Q14 | 2.20 | 1.20 | - | 4.02 | 6.53 | 0.011 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sugawara, N.; Yasui-Furukori, N.; Fukushima, A.; Shimoda, K. Attitudes of Medical Students toward COVID-19 Vaccination: Who Is Willing to Receive a Third Dose of the Vaccine? Vaccines 2021, 9, 1295. https://doi.org/10.3390/vaccines9111295
Sugawara N, Yasui-Furukori N, Fukushima A, Shimoda K. Attitudes of Medical Students toward COVID-19 Vaccination: Who Is Willing to Receive a Third Dose of the Vaccine? Vaccines. 2021; 9(11):1295. https://doi.org/10.3390/vaccines9111295
Chicago/Turabian StyleSugawara, Norio, Norio Yasui-Furukori, Atsuhito Fukushima, and Kazutaka Shimoda. 2021. "Attitudes of Medical Students toward COVID-19 Vaccination: Who Is Willing to Receive a Third Dose of the Vaccine?" Vaccines 9, no. 11: 1295. https://doi.org/10.3390/vaccines9111295
APA StyleSugawara, N., Yasui-Furukori, N., Fukushima, A., & Shimoda, K. (2021). Attitudes of Medical Students toward COVID-19 Vaccination: Who Is Willing to Receive a Third Dose of the Vaccine? Vaccines, 9(11), 1295. https://doi.org/10.3390/vaccines9111295