
Prediction Model for COVID-19 Vaccination Intention among the Mobile Population in China: Validation and Stability

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Measurement
2.3. Statistical Analyses
3. Results
3.1. Demographic Characteristics of Participants
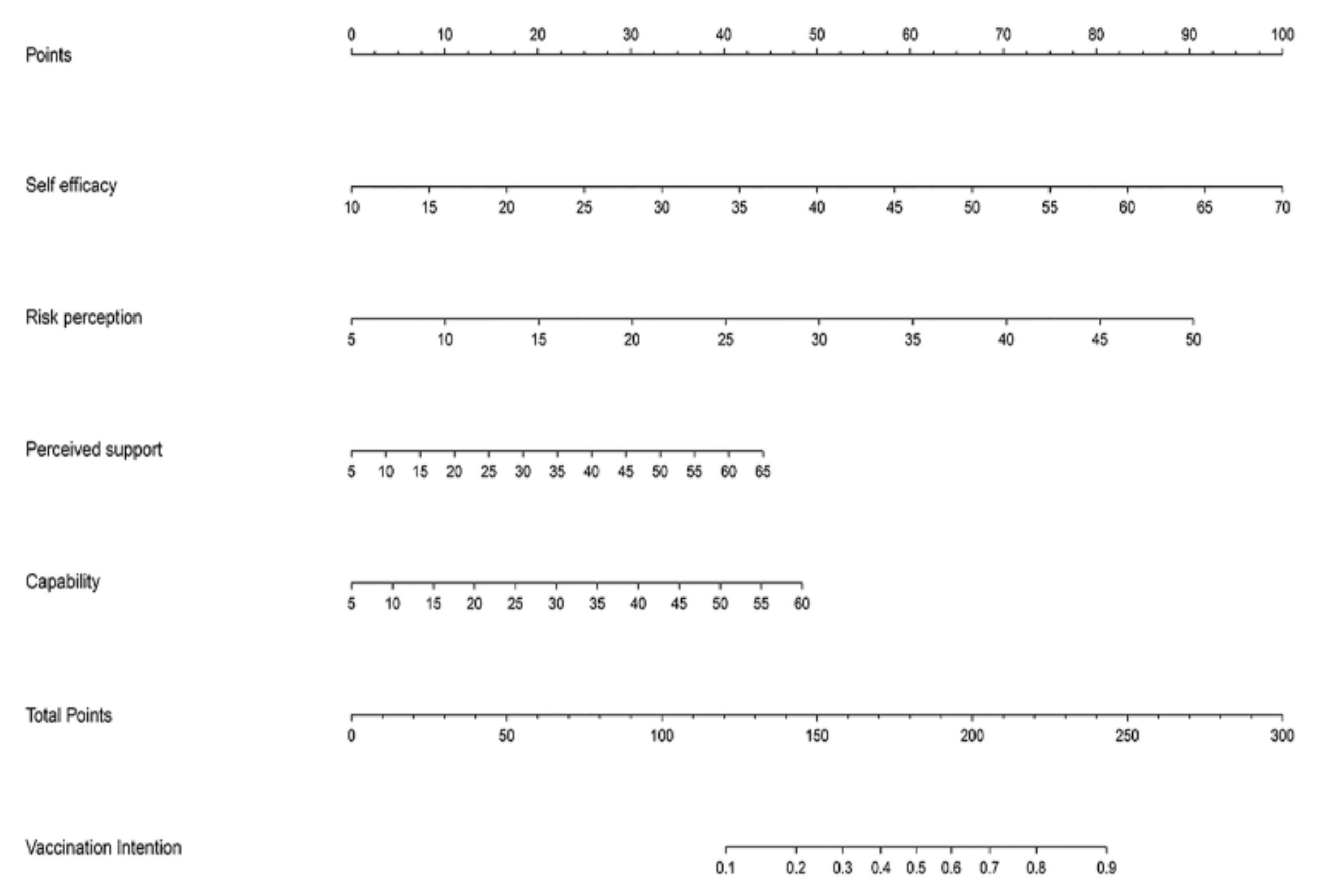
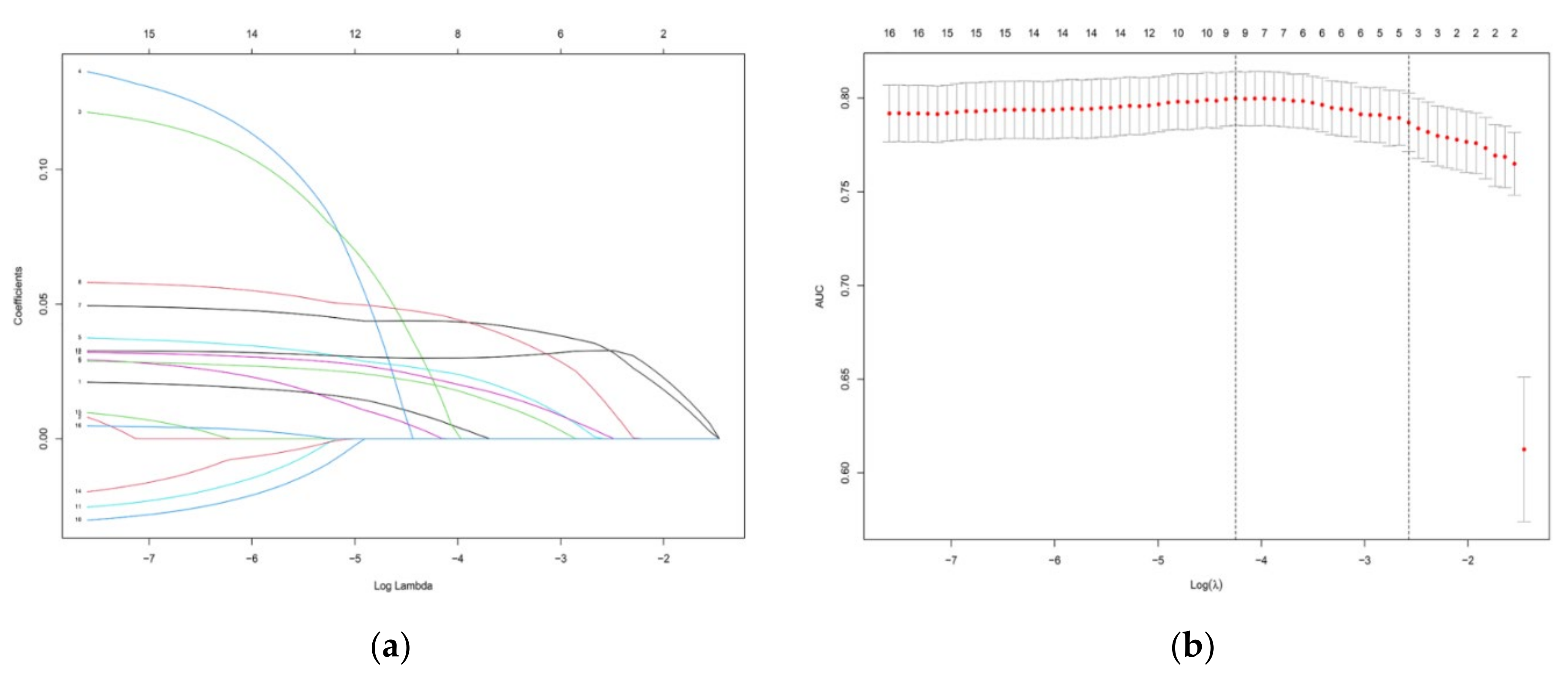
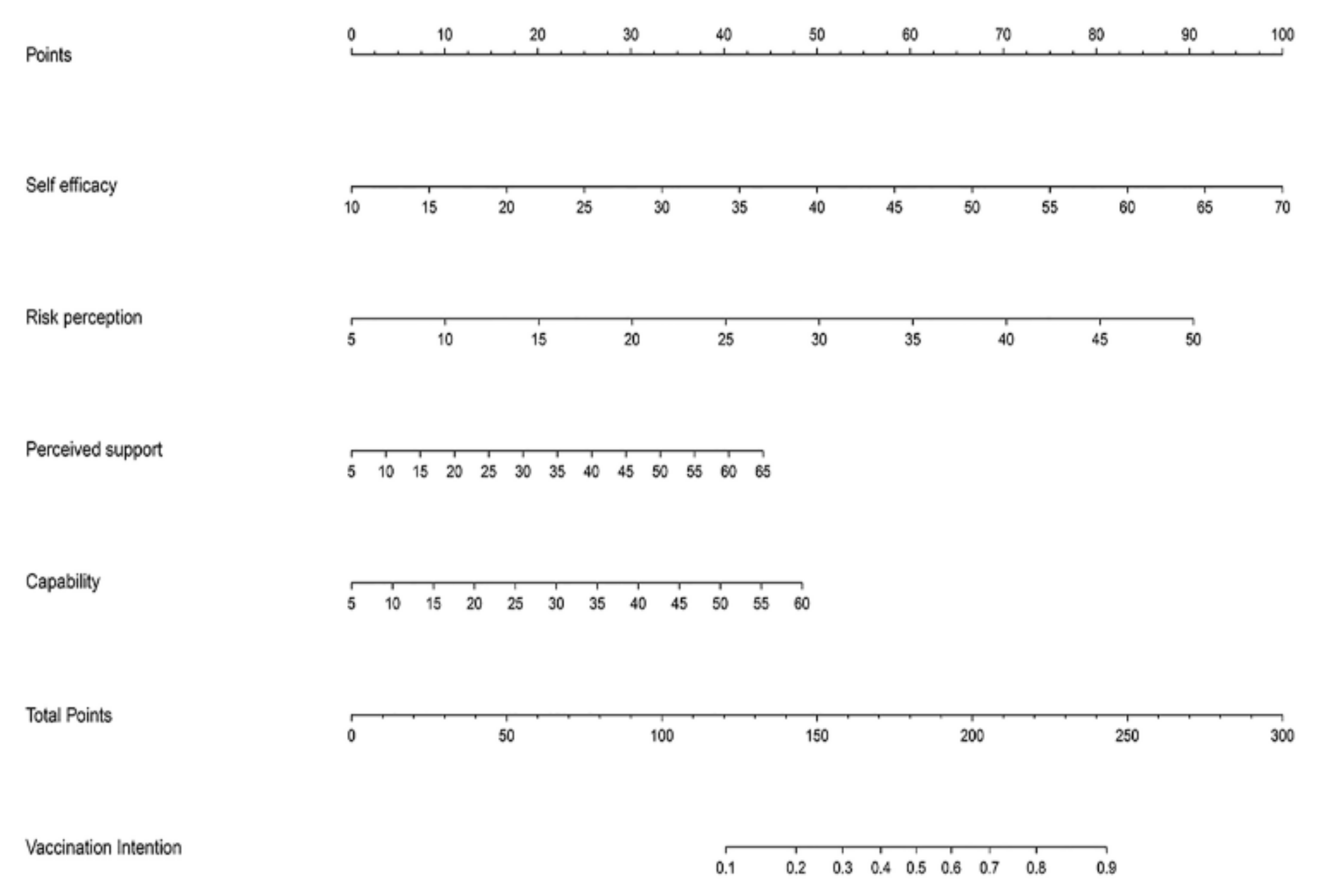
3.2. Predictive Model Construction
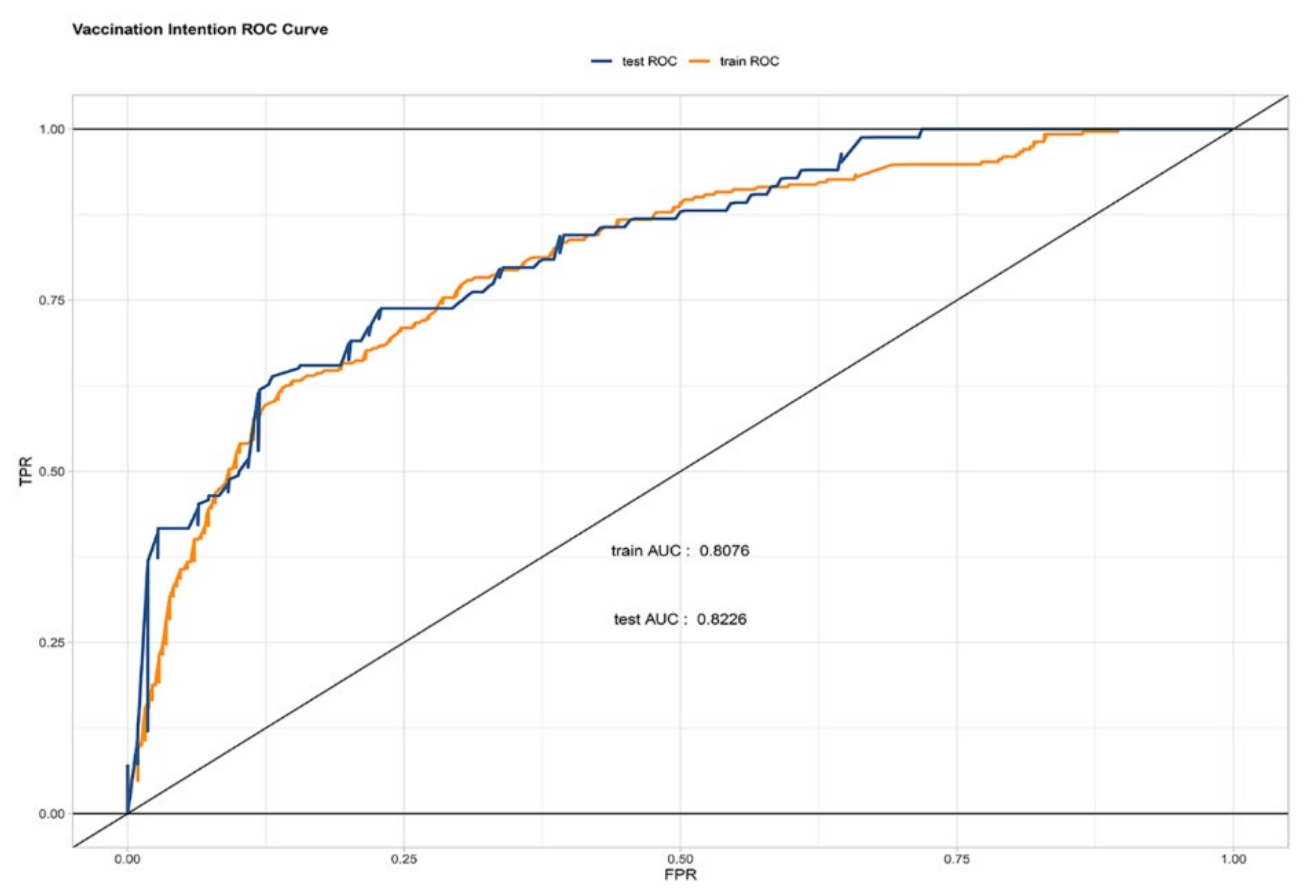
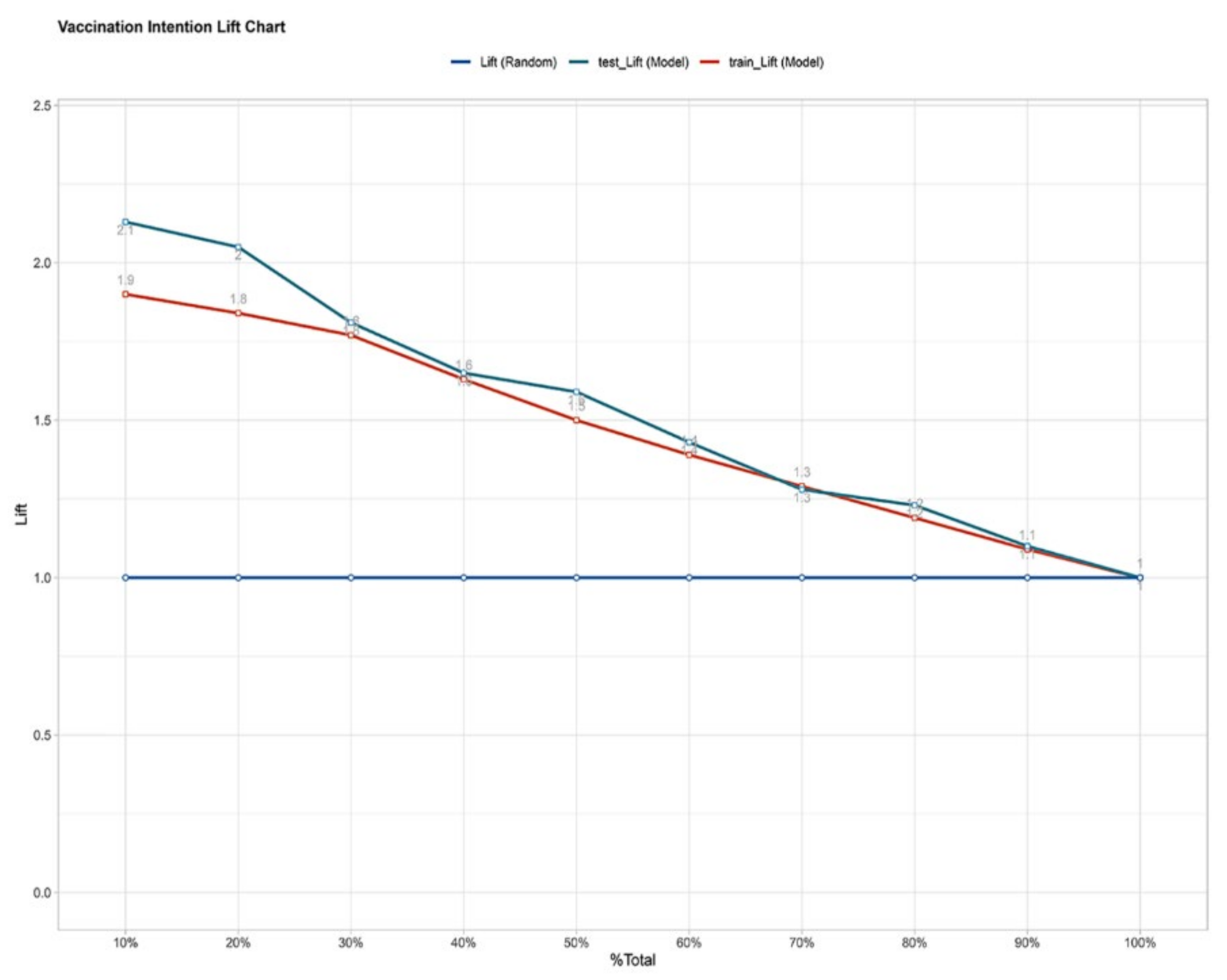
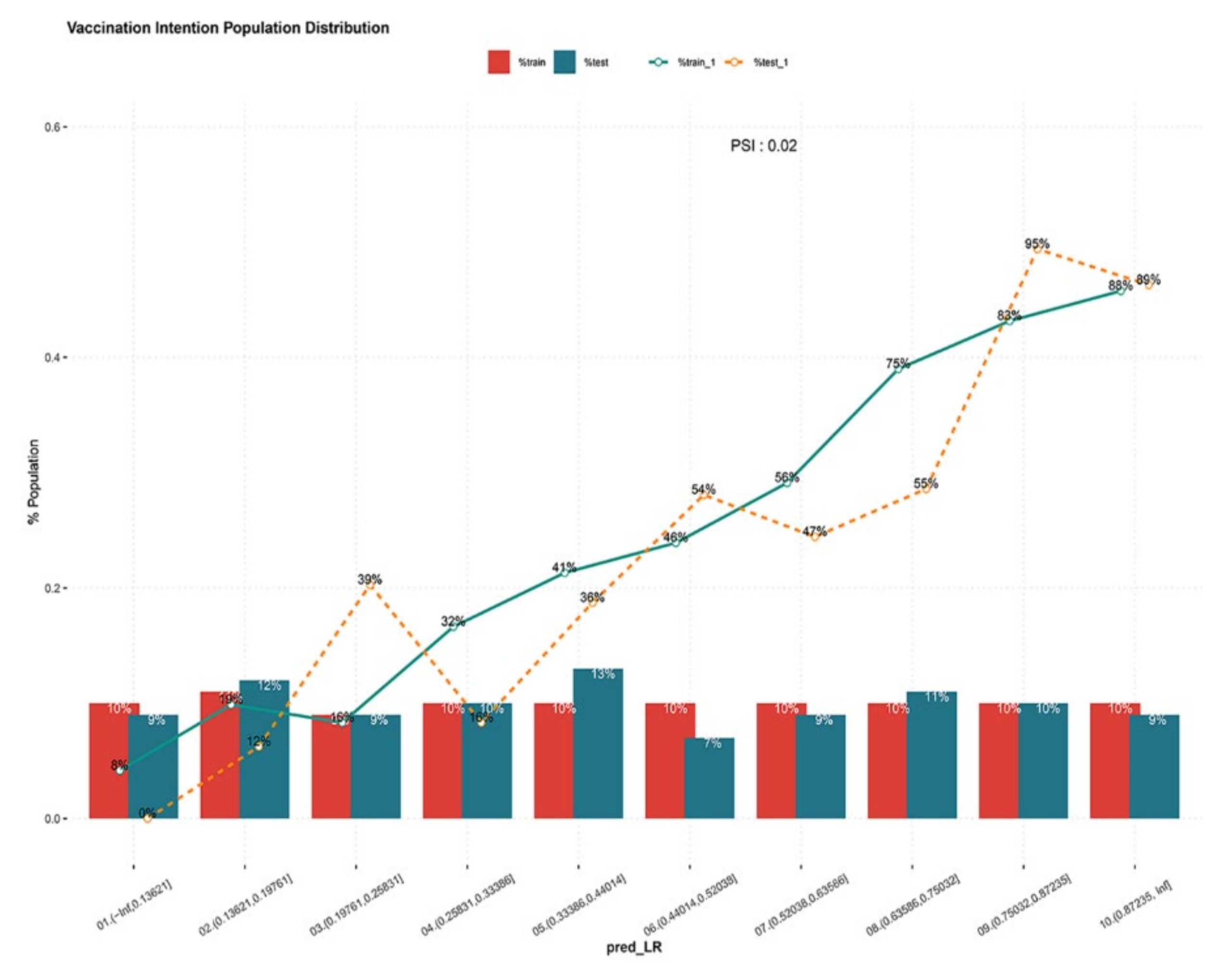
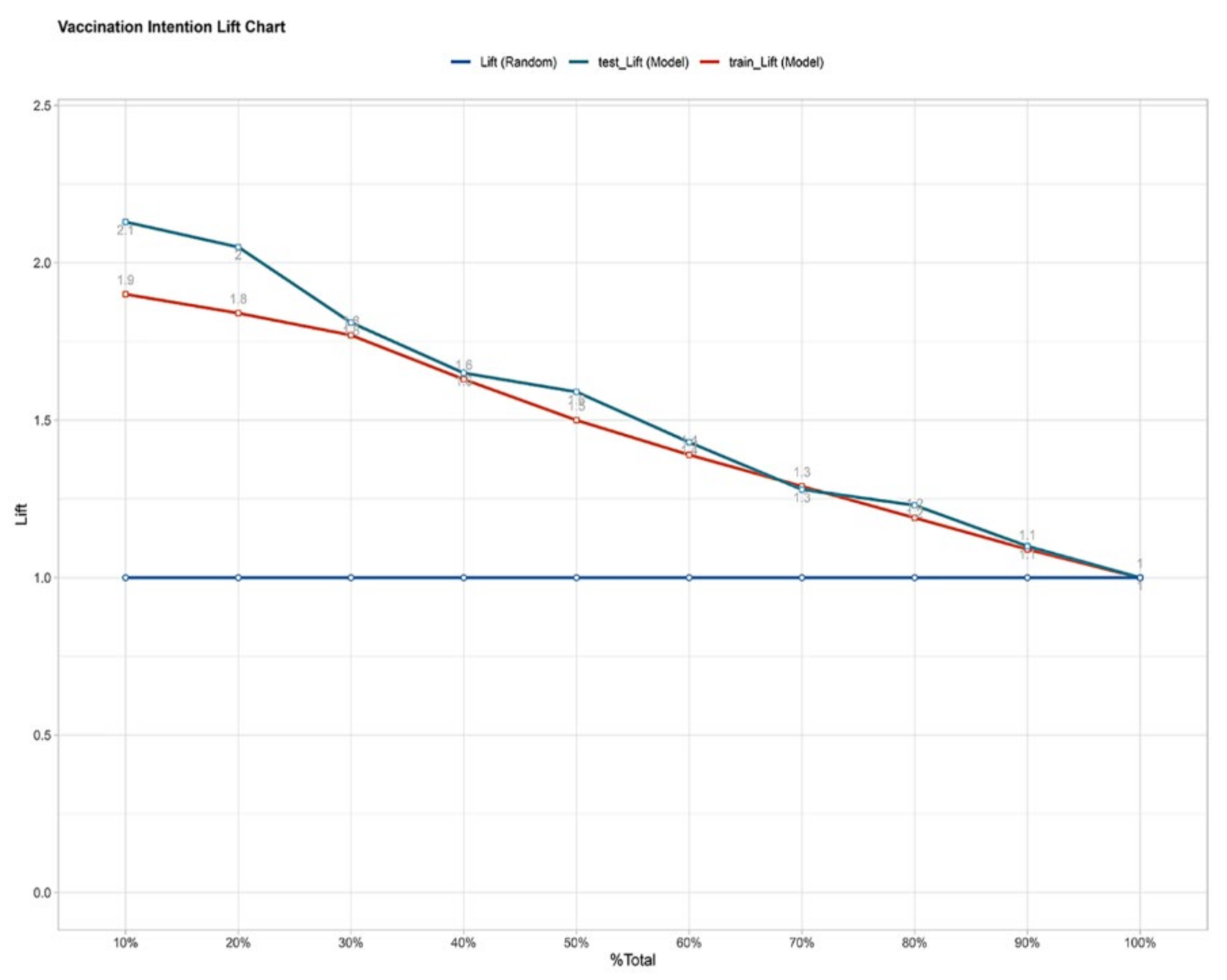
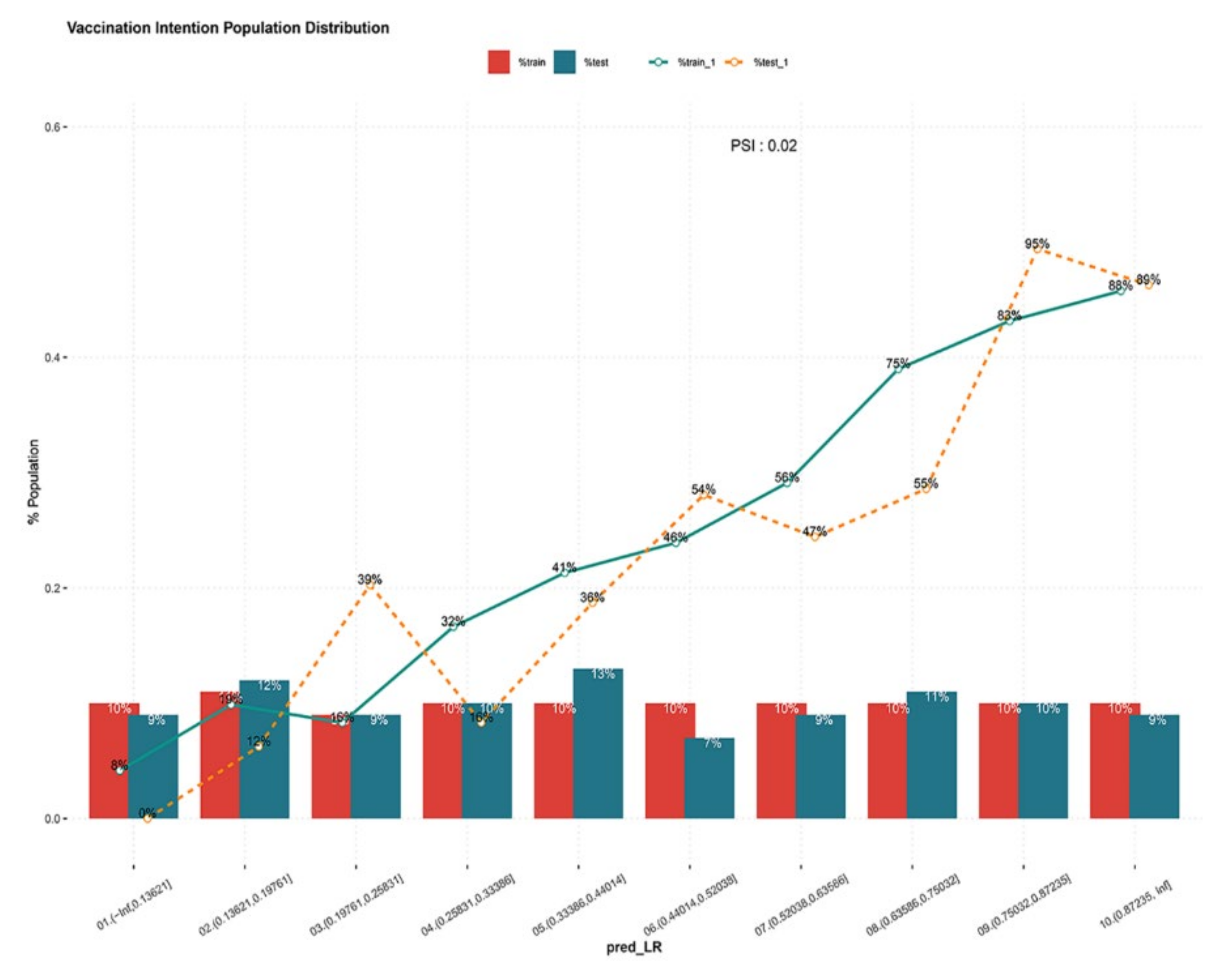
3.3. Prediction Model Validation
4. Discussion
4.1. Association of Mobile Population and Vaccination Intention
4.2. Association of Self-Efficacy and Vaccination Intention
4.3. Association of Risk Perception and Vaccination Intention
4.4. Association of Perceived Support and Vaccination Intention
4.5. Association of Capability and Vaccination Intention
4.6. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Word Health Organization. Coronavirus Disease (COVID-19) Weekly Epidemiological Update and Weekly Operational Update. 2021. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 1 October 2021).
- National Health Commission of the People’s Republic of China. COVID-19 Vaccination. 2021. Available online: http://www.nhc.gov.cn/xcs/yqjzqk/202104/70adf40602524305b66824bece1f298c.shtml (accessed on 1 October 2021).
