
Association between Adult Vaccine Hesitancy and Parental Acceptance of Childhood COVID-19 Vaccines: A Web-Based Survey in a Northwestern Region in China



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Demographics
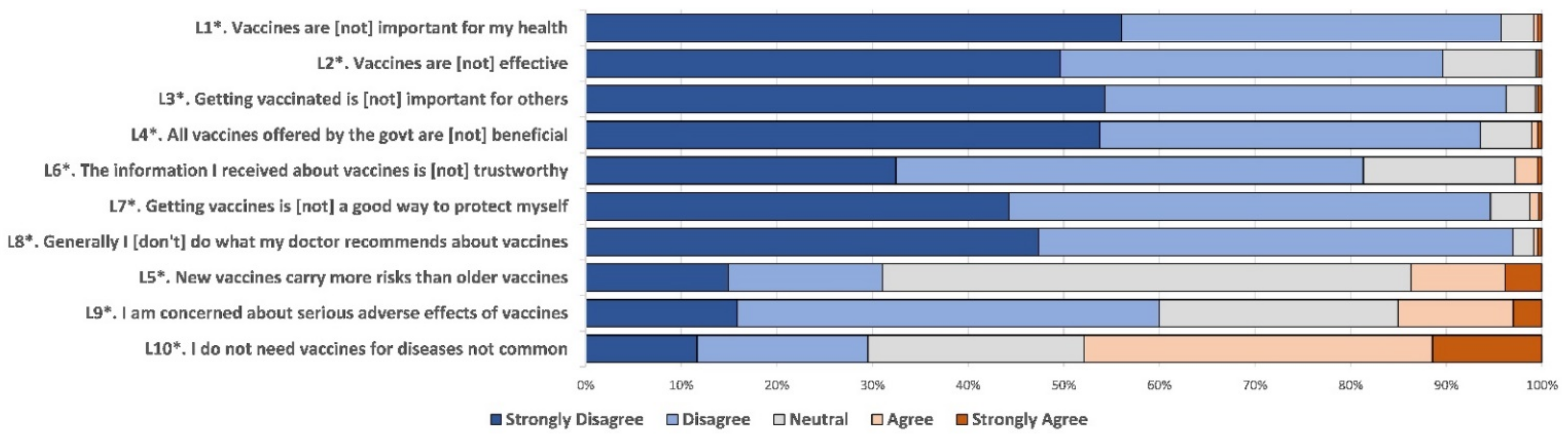
2.3. Adult Vaccine Hesitancy
2.4. COVID-19 Vaccination Behavior and Intent
2.5. History of Childhood Immunization and Pediatric Infectious Diseases
2.6. Discrete Choice Experiment (DCE)
2.7. Heat Map
2.8. Statistical Analysis
3. Results
3.1. Characteristics of Respondents
3.2. Adult Vaccine Hesitancy and COVID-19 Vaccination
3.3. Vaccination of Four Childhood Vaccines and Parental Acceptance of Childhood COVID-19 Vaccines
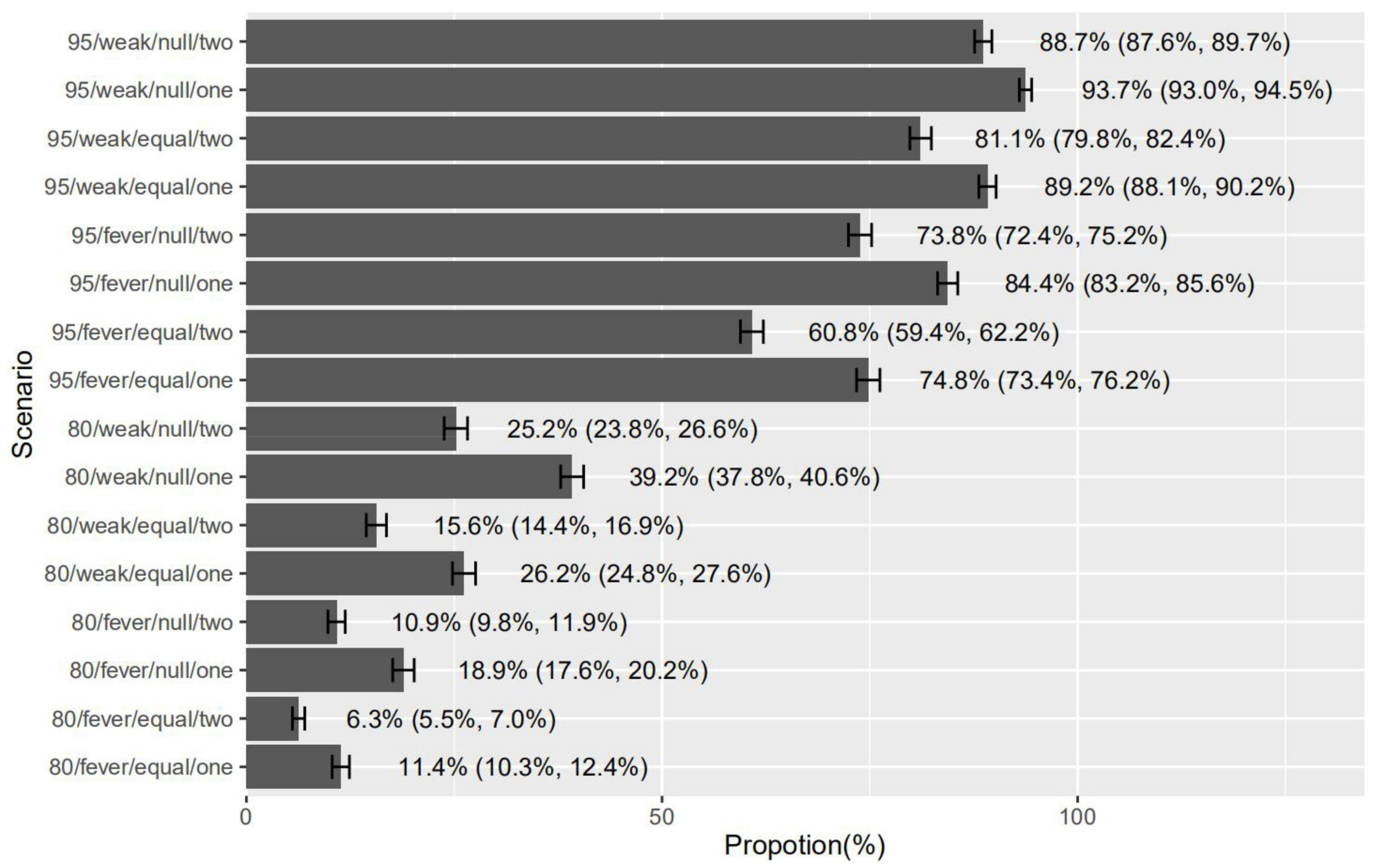
3.4. Parental Preferences for Childhood COVID-19 Vaccines
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- MacDonald, N.E.; SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Dubé, E.; Gagnon, D.; MacDonald, N.; Bocquier, A.; Peretti-Watel, P.; Verger, P. Underlying factors impacting vaccine hesitancy in high income countries: A review of qualitative studies. Expert Rev. Vaccines 2018, 17, 989–1004. [Google Scholar] [CrossRef] [PubMed]
- Simas, C.; Larson, H.J. Overcoming vaccine hesitancy in low-income and middle-income regions. Nat. Rev. Dis. Primers 2021, 7, 41. [Google Scholar] [CrossRef]
- Quinn, S.C.; Jamison, A.M.; An, J.; Hancock, G.R.; Freimuth, V.S. Measuring vaccine hesitancy, confidence, trust and flu vaccine uptake: Results of a national survey of White and African American adults. Vaccine 2019, 37, 1168–1173. [Google Scholar] [CrossRef]
