Intramuscular and Intradermal Electroporation of HIV-1 PENNVAX-GP® DNA Vaccine and IL-12 Is Safe, Tolerable, Acceptable in Healthy Adults

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Study Agents
2.3. Study Schedule and Dose
2.4. Electroporation
2.5. Safety and Tolerability Assessments
2.6. Statistical Methods
3. Results
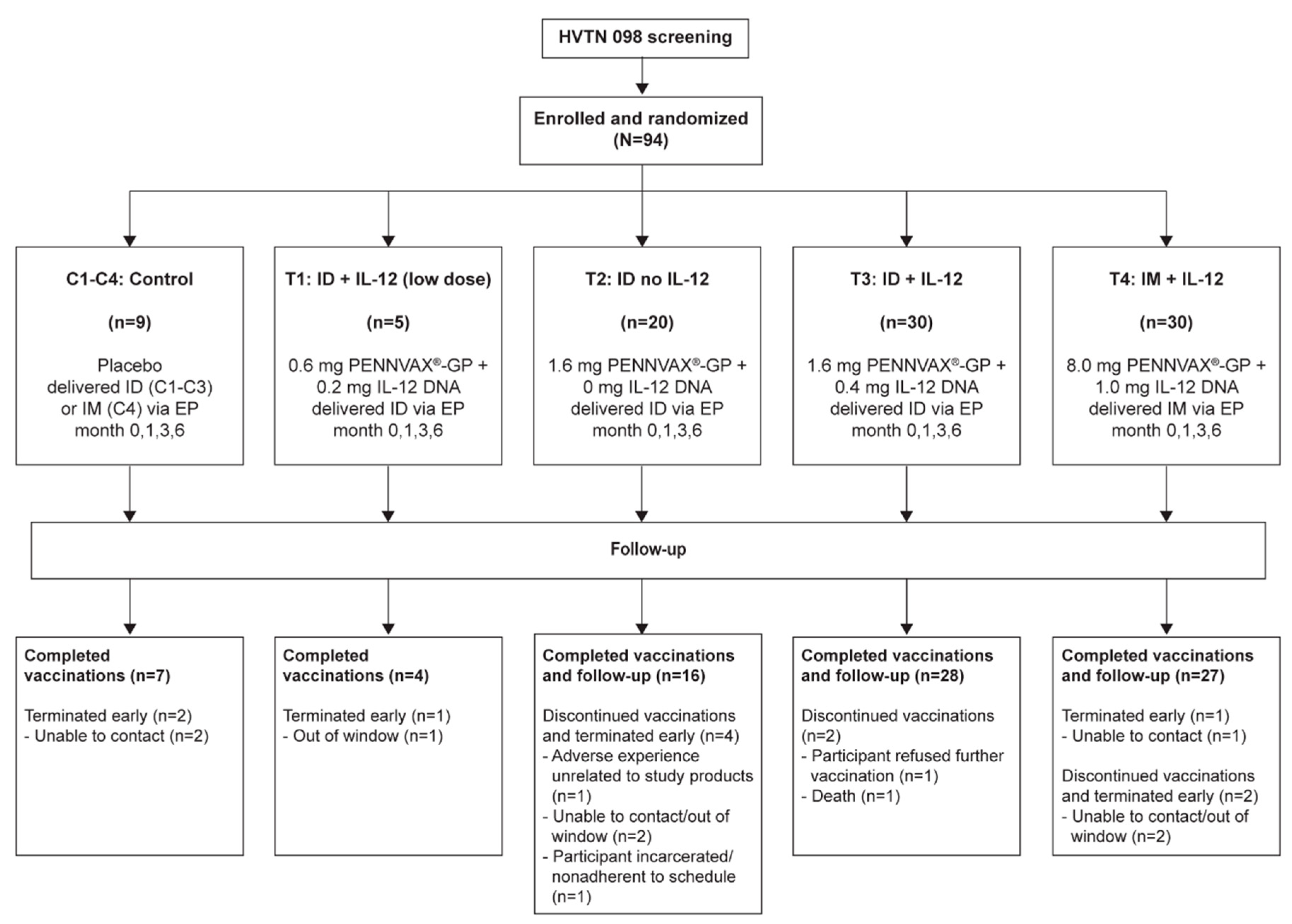
3.1. Study Population Characteristics
3.2. Pain Scores and Reactogenicity
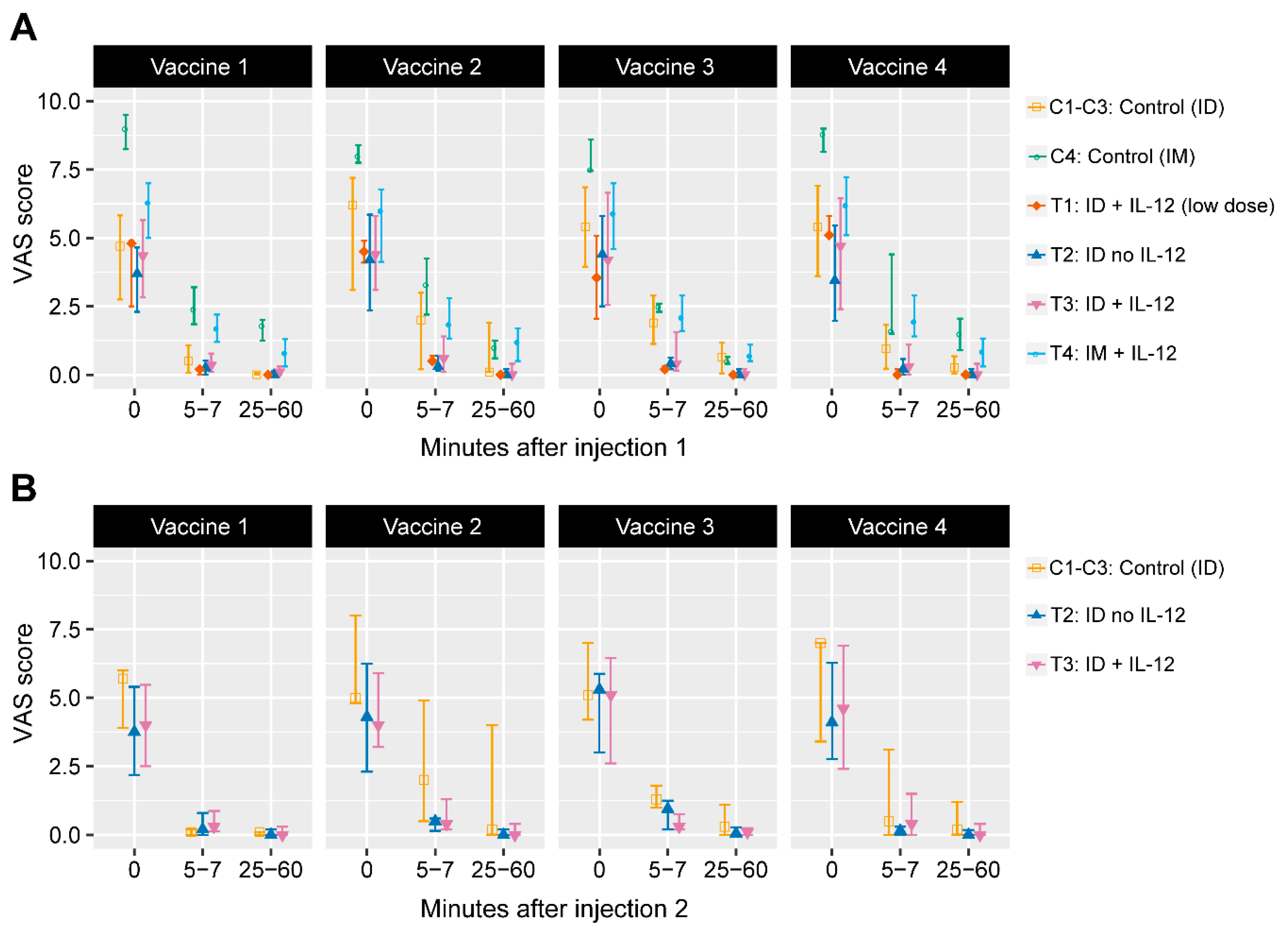
3.2.1. VAS Scores
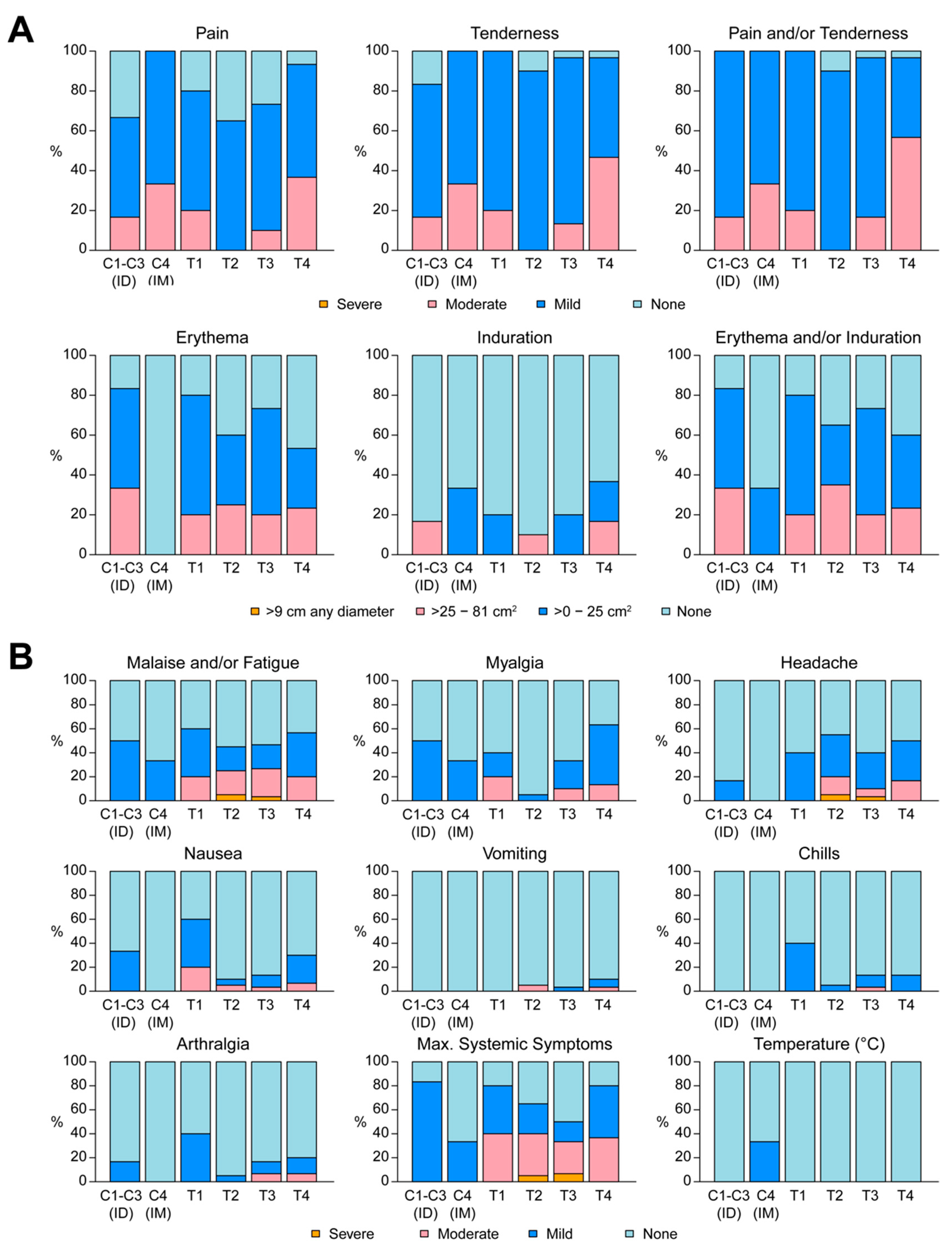
3.2.2. Reactogenicity
3.3. Adverse Events
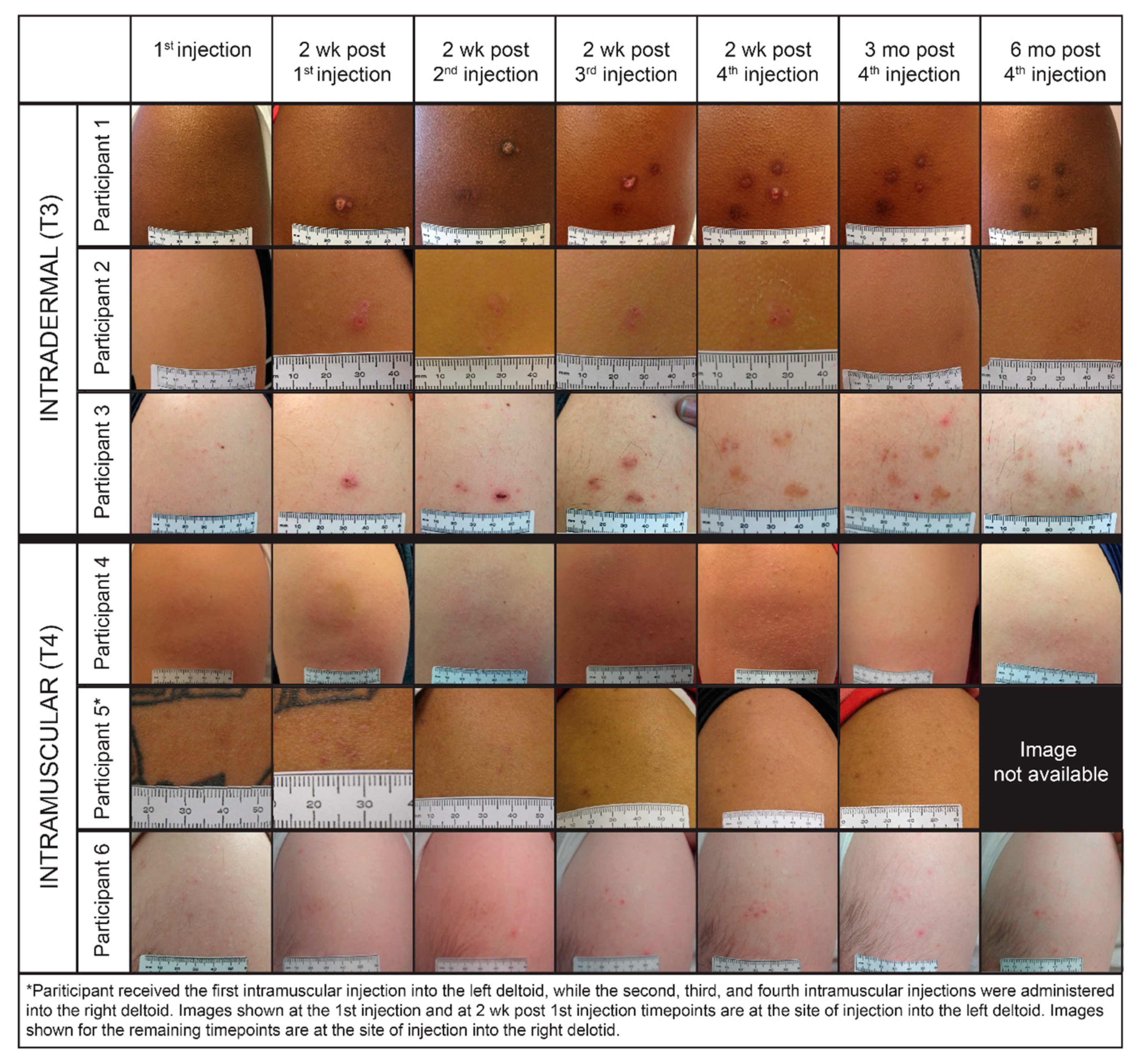
3.4. Acceptability of Electroporation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gary, E.N.; Weiner, D.B. DNA vaccines: Prime time is now. Curr. Opin. Immunol. 2020, 65, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Jin, X.; Morgan, C.; Yu, X.; DeRosa, S.; Tomaras, G.D.; Montefiori, D.C.; Kublin, J.; Corey, L.; Keefer, M.C. Multiple factors affect immunogenicity of DNA plasmid HIV vaccines in human clinical trials. Vaccine 2015, 33, 2347–2353. [Google Scholar] [CrossRef] [PubMed]
- Hokey, D.A.; Weiner, D.B. DNA vaccines for HIV: Challenges and opportunities. Springer Semin Immunopathol. 2006, 28, 267–279. [Google Scholar] [CrossRef]
- Favard, C.; Dean, D.S.; Rols, M.P. Electrotransfer as a non viral method of gene delivery. Curr. Gene Ther. 2007, 7, 67–77. [Google Scholar] [CrossRef] [PubMed]
- Sardesai, N.Y.; Weiner, D.B. Electroporation delivery of DNA vaccines: Prospects for success. Curr. Opin. Immunol. 2011, 23, 421–429. [Google Scholar] [CrossRef]
- Gehl, J.; Mir, L.M. Determination of optimal parameters for in vivo gene transfer by electroporation, using a rapid in vivo test for cell permeabilization. Biochem. Biophys. Res. Commun. 1999, 261, 377–380. [Google Scholar] [CrossRef]
- Broderick, K.E.; Humeau, L.M. Electroporation-enhanced delivery of nucleic acid vaccines. Expert Rev. Vaccines 2015, 14, 195–204. [Google Scholar] [CrossRef]
