Parents’ Knowledge, Attitude and Perceptions on Childhood Vaccination in Saudi Arabia: A Systematic Literature Review


Abstract
:1. Introduction
Objectives
- To describe the KAPs of parents towards childhood vaccination in Saudi Arabia.
- To explore the reasons for the delayed and non-vaccination of children.
- To highlight the evidence gap and make recommendations for the relevant interventions based on the findings of the systematic review.
2. Methods
2.1. Eligibility Criteria
2.2. Data Sources and Search Strategy
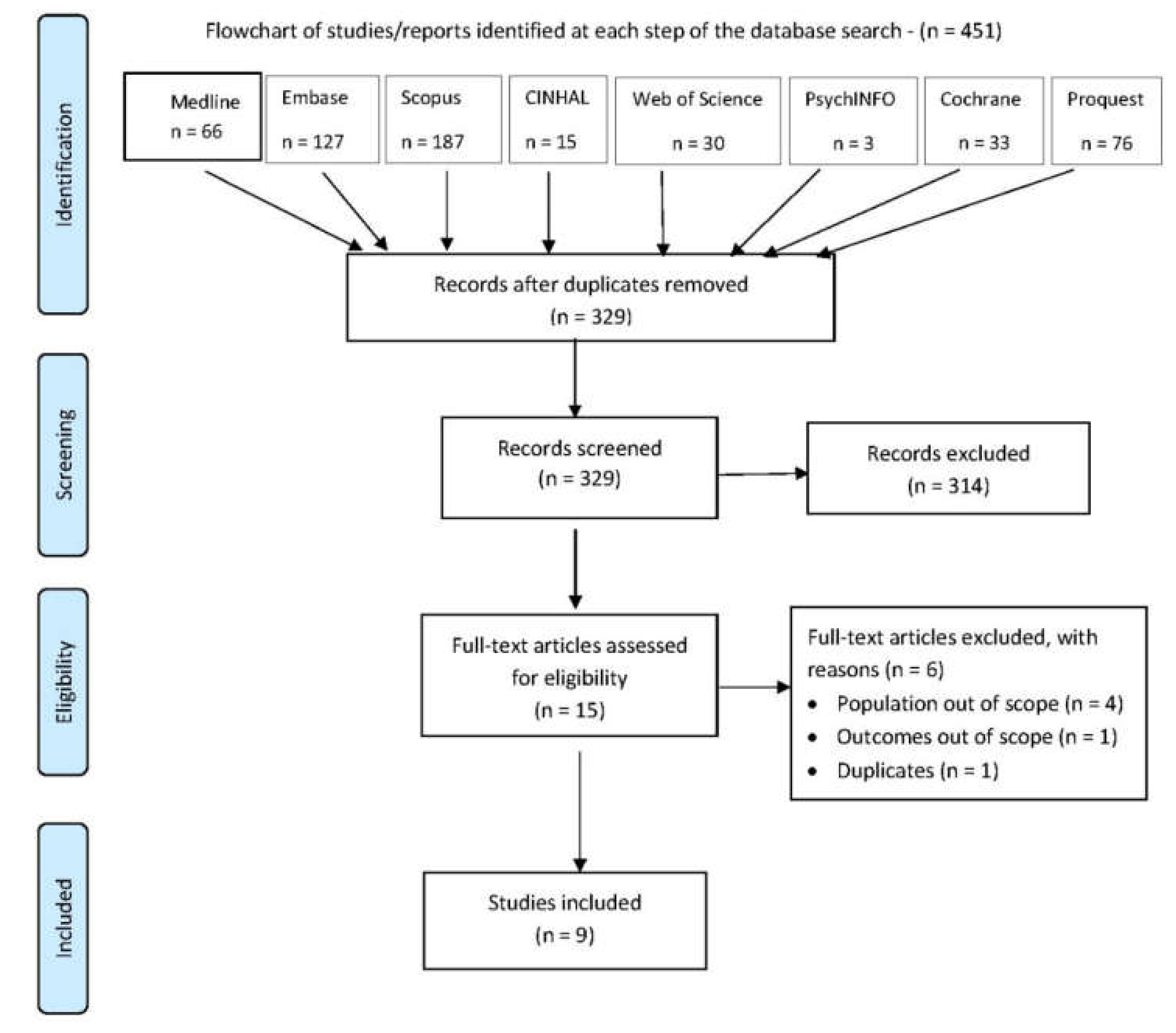
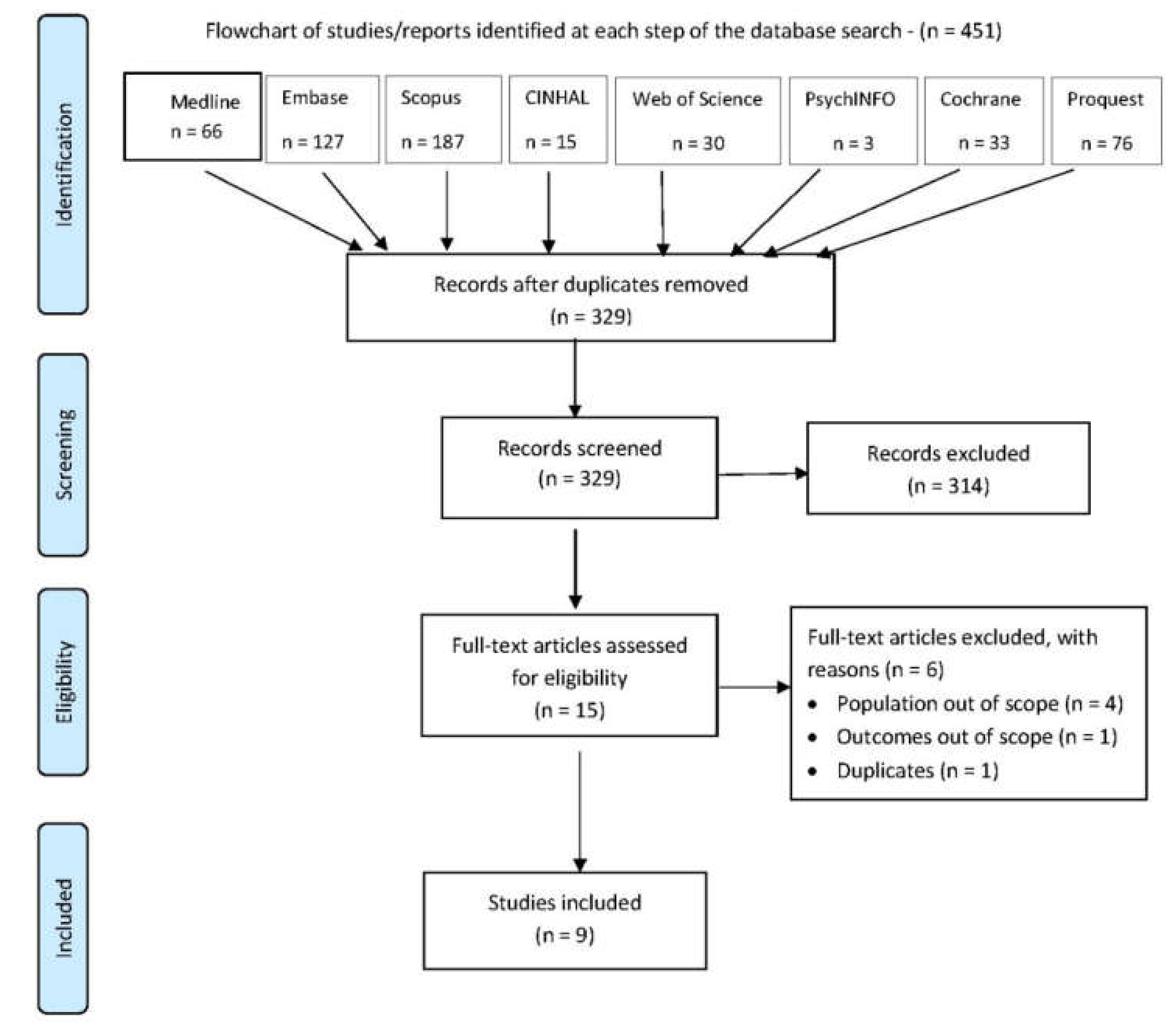
2.3. Study Selection
2.4. Interpretation and Data Extraction
- Study details: study name, study design, year of publication, study setting, country, recruitment method, number of study centres, inclusion and exclusion criteria and sample size.
- Parents’ characteristics: age, gender, education level, income, employment status, residence area (rural/urban), number of children under their care and age of the youngest child.
- Children’s characteristics: age and immunisation status.
- Data collection instruments and characteristics: name, reference and characteristics.
- Outcomes: knowledge, attitude, perceptions and reasons for not vaccinating.