- Guidry, J.P.D.; Laestadius, L.I.; Vraga, E.K.; Miller, C.A.; Perrin, P.B.; Burton, C.W.; Ryan, M.; Fuemmeler, B.F.; Carlyle, K.E. Willingness to get the COVID-19 vaccine with and without emergency use authorization. Am. J. Infect. Control. 2021, 49, 137–142. [Google Scholar] [CrossRef]
- Cherian, V.; Saini, N.K.; Sharma, A.K.; Philip, J. Prevalence and predictors of vaccine hesitancy in an urbanized agglomeration of New Delhi, India. J. Public Health 2021. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Hu, Z.; Zhao, Q.; Alias, H.; Danaee, M.; Wong, L.P. Understanding COVID-19 vaccine demand and hesitancy: A nationwide online survey in China. PLoS Negl. Trop. Dis. 2020, 14, e0008961. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Lu, X.; Lai, X.; Lyu, Y.; Zhang, H.; Fenghuang, Y.; Jing, R.; Li, L.; Yu, W.; Fang, H. The changing acceptance of COVID-19 vaccination in different epidemic phases in China: A longitudinal study. Vaccines 2021, 9, 191. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.; Zhang, Y.; Nicholas, S.; Leng, A.; Maitland, E.; Wang, J. COVID-19 Vaccination willingness among chinese adults under the free vaccination policy. Vaccines 2021, 9, 292. [Google Scholar] [CrossRef] [PubMed]
- Reiter, P.L.; Pennell, M.L.; Katz, M.L. Acceptability of a COVID-19 vaccine among adults in the United States: How many people would get vaccinated? Vaccine 2020, 38, 6500–6507. [Google Scholar] [CrossRef]
- Graffigna, G.; Palamenghi, L.; Boccia, S.; Barello, S. Relationship between citizens’ health engagement and intention to take the COVID-19 vaccine in Italy: A mediation analysis. Vaccines 2020, 8, 576. [Google Scholar] [CrossRef]