- Mereckiene, J.; Cotter, S.; Nicoll, A.; Lévy-Bruhl, D.; Ferro, A.; Tridente, G.; Zanoni, G.; Berra, P.; Salmaso, S.; O’Flanagan, D.; et al. National seasonal influenza vaccination survey in Europe, 2008. Eurosurveillance 2008, 13, 19017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yan, S.; Wang, Y.; Zhu, W.; Zhang, L.; Gu, H.; Liu, D.; Zhu, A.; Xu, H.; Hao, L.; Ye, C. Barriers to influenza vaccination among different populations in Shanghai. Hum. Vaccines Immunother. 2021, 17, 1403–1411. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Xu, Y.; Wang, J.; Che, X.; Gu, W.; Du, J.; Zhang, X.; Zhang, X.; Jiang, W.; Chen, J.; et al. Vaccination pattern of the 23-valent pneumococcal polysaccharide vaccine (PPV23) in Hangzhou, China: A coverage and adverse events following immunization of different age groups. Hum. Vaccines Immunother. 2021, 17, 157–161. [Google Scholar] [CrossRef]
- Ghinai, I.; Willott, C.; Dadari, I.; Larson, H.J. Listening to the rumours: What the northern Nigeria polio vaccine boycott can tell us ten years on. Glob. Public Health 2013, 8, 1138–1150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hviid, A.; Hansen, J.V.; Frisch, M.; Melbye, M. Measles, Mumps, Rubella Vaccination and Autism: A Nationwide Cohort Study. Ann. Intern. Med. 2019, 170, 513–520. [Google Scholar] [CrossRef] [Green Version]
- Phadke, V.K.; Bednarczyk, R.A.; Salmon, D.A.; Omer, S.B. Association Between Vaccine Refusal and Vaccine-Preventable Diseases in the United States: A Review of Measles and Pertussis. JAMA 2016, 315, 1149–1158. [Google Scholar] [CrossRef] [Green Version]
