Current Clinical Trials Protocols and the Global Effort for Immunization against SARS-CoV-2


 , ,
, ,  , ,
, , 
Abstract
1. Introduction
2. Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction, Data Collection, and Risk of Bias Assessment
2.4. Data Analysis
3. Results
3.1. Study Selection
3.2. Overview of Clinical Trial Protocols for Active Immunization for Covid-19
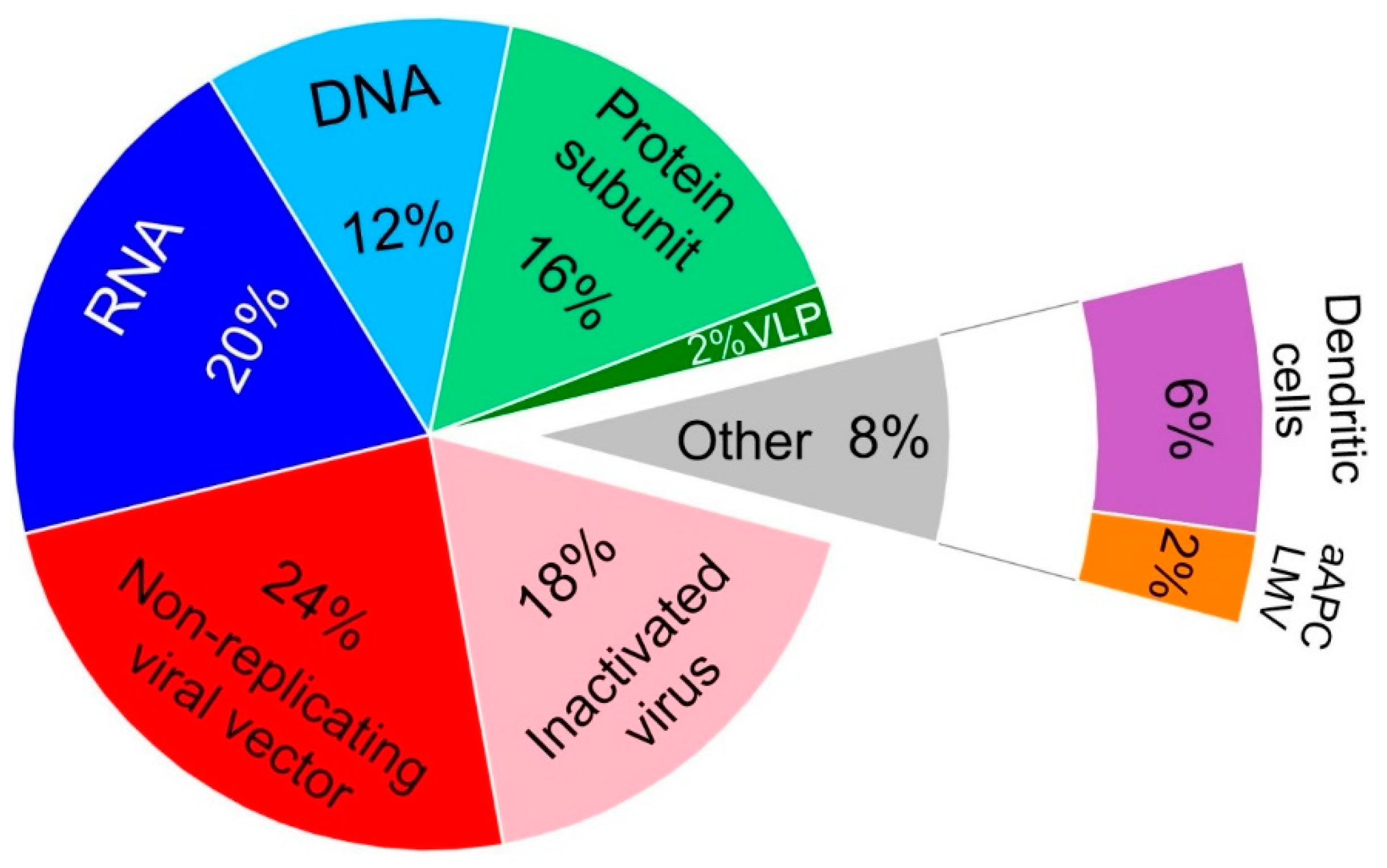
3.3. Properties and Features of Vaccines against COVID-19
3.3.1. Nucleic Acid Vaccines
RNA Vaccines
DNA Vaccines
3.3.2. Non-Replicating Viral Vector Vaccines
3.3.3. Inactivated Virus Vaccines
3.3.4. Protein Subunit Vaccines
3.3.5. Dendritic Cells Vaccines
3.3.6. Virus Like Particles Vaccines
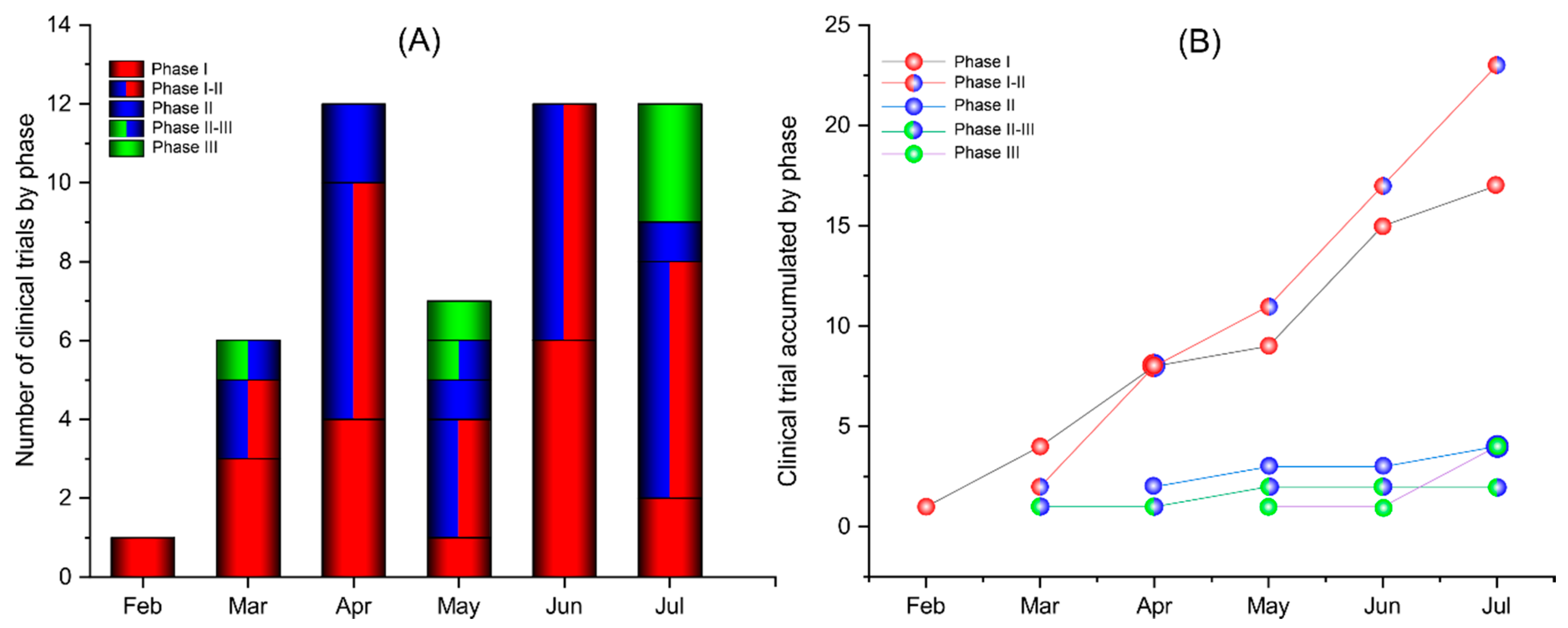
3.4. Trial Progression Rate
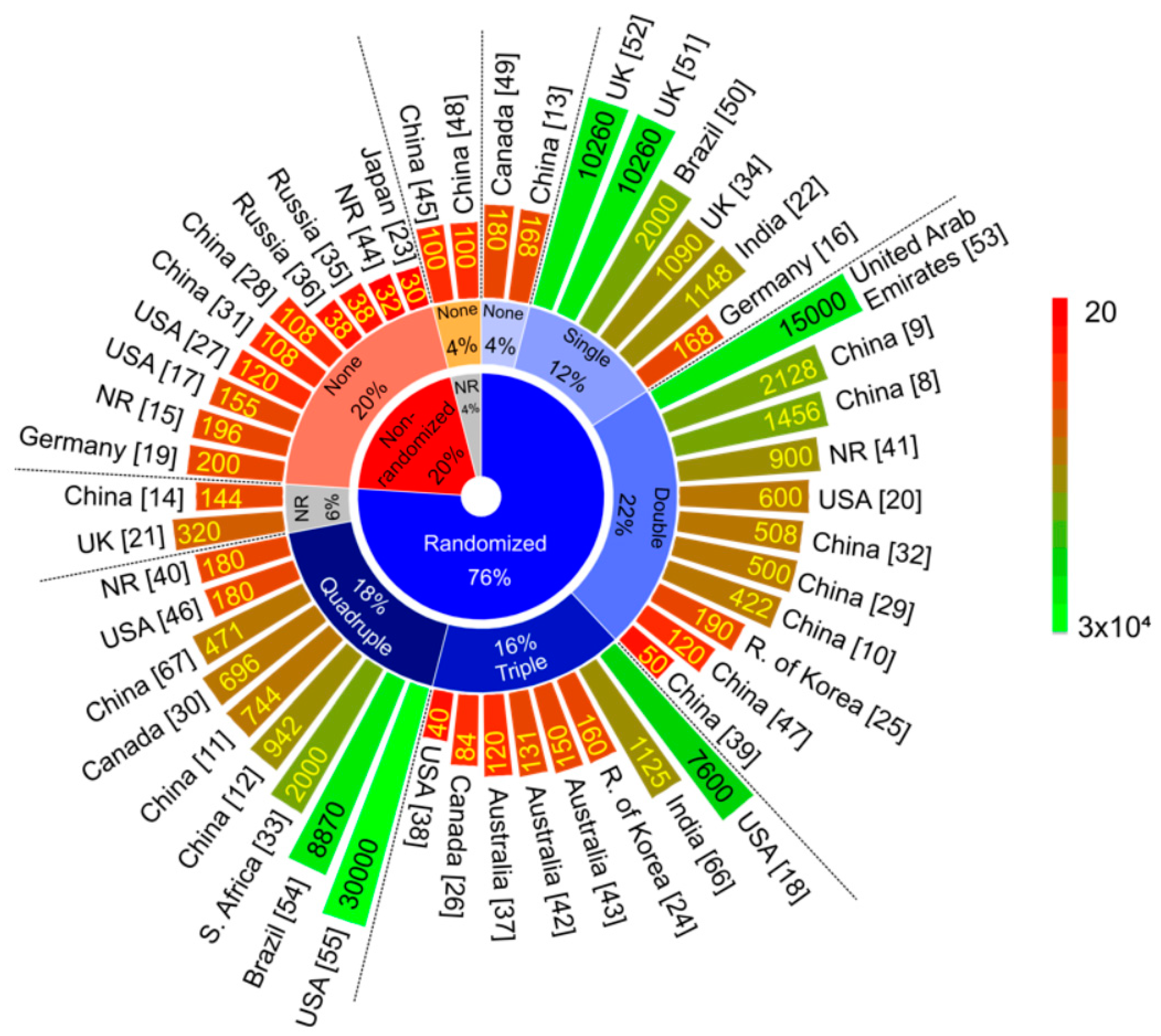
3.5. Study Design of Clinical Trial Protocols
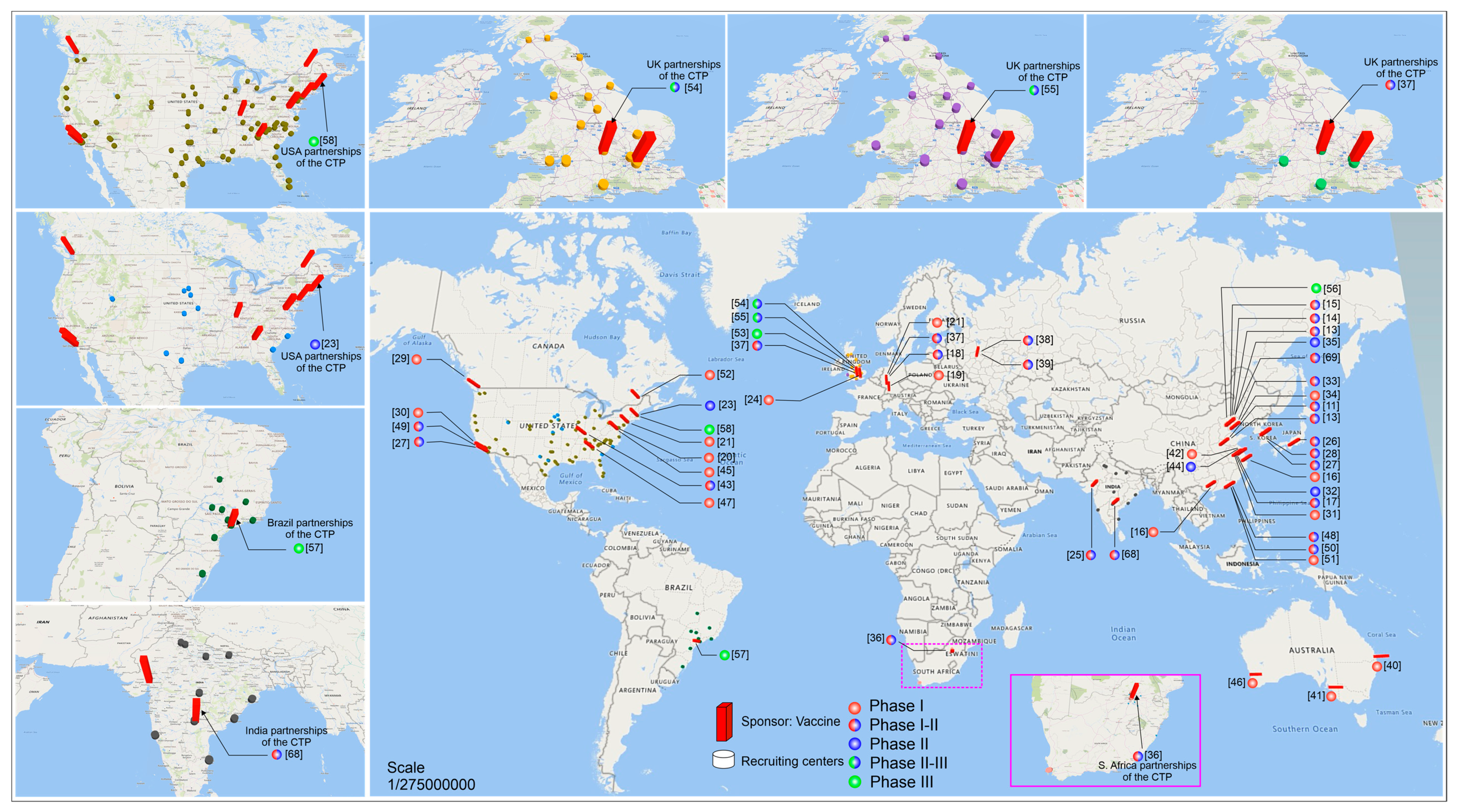
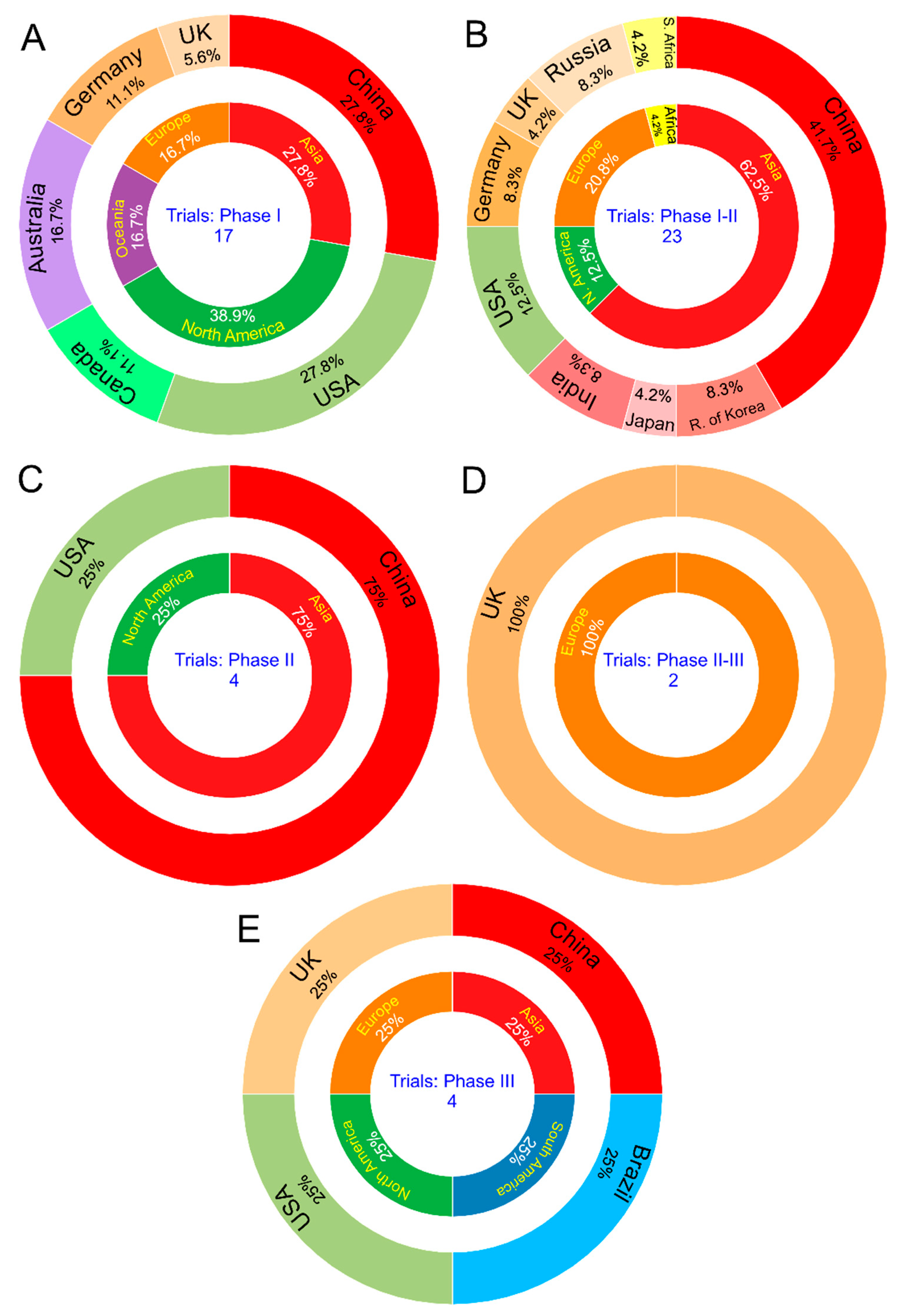
3.6. Global Research Network in Clinical Trial Protocols
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ID Number | Phase | Rehearsal Center | Sponsor | Recruiting Centers | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Name | City | Country | Region | Name | City | Country | Region | |||
| ISRCTN89951424 [50] | III | Single center | University of Oxford (AstraZeneca) | Oxford | United Kingdom | Europe | UNIFESP | Sao Paulo | Brazil | South America |
| NCT04456595 [54] | III | Multicenter | Butantan Institute (Sinovac Life Sciences Co., Ltd./) | Sao Paulo | Brazil | South America | University of Brasilia | Brasilia | Brazil | South America |
| Federal University of Minas Gerais | Belo Horizonte | |||||||||
| Hospital das Clínicas, Federal University of Paraná | Curitiba | |||||||||
| Hospital São Lucas da Pontificia Universidade Catolica do Rio Grande do Sul | Porto Alegre | |||||||||
| Hospital das Clínicas da UNICAMP | Campinas | |||||||||
| Hospital das Clínicas, Faculty of Medicine of Ribeirão Preto, University of São Paulo | Ribeirão Preto | |||||||||
| Emílio Ribas Institute of Infectious Diseases | São Paulo | |||||||||
| Clinical Research Center of the Central Institute of Hospital das Clínicas, Faculty of Medicine, University of São Paulo | ||||||||||
| Israeli Institute of Education and Research Albert Einstein | ||||||||||
| Municipal University of São Caetano do Sul | São Caetano do Sul | |||||||||
| Medical School of São José do Rio Preto—FAMERP | São José do Rio Preto | |||||||||
| Instituto de Infectologia Evandro Chagas—Fiocruz | Rio de Janeiro | |||||||||
| ChiCTR2000034780 [53] | III | Single center | China National Biotec Group Co. Ltd. | Beijing | China | Asia | Shaikh kahlifa Medical City | Abu Dhabi | United Arab Emirates | Asia |
| NCT04470427 [55] | III | Multicenter | ModernaTX, Inc. | Cambridge | USA | North America | Ascension St. Vincent Birmingham | Birmingham | USA | North America |
| Hope Research Institute | Chandler | |||||||||
| Peoria | ||||||||||
| Phoenix | ||||||||||
| Quality of Life Medical and Research Center | Tucson | |||||||||
| Baptist Health Center for Clinical Research | Little Rock | |||||||||
| Advanced Clinical Research—Rancho Paseo | Banning | |||||||||
| University of California San Diego | La Jolla | |||||||||
| eStudySite - La Mesa | La Mesa | |||||||||
| UCLA Vine Street Clinic CRS | Los Angeles | |||||||||
| Paradigm Clinical Research Institute Inc | Redding | |||||||||
| Benchmark Research—Sacramento | Sacramento | |||||||||
| Medical Center For Clinical Research | San Diego | |||||||||
| University of Colorado Hospital | Aurora | |||||||||
| Lynn Institute of The Rockies | Colorado Springs | |||||||||
| George Washington University | Washington | |||||||||
| Accel Research Site | DeLand | |||||||||
| Research Centers of America | Hollywood | |||||||||
| Jacksonville Center for Clinical Research | Jacksonville | |||||||||
| Suncoast Research Group | Miami | |||||||||
| University of Miami | ||||||||||
| Palm Beach Research Center | West Palm Beach | |||||||||
| Grady Health System | Atlanta | |||||||||
| Children’s Healthcare of Atlanta | ||||||||||
| Hope Clinic of The Emory Vaccine Center | Decatur | |||||||||
| Meridian Clinical Research | Savannah | |||||||||
| Clinical Research Atlanta | Stockbridge | |||||||||
| UIC Project WISH CRS | Chicago | |||||||||
| Johnson County Clin-Trials | Lenexa | |||||||||
| Alliance for Multispecialty Research | Newton | |||||||||
| Alliance for Multispecialty Research- East Wichita | Wichita | |||||||||
| Meridian Clinical Research | Baton Rouge | |||||||||
| Benchmark Research - Metairie | Metairie | |||||||||
| University of Maryland School of Medicine | Baltimore | |||||||||
| Meridian Clinical Research | Rockville | |||||||||
| Brigham and Women’s Hospital | Boston | |||||||||
| Henry Ford Health System | Detroit | |||||||||
| MediSync Clinical Research Hattiesburg Clinic | Petal | |||||||||
| Saint Louis University | Saint Louis | |||||||||
| Sundance Clinical Research | ||||||||||
| Meridian Clinical Research | Grand Island | |||||||||
| Norfolk | ||||||||||
| Omaha | ||||||||||
| Clinical Research Center of Nevada | Las Vegas | |||||||||
| AB Clinical Trials | ||||||||||
| Hackensack University Medical Center | Hackensack | |||||||||
| New Jersey Medical School | Newark | |||||||||
| Meridian Clinical Research | Binghamton | |||||||||
| Weill Cornell Chelsea | New York | |||||||||
| Weill Cornell Medical College | ||||||||||
| University of North Carolina at Chapel Hill | Chapel Hill | |||||||||
| Tryon Medical Partners | Charlotte | |||||||||
| Carolina Institute for Clinical Research | Fayetteville | |||||||||
| M3 Wake Research, Inc—M3 Wake | Raleigh | |||||||||
| Trial Management Associates | Wilmington | |||||||||
| Wake Forest University Health Sciences | Winston-Salem | |||||||||
| New Horizons Clinical Research | Cincinnati | |||||||||
| Cincinnati CRS | ||||||||||
| Rapid Medical Research Inc | Cleveland | |||||||||
| Lynn Health Science Institute | Oklahoma | |||||||||
| Crisor | Medford | |||||||||
| Penn Prevention CRS | Philadelphia | |||||||||
| UPMC University Center | Pittsburgh | |||||||||
| Keystone VitaLink Research | Anderson | |||||||||
| Greenville | ||||||||||
| Spartanburg | ||||||||||
| Coastal Carolina Research Center | Mount Pleasant | |||||||||
| Meridian Clinical Research | Dakota Dunes | |||||||||
| WR-ClinSearch | Chattanooga | |||||||||
| Alliance for Multispecialty Research | Knoxville | |||||||||
| Vanderbilt University Medical Center | Nashville | |||||||||
| Benchmark Research | Austin | |||||||||
| Tekton Research | ||||||||||
| Advanced Clinical Research—Be Well MD | Cedar Park | |||||||||
| Global Medical Research—M3 Wake Research | Dallas | |||||||||
| Benchmark Research | Fort Worth | |||||||||