- Mann, J.F.; McKay, P.F.; Fiserova, A.; Klein, K.; Cope, A.; Rogers, P.; Swales, J.; Seaman, M.S.; Combadiere, B.; Shattock, R.J. Enhanced immunogenicity of an HIV-1 DNA vaccine delivered with electroporation via combined intramuscular and intradermal routes. J. Virol. 2014, 88, 6959–6969. [Google Scholar] [CrossRef]
- Kalams, S.A.; Parker, S.D.; Elizaga, M.; Metch, B.; Edupuganti, S.; Hural, J.; De Rosa, S.; Carter, D.K.; Rybczyk, K.; Frank, I.; et al. Safety and comparative immunogenicity of an HIV-1 DNA vaccine in combination with plasmid interleukin 12 and impact of intramuscular electroporation for delivery. J. Infect. Dis. 2013, 208, 818–829. [Google Scholar] [CrossRef]
- Elizaga, M.L.; Li, S.S.; Kochar, N.K.; Wilson, G.J.; Allen, M.A.; Tieu, H.V.N.; Frank, I.; Sobieszczyk, M.E.; Cohen, K.W.; Sanchez, B.; et al. Safety and tolerability of HIV-1 multiantigen pDNA vaccine given with IL-12 plasmid DNA via electroporation, boosted with a recombinant vesicular stomatitis virus HIV Gag vaccine in healthy volunteers in a randomized, controlled clinical trial. PLoS ONE 2018, 13, e0202753. [Google Scholar] [CrossRef]
- Diehl, M.C.; Lee, J.C.; Daniels, S.E.; Tebas, P.; Khan, A.S.; Giffear, M.; Sardesai, N.Y.; Bagarazzi, M.L. Tolerability of intramuscular and intradermal delivery by CELLECTRA((R)) adaptive constant current electroporation device in healthy volunteers. Hum. Vaccines Immunother. 2013, 9, 2246–2252. [Google Scholar] [CrossRef] [PubMed]
- Schultheis, K.; Smith, T.R.; Kiosses, W.B.; Kraynyak, K.A.; Wong, A.; Oh, J.; Broderick, K.E. Delineating the Cellular Mechanisms Associated with Skin Electroporation. Hum. Gene Ther. Methods 2018, 29, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Tebas, P.; Roberts, C.C.; Muthumani, K.; Reuschel, E.L.; Kudchodkar, S.B.; Zaidi, F.I.; White, S.; Khan, A.S.; Racine, T.; Choi, H.; et al. Safety and Immunogenicity of an Anti-Zika Virus DNA Vaccine-Preliminary Report. N. Engl. J. Med. 2017. [Google Scholar] [CrossRef] [PubMed]
