Epidemiologic Profile of Type-Specific Human Papillomavirus Infection after Initiation of HPV Vaccination

 ,
,  ,
, 
 ,
,
Abstract
1. Introduction
2. Material and Methods
3. Results
3.1. Background of Participants
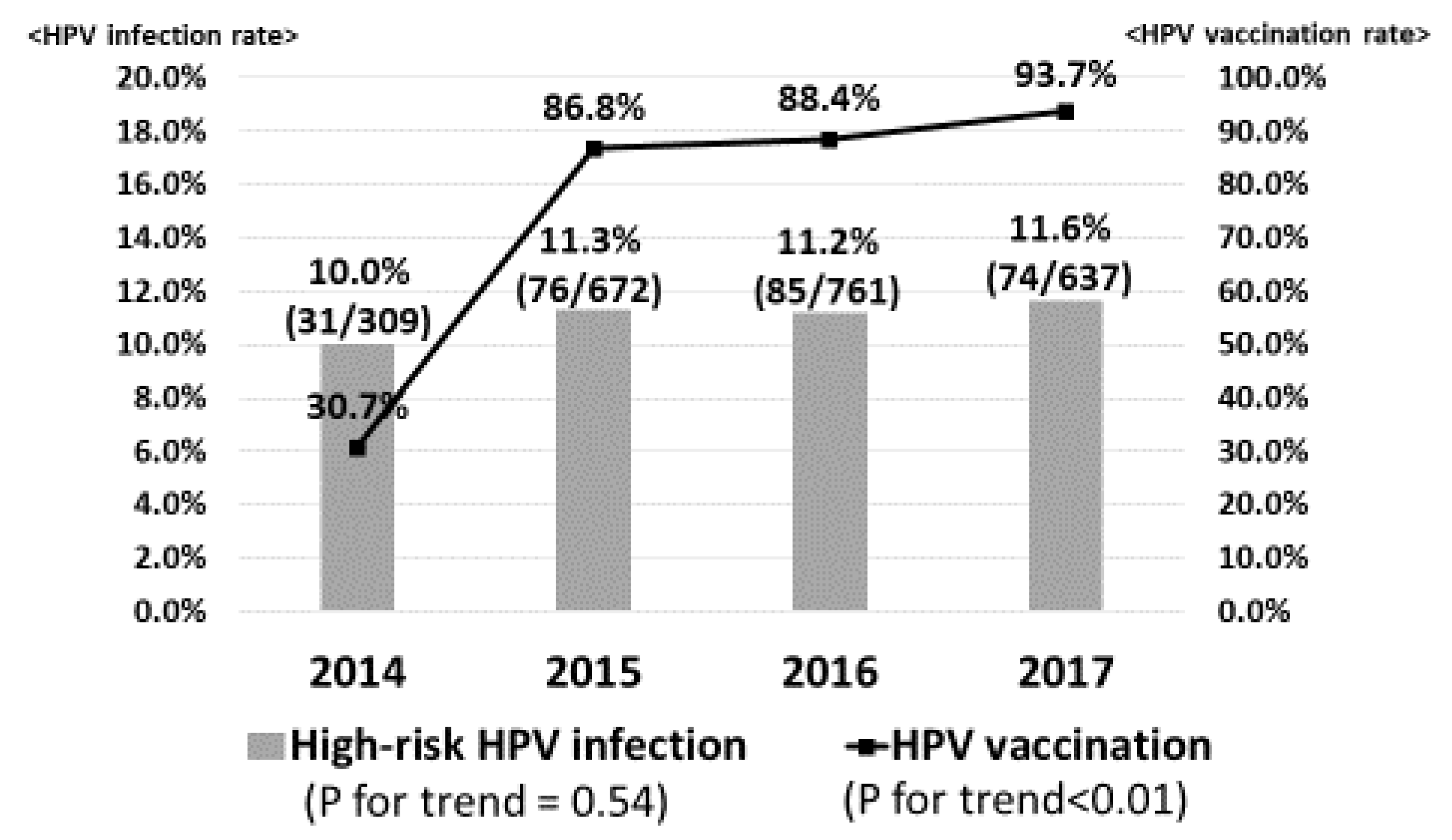
3.2. Prevalence of HPV Infection Rate