| University of Texas Medical Branch | Galveston | |||||||||
| Baylor College of Medicine | Houston | |||||||||
| DM Clinical Research—Texas Center For Drug Development | ||||||||||
| Laguna Clinical Research | Laredo | |||||||||
| Centex Studies | McAllen | |||||||||
| Benchmark Research | San Angelo | |||||||||
| Clinical Trials of Texas, Inc | San Antonio | |||||||||
| DM Clinical Research | Tomball | |||||||||
| Foothill Family Clinic - North | Salt Lake City | |||||||||
| Foothill Family Clinic-South Clinic | ||||||||||
| Kaiser Permanente | Seattle | |||||||||
| NCT04400838 [51] | II-III | Multicenter | University of Oxford (AstraZeneca) | Oxford | United Kingdom | Europe | University Hospital Southampton NHS Foundation Trust | Southampton | United Kingdom | Europe |
| St Georges University Hospital NHS Foundation Trust | London | |||||||||
| University Hospitals Birmingham NHS Foundation Trust | Birmingham | |||||||||
| University Hospitals Bristol and Weston NHS Foundation Trust | Bristol | |||||||||
| North Bristol NHS Trust | Bristol | |||||||||
| NIHR Cambridge Clinical Research Facility | Cambridge | |||||||||
| Public Health Wales | Cardiff | |||||||||
| Castle Hill Hospital | Cottingham | |||||||||
| NHS Lothian, Western General Hospital | Edinburgh | |||||||||
| Glasgow University and NHS Greater Glasgow & Clyde, New Lister Building, Glasgow Royal Infirmary & Queen Elizabeth University Hospital | Glasgow | |||||||||
| Liverpool School of Tropical Medicine (LSTM), Accelerator Research Clinic. Clinical Sciences Accelerator | Liverpool | |||||||||
| London North West University Healthcare Trust (LNWUH), Northwick Park Hospital | London | |||||||||
| University College London Hospitals NHS Foundation Trust | London | |||||||||
| Guy’s and St Thomas’ NHS Foundation Trust, Department of Infection, St Thomas Hospital | London | |||||||||
| Imperial College Healthcare NHS Trust | London | |||||||||
| The Newcastle upon Tyne Hospitals NHS Foundation Trust, Royal Victoria Infirmary | Newcastle | |||||||||
| University of Nottingham Health Service, Cripps Health Centre, University Park | Nottingham | |||||||||
| CCVTM, University of Oxford, Churchill Hospital | Oxford | |||||||||
| John Radcliffe Hospital | Oxford | |||||||||
| Sheffield Teaching Hospitals, Royal Hallamshire Hospital | Sheffield | |||||||||
| EudraCT2020-001228-32 ISRCTN90906759 [52] | II-III | Multicenter | University of Oxford (AstraZeneca) | Oxford | United Kingdom | Europe | Centre for Clinical Vaccinology & Tropical Medicine | Oxford | United Kingdom | Europe |
| University Hospital Southampton NHS Foundation Trust | Southampton | |||||||||
| NIHR Imperial Clinical Research Facility | London | |||||||||
| St Georges University Hospital NHS Foundation Trust | London | |||||||||
| University Hospitals Bristol and Weston NHS Foundation Trust | Bristol | |||||||||
| North Bristol NHS Trust | Bristol | |||||||||
| University of Nottingham Health Service | Nottingham | |||||||||
| Sheffield Teaching Hospitals | Sheffield | |||||||||
| University Hospitals Birmingham NHS Foundation Trust (UHB) | Birmingham | |||||||||
| Wales (Public Health Wales) | Newport | |||||||||
| Greater Glasgow and Clyde NHS Board | Glasgow | |||||||||
| Guy’s and St Thomas’ NHS Foundation Trust | London | |||||||||
| Liverpool School of Tropical Medicine | Liverpool | |||||||||
| The Newcastle upon Tyne Hospitals NHS Foundation Trust | Newcastle upon Tyne | |||||||||
| University College London Hospital (UCLH) | London | |||||||||
| NHS Lothian | Edinburgh | |||||||||
| NIHR Cambridge Clinical Research Facility | Cambridge | |||||||||
| Oxford University Hospital Foundation Trust | Oxford | |||||||||
| Nottingham University Hospitals NHS Trust | Nottingham | |||||||||
| Hull University Teaching Hospitals NHS Trust (HUTH) | Hull | |||||||||
| Northwick Park Hospital | London | |||||||||
| NCT04405076 [20] | II | Multicenter | ModernaTX, Inc. | Cambridge | USA | North America | Meridian Clinical Research | Savannah | USA | North America |
| Heartland Research Associates | Newton | |||||||||
| Heartland Research Associates | Kansas City | |||||||||
| Meridian Clinical Research | Norfolk | |||||||||
| Meridian Clinical Research | Omaha | |||||||||
| Trial Management Associates | Wilmington | |||||||||
| Meridian Clinical Research | Dakota Dunes | |||||||||
| Benchmark Research | Austin | |||||||||
| Benchmark Research | San Angelo | |||||||||
| Advanced Clinical Research/Velocity | West Jordan | |||||||||
| NCT04341389 [32] | II | Single center | Institute of Biotechnology, Academy of Military Medical Sciences, PLA of China | Shanghai | China | Asia | Hubei Provincial Center for Disease Control and Prevention | Wuhan | China | Asia |
| ChiCTR2000031781 [29] | II | Multicenter | Jiangsu Provincial Center for Disease Control and Prevention (CanSino Biological Inc.) | Nanjing | China | Asia | Wuhan Rest Center, Chinese People’s Armed Police Force | Wuhan | China | Asia |
| Hubei Provincial Center for Disease Control and Prevention | ||||||||||
| Zhongnan Hospital of Wuhan University | ||||||||||
| NCT04466085 [41] | II | NR | Anhui Zhifei Longcom Biologic Pharmacy Co., Ltd. | Beijing | China | Asia | NR | NR | NR | NR |
| NCT04445389 [25] | I, II | Single center | Genexine, Inc. | Seongnam | Republic of Korea | Asia | Severance hospital | Seoul | Republic of Korea | Asia |
| NCT04444674 [33] | I, II | Multicenter | University of Witwatersrand | Johannesburg | South Africa | Africa | PHRU Kliptown | Johannesburg | South Africa | Africa |
| Wits RHI Shandukani Research Center | ||||||||||
| Setshaba Research Centre (SRC) | Soshanguve | |||||||||
| Chris Hani Baragwanath Academic Hospital—DST/NRF VPD RMPRU | Soweto | |||||||||
| FAMCRU | Cape Town | |||||||||
| Groote Schuur hospital, Lung infection and immunity unit, UCT | ||||||||||
| NCT04437875 [36] | I, II | Single center | Gamaleya Research Institute of Epidemiology and Microbiology, Health Ministry of the Russian Federation | Moscow | Russia | Europe | Sechenov First Moscow State Medical University | Moscow | Russia | Europe |
| NCT04436471 [35] | I, II | Single center | Gamaleya Research Institute of Epidemiology and Microbiology, Health Ministry of the Russian Federation | Moscow | Russia | Europe | Main military clinical hospital named after academician N. N. Burdenko | Moscow | Russia | Europe |
| NCT04412538 [12] | I, II | Single center | Chinese Academy of Medical Sciences | Beijing | China | Asia | West China Second University Hospital | Sichuan | China | Asia |
| NCT04398147 [30] | I, II | Single center | CanSino Biologics Inc. | Tianjin | China | Asia | Canadian Center for Vaccinology | Halifax | Canada | North America |
| NCT04386252 [46] | I, II | Single center | Aivita Biomedical, Inc. | Irvine | USA | North America | Hoag Memorial Hospital Presbyterian | Newport Beach | USA | North America |