- Fishbein, M.; Ajzen, I. Predicting and Changing Behavior: The Reasoned Action Approach; Psychology Press: London, UK, 2010. [Google Scholar]
- Visser, O.; Hulscher, M.E.; Antonise-Kamp, L.; Akkermans, R.; van der Velden, K.; Ruiter, R.A.; Hautvast, J.L. Assessing determinants of the intention to accept a pertussis cocooning vaccination: A survey among healthcare workers in maternity and paediatric care. Vaccine 2018, 36, 736–743. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Q.-Z.; He, Y.-L.; Liu, H.; Miao, J.-M.; Chen, J.-X.; Xu, H.-N.; Wang, J.-Y. Reliability and validity of Chinese version of the Generalized Anxiety Disorder 7-item(GAD-7) scale in screening anxiety disorders in outpatients from traditional Chinese internal department. Chin. Ment. Health J. 2013, 27, 163–168. [Google Scholar]
- Min, B.; Zhou, A.; Liang, F. Clinical application of Patient Health Questionnaire for self-administered measurement (PHQ-9) as screening tool for depression. J. Neurosci. Ment. Health 2013, 6, 569–572. [Google Scholar]
- Li, X.-M.; Xin, T.-G.; Yuan, J.; Lv, L.-X.; Tao, J.-Y.; Liu, Y. Validity and reliability of the interpersonal needs questionnaire in Chinese college students. Chin. J. Clin. Psychol. 2015, 23, 590–593. [Google Scholar]
- Wouters, O.J.; Shadlen, K.C.; Salcher-Konrad, M.; Pollard, A.J.; Larson, H.J.; Teerawattananon, Y.; Jit, M. Challenges in ensuring global access to COVID-19 vaccines: Production, affordability, allocation, and deployment. Lancet 2021, 397, 1023–1034. [Google Scholar] [CrossRef]