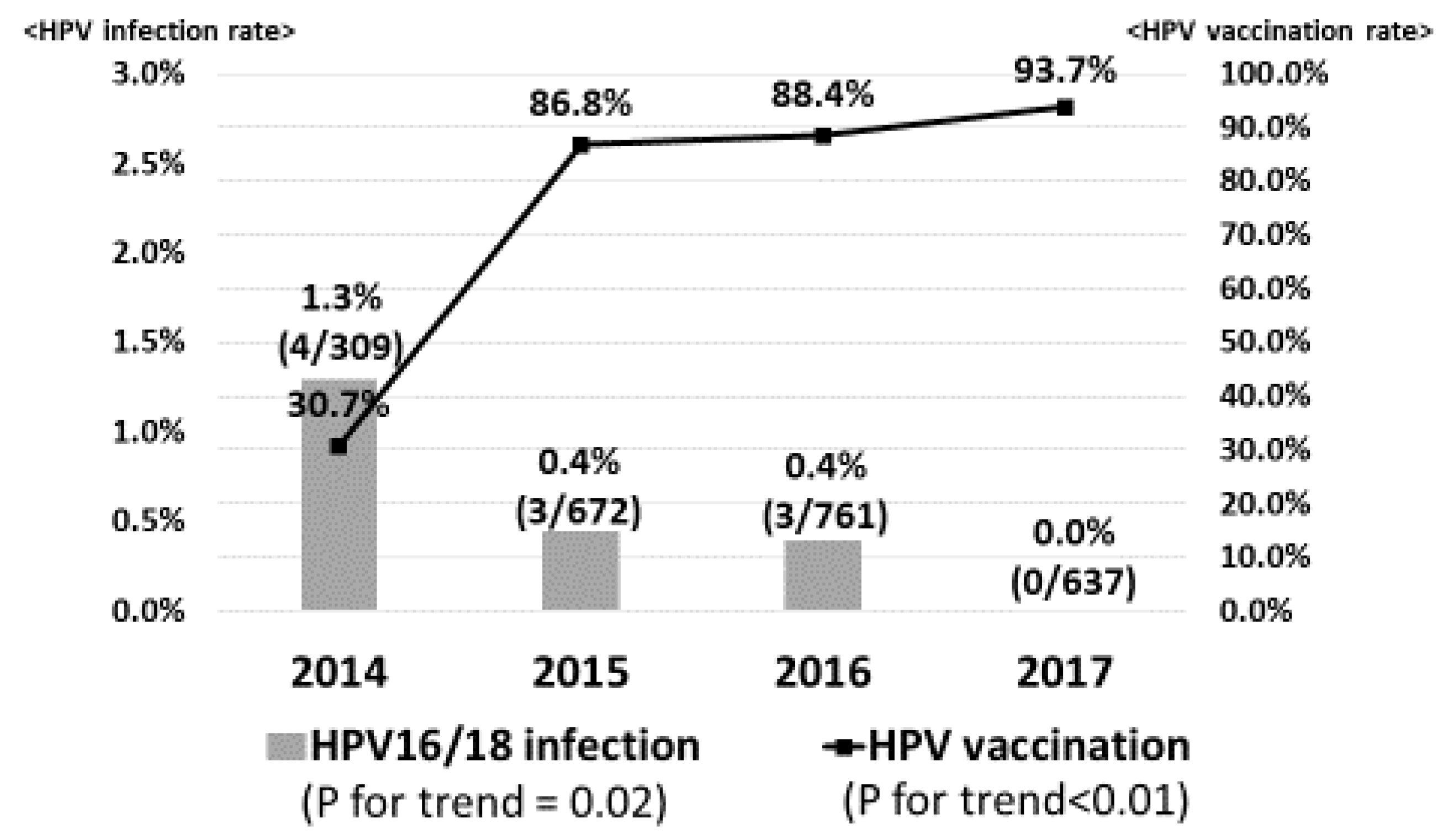
3.3. Profile of Type-Specific HPV Infection
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cancer Registry and Statistics. Cancer Information Service, National Cancer Center, Japan. Available online: https://ganjoho.jp/reg_stat/statistics/dl/ (accessed on 1 June 2020).
