Rubella Vaccine Introduction in the South African Public Vaccination Schedule: Mathematical Modelling for Decision Making

 ,
,  ,
,
Abstract
1. Introduction
2. Methods
2.1. Age-Structured Rubella Model
2.2. Vaccine Introduction Scenarios
2.3. Evaluating Costs of RCV Introduction
2.4. Evaluating DALYs Averted by RCV Introduction
2.5. Evaluating Impact on Outbreak Risk
3. Results
3.1. Rubella Incidence
3.2. CRS Incidence
3.3. CRS Cases Averted
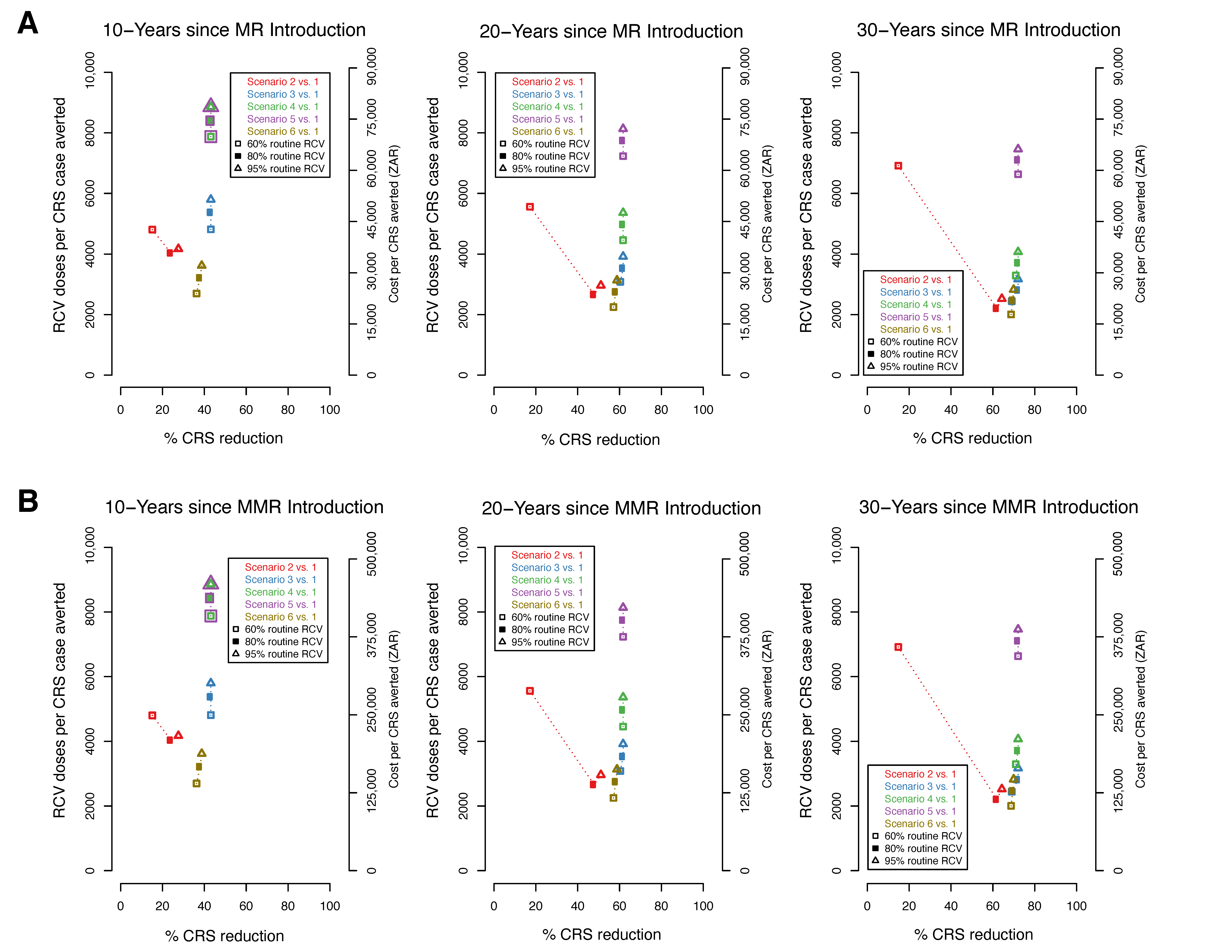
3.4. Efficiency of RCV to Reduce CRS Cases
3.5. Effective Reproductive Number (RE)
4. Discussion
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Alter, S.J.; Bennett, J.S.; Koranyi, K.; Kreppel, A.; Simon, R. Common Childhood Viral Infections. Curr. Probl. Pediatr. Adolesc. Health Care 2015, 45, 21–53. [Google Scholar] [CrossRef] [PubMed]
- Castillo-Solorzano, C.; Marsigli, C.; Bravo-Alcantara, P.; Flannery, B.; Ruiz Matus, C.; Tambini, G.; Gross-Galiano, S.; Andrus, J.K. Elimination of Rubella and Congenital Rubella Syndrome in the Americas. J. Infect. Dis. 2011, 204, S571–S578. [Google Scholar] [CrossRef]
- Panagiotopoulos, T.; Antoniadou, I.; Valassi-Adam, E. Increase in congenital rubella occurrence after immunisation in Greece: Retrospective survey and systematic review. BMJ 1999, 319, 1462–1467. [Google Scholar] [CrossRef]
- Jiménez, G.; Avila-Aguero, M.L.; Morice, A.; Gutiérrez, H.; Soriano, A.; Badilla, X.; Reef, S.; Castillo-Solorzano, C. Estimating the Burden of Congenital Rubella Syndrome in Costa Rica, 1996–2001. Pediatr. Infect. Dis. J. 2007, 26, 382–386. [Google Scholar] [CrossRef] [PubMed]
- Hinman, A.R.; Irons, B.; Lewis, M.; Kandola, K. Economic analyses of rubella and rubella vaccines: A global review. Bull. World Health Organ. 2002, 7, 264–270. [Google Scholar]
- World Health Organization Rubella vaccines. WHO Position Paper. Wkly. Epidemiol. Rec. 2011, 29, 301–316. [Google Scholar]
- DeRoeck, D.; Wang, S.A. Principles and Considerations for Adding a Vaccine to a National Immunization Programme: From Decision to Implementation and Monitoring; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- World Health Organization. Introducing Rubella Vaccine into National Immunization Programmes: A Step-By-Step Guide; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- Endean, C. Gavi Progress Report 2015; The Global Alliance for Vaccines and Immunization: Geneva, Switzerland, 2015. [Google Scholar]
- WHO. Global Measles And Rubella Strategic Plan; WHO: Geneva, Switzerland, 2012. [Google Scholar]
- Motaze, N.V.; Suchard, M.S.; Cohen, C.; Baker, L.; Blumberg, L. Vaccine Information For Parents and Caregivers; Centre for Vaccines and Immunology, National Institute for Communicable Diseases, National Health Laboratory Service, South Africa: Johannesburg, South Africa, 2016.
- Knox, E.G. Strategy for Rubella Vaccination. Int. J. Epidemiol. 1980, 9, 13. [Google Scholar] [CrossRef] [PubMed]