- Tebas, P.; Kraynyak, K.A.; Patel, A.; Maslow, J.N.; Morrow, M.P.; Sylvester, A.J.; Knoblock, D.; Gillespie, E.; Amante, D.; Racine, T.; et al. Intradermal SynCon(R) Ebola GP DNA Vaccine is Temperature Stable and Safely Demonstrates Cellular and Humoral Immunogenicity Advantages in Healthy Volunteers. J. Infect. Dis. 2019, 220, 400–410. [Google Scholar] [CrossRef] [PubMed]
- Kutzler, M.A.; Robinson, T.M.; Chattergoon, M.A.; Choo, D.K.; Choo, A.Y.; Choe, P.Y.; Ramanathan, M.P.; Parkinson, R.; Kudchodkar, S.; Tamura, Y.; et al. Coimmunization with an optimized IL-15 plasmid results in enhanced function and longevity of CD8 T cells that are partially independent of CD4 T cell help. J. Immunol. 2005, 175, 112–123. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.J.; Maguire, H.C., Jr.; Nottingham, L.K.; Morrison, L.D.; Tsai, A.; Sin, J.I.; Chalian, A.A.; Weiner, D.B. Coadministration of IL-12 or IL-10 expression cassettes drives immune responses toward a Th1 phenotype. J. Interferon Cytokine Res. 1998, 18, 537–547. [Google Scholar] [CrossRef]
- Chattergoon, M.A.; Saulino, V.; Shames, J.P.; Stein, J.; Montaner, L.J.; Weiner, D.B. Co-immunization with plasmid IL-12 generates a strong T-cell memory response in mice. Vaccine 2004, 22, 1744. [Google Scholar] [CrossRef]
- Calarota, S.A.; Weiner, D.B. Enhancement of human immunodeficiency virus type 1-DNA vaccine potency through incorporation of T-helper 1 molecular adjuvants. Immunol. Rev. 2004, 199, 84–99. [Google Scholar] [CrossRef]
- Draghia-Akli, R.; Khan, A.S.; Brown, P.A.; Pope, M.A.; Wu, L.; Hirao, L.; Weiner, D.B. Parameters for DNA vaccination using adaptive constant-current electroporation in mouse and pig models. Vaccine 2008, 26, 5230–5237. [Google Scholar] [CrossRef]
- Vignali, D.A.A.; Kuchroo, V.K. IL-12 family cytokines: Immunological playmakers. Nat. Immunol. 2012, 13, 722–728. [Google Scholar] [CrossRef]
- Kalams, S.A.; Parker, S.; Xia, J.; Elizaga, M.; Metch, B.; Wang, M.; Hural, J.; Lubeck, M.; Eldridge, J.; Cardinali, M.; et al. Safety and Immunogenicity of an HIV-1 Gag DNA Vaccine with or without IL-12 and/or IL-15 Plasmid Cytokine Adjuvant in Healthy, HIV-1 Uninfected Adults. PLoS ONE 2012, 7, e29231. [Google Scholar] [CrossRef] [PubMed]