- Motoki, Y.; Mizushima, S.; Taguri, M.; Takahashi, K.; Asano, R.; Kato, H.; Asai-Sato, M.; Katayama, K.; Okamoto, N.; Hirahara, F.; et al. Increasing trends in cervical cancer mortality among young Japanese women below the age of 50 years: An analysis using the Kanagawa population-based Cancer Registry, 19752–012. Cancer Epidemiol. 2015, 39, 700–706. [Google Scholar] [CrossRef] [PubMed]
- Sekine, M.; Kudo, R.; Adachi, S.; Yamaguchi, M.; Ueda, Y.; Takata, T.; Morimoto, A.; Tanaka, Y.; Yagi, A.; Miyagi, E.; et al. Japanese Crisis of HPV Vaccination. Int. Pathol. Clin. Res. 2016. [Google Scholar] [CrossRef]
- Hanley, S.J.; Yoshioka, E.; Ito, Y.; Kishi, R. HPV vaccination crisis in Japan. Lancet 2015, 385, 2571. [Google Scholar] [CrossRef]
- Ozaki, S.; Kato, K.; Abe, Y.; Hara, H.; Kubota, H.; Kubushiro, K.; Kawahara, E.; Inoue, M. Analytical performance of newly developed multiplex human papillomavirus genotyping assay using Luminex xMAP technology (Mebgen HPV Kit). J. Virol. Methods 2014, 204, 73–80. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Nakagawa, S.; Ueda, Y.; Yagi, A.; Ikeda, S.; Hiramatsu, K.; Kimura, T. Corrected human papillomavirus vaccination rates for each birth fiscal year in Japan. Cancer Sci. 2020, 111, 2156. [Google Scholar] [CrossRef]
- Azuma, Y.; Kusumoto-Matsuo, R.; Takeuchi, F.; Uenoyama, A.; Kondo, K.; Tsunoda, H.; Nagasaka, K.; Kawana, K.; Morisada, T.; Iwata, T.; et al. Human papillomavirus genotype distribution in cervical intraepithelial neoplasia grade 2/3 and invasive cervical cancer in Japanese women. Jpn. J. Clin. Oncol. 2014, 44, 910–917. [Google Scholar] [CrossRef]
- Onuki, M.; Matsumoto, K.; Satoh, T.; Oki, A.; Okada, S.; Minaguchi, T.; Ochi, H.; Nakao, S.; Someya, K.; Yamada, N.; et al. Human papillomavirus infections among Japanese women: Age-related prevalence and type-specific risk for cervical cancer. Cancer Sci. 2009, 100, 1312–1316. [Google Scholar] [CrossRef]
- Munoz, N.; Bosch, F.X.; Castellsagué, X.; Díaz, M.; De Sanjose, S.; Hammouda, D.; Shah, K.V.; Meijer, C.J. Against which human papillomavirus types shall we vaccinate and screen? The international perspective. Int. J. Cancer 2004, 111, 278–285. [Google Scholar] [CrossRef]
- Khan, M.J.; Castle, P.E.; Lorincz, A.T.; Wacholder, S.; Sherman, M.; Scott, D.R.; Rush, B.B.; Glass, A.G.; Schiffman, M. The elevated 10-year risk of cervical precancer and cancer in women with human papillomavirus (HPV) type 16 or 18 and the possible utility of type-specific HPV testing in clinical practice. J. Natl. Cancer Inst. 2005, 97, 1072–1079. [Google Scholar] [CrossRef]