- Dong, D.; Xu, R.H.; Wong, E.L.; Hung, C.; Feng, D.; Feng, Z.; Yeoh, E.; Wong, S.Y. Public preference for COVID-19 vaccines in China: A discrete choice experiment. Health Expect 2020, 23, 1543–1578. [Google Scholar] [CrossRef] [PubMed]
- Alabdulla, M.; Reagu, S.M.; Al-Khal, A.; Elzain, M.; Jones, R.M. COVID-19 vaccine hesitancy and attitudes in Qatar: A national cross-sectional survey of a migrant-majority population. Influenza Other Respir. Viruses 2021, 15, 361–370. [Google Scholar] [CrossRef]
- Crawshaw, A.F.; Deal, A.; Rustage, K.; Forster, A.S.; Campos-Matos, I.; Vandrevala, T.; Würz, A.; Pharris, A.; Suk, J.E.; Kinsman, J.; et al. What must be done to tackle vaccine hesitancy and barriers to COVID-19 vaccination in migrants? J. Travel Med. 2021, 28, taab048. [Google Scholar] [CrossRef]
- Funk, C.; Laferrière, C.; Ardakani, A. Target product profile analysis of COVID-19 vaccines in phase III clinical trials and beyond: An early 2021 perspective. Viruses 2021, 13, 418. [Google Scholar] [CrossRef]
- DeStefano, F.; Shimabukuro, T.T. The MMR vaccine and autism. Annu. Rev. Virol. 2019, 6, 585–600. [Google Scholar] [CrossRef]
- Sekine, M.; Kudo, R.; Yamaguchi, M.; Hanley, S.J.B.; Hara, M.; Adachi, S.; Ueda, Y.; Miyagi, E.; Ikeda, S.; Yagi, A.; et al. Japan’s ongoing crisis on HPV vaccination. Vaccines 2020, 8, 362. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, B.; et al. Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Coustasse, A.; Kimble, C.; Maxik, K. COVID-19 and vaccine hesitancy: A challenge the United States must overcome. J. Ambul. Care Manag. 2021, 44, 71–75. [Google Scholar] [CrossRef]
