Moderate Vaccine Effectiveness against Severe Acute Respiratory Infection Caused by A(H1N1)pdm09 Influenza Virus and No Effectiveness against A(H3N2) Influenza Virus in the 2018/2019 Season in Italy

 ,
,  , , , , ,
, , , , ,  ,
,  , ,
, ,  ,
,  and
and
Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Study Setting and Population
2.3. Case Finding
- Age < 6 months at time of recruitment;
- Presence of contraindication for the influenza vaccine;
- Previously hospitalised < 48 h prior to SARI onset;
- SARI onset ≥ 48 h after hospital admission;
- Respiratory specimen taken >7 days after SARI onset;
- Tested positive for any influenza virus in the 2018/19 season before the onset of symptoms leading to the current hospitalisation;
- Vaccination ≤ 14 days before SARI symptom onset, no vaccine record for 2018/19 season, or ambiguous vaccination status;
- Unwilling to participate or unable to communicate and give consent;
- Institutionalised at the time of symptom onset (living in a residence for people who require continual nursing care and have difficulty with activities of daily living).
2.4. Data Collection
2.5. Laboratory Analysis
2.6. Statistical Analysis
2.7. Ethical Approval and Consent
3. Results
3.1. Patient Population
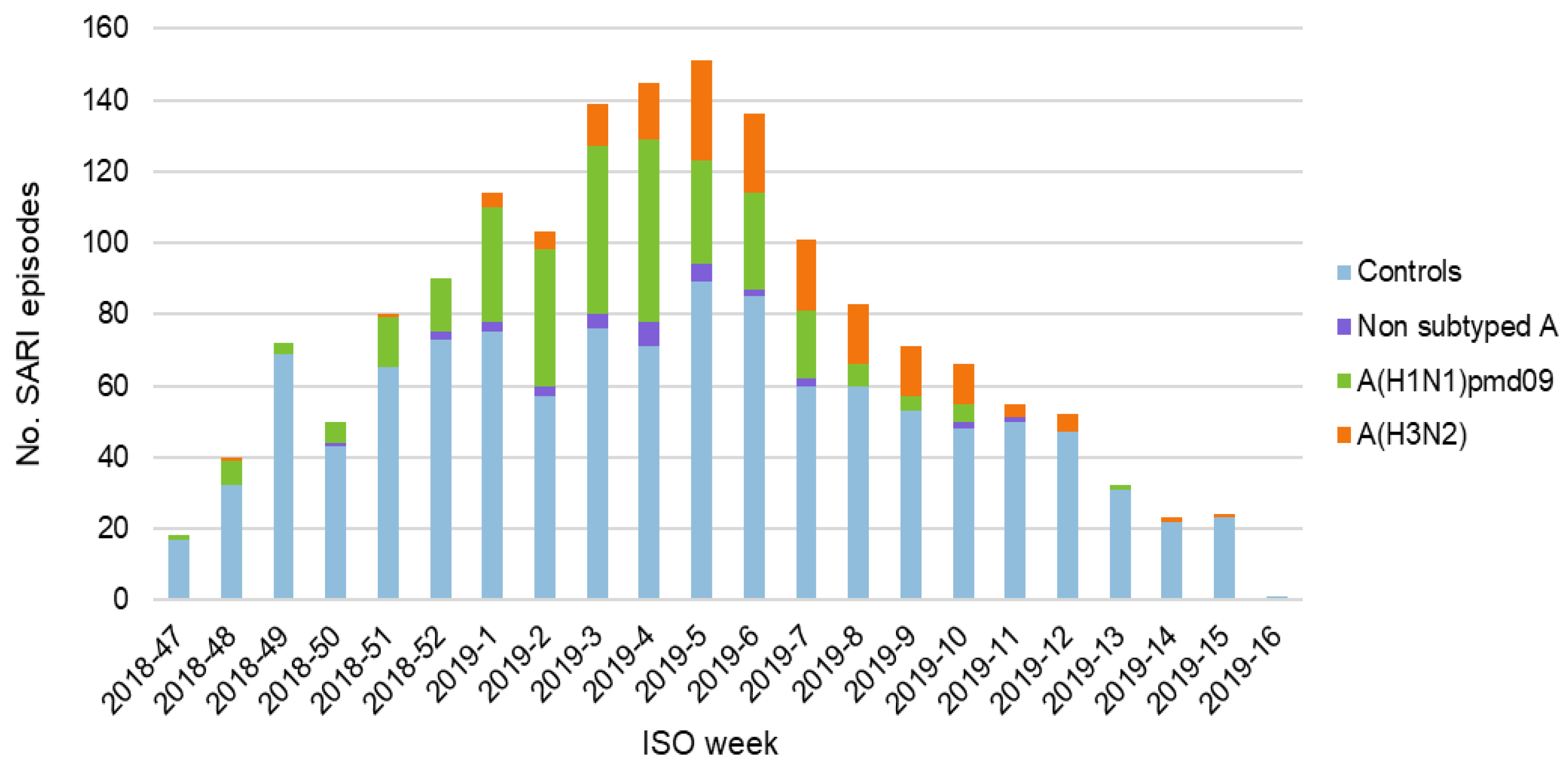
3.2. Surveillance Data
3.3. Vaccine Coverage
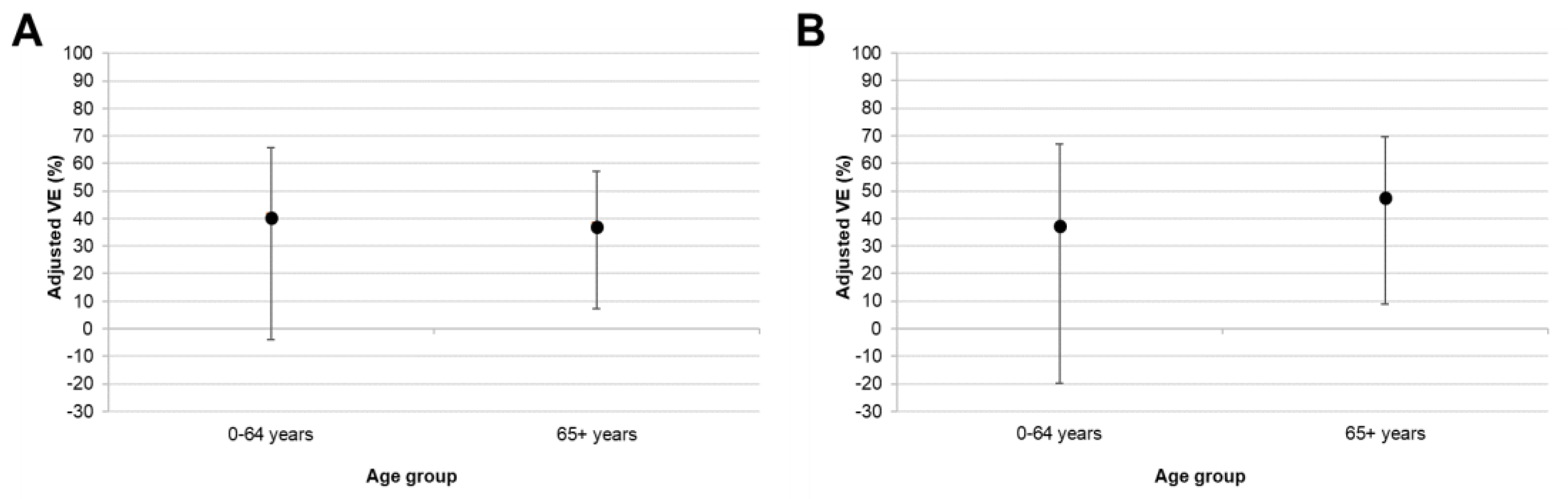
3.4. Vaccine Effectiveness
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- European Centre for Disease Prevention and Control. Seasonal Influenza Vaccination and Antiviral Use in EU/EEA Member States. Available online: https://www.ecdc.europa.eu/en/seasonal-influenza/prevention-and-control/vaccines/vaccination-coverage (accessed on 10 March 2020).