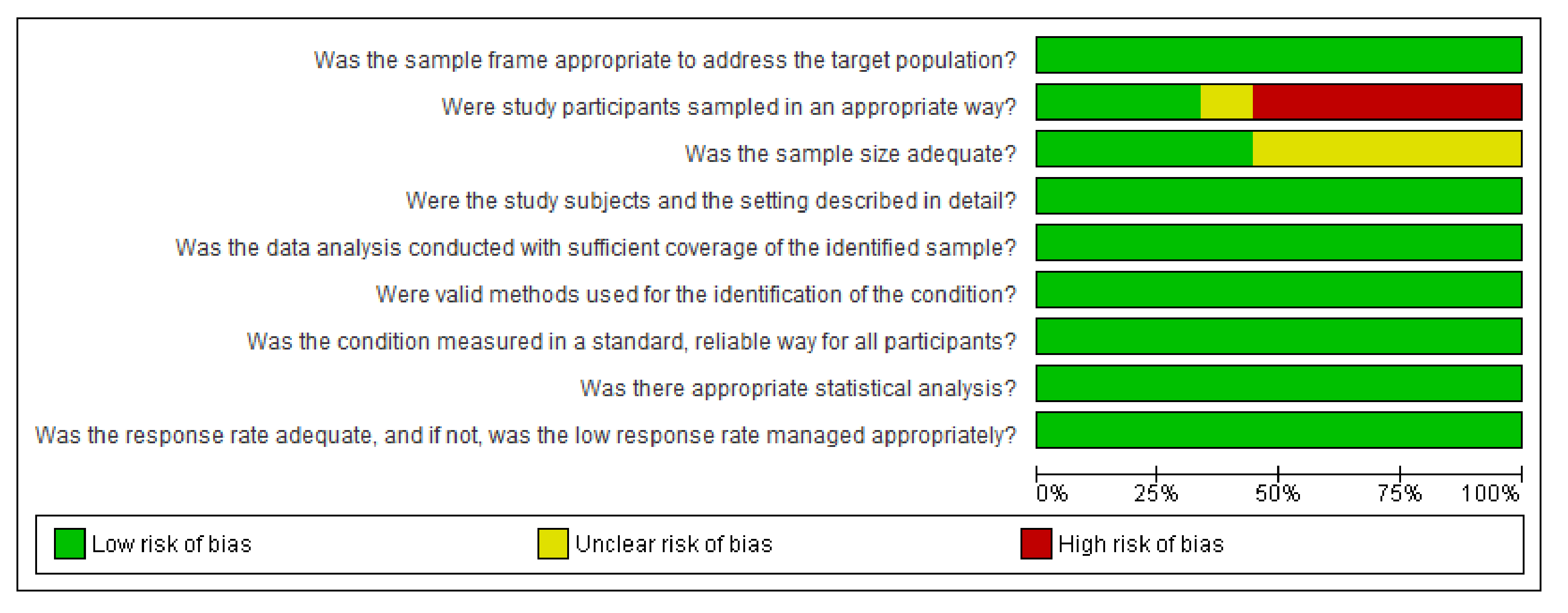
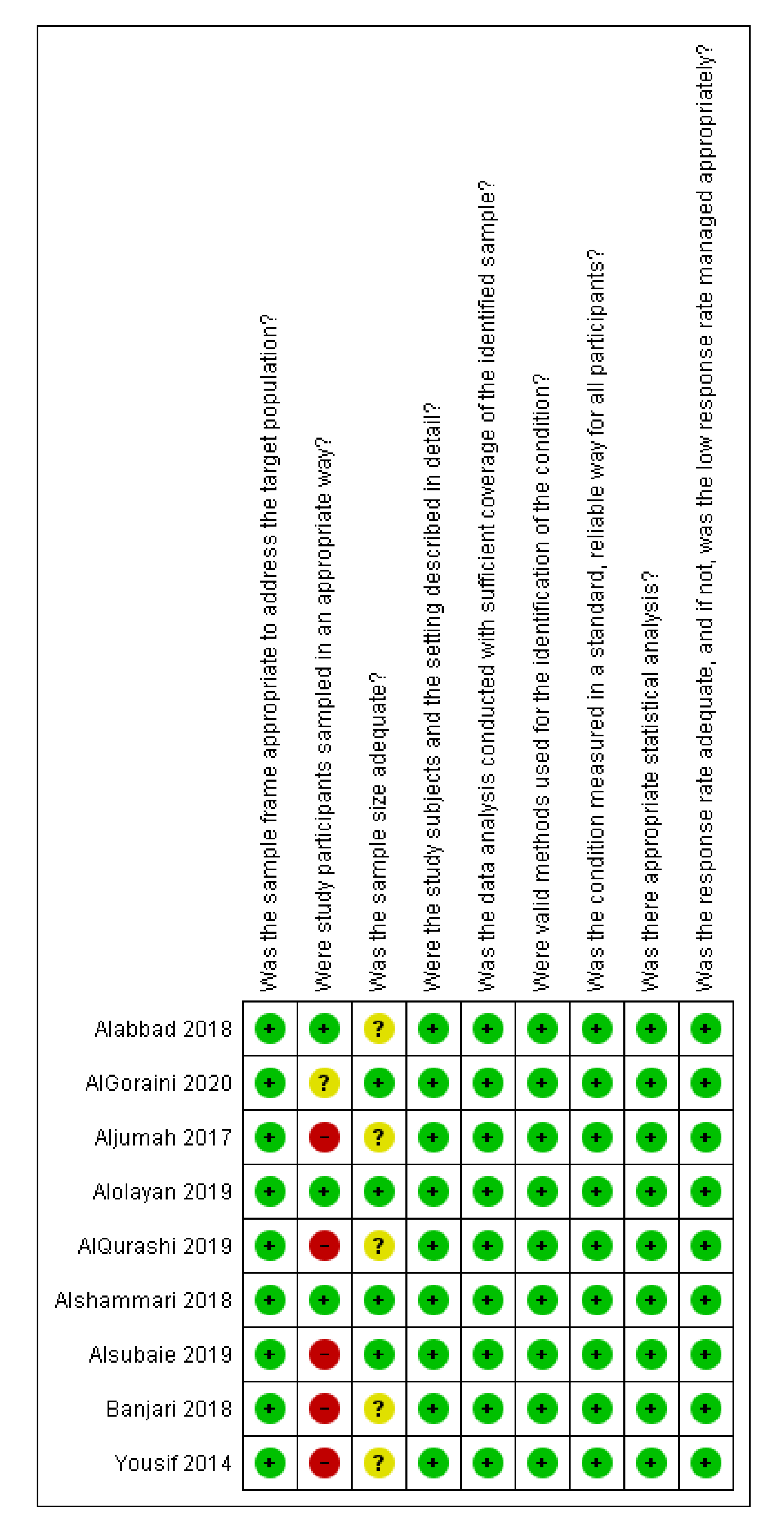
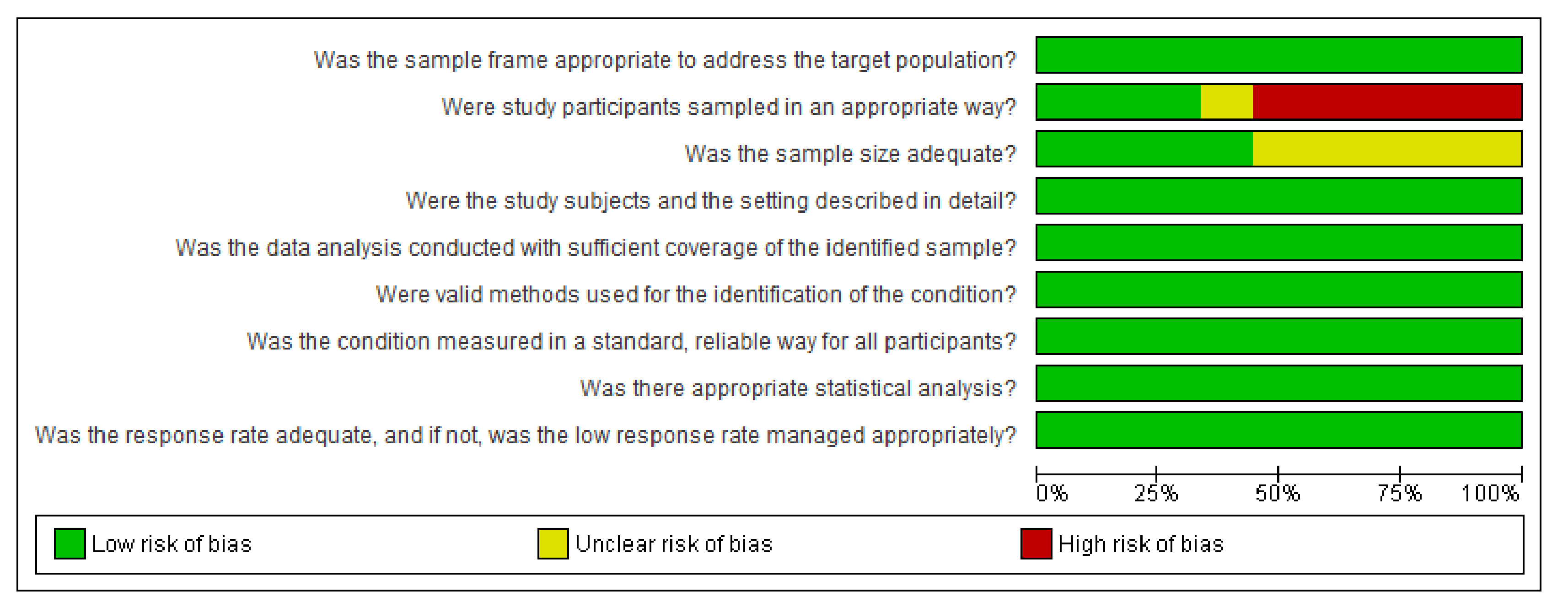
2.5. Quality Appraisal
3. Results
3.1. Studies Characteristics
3.2. Participants’ Characteristics
3.3. DCIs Characteristics
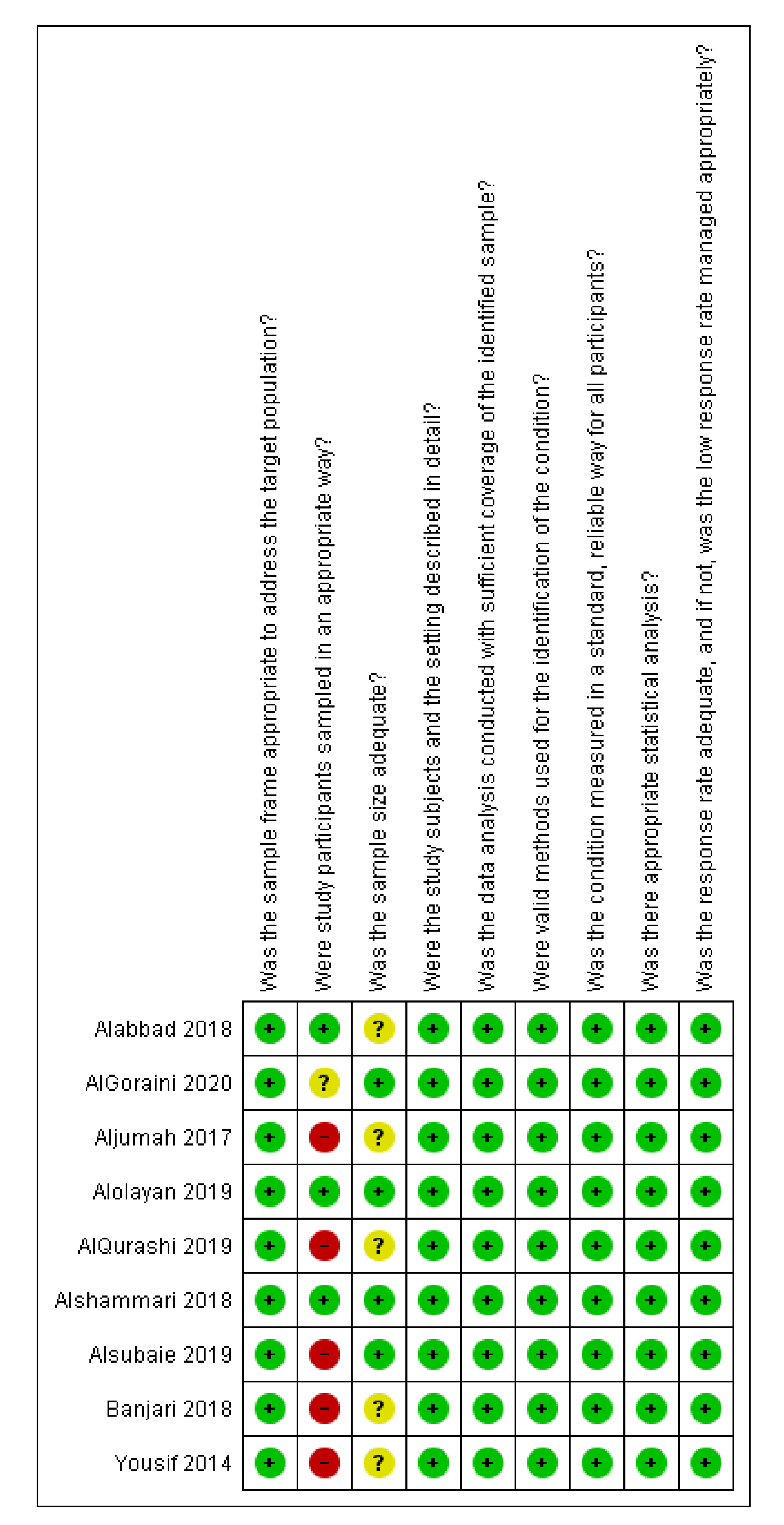
3.4. Quality Assessment
3.5. Knowledge of Parents
3.6. Attitude of Parents
3.7. Perception/Hesitancy of Parents
3.8. Sources of Vaccination Information
3.9. Reasons for Low Vaccine Uptake
4. Discussion
Limitations of Included Studies
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Set# | Searched for | Databases |
|---|---|---|
| S1 | (MESH.EXACT.EXPLODE(“Health Knowledge, Attitudes, Practice”) OR MESH.EXACT.EXPLODE(“Patient Medication Knowledge”) OR MESH.EXACT.EXPLODE(“Knowledge”)) | MEDLINE® |
| S2 | (MESH.EXACT.EXPLODE(“Attitude”) OR MESH.EXACT.EXPLODE(“Attitude to Health”)) | MEDLINE® |
| S3 | (ti,ab(“know” or “aware” or “attitude” or “perception” or “health attitude” or “perceive” or “opinion” or “accept” or “belie” or “knowledge” or “intention” or “interest” or “view” or “awareness” or “practice” or “kap” or “KAP”)) | MEDLINE® |
| S4 | S3 OR S2 OR S1 | MEDLINE® |
| S5 | (MESH.EXACT.EXPLODE(“Vaccination”) OR MESH.EXACT.EXPLODE(“Immunization”) OR (ti,ab(“vaccin” or “immun”))) | MEDLINE® |
| S6 | (MESH.EXACT.EXPLODE(“Child”) OR MESH.EXACT.EXPLODE(“Infant”) OR MESH.EXACT.EXPLODE(“Adolescent”) OR (ti,ab(“boy” or “girl” or “child” or “infant” or “adolescent”))) | MEDLINE® |
| S7 | S6 AND S5 | MEDLINE® |
| S8 | (ti,ab(“saudi arabia”) or ti,ab(“Kingdom of Saudi Arabia”) or ti,ab(“saudi”) or ti,ab(“arabia”)) | MEDLINE® |
| S9 | S8 AND S7 AND S4 | MEDLINE® |
| S10 | (S9) and (pd(>20090925)) and (human(yes)) and (la.exact(“English”)) | MEDLINE® |
| S11 | (S9) and (pd(>20100925)) and (human(yes)) and (la.exact(“English”)) | MEDLINE® |
| S12 | EMB.EXACT.EXPLODE(“knowledge”) OR (EMB.EXACT.EXPLODE(“attitude to health”) OR EMB.EXACT.EXPLODE(“attitude”)) OR (EMB.EXACT(“perception”) OR EMB.EXACT.EXPLODE(“perception deafness”)) | Embase® |
| S13 | ((ti,ab(“know” or “aware” or “attitude” or “perception” or “health attitude” or “perceive” or “opinion” or “accept” or “belie” or “knowledge” or “intention” or “interest” or “view*” or “awareness” or “practice” or “kap” or “KAP”))) | Embase® |
| S14 | S13 OR S12 | Embase® |
| S15 | EMB.EXACT.EXPLODE(“vaccination”) OR ((ti,ab(“vaccin” or “immun” or “immunisation” or “immunization”))) | Embase® |
| S16 | EMB.EXACT.EXPLODE(“adolescent”) OR (EMB.EXACT.EXPLODE(“juvenile”) OR EMB.EXACT.EXPLODE(“child”)) OR EMB.EXACT.EXPLODE(“boy”) OR EMB.EXACT.EXPLODE(“girl”) OR ((ti,ab(“boy” or “girl*” or “child” or “infant” or “adolescent”))) | Embase® |
| S17 | S16 AND S15 | Embase® |
| S18 | ((ti,ab(“saudi arabia”) or ti,ab(“Kingdom of Saudi Arabia”) or ti,ab(“saudi”) or ti,ab(“arabia”))) | Embase® |