- National Health Commission of the People’s Republic of China. Guideline for COVID-19 Vaccination, 1st ed. 2021. Available online: http://www.nhc.gov.cn/xcs/yqfkdt/202103/c2febfd04fc5498f916b1be080905771.shtml (accessed on 1 October 2021).
- Larson, H.J.; Jarrett, C.; Schulz, W.S.; Chaudhuri, M.; Zhou, Y.; Dubé, E.; Schuster, M.; MacDonald, N.E.; Wilson, R. Measuring vaccine hesitancy: The development of a survey tool. Vaccine 2015, 33, 4165–4175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puri, N.; Coomes, E.A.; Haghbayan, H.; Gunaratne, K. Social media and vaccine hesitancy: New updates for the era of COVID-19 and globalized infectious diseases. Hum. Vaccines Immunother. 2020, 16, 2586–2593. [Google Scholar] [CrossRef] [PubMed]
- Corace, K.M.; Srigley, J.A.; Hargadon, D.; Yu, D.; MacDonald, T.K.; Fabrigar, L.R.; Garber, G.E. Using behavior change frameworks to improve healthcare worker influenza vaccination rates: A systematic review. Vaccine 2016, 34, 3235–3242. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Determinants | Determinants Measured | Number of Items |
|---|---|---|
| Personal determinants | Demographic characteristics | 4 |
| Psychosocial determinants | ||
| Depression | 9 | |
| Anxiety | 7 | |
| Interpersonal need | 15 | |
| Behavioral determinants | ||
| General view on vaccination | General beliefs about vaccination | 4 |
| Past experience | 3 | |
| Views on COVID-19 vaccination | Self-efficacy | 10 |