- Our World in Data. Coronavirus (COVID-19) Vaccinations. Available online: http://www.ourworldindata.org/covid-vaccinations (accessed on 8 April 2021).
- Haas, E.J.; Angulo, F.J.; McLaughlin, J.M.; Anis, E.; Singer, S.R.; Khan, F.; Brooks, N.; Smaja, M.; Mircus, G.; Pan, K.; et al. Impact and effectiveness of mRNA BNT162b2 vaccine against SARS-CoV-2 infections and COVID-19 cases, hospitalisations, and deaths following a nationwide vaccination campaign in Israel: An observational study using national surveillance data. Lancet 2021, 397, 1819–1829. [Google Scholar] [CrossRef]
- Dror, A.A.; Eisenbach, N.; Taiber, S.; Morozov, N.G.; Mizrachi, M.; Zigron, A.; Srouji, S.; Sela, E. Vaccine hesitancy: The next challenge in the fight against COVID-19. Eur. J. Epidemiol. 2020, 35, 775–779. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2021, 27, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Xu, W.; Dozier, M.; He, Y.; Kirolos, A.; Lang, Z.; Song, P.; Theodoratou, E. The role of children in the transmission of SARS-CoV2: Updated rapid review. J. Glob. Health 2020, 10, 021101. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; Wen, X.; Guo, Q.; Ji, M.; Zhang, F.; Wagner, A.; Lu, Y. Sensitivity to COVID-19 Vaccine Effectiveness and Safety in Shanghai, China. Vaccines 2021, 9, 472. [Google Scholar] [CrossRef] [PubMed]
- Wenjuanxing (Questionnaire Star). Available online: https://www.wjx.cn (accessed on 20 July 2021).