| S19 | S18 AND S17 AND S14 | Embase® |
| S20 | (S19) and (ud(>20100925)) and (human(yes)) and (la.exact(“English”)) | Embase® |
Appendix B
Appendix C
References
- Australia, H. Immunisation and Vaccinations. Available online: https://www.healthdirect.gov.au/immunisation-and-vaccinations (accessed on 20 September 2020).
- WHO. Assessment Report of the Global Vaccine Action Plan. Strategic Advisory Group of Experts on Immunization; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Hadjipanayis, A.; van Esso, D.; del Torso, S.; Dornbusc, H.J.; Michailidou, K.; Minicuci, N.; Pancheva, R.; Mujkic, A.; Geitmann, K.; Syridou, G.; et al. Vaccine Confidence Among Parents: Large Scale Study in Eighteen European Countries. Vaccine 2020, 38, 1505–1512. [Google Scholar]
- MOH. Childhood Vaccines Available Daily in all Health Centers. Available online: https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/News-2017-07-20-001.aspx (accessed on 20 September 2020).
- Siddiqi, N.; Siddiqi, A.; Nisar, N.; Khan, A. Mothers’ Knowledge about EPI and Its Relation with Age-Appropriate Vaccination of Infants in Peri-Urban Karachi. J. Pak. Med. Assoc. 2010, 60, 940. [Google Scholar]
- Žagminas, K.; Šurkienė, G.; Urbanovič, N.; Stukas, R. Parental attitudes towards children’s vaccination. Medicina 2007, 43, 161. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar]
- Endnote. Available online: https://www.endnote.com/ (accessed on 20 September 2020).
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar]
- Aromataris, E.; Munn, Z. JBI Manual for Evidence Synthesis, in Chapter 11: Scoping Reviews. Available online: https://synthesismanual.jbi.global (accessed on 25 September 2020).
- Statistical Algorithms in Review Manager. Available online: https://www.researchgate.net/profile/Jonathan_Deeks2/publication/252093205_Statistical_Algorithms_in_Review_Manager_5/links/54d159b70cf28370d0e07f9e.pdf (accessed on 25 September 2020).
- AlGoraini, Y.; AlDujayn, N.N.; AlRasheed, M.A.; Bashawri, Y.E.; Alsubaie, S.S.; AlShahrani, D.A. Confidence toward vaccination as reported by parents of children admitted to a tertiary care hospital in Riyadh, Saudi Arabia: A cross sectional study. Vacunas 2020, 21, 95–104. [Google Scholar]
- Alsubaie, S.S.; Gosadi, I.M.; Alsaadi, B.M.; Albacker, N.B.; Bawazir, M.A.; Bin-Daud, N.; Almanie, W.B.; Alsaadi, M.M.; Alzamil, F.A. Vaccine hesitancy among Saudi parents and its determinants. Saudi. Med. J. 2019, 40, 1242–1250. [Google Scholar]
- Banjari, M.A.; Alamri, A.A.; Algarni, A.Y.; Abualjadayel, M.H.; Alshardi, Y.S.; Alahmadi, T.S. How often do children receive their vaccinations late, and why? Saudi Med. J. 2018, 39, 347. [Google Scholar]