| Risk perception | 6 | |
| Fear of vaccination | 5 | |
| Perceived benefits | 4 | |
| Perceived barriers | 2 | |
| Perceived support | Perceived support | 9 |
| Capability | Capability | 8 |
| Intention | Intention | 1 |
| Items | Total (n = 782) | Training Set | Testing Set | p-Value |
|---|---|---|---|---|
| (n = 588) | (n = 194) | |||
| Age (years old) | 32 (28,38) | 32 (28,38) | 33 (28,39) | 0.681 |
| Sex, n (%) | 0.993 | |||
| Male | 363 (46.4) | 273 (46.4) | 90 (46.4) | |
| Female | 419 (53.6) | 315 (53.6) | 104 (53.6) | |
| Education, n (%) | 0.533 | |||
| Junior middle school and below | 48 (6.1) | 34 (5.8) | 14 (7.2) | |
| High school | 224 (28.6) | 175 (29.8) | 49 (25.3) | |
| Junior college | 209 (26.7) | 161 (27.4) | 48 (24.7) | |
| Undergraduate | 238 (30.4) | 172 (29.3) | 66 (34.0) | |
| Postgraduate and above | 63 (8.1) | 46 (7.8) | 17 (8.8) | |
| Income | 0.999 | |||
| Extremely high | 8 (1.0) | 6 (1.0) | 2 (1.0) | |
| High | 48 (6.1) | 36 (6.1) | 12 (6.2) | |
| Middle | 575 (73.5) | 431 (73.3) | 144 (74.2) | |
| Low | 122 (15.6) | 93 (15.8) | 29 (14.9) | |
| Extremely low | 29 (3.7) | 22 (3.75) | 7 (3.6) | |
| Anxiety | 9 (7,14) | 9 (7,14) | 9 (7,14) | 0.748 |
| Depression | 12 (9,18) | 12 (9,18) | 13 (9,18) | 0.538 |
| Interpersonal need | 37 (25,51) | 37 (25,51) | 35 (25,50) | 0.263 |
| General beliefs | 22 (18,26) | 22 (18,26) | 22 (18,26) | 0.796 |
| Past experience | 14 (11,15) | 14 (11,15) | 14 (12,15) | 0.231 |
| Self-efficacy | 51 (41,60) | 51 (42,60) | 51 (40,60) | 0.941 |