| NCT04383574 [10] | I, II | Single center | Sinovac Research and Development Co. Ltd. | Beijing | China | Asia | Renqiu City Center for Disease Control and Prevention | Renqiu | China | Asia |
| NCT04380701 [19] | I, II | Single center | Biontech RNA Pharmaceuticals GmbH | Berlin | Germany | Europe | Contract Research Organization | Berlin | Germany | Europe |
| NCT04352608 [11] | I, II | Single center | Sinovac Research and Development Co. Ltd. | Beijing | China | Asia | Suining County Center for Disease Control and Prevention | Xuzhou | China | Asia |
| NCT04324606 EudraCT2020-001072-15 [34] | I, II | Multicenter | University of Oxford (AstraZeneca) | Oxford | United Kingdom | Europe | University Hospital Southampton NHS Foundation Trust | Southampton | United Kingdom | Europe |
| University Hospitals Bristol and Weston NHS Foundation Trust | Bristol | |||||||||
| St Georges University Hospital NHS Foundation Trust | London | |||||||||
| Imperial College Healthcare NHS Trust | London | |||||||||
| CCVTM, University of Oxford, Churchill Hospital | Oxford | |||||||||
| John Radcliffe Hospital | Oxford | |||||||||
| NCT04276896 [45] | I, II | Multicenter | Shenzhen Geno-Immune Medical Institute | Shenzhen | China | Asia | Shenzhen Geno-Immune Medical Institute | Shenzhen | China | Asia |
| Shenzhen Third People’s Hospital | ||||||||||
| Shenzhen Second People’s Hospital | ||||||||||
| ChiCTR2000032459 [9] | I, II | Single-center | Henan Provincial Center for Disease Control and Prevention (Sinopharm) | Zhengzhou | China | Asia | Liangyuan district centers for disease control and prevention | Shangqiu | China | Asia |
| ChiCTR2000031809 [8] | I, II | Multicenter | Henan Provincial Center for Disease Control and Prevention (Sinopharm) | Zhengzhou | China | Asia | Wuzhi County Center for Disease Control and Prevention | Jiaozuo | China | Asia |
| People’s hospital, Wuzhi county | ||||||||||
| ChiCTR2000030750 [47] | I, II | Multicenter | Shenzhen Third People’s Hospital | Shenzhen | China | Asia | Shenzhen Third People’s Hospital | Shenzhen | China | Asia |
| Shenzhen People’s Hospital | ||||||||||
| EudraCT 2020-001038-36 [15] | I, II | Multicenter | BioNTech RNA Pharmaceuticals GmbH (Fosun Pharma/Pfizer) | Mainz | Germany | Europe | NR | NR | NR | NR |
| NCT04447781 [24] | I, II | Single center | International Vaccine Institute | Seoul | Republic of Korea | Asia | Seoul National University Hospital | Seoul | Republic of Korea | Asia |
| Inovio Pharmaceuticals | San Diego | USA | North America | |||||||
| NCT04463472 [23] | I, II | Single center | AnGes, Inc. | Osaka | Japan | Asia | Osaka City University Hospital | Osaka | Japan | Asia |
| CTRI/2020/07/026352 [22] | I, II | Single center | Cadila Healthcare Ltd. | Ahmedabad | India | Asia | Zydus Research Center | Ahmedabad | India | Asia |
| CTRI/2020/07/026300 NCT04471519 [66] | I, II | Multicenter | Bharat Biotech International Ltd., | Medchal | India | Asia | All India Institute of Medical Sciences | Patna | India | Asia |
| New Delhi | ||||||||||
| Gillukar Multispeciality Hospital | Nagpur | |||||||||
| Institute of Medical Sciences and SUM Hospital | Jajapur | |||||||||
| Jeevan Rekha Hospital | Begaum | |||||||||
| King George Hospital | Visakhapatnam | |||||||||
| Nizam’s Institute of Medical Sciences | Hyderabad | |||||||||
| PGIMS | Rohtak | |||||||||
| Prakhar Hospital | Knapur Nagar | |||||||||
| Rana Hospital and Trauma Center | Gorakhpur | |||||||||
| Redkar Hospital and Research Center | North Goa | |||||||||
| SRM Hospital & Research Center | Kancheepuram | |||||||||
| NCT04470609 [67] | I, II | Multicenter | Chinese Academy of Medical Sciences | Beijing | China | Asia | West China Second University Hospital | Sichuan | China | Asia |
| West China women’s and children’s Hospital | ||||||||||
| NCT04473690 [40] | I, II | NR | Kentucky BioProcessing, Inc. | Owensboro | USA | North America | NR | NR | NR | NR |
| ChiCTR2000034825 [14] | I, II | Multicenter | Jiangsu Provincial Center for Disease Prevention and Control | Nanjung | China | Asia | China Medical City, the Vaccine Engineering Center | Jiangsu | China | Asia |
| Taizhou Center for Disease Control and Prevention | ||||||||||
| Taizhou People’s Hospital | ||||||||||
| NCT04449276 2020-001286-36 [16] | I | Single center | CureVac AG | Tübingen | Germany | Europe | University Hospital Tübingen Institut für Tropenmedizin | Tübingen | Germany | Europe |
| NCT04405908 [43] | I | Single center | Clover Biopharmaceuticals AUS Pty Ltd. (GSK/Dynavax) | Perth | Australia | Oceania | Linear Clinical Research Ltd. | Nedlands | Australia | Oceania |
| NCT04334980 [26] | I | Multicenter | Symvivo Corporation | British Columbia | Canada | North America | Vaccine Evaluation Center, BC Children’s Hospital Research Institute, University of British Columbia | Vancouver | Canada | North America |
| Canadian Center for Vaccinology Dalhousie University, IWK Health Centre | Halifax | |||||||||
| NCT04313127 [31] | I | Single center | CanSino Biologics Inc. | Tianjin | China | Asia | Hubei Provincial Center for Disease Control and Prevention | Wuhan | China | Asia |
| NCT04299724 [48] | I | Single center | Shenzhen Geno-Immune Medical Institute | Shenzhen | China | Asia | Shenzhen Geno-Immune Medical Institute | Shenzhen | China | Asia |
| NCT04283461 [17] | I | Multicenter | National Institute of Allergy and Infectious Diseases (NIAID) (ModernaTX, Inc.) | Bethesda | USA | North America | Emory Vaccine Center—The Hope Clinic | Decatur | USA | North America |
| National Institutes of Health - Clinical Center - Vaccine Research Center Clinical Trials Program | Bethesda | |||||||||
| Kaiser Permanente Washington Health Research Institute—Vaccines and Infectious Diseases | Seattle | |||||||||
| NCT04428073 [44] | I | Single center | GeneCure Biotechnologies | Nercross | USA | North America | NR | NR | NR | NR |
| ChiCTR2000034112 [13] | I | Multicenter | Shulan (Hangzhou) Hospital; | Hangzhou | China | Asia | Shulan (Hangzhou) Hospital | Hangzhou | China | Asia |
| Center for Disease Control and Prevention of Guangxi Zhuang Autonomous Region | Beijing | Yongfu County Center for Disease Control and Prevention | NR | |||||||
| ChiCTR2000030906 [28] | I | Multicenter | Jiangsu Provincial Center for Disease Control and Prevention (CanSino Biological Inc.) | Nanjing | China | Asia | Wuhan Rest Center, Chinese People’s Armed Police Force | Wuhan | China | Asia |
| Tongji Hospital | ||||||||||
| NCT04445194 [39] | I | Single center | Anhui Zhifei Longcom Biologic Pharmacy Co., Ltd. | Beijing | China | Asia | The Second Affiliated Hospital of Chongqing Medical University | Chongqing | China | Asia |