- Iuliano, A.D.; Roguski, K.M.; Chang, H.H.; Muscatello, D.J.; Palekar, R.; Tempia, S.; Cohen, C.; Gran, J.M.; Schanzer, D.; Cowling, B.J.; et al. Estimates of global seasonal influenza-associated respiratory mortality: A modelling study. Lancet 2018, 391, 1285–1300. [Google Scholar] [CrossRef]
- Rapporto Epidemiologico: Stagione Influenzale 2017–2018. Available online: https://www.epicentro.iss.it/influenza/pdf/Rapporto%20InfluNet%202018-17.pdf (accessed on 10 March 2020).
- Zhou, H.; Thompson, W.W.; Viboud, C.G.; Ringholz, C.M.; Cheng, P.Y.; Steiner, C.; Abedi, G.R.; Anderson, L.J.; Brammer, L.; Shay, D.K. Hospitalizations associated with influenza and respiratory syncytial virus in the United States, 1993–2008. Clin. Infect. Dis. 2012, 54, 1427–1436. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. A Manual for Estimating Disease Burden Associated with Seasonal Influenza. 2015. Available online: https://apps.who.int/iris/bitstream/handle/10665/178801/9789241549301_eng.pdf;jsessionid=60C107AA41C6FC91C3D2313F6DB1558E?sequence=1 (accessed on 10 March 2020).
- Ministero della Salute. La Conferenza Permanente Per i Rapporti Tra Lo Stato, Le Regioni e Le Provincie Autonome Di Trento e Di Bolzano. 2019. Available online: www.trovanorme.salute.gov.it/norme/renderNormsanPdf?anno=2019&codLeg=70621&parte=1%20&serie=null (accessed on 10 March 2020).
- Ministero della Salute. Vaccinazione Antinfluenzale: Stagione 2018–2019 Coperture Vaccinali per 100 Abitani. 2019. Available online: www.salute.gov.it/imgs/C_17_tavole_19_allegati_iitemAllegati_0_fileAllegati_itemFile_5_file.pdf (accessed on 10 March 2020).
- Rondy, M.; Kissling, E.; Emborg, H.D.; Gherasim, A.; Pebody, R.; Trebbien, R.; Pozo, F.; Larrauri, A.; McMenamin, J.; Valenciano, M.; et al. Interim 2017/18 influenza seasonal vaccine effectiveness: Combined results from five European studies. Eurosurveillance 2018, 23, 18-00086. [Google Scholar] [CrossRef] [PubMed]
- Bella, A.; Gesualdo, F.; Orsi, A.; Arcuri, C.; Chironna, M.; Loconsole, D.; Napoli, C.; Orsi, G.B.; Manini, I.; Montomoli, E.; et al. Effectiveness of the trivalent MF59 adjuvated influenza vaccine in preventing hospitalization due to influenza B and A(H1N1)pdm09 viruses in the elderly in Italy, 2017–2018 season. Expert Rev. Vaccines 2019, 18, 671–679. [Google Scholar] [CrossRef] [PubMed]
- Bellino, S.; Bella, A.; Puzelli, S.; Di Martino, A.; Facchini, M.; Punzo, O.; Pezzotti, P.; Castrucci, M.R.; The InfluNet Study Group. Moderate influenza vaccine effectiveness against A (H1N1) pdm09 virus, and low effectiveness against A (H3N2) subtype, 2018/19 season in Italy. Expert Rev. Vaccines 2019, 18, 1201–1209. [Google Scholar] [CrossRef] [PubMed]
- Costantino, C.; Restivo, V.; Amodio, E.; Colomba, G.M.E.; Vitale, F.; Tramuto, F. A mid-term estimate of 2018/2019 vaccine effectiveness to prevent laboratory confirmed A(H1N1)pdm09 and A(H3N2) influenza cases in Sicily (Italy). Vaccine 2019, 37, 5812–5816. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. Seasonal Influenza, Annual Epidemiological Report for 2018–2019. 2019. Available online: https://www.ecdc.europa.eu/en/publications-data/seasonal-influenza-annual-epidemiological-report-2018-2019 (accessed on 10 March 2020).