- Akel, K.B.; Masters, N.B.; Shih, S.F.; Lu, Y.; Wagner, A.L. Modification of a vaccine hesitancy scale for use in adult vaccinations in the United States and China. Hum. Vaccines Immunother. 2021, 1–8. [Google Scholar] [CrossRef]
- Creech, C.B.; Walker, S.C.; Samuels, R.J. SARS-CoV-2 Vaccines. JAMA 2021, 325, 1318–1320. [Google Scholar] [CrossRef]
- Johnson, F.R.; Lancsar, E.; Marshall, D.; Kilambi, V.; Mühlbacher, A.; Regier, D.; Bresnahan, B.W.; Kanninen, B.; Bridges, J.F. Constructing experimental designs for discrete-choice experiments: Report of the ISPOR Conjoint Analysis Experimental Design Good Research Practices Task Force. Value Health 2013, 16, 3–13. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.; Guo, W.; Perez, C. Social Support and Life Satisfaction of Ethnic Minority Elderly in China. Int. J. Aging Hum. Dev. 2021, 92, 301–321. [Google Scholar] [CrossRef]
- Smith, L.E.; Amlôt, R.; Weinman, J.; Yiend, J.; Rubin, G.J. A systematic review of factors affecting vaccine uptake in young children. Vaccine 2017, 35, 6059–6069. [Google Scholar] [CrossRef] [Green Version]
- Chung, Y.; Schamel, J.; Fisher, A.; Frew, P.M. Influences on Immunization Decision-Making among US Parents of Young Children. Matern. Child Health J. 2017, 21, 2178–2187. [Google Scholar] [CrossRef]
- Wang, Q.; Xiu, S.; Zhao, S.; Wang, J.; Han, Y.; Dong, S.; Huang, J.; Cui, T.; Yang, L.; Shi, N.; et al. Vaccine Hesitancy: COVID-19 and Influenza Vaccine Willingness among Parents in Wuxi, China-A Cross-Sectional Study. Vaccines 2021, 9, 342. [Google Scholar] [CrossRef] [PubMed]
- Larson, H.J.; Jarrett, C.; Eckersberger, E.; Smith, D.M.; Paterson, P. Understanding vaccine hesitancy around vaccines and vaccination from a global perspective: A systematic review of published literature, 2007–2012. Vaccine 2014, 32, 2150–2159. [Google Scholar] [CrossRef] [PubMed]
- Wagner, A.L.; Masters, N.B.; Domek, G.J.; Mathew, J.L.; Sun, X.; Asturias, E.J.; Ren, J.; Huang, Z.; Contreras-Roldan, I.L.; Gebremeskel, B.; et al. Comparisons of Vaccine Hesitancy across Five Low- and Middle-Income Countries. Vaccines 2019, 7, 155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Martino, G.; Di Giovanni, P.; Di Girolamo, A.; Scampoli, P.; Cedrone, F.; D’Addezio, M.; Meo, F.; Romano, F.; Di Sciascio, M.B.; Staniscia, T. Knowledge and Attitude towards Vaccination among Healthcare Workers: A Multicenter Cross-Sectional Study in a Southern Italian Region. Vaccines 2020, 8, 248. [Google Scholar] [CrossRef]
- Yaqub, O.; Castle-Clarke, S.; Sevdalis, N.; Chataway, J. Attitudes to vaccination: A critical review. Soc. Sci. Med. 2014, 112, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Khubchandani, J.; Sharma, S.; Price, J.H.; Wiblishauser, M.J.; Sharma, M.; Webb, F.J. COVID-19 Vaccination Hesitancy in the United States: A Rapid National Assessment. J. Community Health 2021, 46, 270–277. [Google Scholar] [CrossRef]