| NCT04453852 [38] | I | Single center | Vaxine Pty Ltd./Medytox | Adelaide | Australia | Oceania | PARC Clinical Research | Adelaide | Australia | Oceania |
| ACTRN12620000674932 [37] | I | Single center | Univerty of Queensland/CSL/Seqirus | St Lucia | Australia | Oceania | Q-Pharm Pty—Clive Berghofer Research Centre (CBCRC) | Herston | Australia | Oceania |
| ISRCTN17072692 [21] | I | Multicenter | Imperial College London | London | United Kingdom | Europe | NIHR Imperial Clinical Research Facility | London | United Kingdom | Europe |
| Surrey Clinical Research Facility | Surrey | |||||||||
| University Hospital Southampton | Hampshire | |||||||||
| St. George’s Hospital | London | |||||||||
| NCT04450004 [49] | I | Multicenter | Medicago Inc. | Quebec | Canada | North America | Syneos Health | Montreal | Canada | North America |
| Quebec | ||||||||||
| NCT04368988 [42] | I | Multicenter | Novavax, Inc. | Maryland | USA | North America | Investigational Research Site 1 | Herston | Australia | Oceania |
| Investigational Research Site 2 | Melbourne | |||||||||
| NCT04368728 [18] | I | Multicenter | Biontech SE | Berlin | Germany | Europe | University of Maryland, Center for Vaccine Development and Global Health | Baltimore | USA | North America |
| NYU Langone Health | New York | |||||||||
| Pfizer (Fosun Pharma) | New York | USA | North America | Rochester Regional Health/Rochester General Hospital | Rochester | |||||
| Cincinnati Children’s Hospital Medical Center | Cincinnati | |||||||||
| NCT04336410 [27] | I | Multicenter | Inovio Pharmaceuticals | San Diego | USA | North America | Central Kentucky Research Associates | Lexington | USA | North America |
| Center for Pharmaceutical Research | Kansas City | |||||||||
| University of Pennsylvania | Philadelphia | |||||||||
References
- Hamed, M.A. An overview on COVID-19: Reality and expectation. Bull. Natl. Res. Cent. 2020, 44, 86. [Google Scholar] [CrossRef] [PubMed]
- Worldometer. COVID-19 Pandemic Data Update. 2020. Available online: https://www.worldometers.info/coronavirus/ (accessed on 27 July 2020).
- Zhu, F.C.; Guan, X.H.; Li, Y.H.; Huang, J.Y.; Jiang, T.; Hou, L.H.; Li, J.X.; Yang, B.F.; Wang, L.; Wang, W.J.; et al. Immunogenicity and safety of a recombinant adenovirus type-5-vectored COVID-19 vaccine in healthy adults aged 18 years or older: A randomised, double-blind, placebo-controlled, phase 2 trial. Lancet 2020. [Google Scholar] [CrossRef]
- Zhang, T.; He, Y.; Xu, W.; Ma, A.; Yang, Y.; Xu, K.F. Clinical trials for the treatment of Coronavirus disease 2019 (COVID-19): A rapid response to urgent need. Sci. China Life Sci. 2020, 63, 774–776. [Google Scholar] [CrossRef]
- Md Insiat Islam, R. Current Drugs with Potential for Treatment of COVID-19: A Literature Review. J. Pharm. Pharm. Sci. 2020, 23, 58–64. [Google Scholar] [CrossRef]
- Savioli, F. Is there a rationale for heparin use among severe COVID-19 patients? Einstein 2020, 18, eED5758. [Google Scholar] [CrossRef]
- Osama El-Gendy, A.; Saeed, H.; Ali, A.M.A.; Zawbaa, H.M.; Gomaa, D.; Harb, H.S.; Madney, Y.M.; Osama, H.; Abdelrahman, M.A.; Abdelrahim, M.E.A. Bacillus Calmette–Guérin vaccine, antimalarial, age and gender relation to COVID-19 spread and mortality. Vaccine 2020, 38, 5564–5568. [Google Scholar] [CrossRef] [PubMed]
- ChiCTR2000031809. A Randomized, Double-Blind, Placebo Parallel-Controlled Phase I/II Clinical Trial for Inactivated Novel Coronavirus Pneumonia Vaccine (Vero Cells). 2020. Available online: http://www.chictr.org.cn/hvshowproject.aspx?id=27698 (accessed on 27 July 2020).
- ChiCTR2000032459. A Phase I/II Clinical Trial for Inactivated Novel Coronavirus (2019-CoV) Vaccine (Vero Cells). 2020. Available online: http://www.chictr.org.cn/showprojen.aspx?proj=53003 (accessed on 27 July 2020).
- Safety and Immunogenicity Study of Inactivated Vaccine for Prevention of SARS-CoV-2 Infection(COVID-19). 2020. Available online: https://ClinicalTrials.gov/show/NCT04383574 (accessed on 27 July 2020).
- Safety and Immunogenicity Study of Inactivated Vaccine for Prophylaxis of SARS CoV-2 Infection (COVID-19). 2020. Available online: https://ClinicalTrials.gov/show/NCT04352608 (accessed on 27 July 2020).
- Safety and Immunogenicity Study of an Inactivated SARS-CoV-2 Vaccine for Preventing Against COVID-19. 2020. Available online: https://ClinicalTrials.gov/show/NCT04412538 (accessed on 27 July 2020).
- ChiCTR2000034112. A Phase I Clinical Trial to Evaluate the Safety, Tolerance and Preliminary Immunogenicity of Different Doses of a SARS-CoV-2 mRNA Vaccine in Population Aged 18-59 Years and 60 Years and Above. 2020. Available online: http://www.chictr.org.cn/hvshowproject.aspx?id=40018 (accessed on 27 July 2020).
- ChiCTR2000034825. A Phase I clinical trial of novel coronavirus pneumonia (COVID-19) mRNA Vaccine (BNT162b1) in China 2020. 2020. Available online: http://www.chictr.org.cn/showprojen.aspx?proj=56834 (accessed on 27 July 2020).
- EUCTR 2020-001038-36-DE. Study to Investigate the Safety and Effects of Vaccines in Healthy Adults. 2020. Available online: https://www.clinicaltrialsregister.eu/ctr-search/search?query=eudract_number:2020-001038-36 (accessed on 27 July 2020).
- A Study to Evaluate the Safety, Reactogenicity and Immunogenicity of Vaccine CVnCoV in Healthy Adults. 2020. Available online: https://ClinicalTrials.gov/show/NCT04449276 (accessed on 27 July 2020).
- Safety and Immunogenicity Study of 2019-nCoV Vaccine (mRNA-1273) for Prophylaxis of SARS-CoV-2 Infection (COVID-19). 2020. Available online: https://ClinicalTrials.gov/show/NCT04283461 (accessed on 27 July 2020).
- Study to Describe the Safety, Tolerability, Immunogenicity, and Potential Efficacy of RNA Vaccine Candidates Against COVID-19 in Healthy Adults. 2020. Available online: https://ClinicalTrials.gov/show/NCT04368728 (accessed on 27 July 2020).
- A Trial Investigating the Safety and Effects of Four BNT162 Vaccines Against COVID-2019 in Healthy Adults. 2020. Available online: https://ClinicalTrials.gov/show/NCT04380701 (accessed on 27 July 2020).
- Dose-Confirmation Study to Evaluate the Safety, Reactogenicity, and Immunogenicity of mRNA-1273 COVID-19 Vaccine in Adults Aged 18 Years and Older. 2020. Available online: https://ClinicalTrials.gov/show/NCT04405076 (accessed on 27 July 2020).
- ISRCTN17072692. Clinical Trial to Assess the Safety of a Coronavirus Vaccine in Healthy Men and Women. 2020. Available online: http://www.isrctn.com/ISRCTN17072692 (accessed on 27 July 2020).
- CTRI/2020/07/026352. Novel Corona Virus-2019-nCov Vaccine by Intradermal Route in Healthy Subjects. 2020. Available online: http://www.ctri.nic.in/Clinicaltrials/pmaindet2.php?trialid=45306 (accessed on 27 July 2020).
- Study of COVID-19 DNA Vaccine (AG0301-COVID19). 2020. Available online: https://ClinicalTrials.gov/show/NCT04463472 (accessed on 27 July 2020).