- Alshammari, T.M.; Subaiea, G.M.; Hussain, T.; Moin, A.; Yusuff, K.B. Parental perceptions, attitudes and acceptance of childhood immunization in Saudi Arabia: A cross sectional study. Vaccine 2018, 36, 23–28. [Google Scholar]
- Aljumah, K.; al Badr, H.; Alzaidi, N.; al Mutari, A.; Alhwaitan, A. Parents‘ Adherence, Knowledge and Attitudes towards Childhood Vaccination Program in Saudi Arabia in Value in Health; 360 Park Ave South; Elsevier Science Inc.: New York, NY, USA, 2017; pp. 10010–11710. [Google Scholar]
- Yousif, M.; Abdulrahman, A. Parents’ knowledge and attitudes on childhood immunization, Taif, Saudi Arabia. J. Vaccines Vaccin 2013, 5, 2. [Google Scholar]
- Alolayan, A.; Almotairi, B.; Alshammari, S.; Alhearri, M.; Alsuhaibani, M. Seasonal influenza vaccination among Saudi children: Parental barriers and willingness to vaccinate their children. Int. J. Environ. Res. Public Health 2019, 16, 4226. [Google Scholar]
- AlQurashi, A.; Aljishi, H.; Demyati, E. Parental Perception Towards Flu Vaccination for Asthmatic Children in Saudi Arabia. Cureus 2019, 11, e6460. [Google Scholar]
- Alabbad, A.A.; Alsaad, A.K.; Al Shaalan, M.A.; Alola, S.; Albanyan, E.A. Prevalence of influenza vaccine hesitancy at a tertiary care hospital in Riyadh, Saudi Arabia. J. Infect. Public Health 2018, 11, 491–499. [Google Scholar]
- Larson, H.J.; Jarrett, C.; Schulz, W.S.; Chaudhuri, M.; Zhou, Y.; Dube, E.; Schuster, M.; MacDonald, N.E.; Wilson, R.; SAGE Working Group on Vaccine Hesitancy. Measuring vaccine hesitancy: The development of a survey tool. Vaccine 2015, 33, 4165–4175. [Google Scholar]
- MOH. Health Awareness—Immunization (Vaccines). Available online: https://www.moh.gov.sa/en/HealthAwareness/EducationalContent/vaccination/Pages/003.aspx (accessed on 25 September 2020).
- Facione, N.C. The Triandis model for the study of health and illness behavior: A social behavior theory with sensitivity to diversity. Adv. Nurs. Sci. 1993, 15, 49–58. [Google Scholar]
| Category | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Population |
|
|
| Outcomes | The outcomes consisted of at least one of the following:
| |
| Study Design |
|
|
| Geographical location |
|
|
| Year of Publication |
|
|
| Language |
|
|
| ||
| Source | Number of Hits | Total after De-Duplication |
|---|---|---|
| Medline | 66 | 329 |
| Embase | 127 | |
| CENTRAL | 33 | |
| Scopus | 187 | |
| CINHAL | 15 | |
| PsychINFO | 3 | |
| Web of Science | 30 | |
| ProQuest | 76 |
| R | Aim of the Study | Participants (n) | Vaccine Focus | Kid’s Age | Conclusions |
|---|---|---|---|---|---|
| [12] | To assess the magnitude of hesitancy of parents towards vaccines and to determine the reasons parents either partially vaccinate and/or do not vaccinate children in Riyadh, Saudi Arabia | 384 | National Childhood Immunisation Program | <14 years | Confidence towards vaccinations is good among parents in Riyadh, Saudi Arabia. Only a minority of the parents showed hesitancy |