- Kissling, E.; Rose, A.; Emborg, H.D.; Gherasim, A.; Pebody, R.; Pozo, F.; Trebbien, R.; Mazagatos, C.; Whitaker, H.; Valenciano, M.; et al. Interim 2018/19 influenza vaccine effectiveness: Six European studies, October 2018 to January 2019. Eurosurveillance 2019, 24, 1900121. [Google Scholar] [CrossRef]
- Skowronski, D.M.; Leir, S.; Sabaiduc, S.; Murti, M.; Dickinson, J.A.; Olsha, R.; Gubbay, J.B.; Croxen, M.A.; Charest, H.; Chan, T.; et al. Interim estimates of 2018/19 vaccine effectiveness against influenza A(H1N1)pdm09, Canada, January 2019. Eurosurveillance 2019, 24, 1900055. [Google Scholar] [CrossRef] [PubMed]
- Doyle, J.D.; Chung, J.R.; Kim, S.S.; Gaglani, M.; Raiyani, C.; Zimmerman, R.K.; Nowalk, M.P.; Jackson, M.L.; Jackson, L.A.; Monto, A.S.; et al. Interim Estimates of 2018–19 Seasonal Influenza Vaccine Effectiveness—United States, February 2019. MMWR Morb. Mortal. Wkly. Rep. 2019, 68, 135–139. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Influenza virus Characterisation, March 2019. 2019. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/influenza-virus-characterisation-march-2019.pdf (accessed on 10 March 2020).




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Controls (n = 1167) | Cases (n = 500) | p-Value |
|---|---|---|---|
| Sex = male | 664 (56.9%) | 284 (56.8%) | 0.970 |
| Mean age (years) ± SD | 35.5 ± 34.8 | 35.3 ± 32.9 | 0.920 |
| Age group | 0.124 | ||
| 0–17 | 588 (50.4%) | 244 (45.8%) | |
| 18–64 years | 182 (15.6%) | 108 (21.6%) | |
| 65+ years | 397 (34.0%) | 148 (29.6%) | |
| Mean number of GP visits in past year ± SD | 2.26 ± 2.12 | 1.96 ± 2.12 | 0.015 * |
| Mean number of hospitalisations in past year ±SD | 0.98 ± 1.33 | 0.92 ± 1.50 | 0.266 |
| Smoking status | 0.000 *** | ||
| Never smoked | 781 (66.9%) | 327 (65.4%) | |
| Ex-smoker | 140 (12.0%) | 36 (7.2%) | |
| Occasional smoker | 69 (5.9%) | 18 (3.6%) | |
| Daily smoker | 177 (15.2%) | 119 (23.8%) | |
| Presence of chronic condition | 522 (44.7%) | 256 (51.2%) | 0.015 * |
| Lung disease | 249 (21.3%) | 109 (21.8%) | |
| Cardiovascular disease | 296 (25.4%) | 141 (28.2%) | |
| Diabetes | 144 (12.3%) | 42 (8.4%) | |
| Renal disease | 77 (6.6%) | 24 (4.8%) | |
| Cancer | 65 (5.6%) | 19 (3.8%) | |
| Liver disease | 22 (1.9%) | 9 (1.8%) | |
| Immunodeficiency | 15 (1.3%) | 6 (1.2%) | |
| Obesity | 35 (3.0%) | 19 (3.8%) | |
| Anaemia | 22 (1.9%) | 10 (2.0%) | |
| Dementia | 35 (3.0%) | 11 (2.2%) | |
| Rheumatic disease | 25 (2.1%) | 8 (1.6%) | |
| Age Group | No. People Vaccinated (%) | ||
|---|---|---|---|
| Controls | Cases | Total | |
| All ages | 260 (22.3%) | 85 (17.0%) | 345 (20.7%) |
| 0–17 years | 17 (2.9%) | 10 (4.1%) | 27 (3.2%) |
| 18–64 years | 36 (19.8%) | 13 (12.0%) | 49 (16.9%) |
| 65+ years | 207 (52.1%) | 62 (41.9%) | 269 (49.4%) |
| Influenza Subtype | VE (95% CI) | |||||||
|---|---|---|---|---|---|---|---|---|