- Han, B.; Song, Y.; Li, C.; Yang, W.; Ma, Q.; Jiang, Z.; Li, M.; Lian, X.; Jiao, W.; Wang, L.; et al. Safety, tolerability, and immunogenicity of an inactivated SARS-CoV-2 vaccine (CoronaVac) in healthy children and adolescents: A double-blind, randomised, controlled, phase 1/2 clinical trial. Lancet Infect. Dis. 2021, 21, 181–192. [Google Scholar] [CrossRef]
- Gidengil, C.; Chen, C.; Parker, A.M.; Nowak, S.; Matthews, L. Beliefs around childhood vaccines in the United States: A systematic review. Vaccine. 2019, 37, 6793–6802. [Google Scholar] [CrossRef]
- Bell, S.; Clarke, R.; Mounier-Jack, S.; Walker, J.L.; Paterson, P. Parents’ and guardians’ views on the acceptability of a future COVID-19 vaccine: A multi-methods study in England. Vaccine 2020, 38, 7789–7798. [Google Scholar] [CrossRef]
- Gust, D.A.; Darling, N.; Kennedy, A.; Schwartz, B. Parents with doubts about vaccines: Which vaccines and reasons why. Pediatrics 2008, 122, 718–725. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Already Vaccinated with COVID-19 Vaccines (%) | Intend to Vaccinate COVID-19 Vaccines (%) | Not Intend to Vaccinate COVID-19 Vaccines (%) | p Value | |
|---|---|---|---|---|
| Respondents’ age (years) | <0.001 | |||
| 20–29 | 1025 (60.8) | 489 (29.0) | 172 (10.2) | |
| 30–39 | 5213 (66.6) | 2018 (25.8) | 593 (7.6) | |
| 40–49 | 2657 (67.4) | 1066 (27.0) | 218 (5.5) | |
| Respondents’ sex | <0.001 | |||
| Male | 3202 (65.4) | 1414 (28.9) | 282 (5.8) | |
| Female | 5693 (66.6) | 2159 (25.2) | 701 (8.2) | |
| Children’s age (years) | <0.001 | |||
| 0–5 | 3388 (74.6) | 938 (20.7) | 216 (4.8) | |
| 6–10 | 3106 (64.3) | 1363 (28.2) | 361 (7.5) | |
| 11–18 | 2400 (58.9) | 1172 (28.7) | 505 (12.4) | |
| Number of children | <0.001 | |||
| Single | 3306 (69.5) | 1097 (23.1) | 353 (7.4) | |
| Two or more | 5589 (64.3) | 2476 (28.5) | 630 (7.2) | |
| Ethnicity | <0.001 | |||
| Han Chinese | 6456 (70.1) | 2204 (23.9) | 551 (6.0) | |
| Minority Chinese | 2439 (57.5) | 1369 (32.3) | 432 (10.2) | |
| Educational level | <0.001 | |||
| Middle school or below | 3973 (58.0) | 2286 (33.4) | 593 (8.7) | |
| High school | 1865 (67.6) | 713 (25.8) | 182 (6.6) | |
| College and university | 3057 (79.6) | 574 (15.0) | 208 (5.4) | |
| Registered residence | <0.001 | |||
| In urban areas | 3975 (74.8) | 1013 (19.1) | 327 (6.2) | |
| In rural areas | 4920 (60.5) | 2560 (31.5) | 656 (8.1) | |
| Monthly family income, CNY | <0.001 | |||
| <5000 | 3392 (60.0) | 1763 (31.2) | 500 (8.8) | |
| 5000–7499 | 2354 (67.2) | 924 (26.4) | 226 (6.4) | |
| ≥7500 | 3149 (73.4) | 886 (20.6) | 257 (6.0) | |
| Adult vaccine hesitancy | <0.001 | |||
| Mean ± SD | 20.50 ± 4.33 | 21.21 ± 4.17 | 23.78 ± 4.39 |