| [13] | To assess the prevalence of vaccine hesitancy among Saudi parents along with its determinants | 500 | National Childhood Immunisation Program | 2 months–7 years | Vaccine hesitancy is a major concern among parents in the Kingdom of Saudi Arabia (KSA) suggesting risk to the currently reported high vaccination level. Vaccination status of children cannot be used as the main indicator to assess vaccine hesitancy, as it does not consider parents who have significant concerns towards vaccines |
| [14] | To assess vaccination timeliness, risk factors associated with delays and the reasons for delayed vaccinations among children below the age of 3 years in Jeddah, Saudi Arabia. | 351 | National Childhood Immunisation Program | <3 years | Adherence to vaccination is fairly common in this part of the country. However, vaccination delays are still present and should be addressed to improve health care |
| [15] | To assess perceptions of and attitudes towards routine childhood immunisation among Saudi parents | 467 | National Childhood Immunisation Program | <5 years | Confidence in and acceptance of childhood vaccinations and perceptions of vaccine-related health benefits were quite good among Saudi parents. Parents also appeared to have easy access to diverse sources of vaccine-related information and education |
| [16] | To assess parents’ adherence, knowledge and attitudes on childhood vaccination program among the Saudi population | 180 | National Childhood Immunisation Program | 0–2 years | Although parents had good adherence, knowledge and positive attitudes on some aspects related to childhood immunisation, gaps in both studied domains were identified |
| [17] | To assess parental knowledge and attitudes on childhood immunisation among Saudi parents | 731 | National Childhood Immunisation Program | 0–12 years | The parents had good knowledge and positive attitudes on some aspects related to childhood immunisation. However, gaps in both studied domains were identified |
| [18] | To demonstrate parents’ attitudes towards the influenza vaccine and to identify possible barriers towards having their children vaccinated against influenza | 399 | Influenza vaccination | >6 months | Although parents’ knowledge level was poor, parental attitudes towards the seasonal influenza vaccine were generally positive. The majority of parents were aware of the seasonal influenza vaccine; however, adherence to receiving the vaccination for both themselves and their children was low |