- Safety, Tolerability and Immunogenicity of INO-4800 Followed by Electroporation in Healthy Volunteers for COVID19. 2020. Available online: https://ClinicalTrials.gov/show/NCT04447781 (accessed on 27 July 2020).
- Safety and Immunogenicity Study of GX-19, a COVID-19 Preventive DNA Vaccine in Healthy Adults. 2020. Available online: https://ClinicalTrials.gov/show/NCT04445389 (accessed on 27 July 2020).
- Evaluating the Safety, Tolerability and Immunogenicity of bacTRL-Spike Vaccine for Prevention of COVID-19. 2020. Available online: https://ClinicalTrials.gov/show/NCT04334980 (accessed on 27 July 2020).
- Safety, Tolerability and Immunogenicity of INO-4800 for COVID-19 in Healthy Volunteers. 2020. Available online: https://ClinicalTrials.gov/show/NCT04336410 (accessed on 27 July 2020).
- ChiCTR2000030906. A Phase I Clinical Trial for Recombinant Novel Coronavirus (2019-COV) Vaccine (Adenoviral Vector). 2020. Available online: http://www.chictr.org.cn/hvshowproject.aspx?id=24074 (accessed on 27 July 2020).
- ChiCTR2000031781. A Randomized, Double-Blinded, Placebo-Controlled Phase II Clinical Trial for Recombinant Novel Coronavirus (2019-nCOV) Vaccine (Adenovirus Vector). 2020. Available online: http://www.chictr.org.cn/showprojen.aspx?proj=52006 (accessed on 27 July 2020).
- Phase I/II Clinical Trial of Recombinant Novel Coronavirus Vaccine (Adenovirus Type 5 Vector) in Canada. 2020. Available online: https://ClinicalTrials.gov/show/NCT04398147 (accessed on 27 July 2020).
- Phase I Clinical Trial of a COVID-19 Vaccine in 18-60 Healthy Adults. 2020. Available online: https://ClinicalTrials.gov/show/NCT04313127 (accessed on 27 July 2020).
- A Phase II Clinical Trial to Evaluate the Recombinant Vaccine for COVID-19 (Adenovirus Vector). 2020. Available online: https://ClinicalTrials.gov/show/NCT04341389 (accessed on 27 July 2020).
- COVID-19 Vaccine (ChAdOx1 nCoV-19) Trial in South African Adults With and Without HIV-infection. 2020. Available online: https://ClinicalTrials.gov/show/NCT04444674 (accessed on 27 July 2020).
- A Study of a Candidate COVID-19 Vaccine (COV001). 2020. Available online: https://ClinicalTrials.gov/show/NCT04324606 (accessed on 27 July 2020).
- Development. An Open Study of the Safety, Tolerability and Immunogenicity of the Drug “Gam-COVID-Vac” Vaccine Against COVID-19. 2020. Available online: https://ClinicalTrials.gov/show/NCT04436471 (accessed on 27 July 2020).
- Development. An Open Study of the Safety, Tolerability and Immunogenicity of “Gam-COVID-Vac Lyo” Vaccine Against COVID-19. 2020. Available online: https://ClinicalTrials.gov/show/NCT04437875 (accessed on 27 July 2020).
- ACTRN12620000674932. An Interventional Study to Evaluate the Safety and Immune Response of a Vaccine Against Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2, the Virus that Causes COVID-19 Infection) when Given to Healthy Adult Participants. 2020. Available online: http://www.anzctr.org.au/TrialSearch.aspx?searchTxt=ACTRN12620000674932 (accessed on 27 July 2020).
- Monovalent Recombinant COVID19 Vaccine. 2020. Available online: https://ClinicalTrials.gov/show/NCT04453852 (accessed on 27 July 2020).
- Phase I Clinical Study of Recombinant Novel Coronavirus Vaccine. 2020. Available online: https://ClinicalTrials.gov/show/NCT04445194 (accessed on 27 July 2020).
- KBP-201 COVID-19 Vaccine Trial in Healthy Volunteers. 2020. Available online: https://ClinicalTrials.gov/show/NCT04473690 (accessed on 27 July 2020).
- Clinical Study of Recombinant Novel Coronavirus Vaccine. 2020. Available online: https://ClinicalTrials.gov/show/NCT04466085 (accessed on 27 July 2020).
- Novavax. Evaluation of the Safety and Immunogenicity of a SARS-CoV-2 rS (COVID-19) Nanoparticle Vaccine With/Without Matrix-M Adjuvant. 2020. Available online: https://ClinicalTrials.gov/show/NCT04368988 (accessed on 27 July 2020).
- SCB-2019 as COVID-19 Vaccine. 2020. Available online: https://ClinicalTrials.gov/show/NCT04405908 (accessed on 27 July 2020).
- Therapeutic Vaccine Trial of COVID-19 for Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection. 2020. Available online: https://ClinicalTrials.gov/show/NCT04428073 (accessed on 27 July 2020).
- Immunity and Safety of Covid-19 Synthetic Minigene Vaccine. 2020. Available online: https://ClinicalTrials.gov/show/NCT04276896 (accessed on 27 July 2020).
- Phase Ib-II Trial of Dendritic Cell Vaccine to Prevent COVID-19 in Adults. 2020. Available online: https://ClinicalTrials.gov/show/NCT04386252 (accessed on 27 July 2020).
- ChiCTR2000030750. A Clinical Study for Effectiveness and Safety Evaluation for Recombinant Chimeric COVID-19 Epitope DC Vaccine in the Treatment of Novel Coronavirus Pneumonia. 2020. Available online: http://www.chictr.org.cn/showproj.aspx?proj=50928 (accessed on 27 July 2020).
- Safety and Immunity of Covid-19 aAPC Vaccine. 2020. Available online: https://ClinicalTrials.gov/show/NCT04299724 (accessed on 27 July 2020).
- Medicago. Safety, Tolerability and Immunogenicinity of a Coronavirus-Like Particle COVID-19 Vaccine in Adults Aged 18-55 Years. 2020. Available online: https://ClinicalTrials.gov/show/NCT04450004 (accessed on 27 July 2020).
- ISRCTN89951424. A Phase III Study to Investigate a Vaccine Against COVID-19. 2020. Available online: http://www.isrctn.com/ISRCTN90853814:2020. (accessed on 27 July 2020).
- Investigating a Vaccine Against COVID-19. 2020. Available online: https://ClinicalTrials.gov/show/NCT04400838 (accessed on 27 July 2020).
- EUCTR2020-001228-32-GB. Investigating a Vaccine Against COVID-19. 2020. Available online: https://www.clinicaltrialsregister.eu/ctr-search/trial/2020-001228-32/GB (accessed on 27 July 2020).
- ChiCTR2000034780. A Phase III Clinical Trial for Inactivated Novel Coronavirus Pneumonia (COVID-19) Vaccine (Vero Cells). 2020. Available online: http://www.chictr.org.cn/hvshowproject.aspx?id=43780 (accessed on 27 July 2020).
- Clinical Trial of Efficacy and Safety of Sinovac’s Adsorbed COVID-19 (Inactivated) Vaccine in Healthcare Professionals. 2020. Available online: https://ClinicalTrials.gov/show/NCT04456595 (accessed on 27 July 2020).
- A Study to Evaluate Efficacy, Safety, and Immunogenicity of mRNA-1273 Vaccine in Adults Aged 18 Years and Older to Prevent COVID-19. 2020. Available online: https://ClinicalTrials.gov/show/NCT04470427 (accessed on 27 July 2020).
- Nasrollahzadeh, M.; Sajjadi, M.; Soufi, G.J.; Iravani, S.; Varma, R.S. Nanomaterials and Nanotechnology-Associated Innovations against Viral Infections with a Focus on Coronaviruses. Nanomaterials 2020, 10, 1072. [Google Scholar] [CrossRef] [PubMed]
- Itani, R.; Tobaiqy, M.; Al Faraj, A. Optimizing use of theranostic nanoparticles as a life-saving strategy for treating COVID-19 patients. Theranostics 2020, 10, 5932–5942. [Google Scholar] [CrossRef]
- Wang, F.; Kream, R.M.; Stefano, G.B. An Evidence Based Perspective on mRNA-SARS-CoV-2 Vaccine Development. Med. Sci. Monit. 2020, 26, e924700. [Google Scholar] [CrossRef]
- Wadman, M. Antivaccine forces gaining online. Science 2020, 368, 699. [Google Scholar] [CrossRef]
- Pagliusi, S.; Jarrett, S.; Hayman, B.; Kreysa, U.; Prasad, S.D.; Reers, M.; Hong Thai, P.; Wu, K.; Zhang, Y.T.; Baek, Y.O.; et al. Emerging manufacturers engagements in the COVID −19 vaccine research, development and supply. Vaccine 2020, 38, 5418–5423. [Google Scholar] [CrossRef] [PubMed]
- Hodgson, J. The pandemic pipeline. Nat. Biotechnol. 2020, 38, 523–532. [Google Scholar] [CrossRef] [PubMed]
- Amanat, F.; Krammer, F. SARS-CoV-2 Vaccines: Status Report. Immunity 2020, 52, 583–589. [Google Scholar] [CrossRef] [PubMed]
- Convalescent Plasma for Patients With COVID-19: A Randomized, Open Label, Parallel, Controlled Clinical Study. 2020. Available online: https://ClinicalTrials.gov/show/NCT04332835 (accessed on 27 July 2020).
- Selçuk, A.A. A Guide for Systematic Reviews: PRISMA. Turk. Arch. Otorhinolaryngol. 2019, 57, 57–58. [Google Scholar] [CrossRef]
- WHO. DRAFT Landscape of COVID-19 Candidate Vaccines. Available online: https://www.who.int/publications/m/item/draft-landscape-of-covid-19-candidate-vaccines (accessed on 30 June 2020).
- Whole-Virion Inactivated SARS-CoV-2 Vaccine (BBV152) for COVID-19 in Healthy Volunteers. 2020. Available online: https://ClinicalTrials.gov/show/NCT04471519 (accessed on 27 July 2020).
- Prevention. Safety and Immunogenicity Study of an Inactivated SARS-CoV-2 Vaccine for Preventing Against COVID-19 in People Aged ⩾60 Years. 2020. Available online: https://ClinicalTrials.gov/show/NCT04470609 (accessed on 27 July 2020).
- Rees, V. Germany to Begin First Clinical Trial of COVID-19 Vaccine Candidate. Available online: https://www.europeanpharmaceuticalreview.com/news/117624/germany-to-begin-first-clinical-trial-of-covid-19-vaccine-candidate/ (accessed on 30 June 2020).