- Hosaka, M.; Fujita, H.; Hanley, S.J.; Sasaki, T.; Shirakawa, Y.; Abiko, M.; Kudo, M.; Kaneuchi, M.; Watari, H.; Kikuchi, K.; et al. Incidence risk of cervical intraepithelial neoplasia 3 or more severe lesions is a function of human papillomavirus genotypes and severity of cytological and histological abnormalities in adult Japanese women. Int. J. Cancer 2013, 132, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, T.F.; Spaczynski, M.; Schneider, A.; Wysocki, J.; Galaj, A.; Perona, P.; Poncelet, S.; Zahaf, T.; Hardt, K.; Descamps, D.; et al. Immunogenicity and tolerability of an HPV-16/18 AS04-adjuvanted prophylactic cervical cancer vaccine in women aged 155–5 years. Vaccine 2009, 27, 581–587. [Google Scholar] [CrossRef] [PubMed]
- Lehtinen, M.; Dillner, J. Clinical trials of human papillomavirus vaccines and beyond. Nat. Rev. Clin. Oncol. 2013, 10, 400–410. [Google Scholar] [CrossRef] [PubMed]
- Joura, E.A.; Giuliano, A.R.; Iversen, O.E.; Bouchard, C.; Mao, C.; Mehlsen, J.; Moreira, E.D., Jr.; Ngan, Y.; Petersen, L.K.; Lazcano-Ponce, E.; et al. A 9-valent HPV vaccine against infection and intraepithelial neoplasia in women. N. Engl. J. Med. 2015, 372, 711–723. [Google Scholar] [CrossRef] [PubMed]
- Tabrizi, S.N.; Brotherton, J.M.; Kaldor, J.M.; Skinner, S.R.; Liu, B.; Bateson, D.; McNamee, K.; Garefalakis, M.; Phillips, S.; Cummins, E.; et al. Assessment of herd immunity and cross-protection after a human papillomavirus vaccination programme in Australia: A repeat cross-sectional study. Lancet Infect. Dis. 2014, 14, 958–966. [Google Scholar] [CrossRef]
- Cameron, R.L.; Kavanagh, K.; Pan, J.; Love, J.; Cuschieri, K.; Robertson, C.; Ahmed, S.; Palmer, T.; Pollock, K.G. Human Papillomavirus Prevalence and Herd Immunity after Introduction of Vaccination Program, Scotland, 2009–2013. Emerg. Infect Dis. 2016, 22, 56–64. [Google Scholar] [CrossRef]
- Berenson, A.B.; Hirth, J.M.; Chang, M. Change in Human Papillomavirus Prevalence Among, U.S. Women Aged 18–59 Years, 2009–2014. Obstet. Gynecol. 2017, 130, 693–701. [Google Scholar] [CrossRef]
- Tanaka, Y.; Ueda, Y.; Egawa-Takata, T.; Yagi, A.; Yoshino, K.; Kimura, T. Outcomes for girls without HPV vaccination in Japan. Lancet Oncol. 2016, 17, 868–869. [Google Scholar] [CrossRef]
- Mesher, D.; Soldan, K.; Lehtinen, M.; Beddows, S.; Brisson, M.; Brotherton, J.M.; Chow, E.P.; Cummings, T.; Drolet, M.; Fairley, C.K.; et al. Population-Level Effects of Human Papillomavirus Vaccination Programs on Infections with Nonvaccine Genotypes. Emerg. Infect. Dis. 2016, 22, 1732. [Google Scholar] [CrossRef]
- Drolet, M.; Benard, E.; Perez, N.; Brisson, M. Population-level impact and herd effects following the introduction of human papillomavirus vaccination programmes: Updated systematic review and meta-analysis. Lancet 2019, 394, 497–509. [Google Scholar] [CrossRef]
- Lehtinen, M.; Luostarinen, T.; Vänskä, S.; Söderlund-Strand, A.; Eriksson, T.; Natunen, K.; Apter, D.; Baussano, I.; Harjula, K.; Hokkanen, M.; et al. Gender-neutral vaccination provides improved control of human papillomavirus types 18/31/33/35 through herd immunity: Results of a community randomized trial (III). Int. J. Cancer 2018, 143, 2299–2310. [Google Scholar] [CrossRef]