| [19] | To review the perception of parents with asthmatic children towards flu vaccination and its influence on their decision to vaccinate their children in KSA | 190 | Influenza Vaccination | 6 months–15 years | Parents agreed with most of the positive statements of perception towards the vaccine against the flu in asthmatic children, including that non-vaccinated children are more likely to contract the flu virus. The rate of vaccination among their children was, however, low and most of the parents believe that vaccination does not prevent flu virus |
| [20] | To assess the prevalence of influenza vaccine hesitancy among parents, adult patients and HCWs at King Abdulaziz Medical City, Riyadh | 300 | Influenza Vaccination | Up to 14 years | Influenza vaccination hesitancy in King Abdulaziz Medical City in Riyadh was low (17%) |
| R | Data Collection Instrument (DCI) | DCI Reference | DCI Characteristics |
|---|---|---|---|
| [12] | WHO standardised questionnaire | Not Relevant (NR) | Article in press—DCI characteristics are not reported in the abstract |
| [13] | 11-item vaccine hesitancy scale, designed by the SAGE group | [21] | Parents completed 10 dichotomous (yes/no) questions, 11 Likert-type scale (strongly agree, agree, neutral, disagree, or strongly disagree) vaccine hesitancy scale questions and 5 open-ended questions |
| [14] | 28-item semi-structured questionnaire | [14] | Questions were asked at a simple reading level in both Arabic and English. The study instrument had 5 sections. The first examined the child’s personal information such as date of birth, gender and nationality. The second was regarding the biodata of the parents and inquired about their financial status, educational background and health status. The third section assessed the caretaker’s perspective on vaccinations and whether they presumed that they have vaccination delays using the Likert scale. The fourth section concentrated on the child’s physical well-being that could affect his/her vaccination status. The last section focussed on possible reasons for vaccine delays. Additionally, a blank space was provided for the caretaker to give additional reasons. |
| [15] | 18-item structured questionnaire | [15] | The questionnaire had 3 sections. The first section focussed on gender, parents’ ages, education, occupation, the number of children less than 5 years old in family and monthly income. The second section assessed parents’ awareness of the benefits associated with and purpose of vaccination, as well as parents’ confidence in recommending vaccinations to others and sources of information about vaccination and immunisation programs in Saudi Arabia. The third section focussed on current practices in vaccination, including the vaccination status of their children, problems experienced in accessing vaccinations, hospital visits associated with adverse events following vaccination and views about religion and childhood vaccinations that are recommended for children up to 5 years according to the immunisation program. |