- De Rosa, S.C.; Edupuganti, S.; Huang, Y.; Han, X.; Elizaga, M.; Swann, E.; Polakowski, L.; Kalams, S.A.; Keefer, M.C.; Maenza, J.; et al. Robust antibody and cellular responses induced by DNA-only vaccination for HIV. JCI Insight 2020, 5, e137079. [Google Scholar] [CrossRef] [PubMed]
- Graham, B.S.; Koup, R.A.; Roederer, M.; Bailer, R.T.; Enama, M.E.; Moodie, Z.; Martin, J.E.; McCluskey, M.M.; Chakrabarti, B.K.; Lamoreaux, L.; et al. Phase 1 safety and immunogenicity evaluation of a multiclade HIV-1 DNA candidate vaccine. J. Infect. Dis. 2006, 194, 1650–1660. [Google Scholar] [CrossRef]
- Trimble, C.L.; Morrow, M.P.; Kraynyak, K.A.; Shen, X.; Dallas, M.; Yan, J.; Edwards, L.; Parker, R.L.; Denny, L.; Giffear, M.; et al. Safety, efficacy, and immunogenicity of VGX-3100, a therapeutic synthetic DNA vaccine targeting human papillomavirus 16 and 18 E6 and E7 proteins for cervical intraepithelial neoplasia 2/3: A randomised, double-blind, placebo-controlled phase 2b trial. Lancet 2015, 386, 2078–2088. [Google Scholar] [CrossRef]
- Kenney, R.T.; Frech, S.A.; Muenz, L.R.; Villar, C.P.; Glenn, G.M. Dose sparing with intradermal injection of influenza vaccine. N. Engl. J. Med. 2004, 351, 2295–2301. [Google Scholar] [CrossRef]
- Enama, M.E.; Ledgerwood, J.E.; Novik, L.; Nason, M.C.; Gordon, I.J.; Holman, L.; Bailer, R.T.; Roederer, M.; Koup, R.A.; Mascola, J.R.; et al. Phase I randomized clinical trial of VRC DNA and rAd5 HIV-1 vaccine delivery by intramuscular (i.m.), subcutaneous (s.c.) and intradermal (i.d.) administration (VRC 011). PLoS ONE 2014, 9, e91366. [Google Scholar] [CrossRef]
- Hung, I.F.; Levin, Y.; To, K.K.; Chan, K.H.; Zhang, A.J.; Li, P.; Li, C.; Xu, T.; Wong, T.Y.; Yuen, K.Y. Dose sparing intradermal trivalent influenza (2010/2011) vaccination overcomes reduced immunogenicity of the 2009 H1N1 strain. Vaccine 2012, 30, 6427–6435. [Google Scholar] [CrossRef]
- Khan, A.S.; Broderick, K.E.; Sardesai, N.Y. Clinical development of intramuscular electroporation: Providing a "boost" for DNA vaccines. Methods Mol. Biol. 2014, 1121, 279–289. [Google Scholar] [CrossRef]