- Cutts, F.T.; Metcalf, C.J.E.; Lessler, J.; Grenfell, B.T. Rubella vaccination: Must not be business as usual. Lancet 2012, 380, 217–218. [Google Scholar] [CrossRef]
- Vynnycky, E.; Adams, E.J.; Cutts, F.T.; Reef, S.E.; Navar, A.M.; Simons, E.; Yoshida, L.-M.; Brown, D.W.; Jackson, C.; Strebel, P.M.; et al. Using seroprevalence and immunisation coverage data to estimate the global burden of congenital rubella syndrome, 1996–2010: A systematic review. PLoS ONE 2016, 11, e0149160. [Google Scholar] [CrossRef] [PubMed]
- Cutts, F.T.; Vynnucky, E. Modelling incidence of CRS in developing countries. Int. J. Epid. 1999, 28, 1179–1184. [Google Scholar] [CrossRef]
- Metcalf, C.J.E.; Lessler, J.; Klepac, P.; Cutts, F.; Grenfell, B.T. Impact of birth rate, seasonality and transmission rate on minimum levels of coverage needed for rubella vaccination. Epidemiol. Infect. 2012, 140, 2290–2301. [Google Scholar] [CrossRef]
- Wesolowski, A.; Mensah, K.; Brook, C.E.; Andrianjafimasy, M.; Winter, A.; Buckee, C.O.; Razafindratsimandresy, R.; Tatem, A.J.; Heraud, J.-M.; Metcalf, C.J.E. Introduction of rubella-containing-vaccine to Madagascar: Implications for roll-out and local elimination. J. R. Soc. Interface 2016, 13, 20151101. [Google Scholar] [CrossRef]
- Winter, A.K. Integrating Data, Demography, and Dynamics to Inform Vaccination Policy: Measles and Rubella in a Changing World; Princeton University: Princeton, NJ, USA, 2016. [Google Scholar]
- Metcalf, C.J.E.; Cohen, C.; Lessler, J.; McAnerney, J.M.; Ntshoe, G.M.; Puren, A.; Klepac, P.; Tatem, A.; Grenfell, B.T.; Bjornstad, O.N. Implications of spatially heterogeneous vaccination coverage for the risk of congenital rubella syndrome in South Africa. J. R. Soc. Interface 2012, 10, 20120756. [Google Scholar] [CrossRef]
- Metcalf, C.J.E.; Lessler, J.; Klepac, P.; Morice, A.; Grenfell, B.T.; Bjørnstad, O.N. Structured models of infectious disease: Inference with discrete data. Theor. Popul. Biol. 2012, 82, 275–282. [Google Scholar] [CrossRef] [PubMed]
- Lessler, J.; Metcalf, C.J.E. Balancing evidence and uncertainty when considering rubella vaccine introduction. PLoS ONE 2013, 8, e67639. [Google Scholar] [CrossRef] [PubMed]
- Cutts, F.T.; Abebe, A.; Messele, T.; Dejene, A.; Enquselassie, F.; Nigatu, W.; Nokes, D.J. Sero-epidemiology of rubella in the urban population of Addis Ababa, Ethiopia. Epidemiol. Infect. 2000, 124, 467–479. [Google Scholar] [CrossRef] [PubMed]
- Metcalf, C.J.E.; BjøRnstad, O.N.; Ferrari, M.J.; Klepac, P.; Bharti, N.; Lopez-Gatell, H.; Grenfell, B.T. The epidemiology of rubella in Mexico: Seasonality, stochasticity and regional variation. Epidemiol. Infect. 2011, 139, 1029–1038. [Google Scholar] [CrossRef]
- Wesolowski, A.; Metcalf, C.J.E.; Eagle, N.; Kombich, J.; Grenfell, B.T.; Bjørnstad, O.N.; Lessler, J.; Tatem, A.J.; Buckee, C.O. Quantifying seasonal population fluxes driving rubella transmission dynamics using mobile phone data. Proc. Natl. Acad. Sci. USA 2015, 112, 11114–11119. [Google Scholar] [CrossRef]