- Gao, Q.; Bao, L.; Mao, H.; Wang, L.; Xu, K.; Yang, M.; Li, Y.; Zhu, L.; Wang, N.; Lv, Z.; et al. Rapid development of an inactivated vaccine candidate for SARS-CoV-2. Science 2020. [Google Scholar] [CrossRef]
- Chen, X.; Han, W.; Wang, G.; Zhao, X. Application prospect of polysaccharides in the development of anti-novel coronavirus drugs and vaccines. Int. J. Biol. Macromol. 2020, 164, 331–343. [Google Scholar] [CrossRef]
- Jean, S.S.; Lee, P.I.; Hsueh, P.R. Treatment options for COVID-19: The reality and challenges. J. Microbiol. Immunol. Infect.—Wei mian yu gan ran za zhi 2020, 53, 436–443. [Google Scholar] [CrossRef]
- Shadmi, E.; Chen, Y.; Dourado, I.; Faran-Perach, I.; Furler, J.; Hangoma, P.; Hanvoravongchai, P.; Obando, C.; Petrosyan, V.; Rao, K.D.; et al. Health equity and COVID-19: Global perspectives. Int. J. Equity Health 2020, 19, 104. [Google Scholar] [CrossRef]
- Thanh Le, T.; Andreadakis, Z.; Kumar, A.; Gómez Román, R.; Tollefsen, S.; Saville, M.; Mayhew, S. The COVID-19 vaccine development landscape. Nat. Rev. Drug Discov. 2020, 19, 305–306. [Google Scholar] [CrossRef]
- Tan, W.G.; Jin, H.T.; West, E.E.; Penaloza-MacMaster, P.; Wieland, A.; Zilliox, M.J.; McElrath, M.J.; Barouch, D.H.; Ahmed, R. Comparative analysis of simian immunodeficiency virus gag-specific effector and memory CD8+ T cells induced by different adenovirus vectors. J. Virol. 2013, 87, 1359–1372. [Google Scholar] [CrossRef]
- Folegatti, P.M.; Ewer, K.J.; Aley, P.K.; Angus, B.; Becker, S.; Belij-Rammerstorfer, S.; Bellamy, D.; Bibi, S.; Bittaye, M.; Clutterbuck, E.A.; et al. Safety and immunogenicity of the ChAdOx1 nCoV-19 vaccine against SARS-CoV-2: A preliminary report of a phase 1/2, single-blind, randomised controlled trial. Lancet 2020. [Google Scholar] [CrossRef]
- Afrough, B.; Dowall, S.; Hewson, R. Emerging viruses and current strategies for vaccine intervention. Clin. Exp. Immunol. 2019, 196, 157–166. [Google Scholar] [CrossRef]
- Cohen, J. Vaccine designers take first shots at COVID-19. Science 2020, 368, 14–16. [Google Scholar] [CrossRef] [PubMed]
- Ura, T.; Okuda, K.; Shimada, M. Developments in Viral Vector-Based Vaccines. Vaccines 2014, 2, 624–641. [Google Scholar] [CrossRef] [PubMed]
- Ewer, K.J.; Lambe, T.; Rollier, C.S.; Spencer, A.J.; Hill, A.V.; Dorrell, L. Viral vectors as vaccine platforms: From immunogenicity to impact. Curr. Opin. Immunol. 2016, 41, 47–54. [Google Scholar] [CrossRef]
- Zhu, F.C.; Li, Y.H.; Guan, X.H.; Hou, L.H.; Wang, W.J.; Li, J.X.; Wu, S.P.; Wang, B.S.; Wang, Z.; Wang, L.; et al. Safety, tolerability, and immunogenicity of a recombinant adenovirus type-5 vectored COVID-19 vaccine: A dose-escalation, open-label, non-randomised, first-in-human trial. Lancet 2020, 395, 1845–1854. [Google Scholar] [CrossRef]
- Klug, B.; Robertson, J.S.; Condit, R.C.; Seligman, S.J.; Laderoute, M.P.; Sheets, R.; Williamson, A.L.; Gurwith, M.; Kochhar, S.; Chapman, L.; et al. Adventitious agents and live viral vectored vaccines: Considerations for archiving samples of biological materials for retrospective analysis. Vaccine 2016, 34, 6617–6625. [Google Scholar] [CrossRef] [PubMed]
- Alharbi, N.K.; Padron-Regalado, E.; Thompson, C.P.; Kupke, A.; Wells, D.; Sloan, M.A.; Grehan, K.; Temperton, N.; Lambe, T.; Warimwe, G.; et al. ChAdOx1 and MVA based vaccine candidates against MERS-CoV elicit neutralising antibodies and cellular immune responses in mice. Vaccine 2017, 35, 3780–3788. [Google Scholar] [CrossRef] [PubMed]
- van Doremalen, N.; Haddock, E.; Feldmann, F.; Meade-White, K.; Bushmaker, T.; Fischer, R.J.; Okumura, A.; Hanley, P.W.; Saturday, G.; Edwards, N.J.; et al. A single dose of ChAdOx1 MERS provides protective immunity in rhesus macaques. Sci. Adv. 2020, 6, eaba8399. [Google Scholar] [CrossRef]
- Rauch, S.; Jasny, E.; Schmidt, K.E.; Petsch, B. New Vaccine Technologies to Combat Outbreak Situations. Front. Immunol. 2018, 9, 1963. [Google Scholar] [CrossRef]
- Sahin, U.; Karikó, K.; Türeci, Ö. mRNA-based therapeutics—Developing a new class of drugs. Nat. Rev. Drug Discov. 2014, 13, 759–780. [Google Scholar] [CrossRef]
- Ahmed, S.F.; Quadeer, A.A.; McKay, M.R. Preliminary Identification of Potential Vaccine Targets for the COVID-19 Coronavirus (SARS-CoV-2) Based on SARS-CoV Immunological Studies. Viruses 2020, 12, 254. [Google Scholar] [CrossRef]
- Phan, T. Genetic diversity and evolution of SARS-CoV-2. Infect. Genet. Evol. 2020, 81, 104260. [Google Scholar] [CrossRef] [PubMed]
- Ugurel, O.M.; Ata, O.; Turgut-Balik, D. An updated analysis of variations in SARS-CoV-2 genome. Turk. J. Biol.—Turk biyoloji dergisi 2020, 44, 157–167. [Google Scholar] [CrossRef] [PubMed]
- Lim, M.; Badruddoza, A.Z.M.; Firdous, J.; Azad, M.; Mannan, A.; Al-Hilal, T.A.; Cho, C.S.; Islam, M.A. Engineered Nanodelivery Systems to Improve DNA Vaccine Technologies. Pharmaceutics 2020, 12, 30. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.R.F.; Patel, A.; Ramos, S.; Elwood, D.; Zhu, X.; Yan, J.; Gary, E.N.; Walker, S.N.; Schultheis, K.; Purwar, M.; et al. Immunogenicity of a DNA vaccine candidate for COVID-19. Nat. Commun. 2020, 11, 2601. [Google Scholar] [CrossRef]
- Pandey, S.C.; Pande, V.; Sati, D.; Upreti, S.; Samant, M. Vaccination strategies to combat novel corona virus SARS-CoV-2. Life Sci. 2020, 256, 117956. [Google Scholar] [CrossRef]
- Spruth, M.; Kistner, O.; Savidis-Dacho, H.; Hitter, E.; Crowe, B.; Gerencer, M.; Brühl, P.; Grillberger, L.; Reiter, M.; Tauer, C.; et al. A double-inactivated whole virus candidate SARS coronavirus vaccine stimulates neutralising and protective antibody responses. Vaccine 2006, 24, 652–661. [Google Scholar] [CrossRef]
- Thèves, C.; Crubézy, E.; Biagini, P. History of Smallpox and Its Spread in Human Populations. Microbiol. Spectr. 2016, 4, 161–172. [Google Scholar] [CrossRef]
- Foley, K.E. A Brief Overview of All the Covid-19 Vaccines in the Pipeline. Available online: https://qz.com/1854077/a-brief-overview-of-all-the-covid-19-vaccines-in-the-pipeline/ (accessed on 29 June 2020).
- Gupta, T.; Gupta, S.K. Potential adjuvants for the development of a SARS-CoV-2 vaccine based on experimental results from similar coronaviruses. Int. Immunopharmacol. 2020, 86, 106717. [Google Scholar] [CrossRef]
- Garçon, N.; Vaughn, D.W.; Didierlaurent, A.M. Development and evaluation of AS03, an Adjuvant System containing α-tocopherol and squalene in an oil-in-water emulsion. Expert Rev. Vaccines 2012, 11, 349–366. [Google Scholar] [CrossRef] [PubMed]






| ID Number | Phase | Vaccine Name | Properties | Vaccine Features | Coronavirus Target | Start Date | Completion Date | Progress (%) | Recruitment Status | Recruitment Country |
|---|---|---|---|---|---|---|---|---|---|---|
| ISRCTN89951424# [50] | III | ChAdOx1 nCoV-19 | Non replicating viral vector | Chimpanzee r-ADV vaccine encoding S protein | S protein of SARS-CoV-2 | 05/01/2020 | 07/31/2021 | 18.9 | Recruiting | Brazil |
| NCT04456595 [54] | III | Adsorbed inactivated SARS-CoV-2 | Inactivated virus | Adsorbed SARS-CoV-2 (CN2 strain) vaccine inactivated by BPL | Multiple proteins of SARS-CoV-2 | 07/01/2020 | 10/01/2021 | 5.5 | Not yet recruiting | Brazil |
| ChiCTR2000034780 [53] | III | Purified inactivated SARS-CoV-2 | Inactivated virus | SARS-CoV-2 strain inactivated inside Vero Cells | Multiple proteins of SARS-CoV-2 | 07/16/2020 | 07/16/2021 | 2.7 | Recruiting | United Arab Emirates |
| NCT04470427 [55] | III | mRNA1273 | mRNA | LNP-encapsulated mRNA-1273 encoding S protein | S protein of SARS-CoV-2 | 07/27/2020 | 10/27/2022 | 0.0 | Not yet recruiting | USA |
| NCT04400838 [51] | II-III | ChAdOx1 nCoV-19 | Non replicating viral vector | Chimpanzee r-ADV vaccine encoding S protein | S protein of SARS-CoV-2 | 05/01/2020 | 08/01/2021 | 18.8 | Not yet recruiting | United Kingdom |
| EudraCT2020-001228-32 ISRCTN90906759 [52] | II-III | ChAdOx1 nCoV-19 | Non replicating viral vector | Chimpanzee r-ADV vaccine encoding S protein | S protein of SARS-CoV-2 | 03/02/2020 | 06/30/2021 | 30.1 | Ongoing | United Kingdom |
| NCT04405076 [20] | II | mRNA1273 | mRNA | LNP-encapsulated mRNA-1273 encoding S protein | S protein of SARS-CoV-2 | 05/29/2020 | 08/01/2021 | 13.5 | Recruiting | USA |
| NCT04341389 [32] | II | Adenovirus Type 5 (Ad5-nCoV) | Non replicating viral vector | Serotype 5 r-ADV vaccine encoding S protein | Full-length S protein of SARS-CoV-2 | 04/12/2020 | 01/31/2021 | 35.7 | Active, not recruiting | China |
| ChiCTR2000031781 [29] | II | Adenovirus Type 5 (Ad5-nCoV) | Non replicating viral vector | Serotype 5 r-ADV vaccine encoding S protein | Full-length S protein of SARS-CoV-2 | 04/12/2020 | 01/31/2021 | 35.7 | Not yet recruiting | China |
| NCT04466085 [41] | II | CHO cells vaccine | Protein Subunit | Recombinant protein produced with CHO cells + adjuvant (RBD-Dimer) | S protein of SARS-CoV-2 | 07/12/2020 | 09/15/2021 | 3.3 | Not yet recruiting | NR |
| NCT04445389 [25] | I-II | GX-19 | DNA | DNA vaccine | Unspecified protein of SARS-CoV-2 | 06/17/2020 | 06/17/2022 | 5.3 | Recruiting | Republic of Korea |
| NCT04444674 [33] | I-II | ChAdOx1 nCoV-19 | Non replicating viral vector | Chimpanzee r-ADV vaccine encoding S protein | S protein of SARS-CoV-2 | 06/01/2020 | 12/01/2021 | 10.0 | Not yet recruiting | South Africa |