- Ho, K.; Spence, J.; Murphy, M.F. Review of Pain-Measurement Tools. Ann. Emerg. Med. 1996, 27, 427–432. [Google Scholar] [CrossRef]
- Grant, S.; Aitchison, T.; Henderson, E.; Christie, J.; Zare, S.; Mc Murray, J.; Dargie, H. A Comparison of the Reproducibility and the Sensitivity to Change of Visual Analogue Scales, Borg Scales, and Likert Scales in Normal Subjects During Submaximal Exercise. Chest 1999, 116, 1208–1217. [Google Scholar] [CrossRef]
- Benjimini, Y.; Hochberg, Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J. R. Stat. Soc. Ser. B. 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Vasan, S.; Hurley, A.; Schlesinger, S.J.; Hannaman, D.; Gardiner, D.F.; Dugin, D.P.; Boente-Carrera, M.; Vittorino, R.; Caskey, M.; Andersen, J.; et al. In vivo electroporation enhances the immunogenicity of an HIV-1 DNA vaccine candidate in healthy volunteers. PLoS ONE 2011, 6, e19252. [Google Scholar] [CrossRef] [PubMed]
- Ake, J.A.; Schuetz, A.; Pegu, P.; Wieczorek, L.; Eller, M.A.; Kibuuka, H.; Sawe, F.; Maboko, L.; Polonis, V.; Karasavva, N.; et al. Safety and Immunogenicity of PENNVAX-G DNA Prime Administered by Biojector 2000 or CELLECTRA Electroporation Device With Modified Vaccinia Ankara-CMDR Boost. J. Infect. Dis. 2017, 216, 1080–1090. [Google Scholar] [CrossRef] [PubMed]
- Canton, D.A.; Shirley, S.; Wright, J.; Connolly, R.; Burkart, C.; Mukhopadhyay, A.; Twitty, C.; Qattan, K.E.; Campbell, J.S.; Le, M.H.; et al. Melanoma treatment with intratumoral electroporation of tavokinogene telseplasmid (pIL-12, tavokinogene telseplasmid). Immunotherapy 2017, 9, 1309–1321. [Google Scholar] [CrossRef] [PubMed]
- Mpendo, J.; Mutua, G.; Nyombayire, J.; Ingabire, R.; Nanvubya, A.; Anzala, O.; Karita, E.; Hayes, P.; Kopycinski, J.; Dally, L.; et al. A Phase I Double Blind, Placebo-Controlled, Randomized Study of the Safety and Immunogenicity of Electroporated HIV DNA with or without Interleukin 12 in Prime-Boost Combinations with an Ad35 HIV Vaccine in Healthy HIV-Seronegative African Adults. PLoS ONE 2015, 10, e0134287. [Google Scholar] [CrossRef] [PubMed]