| Any Seasonal Vaccine (n = 260 Controls, 85 Cases) | Fluad (n = 154 Controls, 51 Cases) | Fluarix Tetra (n = 83 Controls, 18 Cases) | Vaxigrip Tetra (n = 20 Controls, 14 Cases) | |||||
| Crude | Adjusted | Crude | Adjusted | Crude | Adjusted | Crude | Adjusted | |
| All type A | 28.5 (6.3 to 45.5) | 40.5 (18.7 to 56.4) | 27.6 (−14.1 to 48.3) | 40.2 (11.9 to 59.4) | 52.6 (20.1 to 71.9) | 63.2 (36.8 to 78.5) | −52.99 (−205.9 to 23.5) | −28.1 (−159.4 to 36.7) |
| A(H1N1)pdm09 | 54.4 (34.0 to 68.5) | 55.0 (34.5 to 69.1) | 60.0 (34.7 to 75.5) | 60.9 (35.7 to 76.2) | 66.3 (29.8 to 83.8) | 66.3 (29.4 to 83.9) | −20.45 (−169.0 to 46.1) | −18.7 (−169.3 to 47.6) |
| A(H3N2) | −54.5 (−122.8 to −7.1) | 2.5 (−50.0 to 36.7) | −69.7 (−162.5 to −9.7) | −17.0 (−98.2 to 30.9) | −0.8 (−105.0 to 50.5) | 42.9 (−20.8 to 73.0) | −120.7 (−443.9 to 10.4) | −49.8 (−294.9 to 43.2) |
| Influenza Subtype | Adjusted VE (95% CI) | |
|---|---|---|
| 0–64 Years (n = 770 Controls, 352 Cases) | 65+ Years (n = 397 Controls, 148 Cases) | |
| All type A | 40.4 (−3.8 to 65.8) | 37.1 (7.3 to 57.3) |
| A(H1N1)pdm09 | 37.2 (−19.7 to 67.1) | 47.5 (8.9 to 69.7) |
| A(H3N2) | 23.4 (−7.2 to 66.0) | −2.7 (−0.74 to 39.4) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rizzo, C.; Gesualdo, F.; Loconsole, D.; Pandolfi, E.; Bella, A.; Orsi, A.; Guarona, G.; Panatto, D.; Icardi, G.; Napoli, C.; et al. Moderate Vaccine Effectiveness against Severe Acute Respiratory Infection Caused by A(H1N1)pdm09 Influenza Virus and No Effectiveness against A(H3N2) Influenza Virus in the 2018/2019 Season in Italy. Vaccines 2020, 8, 427. https://doi.org/10.3390/vaccines8030427
Rizzo C, Gesualdo F, Loconsole D, Pandolfi E, Bella A, Orsi A, Guarona G, Panatto D, Icardi G, Napoli C, et al. Moderate Vaccine Effectiveness against Severe Acute Respiratory Infection Caused by A(H1N1)pdm09 Influenza Virus and No Effectiveness against A(H3N2) Influenza Virus in the 2018/2019 Season in Italy. Vaccines. 2020; 8(3):427. https://doi.org/10.3390/vaccines8030427
Chicago/Turabian StyleRizzo, Caterina, Francesco Gesualdo, Daniela Loconsole, Elisabetta Pandolfi, Antonino Bella, Andrea Orsi, Giulia Guarona, Donatella Panatto, Giancarlo Icardi, Christian Napoli, and et al. 2020. "Moderate Vaccine Effectiveness against Severe Acute Respiratory Infection Caused by A(H1N1)pdm09 Influenza Virus and No Effectiveness against A(H3N2) Influenza Virus in the 2018/2019 Season in Italy" Vaccines 8, no. 3: 427. https://doi.org/10.3390/vaccines8030427
APA StyleRizzo, C., Gesualdo, F., Loconsole, D., Pandolfi, E., Bella, A., Orsi, A., Guarona, G., Panatto, D., Icardi, G., Napoli, C., Orsi, G. B., Manini, I., Montomoli, E., Campagna, I., Russo, L., Alfonsi, V., Puzelli, S., Reale, A., Raucci, U., ... Tozzi, A. E. (2020). Moderate Vaccine Effectiveness against Severe Acute Respiratory Infection Caused by A(H1N1)pdm09 Influenza Virus and No Effectiveness against A(H3N2) Influenza Virus in the 2018/2019 Season in Italy. Vaccines, 8(3), 427. https://doi.org/10.3390/vaccines8030427