| NCT04437875 [36] | I-II | Gam-COVID-Vac Lyo | Non replicating viral vector | Combined serotypes 5 and 26 r-ADV vectored vaccine encoding S protein | S protein of SARS-CoV-2 | 06/17/2020 | 08/15/2020 | 66.1 | Recruiting | Russia |
| NCT04436471 [35] | I-II | Gam-COVID-Vac | Non replicating viral vector | Combined serotypes 5 and 26 r-ADV vectored vaccine encoding S protein | S protein of SARS-CoV-2 | 06/17/2020 | 08/15/2020 | 66.1 | Recruiting | Russia |
| NCT04412538 [12] | I-II | Purified inactivated SARS-CoV-2 | Inactivated virus | Purified inactivated SARS-CoV-2 | Multiple proteins of SARS-CoV-2 | 05/15/2020 | 09/01/2021 | 15.2 | Recruiting | China |
| NCT04398147 [30] | I-II | Adenovirus Type 5 (Ad5-nCoV) | Non replicating viral vector | Serotype 5 r-ADV vaccine encoding S protein intramuscularly | Full-length S protein of SARS-CoV-2 | 05/01/2020 | 08/01/2021 | 18.8 | Not yet recruiting | Canada |
| NCT04386252 [46] | I-II | AV-COVID-19 | Dendritic cells | Autologous DCs differentiated in vitro from monocytes incubated with IL-4 and GM-CSF loaded with antigens from SARS-CoV-2 | Unspecified proteins of SARS-CoV-2 | 07/01/2020 | 03/01/2021 | 10.3 | Not yet recruiting | USA |
| NCT04383574 [10] | I-II | Adsorbed inactivated SARS-CoV-2 | Inactivated virus | Adsorbed SARS-CoV-2 (CN2 strain) vaccine inactivated by BPL | Multiple proteins of SARS-CoV-2 | 05/20/2020 | 07/20/2020 | 100 | Completed | China |
| NCT04380701 [19] | I-II | BNT162 | mRNA | LNP-encapsulated nucleoside modified mRNA (BNT162) | S protein of SARS-CoV-2 | 04/23/2020 | 08/01/2020 | 94.0 | Recruiting | Germany |
| NCT04352608 [11] | I-II | Adsorbed inactivated SARS-CoV-2 | Inactivated virus | Adsorbed SARS-CoV-2 (CN2 strain) vaccine inactivated by BPL | Multiple proteins of SARS-CoV-2 | 04/16/2020 | 12/13/2020 | 41.9 | Recruiting | China |
| NCT04324606 EudraCT2020-001072-15 [34] | I-II | ChAdOx1 nCoV-19 | Non replicating viral vector | Chimpanzee r-ADV vaccine encoding S protein | S protein of SARS-CoV-2 | 04/23/2020 | 05/01/2021 | 25.2 | Active, not recruiting | United Kingdom |
| NCT04276896 [45] | I-II | Lentiviral Minigene vaccine (LV-SMENP) | Dendritic cells | DCs modified by lentiviral vector system (NHP/TYF) + CTLs | Multiple proteins of SARS-CoV-2 | 03/24/2020 | 12/31/2024 | 7.1 | Recruiting | China |
| ChiCTR2000032459 [9] | I-II | Purified inactivated SARS-CoV-2 | Inactivated virus | SARS-CoV-2 strain inactivated inside Vero Cells | Multiple proteins of SARS-CoV-2 | 04/28/2020 | 11/28/2021 | 15.4 | Recruiting | China |
| ChiCTR2000031809 [8] | I-II | Purified inactivated SARS-CoV-2 | Inactivated virus | SARS-CoV-2 strain inactivated inside Vero Cells | Multiple proteins of SARS-CoV-2 | 04/11/2020 | 11/10/2021 | 18.3 | Not yet recruiting | China |
| ChiCTR2000030750 [47] | I-II | Dendritic cells vaccine | Dendritic cells | COVID-19 epitope gene recombinant chimeric DC vaccine | SARS-CoV-2 epitope | 03/01/2020 | 02/28/2021 | 40.4 | Not yet recruiting | China |
| EudraCT 2020-001038-36 [15] | I-II | BNT162 | mRNA | LNP-encapsulated nucleoside modified mRNA (BNT162) | S protein epitope of SARS-CoV-2 | 04/20/2020 | 07/26/2020 * | NR | Ongoing | NR |
| NCT04447781 [24] | I-II | INO-4800 | DNA | DNA plasmid (pGX9501) vaccine with electroporation (INO-4800) | Full-length S protein of SARS-CoV-2 | 06/22/2020 | 02/22/2022 | 5.6 | Not yet recruiting | Republic of Korea |
| NCT04463472 [23] | I-II | AG0301-COVID19 | DNA | DNA plasmid vaccine | Multiples antigens from SARS-CoV-2 | 06/29/2020 | 07/31/2021 | 6.8 | Recruiting | Japan |
| CTRI/2020/07/026352 [22] | I-II | ZYCOV-D | DNA | DNA plasmid vaccine | S protein of SARS-CoV-2 | 07/13/2020 | 07/13/2021 | 3.6 | Recruiting | India |
| CTRI/2020/07/026300/NCT04471519 [66] | I-II | Covaxin (BBV152) | Inactivated virus | Whole-Virion Inactivated SARS-CoV-2 Vaccine (BBV152A, BBV152B and BBV152C) | Multiples antigens from SARS-CoV-2 | 07/13/2020 | 06/30/2021 | 3.7 | Recruiting | India |
| NCT04470609 [67] | I-II | SARS-CoV-2 Vaccine | Inactivated virus | Purified inactivated SARS-CoV-2 vaccine | Multiples antigens from SARS-CoV-2 | 07/10/2020 | 11/10/2021 | 3.3 | Enrolling by invitation | China |
| NCT04473690 [40] | I-II | KBP-COVID-19 | Protein Subunit | RBD-based vaccine developed with fast-growing tobacco plant technology | RBD S protein of SARS-CoV2 | 07/25/2020 | 11/18/2021 | 0.2 | Not yet recruiting | NR |
| ChiCTR2000034825 [14] | I-II | BNT162b1 | mRNA | 3 LNP-mRNAs | RBD S protein of SARS-CoV2 | 07/20/2020 | 12/31/2020 | 3.7 | Recruiting | China |
| NCT04449276 EudraCT 2020-001286-36 [16] | I | CVnCoV | mRNA | mRNA vaccine | Unspecified protein of SARS-CoV-2 | 06/17/2020 | 08/31/2020 | 52.0 | Recruiting | Germany |
| NCT04405908 [43] | I | SCB-2019 | Protein subunit | Recombinant 2019-nCoV S protein subunit-trimer vaccine + AS03 or CpG 1018 + Alum adjuvants | S protein of SARS-CoV-2 | 06/19/2020 | 03/30/2021 | 13.0 | Recruiting | Australia |
| NCT04334980 [26] | I | bacTRL-Spike | DNA | Genetically modified probiotic bacteria containing plasmid encoding S protein | S protein of SARS-CoV-2 | 04/30/2020 | 12/31/2021 | 14.3 | Not yet recruiting | Canada |
| NCT04313127 [31] | I | Adenovirus Type 5 (Ad5-nCoV) | Non replicating viral vector | r-ADV vaccine encoding S protein | Full-length S protein of SARS-CoV-2 | 03/16/2020 | 12/20/2022 | 13.1 | Active, not recruiting | China |
| NCT04299724 [48] | I | aAPC | aAPC lentiviral modified vector | aAPC modified by lentiviral vector system NHP/TYF | Multiple proteins of SARS-CoV-2 | 02/15/2020 | 12/31/2024 | 9.1 | Recruiting | China |
| NCT04283461 [17] | I | mRNA-1273 | mRNA | LNP-encapsulated mRNA-1273 | S protein of SARS-CoV-2 | 03/16/2020 | 11/22/2021 | 21.4 | Recruiting | USA |
| NCT04428073 [44] | I | Covax-19™ | Protein subunit | Advax™ adjuvant with a recombinant SARS-CoV-2 S protein | S protein of SARS-CoV-2 | 07/01/2020 | 12/01/2021 | 4.8 | Not yet recruiting | NR |
| ChiCTR2000034112 [13] | I | NR | mRNA | mRNA vaccine | RBD S protein of SARS-CoV2 | 06/25/2020 | 12/31/2021 | 5.6 | Not yet recruiting | China |
| ChiCTR2000030906 [28] | I | Adenovirus Type 5 (Ad5-nCoV) | Non replicating viral vector | Serotype 5 r-ADV vaccine encoding S protein intramuscularly | Full-length S protein of SARS-CoV-2 | 03/16/2020 | 12/31/2020 | 45.5 | Recruiting | China |
| NCT04445194 [39] | I | CHO cells vaccine | Protein Subunit | Adjuvanted recombinant protein (RBD-Dimer) | S protein of SARS-CoV-2 | 06/22/2020 | 09/20/2021 | 7.5 | Recruiting | China |
| NCT04453852 [38] | I | Covax-19™ | Protein Subunit | Advax™ adjuvant combined with a SARS-CoV-2 recombinantS protein | S protein of SARS-CoV-2 | 06/30/2020 | 07/01/2021 | 7.1 | Recruiting | Australia |
| ACTRN12620000674932 [37] | I | SARS-CoV-2 Sclamp | Protein Subunit | Molecular clamp stabilized S protein with MF59 adjuvant | S protein of SARS-CoV-2 | 06/06/2020 | 07/26/2020 * | NR | Recruiting | Australia |
| ISRCTN17072692 [21] | I | LNP-nCoVsaRNA | saRNA | saRNA vaccine encoding S protein | S protein of SARS-CoV-2 | 04/01/2020 | 07/31/2021 | 23.9 | Recruiting | United Kingdom |
| NCT04450004 [49] | I | Plant-derived VLP | VLP | Plant-derived VLP + CpG 1018 or AS03 adjuvants | S protein of SARS-CoV-2 | 07/10/2020 | 04/30/2021 | 5.4 | Recruiting | Canada |
| NCT04368988 [42] | I | NVX-CoV2373 | Protein subunit | Recombinant SARS CoV-2 S protein NP vaccine + Matrix M adjuvant | S protein of SARS-CoV-2 | 05/25/2020 | 07/31/2021 | 14.4 | Recruiting | Australia |
| NCT04368728 [18] | I | BNT162 | mRNA | LNP-encapsulated nucleoside modified mRNA (BNT162) | S protein epitope of SARS-CoV-2 | 04/29/2020 | 01/23/2023 | 8.8 | Recruiting | USA |
| NCT04336410 [27] | I | INO-4800 | DNA | DNA plasmid (pGX9501) vaccine with electroporation (INO-4800) | Full-length S protein of SARS-CoV-2 | 04/03/2020 | 07/01/2021 | 25.1 | Recruiting | USA |
| ID Number | Rehearsal Center | Estimated Enrollment | Allocation | Intervention Model | Masking | Intervention (Route) | Arm | Dose (Day) | Age Range (Years) |
|---|---|---|---|---|---|---|---|---|---|
| ISRCTN89951424 [50] | Single center | 2000 | Randomized | Sequential Assignment | Single | ChAdOx1 nCoV-19 (i.m) or MenACWY (i.m) | 2 | ChAdOx1 nCoV-19: 5 × 1010 vp Men ACWY: 0.5 ml | 18–55 |
| NCT04456595 [54] | Multicenter | 8870 | Randomized | Parallel Assignment | Quadruple | Inactivated SARS-CoV-2 Vaccine (i.m. − deltoid muscle) × Placebo (i.m) | 4 | NR (2 times: 0,14) | >18 |
| ChiCTR2000034780 [53] | Single center | 15,000 | Randomized | Parallel Assignment | Double | Inactivated SARS-CoV-2 Vaccine × Placebo | 3 | NR (2 times) | >18 |
| NCT04470427 [55] | Multicenter | 30,000 | Randomized | Parallel Assignment | Quadruple | mRNA-1273 Vaccine (.i.m) × Placebo (i.m) | 2 | 100 μg (2 times: 0,28) | >18 |
| NCT04400838 [51] | Multicenter | 10,260 | Randomized | Sequential Assignment | Single | ChAdOx1 nCoV-19 (i.m) × MenACWY vaccine (licensed control vaccine (i.m) | 14 | 2.5 × 1010 vp; 5 × 1010 vp (single or 2 times: 1,28) | >5 |
| EudraCT2020-001228-32 ISRCTN90906759 [52] | Multicenter | 10,260 | Randomized | NR | Single | ChAdOx1 nCoV-19 (i.m) × MenACWY vaccine (licensed control vaccine (i.m) | 5 | NR | 5–12; 18–55; >56 |
| NCT04405076 [20] | Multicenter | 600 | Randomized | Sequential Assignment | Double | Crossover: mRNA-1273 SARS-COV-2 Vaccine <---> Placebo | 4 | 50 mcg; 100 mcg (0) | 18–54; >55 |