- Chin, L.J.; Berenson, J.A.; Klitzman, R.L. Typologies of Altruistic and Financial Motivations for Research Participation. J. Empir. Res. Hum. Res. Ethics JERHRE 2016, 11, 299–310. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Control: C1-C4 (n = 9) | T1: ID low dose (n = 5) | T2: ID no IL-12 (n = 20) | T3: ID + IL-12 (n = 30) | T4: IM + IL-12 (n = 30) | Total (n = 94) |
|---|---|---|---|---|---|---|
| Sex | ||||||
| Male | 4 (44%) | 4 (80%) | 12 (60%) | 20 (67%) | 13 (43%) | 53 (56%) |
| Female | 5 (56%) | 1 (20%) | 8 (40%) | 10 (33%) | 17 (57%) | 41 (44%) |
| Race | ||||||
| White | 7 (78%) | 5 (100%) | 19 (95%) | 24 (80%) | 21 (70%) | 76 (81%) |
| Black/African American | 1 (11%) | 0 (0%) | 0 (0%) | 4 (13%) | 3 (10%) | 8 (9%) |
| Asian | 1 (11%) | 0 (0%) | 1 (5%) | 0 (0%) | 1 (3%) | 3 (3%) |
| Native Hawaiian/Pacific Islander | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Native American/Alaskan Native | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Multiracial | 0 (0%) | 0 (0%) | 0 (0%) | 2 (7%) | 5 (17%) | 7 (7%) |
| Other | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Ethnicity | ||||||
| Hispanic or Latino/a | 1 (11%) | 0 (0%) | 0 (0%) | 1 (3%) | 3 (10%) | 5 (5%) |
| Non-Hispanic or Latino/a | 8 (89%) | 5 (100%) | 20 (100%) | 29 (97%) | 27 (90%) | 89 (95%) |
| Age (Years) | ||||||
| Less than 18 | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| 18–20 | 0 (0%) | 0 (0%) | 2 (10%) | 3 (10%) | 3 (10%) | 8 (9%) |
| 21–30 | 6 (67%) | 3 (60%) | 9 (45%) | 13 (43%) | 17 (57%) | 48 (51%) |
| 31–40 | 2 (22%) | 1 (20%) | 7 (35%) | 5 (17%) | 2 (7%) | 17 (18%) |
| 41–50 | 1 (11%) | 0 (0%) | 2 (10%) | 8 (27%) | 7 (23%) | 18 (19%) |
| Over 50 | 0 (0%) | 1 (20%) | 0 (0%) | 1 (3%) | 1 (3%) | 3 (3%) |
| Median | 27.0 | 30.0 | 27.0 | 30.0 | 28.0 | 28.0 |
| Range | 23–45 | 24–54 | 18–45 | 18–51 | 18–54 | 18–54 |
| Vaccination Frequencies | ||||||
| Day 0 (Vaccine 1) | 9 (100%) | 5 (100%) | 20 (100%) | 30 (100%) | 30 (100%) | 94 (100%) |
| Day 28 (Vaccine 2) | 9 (100%) | 5 (100%) | 19 (95%) | 29 (97%) | 30 (100%) | 92 (98%) |