- Woestenberg, P.J.; King, A.J.; Van Benthem, B.H.; Donken, R.; Leussink, S.; Van Der Klis, F.R.; De Melker, H.E.; Van Der Sande, M.A.; Hoebe, C.J.; Bogaards, J.A. Bivalent Vaccine Effectiveness Against Type-Specific HPV Positivity: Evidence for Cross-Protection Against Oncogenic Types Among Dutch STI Clinic Visitors. J. Infect. Dis. 2018, 217, 213–222. [Google Scholar] [CrossRef] [PubMed]
- Gray, P.; Palmroth, J.; Luostarinen, T.; Apter, D.; Dubin, G.; Garnett, G.; Eriksson, T.; Natunen, K.; Merikukka, M.; Pimenoff, V.; et al. Evaluation of HPV type-replacement in unvaccinated and vaccinated adolescent females-Post-hoc analysis of a community-randomized clinical trial (II). Int. J. Cancer 2018, 142, 2491–2500. [Google Scholar] [CrossRef] [PubMed]
- Tota, J.E.; Struyf, F.; Merikukka, M.; Gonzalez, P.; Kreimer, A.R.; Bi, D.; Castellsagué, X.; De Carvalho, N.S.; Garland, S.M.; Harper, D.M.; et al. Evaluation of Type Replacement Following HPV16/18 Vaccination: Pooled Analysis of Two Randomized Trials. JNCI J. Natl. Cancer Inst. 2017, 109. [Google Scholar] [CrossRef]
- Kudo, R.; Yamaguchi, M.; Sekine, M.; Adachi, S.; Ueda, Y.; Miyagi, E.; Hara, M.; Hanley, S.J.; Enomoto, T. Bivalent Human Papillomavirus Vaccine Effectiveness in a Japanese Population: High Vaccine-Type-Specific Effectiveness and Evidence of Cross-Protection. J. Infect. Dis. 2019, 219, 382–390. [Google Scholar] [CrossRef] [PubMed]
- Man, I.; Vänskä, S.; Lehtinen, M.; Bogaards, J.A. Human papillomavirus genotype replacement: Still too early to tell? J. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Pons-Salort, M.; Thiébaut, A.C.; Guillemot, D.; Favre, M.; Delarocque-Astagneau, E. HPV genotype replacement: Too early to tell. Lancet Infect. Dis. 2013, 13, 1012. [Google Scholar] [CrossRef]
- Gray, P.; Luostarinen, T.; Vänskä, S.; Eriksson, T.; Lagheden, C.; Man, I.; Palmroth, J.; Pimenoff, V.N.; Söderlund-Strand, A.; Dillner, J.; et al. Occurrence of human papillomavirus (HPV) type replacement by sexual risk-taking behaviour group: Post-hoc analysis of a community randomized clinical trial up to 9 years after vaccination (IV). Int. J. Cancer 2019, 145, 785–796. [Google Scholar] [CrossRef]
- Covert, C.; Ding, L.; Brown, D.; Franco, E.L.; Bernstein, D.I.; Kahn, J.A. Evidence for cross-protection but not type-replacement over the 11 years after human papillomavirus vaccine introduction. Hum Vaccines Immunother. 2019, 15, 1962–1969. [Google Scholar] [CrossRef]
- Chatterjee, A. The next generation of HPV vaccines: Nonavalent vaccine V503 on the horizon. Exp. Rev. Vaccines 2014, 13, 1279–1290. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Fiscal Year | 20 Years | 21 Years | (Age) |
|---|---|---|---|