| Risk perception | 30 (26,35) | 30 (26,35) | 30 (26,35) | 0.694 |
| Fear of vaccination | 18 (15,24) | 18 (15,24) | 19 (15,24) | 0.605 |
| Perceived benefits | 25 (21,28) | 25 (21,28) | 24.5 (21,28) | 0.696 |
| Perceived barriers | 7 (5,9) | 7 (6,9) | 7 (5,9) | 0.319 |
| Perceived support | 38 (34,49) | 38 (35,50) | 37 (32,47) | 0.274 |
| Capability | 40.5 (32,50) | 40 (32,50) | 42 (33,50) | 0.492 |
| Determinants | β-Coefficient | p-Value | OR (95% CI) |
|---|---|---|---|
| Self-efficacy | 0.060 | <0.001 a | 1.062 (1.030–1.095) |
| Risk perception | 0.072 | <0.001 a | 1.075 (1.046–1.105) |
| Perceived support | 0.026 | 0.033 a | 1.027 (1.002–1.052) |
| Capability | 0.032 | 0.073 | 1.032 (0.997–1.068) |
| PSI | Test_Lift | Train_Lift | Test_K-S | Train_K-S | %Test_cumB | %Test_cumG | %Train_cumB | %Train_cumG | %Test_B | %Train_B | %Test | %Train | #Test | #Train | #Total |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0 | 1 | 1 | 0.16 | 0.15 | 0 | 0.16 | 0.02 | 0.17 | 0 | 0.08 | 0.09 | 0.1 | 18 | 59 | 77 |
| 0 | 1.1 | 1.09 | 0.32 | 0.28 | 0.04 | 0.35 | 0.07 | 0.34 | 0.12 | 0.19 | 0.12 | 0.11 | 24 | 67 | 91 |
| 0 | 1.23 | 1.19 | 0.34 | 0.38 | 0.12 | 0.45 | 0.1 | 0.48 | 0.39 | 0.16 | 0.09 | 0.09 | 18 | 51 | 69 |
| 0 | 1.28 | 1.29 | 0.45 | 0.44 | 0.15 | 0.6 | 0.17 | 0.6 | 0.16 | 0.32 | 0.1 | 0.1 | 19 | 59 | 78 |
| 0.01 | 1.43 | 1.39 | 0.48 | 0.46 | 0.26 | 0.75 | 0.25 | 0.72 | 0.36 | 0.41 | 0.13 | 0.1 | 25 | 59 | 84 |
| 0.01 | 1.59 | 1.5 | 0.45 | 0.46 | 0.35 | 0.8 | 0.35 | 0.82 | 0.54 | 0.46 | 0.07 | 0.1 | 0.13 | 59 | 72 |