| Day 84 (Vaccine 3) | 9 (100%) | 4 (80%) | 18 (90%) | 27 (90%) | 29 (97%) | 87 (93%) |
| Day 168 (Vaccine 4) | 9 (100%) | 5 (100%) | 16 (80%) | 27 (90%) | 28 (93%) | 85 (90%) |
| Question | Acceptable | Unacceptable | Don’t Know/Don’t Remember |
|---|---|---|---|
| Level of discomfort during vaccination with EP | ID 262/286.92% IM 127/155.82% | ID 22/286.8% IM 22/155.14% | ID 2/286.1% IM 6/155.4% |
| Level of discomfort during the week after vaccination with EP | ID 285/286.100% IM 154/155.99% | ID 1/286.0% IM 1/155.1% | ID 0/286.0% IM 0/155.0% |
| Level of anxiety with EP vaccination | ID 271/286.95% IM 135/155.87% | ID 14/286.5% IM 10/155.6% | ID 1/286.0% IM 10/155.6% |
| Appearance of the injection site | ID 274/286.96% IM 152/155.98% | ID 10/286.3% IM 2/155.1% | ID 2/286.1% IM 1/155.1% |
| Any other side effects experienced from vaccination with EP? a | ID 42/286.15% IM 19/155.12% | ID 1/286.0% IM 1/155.1% | ID 1/286.0% IM 3/155.2% |
| Question | Yes | No | Don’t Know |
|---|---|---|---|
| Would you recommend in the real world if it would feel exactly the same as your experience? | ID 283/286.99% IM 144/155.93% | ID 0/286.0% IM 3/155.2% | ID 3/286.1% IM 8/155.5% |
| Would you recommend in the real world if it would feel more painful than your experience? | ID 203/286.71% IM 77/155.50% | ID 31/286.11% IM 32/155.21% | ID 52/286.18% IM 46/155.30% |
| Would you recommend in the real world if it would leave a mark on the skin lasting for weeks? | ID 280/286.98% IM 149/155.96% | ID 3/286.1% IM 3/155.2% | ID 3/286.1% IM 3/155.2% |
| Would you recommend in the real world if it would leave a permanent scar? | ID 269/286.94% IM 134/155.86% | ID 2/286.1% IM 3/155.2% | ID 15/286.5% IM 18/155.12% |
| Would you recommend in the real world if the vaccine would be 50% effective? | ID 225/286.79% IM 100/155.65% | ID 34/286.12% IM 9/155.6% | ID 27/286.9% IM 46/155.30% |
| Would you recommend in the real world if the vaccine would be 30% effective? | ID 175/286.61% IM 43/155.28% | ID 67/286.23% IM 48/155.31% | ID 44/286.15% IM 64/155.41% |