| NCT04341389 [32] | Single center | 508 | Randomized | Crossover Assignment | Double | rAd5-nCoV (i.m) × Placebo (i.m) | 3 | 1 × 1011vp; 5 × 1010 vp (0) | >18 |
| ChiCTR2000031781 [29] | Multicenter | 500 | Randomized | Parallel Assignment | Double | rAd5-nCoV (i.m) × Placebo (i.m) | 3 | 5 × 1010vp; 1 × 1011 vp | >18 |
| NCT04466085 [41] | NR | 900 | Randomized | Parallel Assignment | Double | Recombinant new coronavirus vaccine (CHO cells) (i.m.− deltoid muscle) × Placebo (i.m − deltoid muscle) | 6 | 25 μg/0.5 mL; 50 μg/0.5 mL (2 and 3 times: 0,1 month) | 18–59 |
| NCT04445389 [25] | Single center | 190 | Randomized | Parallel Assignment | Double | GX-19 (i.m) × Placebo (i.m) | 3 | GX-19 dose A; B (1, 29) | 18–50 |
| NCT04444674 [33] | Multicenter | 2000 | Randomized | Parallel assignment | Quadruple | ChAdOx1 nCoV-19 (i.m. − deltoid muscle x Placebo (i.m. − deltoid muscle) | 8 | 5 × 1010 vp (single or 2 times; 0,28) | 18–65 |
| NCT04437875 [36] | Single center | 38 | Non-randomized | Parallel Assignment | None | rAd26 (i.m) × rAd5 (i.m.) × rAd26 + rAd5 (i.m.) | 3 | rAd26 (1), rAd5 (1), rAd26 (1) + rAd5 (21) | 18–60 |
| NCT04436471 [35] | Single center | 38 | Non-randomized | Parallel Assignment | None | rAd26 (i.m) × rAd5 (i.m.) × rAd26 + rAd5 (i.m.) | 3 | rAd26 (1), rAd5 (1), rAd26 (1) + rAd5 (21) | 18–60 |
| NCT04412538 [12] | Single center | 942 | Randomized | Parallel Assignment | Quadruple | Inactivated SARS-CoV-2 Vaccine × Placebo | 8 | 50 U/0.5 mL; 100 U/0.5 mL; 150 U/0.5 mL (2 times: 0,14 or 0,28) | 18–59 |
| NCT04398147 [30] | Single center | 696 | Randomized | Parallel Assignment | Quadruple | rAd5-nCoV (i.m) × Placebo (i.m) | 28 | 5 × 1010 vp; 10 × 1010 vp (single or 2 times: 0,56) | 18–55;65–85; |
| NCT04386252 [46] | Single center | 180 | Randomized | Parallel Assignment | Quadruple | Dendritic cells vaccine × GM-CSF (s.c) × Placebo (s.c) | 9 | DC loaded with 1×, 10× and 30× antigen + 250 and 500 mcg GM-CSF (0) | >18 |
| NCT04383574 [10] | Single center | 422 | Randomized | Parallel Assignment | Double | Inactivated SARS-CoV-2 vaccine × Placebo | 4 | 300 SU/mL; 600 SU/mL; 1200 SU/mL (2 times: 0,28) | >60 |
| NCT04380701 [19] | Single center | 200 | Non-randomized | Sequential Assignment | None | BNT162a1; BNT162b1; BNT162b2; BNT162c2 | 4 | Escalating dose levels (BNT162a1, BNT162b1, BNT162b2); Single dose (BNT162c2) | 18–55 |
| NCT04352608 [11] | Single center | 744 | Randomized | Parallel Assignment | Quadruple | Inactivated SARS-CoV-2 vaccine (i.m) × Placebo (i.m.) | 6 | 600 SU/0.5 mL; 1200 SU/0.5 mL (2 times: 0,14 or 0,28) | 18–59 |
| NCT04324606 EudraCT2020-001072-15 [34] | Multicenter | 1090 | Randomized | Sequential Assignment | Single | ChAdOx1 nCoV-19 (i.m) × MenACWY vaccine (i.m) ± Paracetamol (oral) | 9 | 5 × 1010 vp (Single: 0) | 18–55 |
| NCT04276896 [45] | Multicenter | 100 | NR | Single Group Assignment | None | LV-SMENP-DC vaccine (s.c) and antigen-specific CTLs (i.v) | 1 | 5 × 106 DC + 1 × 108 CTLs | 0.5–80 |
| ChiCTR2000032459 [9] | Single center | 2128 (I: 480; II: 1648) | Randomized | Parallel Assignment | Double | Inactivated SARS-CoV-2 vaccine × Placebo | 30 (Phase I); 38 (Phase II) | Low; Medium; High | >3 |
| ChiCTR2000031809 [8] | Multicenter | 1456 (I: 288; II: 1168) | Randomized | Parallel Assignment | Double | Inactivated SARS-CoV-2 vaccine × Placebo | 18 (Phase I); 26 (Phase II) | Low; Medium; High | >6 |
| ChiCTR2000030750 [47] | Multicenter | 120 | Randomized | Parallel Assignment | Double | Recombinant chimeric DC vaccine × Blank vaccine | 4 | NR | 25–65 |
| EudraCT 2020-001038-36 [15] | Multicenter | 196 | Non-randomized | Parallel Assignment | None | BNT162a1 × BNT162b1 × BNT162b2 × BNT162c2 | 4 | Prime/Boost Regimen | 18–64 |
| NCT04447781 [24] | Single center | 160 | Randomized | Sequential Assignment | Triple | INO-4800 (i.d. + EP) × Placebo (i.d. + EP) | 4 | 1 mg/dose + EP; 2 mg/dose + EP (2 times: 0,28) | 19–64 |
| NCT04463472 [23] | Single center | 30 | Non-Randomized | Sequential Assignment | None | AG0301 DNA Vaccine (i.m.) | 2 | 1.0 mg; 2.0 mg (2 times: 0,14) | 20–65 |
| CTRI/2020/07/026352 [22] | Single center | 1148 | Randomized | Sequential Assignment | Single | Novel Corona Virus-2019-nCov vaccine (i.d.) × Placebo (i.d) | NR | 0.1 mL (Three times: 0,28,56) | 18–55 |
| CTRI/2020/07/026300 NCT04471519 [66] | Multicenter | 1125 | Randomized | Parallel Assignment | Triple | BBV152A (i.m) × BBV152B (i.m) × BBV152C (i.m.) × Placebo (i.m) | 3 | 0.5 mL (Two times: 0;14) | 12–55; 12–65 |
| NCT04470609 [67] | Multicenter | 471 | Randomized | Parallel Assignment | Quadruple | Inactivated SARS-CoV-2 vaccine × Placebo | 4 | 50 U/0.5 mL; 100 U/0.5 mL (2 times: 0,28) | >60 |
| NCT04473690 [40] | NR | 180 | Randomized | Parallel Assignment | Quadruple | KBP × Placebo | 3 | Low and high doses | 18–49; 50–70 |
| ChiCTR2000034825 [14] | Multicenter | 144 | Randomized | Parallel Assignment | NR | BNT162b1 mRNA vaccine × Placebo | 6 | Low and high doses (2 times: 0,21) | 18–55; >55 |
| NCT04449276 EudraCT 2020-001286-36 [16] | Single center | 168 | Randomized | Sequential Assignment | Single | CVnCoV (i.m. − deltoid muscle) × Placebo (i.m − deltoid muscle) | 2 | 2, 4 and 8 μg (1 and 29) | 18–60 |
| NCT04405908 [43] | Single center | 150 | Randomized | Sequential Assignment | Triple | SCB-2019 vaccine (i.m); SCB-2019 + AS03 (i.m) and SCB-2019 + CpG 1018 + Alum (i.m) | 15 | 3 µg; 9 µg; 30 µg (1,22) | 18–54; 55–75 |
| NCT04334980 [26] | Multicenter | 84 | Randomized | Parallel Assignment | Triple | bacTRL-Spike (oral) × Placebo (oral) | 6 | 1 cfu; 3 cfu; 10 cfu (0) | 19–45 |
| NCT04313127 [31] | Single center | 108 | Non-randomized | Sequential Assignment | None | Ad5-nCoV (i.m) | 3 | 5 × 1010 vp; 1 × 1011 vp; 1.5 × 1011 vp (Single: 0) | 18–60 |
| NCT04299724 [48] | Single center | 100 | N/A | Single Group Assignment | None | Pathogen-specific aAPC vaccine (s.c) | 1 | 5 × 106 cells (Three times: 0,14,28) | 0.5–80 |
| NCT04283461 [17] | Multicenter | 155 | Non-randomized | Sequential Assignment | None | LNP- encapsulated mRNA-1273 (i.m.) | 13 | 10 mcg; 25 mcg; 50 mcg; 100 mcg; 250 mcg (2 times; 1,29) | 18–55; 56–70; >70 |
| NCT04428073 [44] | Single center | 32 | Non-randomized | Sequential Assignment | None | Covax-19 vaccine | 2 | 1.0 mL of low dose; 1.0 mL of high dose | 18–60 |
| ChiCTR2000034112 [13] | Multicenter | 168 | Randomized | Parallel Assignment | None | mRNA vaccine | 3 | Low; Medium; High | 18–59; 60–80 |
| ChiCTR2000030906 [28] | Multicenter | 108 | Non-randomized | Parallel Assignment | None | rAd5-nCoV (i.m.) | 3 | 5 × 1010 vp; 1 × 1011 vp; 1.5 × 1011 vp | 18–60 |
| NCT04445194 [39] | Single center | 50 | Randomized | Parallel Assignment | Double | Recombinant new coronavirus vaccine (CHO cell) (i.m) × Placebo (i.m) | 3 | 25 μg/0.5 mL; 50 μg/0.5 mL | 18–59 |
| NCT04453852 [38] | Single center | 40 | Randomized | Parallel Assignment | Triple | Covax-19 vaccine × Placebo | 2 | 25 ug Spike antigen + 15 mg Advax-2 adjuvant | 18–68 |
| ACTRN12620000674932 [37] | Single center | 120 | Randomized | Parallel Assignment | Triple | SARS-CoV-2 Sclamp vaccine (i.m) × Placebo (i.m) | 4 | 1 × 5 mcg/0.5 mL; 1 × 15 mcg/0.5 mL; 1 × 45 mcg/0.5 mL (2 times: 0,28) | 18–55 |
| ISRCTN17072692 [21] | Multicenter | 320 | Randomized | Sequential Assignment | NR | COVAC mRNA vaccine (i.m. − deltoid muscle) | 3 | 0.1 µg; 0.3 µg; 1.0 µg | 18–45; 18–75 |
| NCT04450004 [49] | Multicenter | 180 | Randomized | Sequential Assignment | None | Coronavirus-like particle COVID-19 vaccine ± CpG 1018 or AS03 (i.m) | 9 | 3.75 µg; 7.5 µg; 15 µg + CpG 1018 or AS03 | 18–55 |
| NCT04368988 [42] | Multicenter | 131 | Randomized | Parallel Assignment | Triple | NVX-CoV2373 (Matrix-M) (i.m) × Placebo (i.m) | 5 | 5 μg or 25 μg with/without 50 μg Matrix-M (2 times: 0,21) | 18–59 |
| NCT04368728 [18] | Multicenter | 7600 | Randomized | Parallel Assignment | Triple | BNT162a1 (i.m); BNT162b1 (i.m); BNT162b2 (i.m); BNT162c2 (i.m); Placebo (i.m) | 21 | 0.5 mL (Single or 2 times: 0,21). Prime/boost regimen | 18–55; 65–85; 18–85 |
| NCT04336410 [27] | Multicenter | 120 | Non-randomized | Sequential Assignment | None | INO-4800 (i.d + EP) | 3 | 0.5 mg + EP; 1.0 mg + EP; 2.0 mg + EP (2 times: 0,28) | >18 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rego, G.N.A.; Nucci, M.P.; Alves, A.H.; Oliveira, F.A.; Marti, L.C.; Nucci, L.P.; Mamani, J.B.; Gamarra, L.F. Current Clinical Trials Protocols and the Global Effort for Immunization against SARS-CoV-2. Vaccines 2020, 8, 474. https://doi.org/10.3390/vaccines8030474
Rego GNA, Nucci MP, Alves AH, Oliveira FA, Marti LC, Nucci LP, Mamani JB, Gamarra LF. Current Clinical Trials Protocols and the Global Effort for Immunization against SARS-CoV-2. Vaccines. 2020; 8(3):474. https://doi.org/10.3390/vaccines8030474
Chicago/Turabian StyleRego, Gabriel N. A., Mariana P. Nucci, Arielly H. Alves, Fernando A. Oliveira, Luciana C. Marti, Leopoldo P. Nucci, Javier B. Mamani, and Lionel F. Gamarra. 2020. "Current Clinical Trials Protocols and the Global Effort for Immunization against SARS-CoV-2" Vaccines 8, no. 3: 474. https://doi.org/10.3390/vaccines8030474
APA StyleRego, G. N. A., Nucci, M. P., Alves, A. H., Oliveira, F. A., Marti, L. C., Nucci, L. P., Mamani, J. B., & Gamarra, L. F. (2020). Current Clinical Trials Protocols and the Global Effort for Immunization against SARS-CoV-2. Vaccines, 8(3), 474. https://doi.org/10.3390/vaccines8030474