| 2014 | 1994 | 1993 | (Birth year) |
| 2015 | 1995 | 1994 | (Birth year) |
| 2016 | 1996 | 1995 | (Birth year) |
| 2017 | 1997 | 1996 | (Birth year) |
| 1993: pre-OHPV generation | |||
| 1994–1997: OHPV generation | |||
| 2014 | 2015 | 2016 | 2017 | p-Value | |||||
|---|---|---|---|---|---|---|---|---|---|
| n = 309 | n = 672 | n = 761 | n = 637 | ||||||
| HPV Vaccination | 95 | (30.7%) | 583 | (86.6%) | 673 | (88.4%) | 597 | (93.7%) | <0.01 * |
| Age at sexual debut | 17.5 | (±1.9) | 17.4 | (±1.9) | 17.3 | (±1.8) | 17.5 | (±1.8) | 0.27 † |
| Number of sexual partners | |||||||||
| ≥10 | 24 | (7.8%) | 36 | (5.4%) | 49 | (6.4%) | 32 | (5.0%) | 0.08 * |
| 6–9 | 15 | (4.9%) | 50 | (7.4%) | 46 | (6.0%) | 26 | (4.1%) | |
| 2–5 | 118 | (38.2%) | 244 | (36.3%) | 251 | (33.0%) | 206 | (32.3%) | |
| 0–1 | 141 | (45.6%) | 283 | (42.1%) | 352 | (46.3%) | 308 | (48.4%) | |
| 2014 (n = 309) | 2015–2017 (n = 2070) | ||||
|---|---|---|---|---|---|
| Genotyping | n | % | Genotyping | n | % |
| HPV52 | 10 | 3.24% | HPV52 | 64 | 3.09% |
| HPV16 | 4 | 1.29% | HPV58 | 45 | 2.17% |
| HPV56 | 4 | 1.29% | HPV56 | 41 | 1.98% |
| HPV33 | 2 | 0.65% | HPV51 | 30 | 1.45% |
| HPV51 | 2 | 0.65% | HPV59 | 28 | 1.35% |
| HPV58 | 2 | 0.65% | HPV39 | 20 | 0.97% |
| HPV68 | 2 | 0.65% | HPV68 | 15 | 0.72% |
| HPV31 | 1 | 0.32% | HPV31 | 7 | 0.34% |
| HPV39 | 1 | 0.32% | HPV33 | 7 | 0.34% |
| HPV59 | 1 | 0.32% | HPV35 | 6 | 0.29% |
| HPV18 | 0 | 0.00% | HPV16 | 5 | 0.24% |
| HPV35 | 0 | 0.00% | HPV45 | 3 | 0.14% |
| HPV45 | 0 | 0.00% | HPV18 | 1 | 0.05% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sekine, M.; Yamaguchi, M.; Kudo, R.; J. B. Hanley, S.; Hara, M.; Adachi, S.; Ueda, Y.; Miyagi, E.; Ikeda, S.; Yagi, A.; et al. Epidemiologic Profile of Type-Specific Human Papillomavirus Infection after Initiation of HPV Vaccination. Vaccines 2020, 8, 425. https://doi.org/10.3390/vaccines8030425
Sekine M, Yamaguchi M, Kudo R, J. B. Hanley S, Hara M, Adachi S, Ueda Y, Miyagi E, Ikeda S, Yagi A, et al. Epidemiologic Profile of Type-Specific Human Papillomavirus Infection after Initiation of HPV Vaccination. Vaccines. 2020; 8(3):425. https://doi.org/10.3390/vaccines8030425
Chicago/Turabian StyleSekine, Masayuki, Manako Yamaguchi, Risa Kudo, Sharon J. B. Hanley, Megumi Hara, Sosuke Adachi, Yutaka Ueda, Etsuko Miyagi, Sayaka Ikeda, Asami Yagi, and et al. 2020. "Epidemiologic Profile of Type-Specific Human Papillomavirus Infection after Initiation of HPV Vaccination" Vaccines 8, no. 3: 425. https://doi.org/10.3390/vaccines8030425
APA StyleSekine, M., Yamaguchi, M., Kudo, R., J. B. Hanley, S., Hara, M., Adachi, S., Ueda, Y., Miyagi, E., Ikeda, S., Yagi, A., & Enomoto, T. (2020). Epidemiologic Profile of Type-Specific Human Papillomavirus Infection after Initiation of HPV Vaccination. Vaccines, 8(3), 425. https://doi.org/10.3390/vaccines8030425