| Would you recommend in the real world if the person receiving the vaccine is under 16? | ID 213/286.74% IM 68/155.44% | ID 30/286.10% IM 40/155.26% | ID 43/286.15% IM 47/155.30% |
| Would you recommend in the real world if the person is your family member or friend? | ID 280/286.98% IM 147/155.95% | ID 1/286.0% IM 2/155.1% | ID 5/286.2% IM 6/155.4% |
| Would you recommend the vaccine if the person is at low risk for infection? | ID 175/286.61% IM 54/155.35% | ID 62/286.22% IM 52/155.34% | ID 49/286.17% IM 49/155.32% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Edupuganti, S.; C. De Rosa, S.; Elizaga, M.; Lu, Y.; Han, X.; Huang, Y.; Swann, E.; Polakowski, L.; A. Kalams, S.; Keefer, M.; et al. Intramuscular and Intradermal Electroporation of HIV-1 PENNVAX-GP® DNA Vaccine and IL-12 Is Safe, Tolerable, Acceptable in Healthy Adults. Vaccines 2020, 8, 741. https://doi.org/10.3390/vaccines8040741
Edupuganti S, C. De Rosa S, Elizaga M, Lu Y, Han X, Huang Y, Swann E, Polakowski L, A. Kalams S, Keefer M, et al. Intramuscular and Intradermal Electroporation of HIV-1 PENNVAX-GP® DNA Vaccine and IL-12 Is Safe, Tolerable, Acceptable in Healthy Adults. Vaccines. 2020; 8(4):741. https://doi.org/10.3390/vaccines8040741
Chicago/Turabian StyleEdupuganti, Srilatha, Stephen C. De Rosa, Marnie Elizaga, Yiwen Lu, Xue Han, Yunda Huang, Edith Swann, Laura Polakowski, Spyros A. Kalams, Michael Keefer, and et al. 2020. "Intramuscular and Intradermal Electroporation of HIV-1 PENNVAX-GP® DNA Vaccine and IL-12 Is Safe, Tolerable, Acceptable in Healthy Adults" Vaccines 8, no. 4: 741. https://doi.org/10.3390/vaccines8040741
APA StyleEdupuganti, S., C. De Rosa, S., Elizaga, M., Lu, Y., Han, X., Huang, Y., Swann, E., Polakowski, L., A. Kalams, S., Keefer, M., Maenza, J., C. Wise, M., Yan, J., Morrow, M. P., Khan, A. S., Boyer, J. D., Humeau, L., White, S., Sardesai, N. Y., ... the NIAID-Funded HIV Vaccine Trials Network. (2020). Intramuscular and Intradermal Electroporation of HIV-1 PENNVAX-GP® DNA Vaccine and IL-12 Is Safe, Tolerable, Acceptable in Healthy Adults. Vaccines, 8(4), 741. https://doi.org/10.3390/vaccines8040741