| [16] | Arabic validated questionnaire | NR | An Arabic validated questionnaire was used to collect demographic data, education level, time of vaccination, adherence, knowledge about childhood vaccination programs and attitudes of the parents |
| [17] | The questionnaire was formulated based on questions and answers published by the Ministry of Health, Saudi Arabia | [22] | The questionnaire was thoroughly revised by the research team for validity, comprehensiveness and appropriateness to collect the required information from the targeted population. There were three main sections to collect data on parents’ demographics, parents’ knowledge and attitudes on childhood immunisation. Responses to knowledge questions were recorded as “Yes”, “No” and “Don’t know”. A five-point-Likert scale (“Strongly agree”, “Agree”, “Not sure”, “Disagree” and “Strongly disagree”) was used to assess parents’ attitudes towards childhood immunisation. |
| [18] | 29-question questionnaire | NR | The questionnaire included four sections: Section 1, demographic data; Section 2, influenza vaccine awareness; Section 3, influenza vaccine knowledge; Section 4, attitudes towards the influenza vaccine |
| [19] | Survey tool adopted from the Triandis model | [23] | The semi-structured questionnaire was developed to obtain data on demographics, knowledge, attitudes, social support, perceived benefits and causes of non-adherence. The respondents’ agreement was measured using the Likert agreement scale |
| [20] | Authors’ developed and validated questionnaire to evaluate influenza vaccine hesitancy | [20] | The questionnaire included data on demographics (age, sex, chronic illnesses, education level), willingness to take the vaccine both in the past and in the future, reasons for not taking the vaccine, knowledge of the vaccine and sources of this knowledge and confidence in the vaccine |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alabadi, M.; Aldawood, Z. Parents’ Knowledge, Attitude and Perceptions on Childhood Vaccination in Saudi Arabia: A Systematic Literature Review. Vaccines 2020, 8, 750. https://doi.org/10.3390/vaccines8040750
Alabadi M, Aldawood Z. Parents’ Knowledge, Attitude and Perceptions on Childhood Vaccination in Saudi Arabia: A Systematic Literature Review. Vaccines. 2020; 8(4):750. https://doi.org/10.3390/vaccines8040750
Chicago/Turabian StyleAlabadi, Marwa, and Zakariya Aldawood. 2020. "Parents’ Knowledge, Attitude and Perceptions on Childhood Vaccination in Saudi Arabia: A Systematic Literature Review" Vaccines 8, no. 4: 750. https://doi.org/10.3390/vaccines8040750
APA StyleAlabadi, M., & Aldawood, Z. (2020). Parents’ Knowledge, Attitude and Perceptions on Childhood Vaccination in Saudi Arabia: A Systematic Literature Review. Vaccines, 8(4), 750. https://doi.org/10.3390/vaccines8040750