| Odds Ratio (OR) Value (95% CI) | ||||||
|---|---|---|---|---|---|---|
| Number of Respondents | Pneumonia Vaccine | Influenza Vaccine | Rotavirus Vaccine | EV-71 Vaccine | Intent to Accept Child COVID-19 Vaccine | |
| Children’s age (years) | ||||||
| 0–5 | 4542 | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 |
| 6–10 | 4830 | 2.5 (2.1, 2.9) * | 1.9 (1.7, 2.2) * | 3.2 (2.7, 3.9) * | 2.9 (2.4, 3.6) * | 0.2 (0.1, 0.2) * |
| 11–18 | 4079 | 1.8 (1.6, 2.1) * | 1.6 (1.4, 1.8) * | 1.9 (1.6, 2.2) * | 1.6 (1.3, 2.0) * | 0.3 (0.3, 0.3) * |
| Respondents’ age (years) | ||||||
| 20–29 | 1686 | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 |
| 30–39 | 7824 | 1.0 (0.8, 2.0) | 0.9 (0.8, 1.1) | 1.2 (0.9, 1.5) | 1.1 (0.8, 1.4) | 1.0 (0.9, 1.2) |
| 40–49 | 3941 | 1.0 (0.9, 1.2) | 1.1 (0.9, 1.1) | 1.2 (0.9, 1.4) | 1.2 (0.9, 1.4) | 0.9 (0.8, 1.0) |
| Number of children | ||||||
| Single | 4756 | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 |
| Two or more | 8695 | 1.1 (0.9, 1.2) | 1.0 (0.9, 1.1) | 1.2 (1.1, 1.4) * | 1.3 (1.2, 1.5) * | 0.9 (0.9, 1.0) |
| Ethnicity | ||||||
| Han Chinese | 9211 | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 |
| Minority Chinese | 4240 | 1.2 (1.1, 1.4) * | 1.3 (1.2, 1.4) * | 1.3 (1.2, 1.5) * | 1.2 (1.0, 1.4) * | 1.2 (1.1, 1.3) * |
| Educational level | ||||||
| Middle school or below | 6852 | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 |
| High school | 2760 | 0.7 (0.6, 0.8) * | 0.6 (0.5, 0.7) * | 0.8 (0.7, 0.9) * | 0.9 (0.8, 0.9) * | 0.9 (0.8, 0.9) * |
| College and university | 3839 | 0.9 (0.8, 0.9) * | 0.8 (0.7, 0.9) * | 0.9 (0.8, 0.9) * | 0.9 (0.8, 0.9) * | 0.9 (0.9, 0.9) * |
| Registered residence | ||||||
| In urban areas | 5315 | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 |
| In rural areas | 8316 | 0.9 (0.7, 1.0) | 0.9 (0.9, 1.0) | 0.9 (0.8, 1.0) | 0.9 (0.7, 1.0) | 1.1 (1.0, 1.2) * |
| Monthly family income, CNY | ||||||
| <5000 | 5655 | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 |
| 5000–7499 | 3504 | 1.0 (0.9, 1.2) | 0.9 (0.8, 1.0) | 1.0 (0.9, 1.2) | 1.2 (0.9, 1.4) | 1.0 (0.9, 1.1) |
| ≥7500 | 4292 | 1.1 (0.9, 1.2) | 1.0 (0.9, 1.1) | 0.9 (0.8, 1.1) | 1.1 (0.9, 1.3) | 1.0 (0.9, 1.2) |
| Medical history of pneumonia | ||||||
| No | 11,439 | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 |
| Yes | 2012 | 0.8 (0.7, 0.9) * | 0.8 (0.7, 0.9) * | 0.9 (0.8, 1.1) | 1.1 (0.9, 1.3) | 1.0 (0.8, 1.1) |
| Medical history of influenza | ||||||
| No | 10,243 | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 |
| Yes | 3208 | 0.8 (0.7, 0.9) * | 0.6 (0.6, 0.7) * | 0.9 (0.7, 1.0) | 1.0 (0.8, 1.2) | 0.9 (0.8, 1.0) |
| Medical history of diarrhea | ||||||
| No | 10,913 | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 |
| Yes | 2538 | 1.1 (0.9, 1.2) | 1.1 (0.9, 1.2) | 1.4 (1.2, 1.7) * | 1.1 (0.9, 1.4) | 1.0 (0.9, 1.2) |