| 0 | 1.65 | 1.63 | 0.44 | 0.42 | 0.44 | 0.88 | 0.47 | 0.9 | 0.47 | 0.56 | 0.09 | 0.1 | 17 | 59 | 76 |
| 0 | 1.81 | 1.33 | 0.39 | 0.31 | 0.58 | 0.97 | 0.64 | 0.95 | 0.55 | 0.75 | 0.11 | 0.1 | 22 | 59 | 81 |
| 0 | 2.05 | 1.84 | 0.17 | 0.16 | 0.81 | 0.98 | 0.82 | 0.98 | 0.95 | 0.83 | 0.1 | 0.1 | 20 | 59 | 79 |
| 0 | 2.13 | 1.9 | 0 | 0 | 1 | 1 | 1 | 1 | 0.89 | 0.88 | 0.09 | 0.1 | 18 | 57 | 75 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, F.; Gong, R.; Chen, Y.; Zhang, J.; Hu, T.; Chen, Y.; Zhang, K.; Shang, M.; Cai, Y. Prediction Model for COVID-19 Vaccination Intention among the Mobile Population in China: Validation and Stability. Vaccines 2021, 9, 1221. https://doi.org/10.3390/vaccines9111221
Hu F, Gong R, Chen Y, Zhang J, Hu T, Chen Y, Zhang K, Shang M, Cai Y. Prediction Model for COVID-19 Vaccination Intention among the Mobile Population in China: Validation and Stability. Vaccines. 2021; 9(11):1221. https://doi.org/10.3390/vaccines9111221
Chicago/Turabian StyleHu, Fan, Ruijie Gong, Yexin Chen, Jinxin Zhang, Tian Hu, Yaqi Chen, Kechun Zhang, Meili Shang, and Yong Cai. 2021. "Prediction Model for COVID-19 Vaccination Intention among the Mobile Population in China: Validation and Stability" Vaccines 9, no. 11: 1221. https://doi.org/10.3390/vaccines9111221
APA StyleHu, F., Gong, R., Chen, Y., Zhang, J., Hu, T., Chen, Y., Zhang, K., Shang, M., & Cai, Y. (2021). Prediction Model for COVID-19 Vaccination Intention among the Mobile Population in China: Validation and Stability. Vaccines, 9(11), 1221. https://doi.org/10.3390/vaccines9111221