| Medical history of hand, foot and mouth disease | ||||||
| No | 12,470 | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 |
| Yes | 981 | 0.9 (0.8, 1.1) | 0.8 (0.7, 0.9) * | 0.7 (0.6, 0.9) * | 0.8 (0.6, 0.9) * | 1.0 (0.8, 1.1) |
| History of AEFI ** | ||||||
| No/not sure | 13,126 | - | - | - | - | 1.0 |
| Yes | 325 | - | - | - | - | 1.5 (1.2, 1.9) * |
| Adult vaccine hesitancy | ||||||
| per incremental 1 score | - | 0.9 (0.9, 0.9) * | 0.9 (0.9, 0.9) * | 0.9 (0.9, 0.9) * | 0.9 (0.9, 0.9) * | 0.9 (0.9, 0.9) * |
| Vaccine Effectiveness 95% vs. 80% | Mild Common AEFI 1 Day of Headache, Fatigue vs. 1–2 Days of Fever | Rare but Severe AEFI No Risk vs. Same Risk as Flu Vaccine | No. Doses 1 Dose vs. 2 Doses | |
|---|---|---|---|---|
| Total (n = 13,451) | ||||
| % Pos * | 79.2 | 90.1 | 85.3 | 61.5 |
| Estimate (SD) | 1.138 | 1.993 | 1.731 | 0.788 |
| SD | 1.001 | 1.020 | 1.021 | 1.022 |
| p value | <0.001 | <0.001 | <0.001 | <0.001 |
| Vaccine hesitancy score ≤18 (n = 4055) | ||||
| % Pos * | 77.2 | 87.5 | 79.7 | 66.9 |
| Estimate | 1.137 | 1.889 | 1.675 | 0.827 |
| SD | 1.002 | 1.030 | 1.040 | 1.041 |
| p value | <0.001 | <0.001 | <0.001 | <0.001 |
| Vaccine hesitancy score 19–24 (n = 6591) | ||||
| % Pos * | 81.5 | 92.4 | 83.8 | 59.7 |
| Estimate | 1.140 | 2.070 | 1.724 | 0.759 |
| SD | 1.002 | 1.038 | 1.031 | 1.032 |
| p value | <0.001 | <0.001 | <0.001 | <0.001 |
| Vaccine hesitancy score ≥25 (n = 2805) | ||||
| % Pos * | 76.7 | 94.3 | 89.3 | 63.1 |
| Estimate | 1.135 | 2.136 | 1.835 | 0.798 |
| SD | 1.003 | 1.046 | 1.048 | 1.049 |
| p value | <0.001 | <0.001 | <0.001 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
A, K.; Lu, X.; Wang, J.; Hu, L.; Li, B.; Lu, Y. Association between Adult Vaccine Hesitancy and Parental Acceptance of Childhood COVID-19 Vaccines: A Web-Based Survey in a Northwestern Region in China. Vaccines 2021, 9, 1088. https://doi.org/10.3390/vaccines9101088
A K, Lu X, Wang J, Hu L, Li B, Lu Y. Association between Adult Vaccine Hesitancy and Parental Acceptance of Childhood COVID-19 Vaccines: A Web-Based Survey in a Northwestern Region in China. Vaccines. 2021; 9(10):1088. https://doi.org/10.3390/vaccines9101088
Chicago/Turabian StyleA, Kezhong, Xinyue Lu, Jing Wang, Linjie Hu, Bingzhe Li, and Yihan Lu. 2021. "Association between Adult Vaccine Hesitancy and Parental Acceptance of Childhood COVID-19 Vaccines: A Web-Based Survey in a Northwestern Region in China" Vaccines 9, no. 10: 1088. https://doi.org/10.3390/vaccines9101088
APA StyleA, K., Lu, X., Wang, J., Hu, L., Li, B., & Lu, Y. (2021). Association between Adult Vaccine Hesitancy and Parental Acceptance of Childhood COVID-19 Vaccines: A Web-Based Survey in a Northwestern Region in China. Vaccines, 9(10), 1088. https://doi.org/10.3390/vaccines9101088