- Mahmud, A.; Metcalf, C.J.E.; Grenfell, B. Comparative dynamics, seasonality in transmission, and predictability of childhood infections in Mexico. Epidemiol. Inf. 2017, 145, 607–625. [Google Scholar] [CrossRef]
- Mossong, J.; Hens, N.; Jit, M.; Beutels, P.; Auranen, K.; Mikolajczyk, R.; Massari, M.; Salmaso, S.; Tomba, G.S.; Wallinga, J.; et al. Social contacts and mixing patterns relevant to the spread of infectious diseases. PLoS Med. 2008, 5, e74. [Google Scholar] [CrossRef]
- Bjornstad, O.N.; Finkenstadt, B.F.; Grenfell, B.T. Dynamics of Measles Epidemics: Estimating Scaling of Transmission Rates Using a Time Series SIR Model. Ecol. Monogr. 2002, 72, 169–184. [Google Scholar] [CrossRef]
- Nicoara, C.; Zäch, K.; Trachsel, D.; Germann, D.; Matter, L. Decay of Passively Acquired Maternal Antibodies against Measles, Mumps, and Rubella Viruses. Clin. Diagn. Lab. Immunol. 1999, 6, 868–871. [Google Scholar] [CrossRef] [PubMed]
- Boulianne, N.; De Serres, G.; Ratnam, S.; Ward, B.J.; Joly, J.R.; Duval, B. Measles, Mumps, and Rubella Antibodies in Children 5–6 Years After Immunization: Effect of Vaccine Type and Age at Vaccination. Vaccine 1995, 13, 1611–1616. [Google Scholar] [CrossRef]
- United Nations, Population Division. World Population Prospects, 2015. Available online: https://www.un.org/en/development/desa/publications/world-population-prospects-2015-revision.html (accessed on 11 March 2016).
- World Health Organization WHO and UNICEF Review of National Immunization Coverage, 1980–2016: South Africa. Available online: http://www.who.int/immunization/monitoring_surveillance/data/zaf.pdf (accessed on 7 September 2017).
- South African Medicine Price Registry Database of Medicine Prices, 2019. Available online: https://health-e.org.za/medicine-price-registry/ (accessed on 12 May 2019).
- World Health Organization. MI4A/V3P Vaccine Purchase Database, 2019. Available online: https://www.who.int/immunization/programmes_systems/procurement/mi4a/platform/module1/en/ (accessed on 12 May 2019).
- Simons, E.A.; Reef, S.E.; Cooper, L.Z.; Zimmerman, L.; Thompson, K.M. Systematic Review of the Manifestations of Congenital Rubella Syndrome in Infants and Characterization of Disability-Adjusted Life Years (DALYs): Manifestations of Congenital Rubella Syndrome in Infants and Characterization of DALYs. Risk Anal. 2016, 36, 1332–1356. [Google Scholar] [CrossRef] [PubMed]
- GIVS. Global Immunization Vision and Strategy: 2006–2015; WHO: Geneva, Switzerland, 2005. [Google Scholar]
- Vynnycky, E.; White, R. An Introduction to Infectious Disease Modelling; Oxford University Press: Oxford, UK, 2010. [Google Scholar]
- Gay, N.J.; Hesketh, L.; Morgan-Capner, P.; Miller, E. Interpretation of serological surveillance data for mathematical models: Implications for vaccine. Age 1995, 15, 24. [Google Scholar]
- Hens, N.; Abrams, S.; Santermans, E.; Theeten, H.; Goeyvaerts, N.; Lernout, T.; Leuridan, E.; Van Kerckhove, K.; Goossens, H.; Van Damme, P.; et al. Assessing the risk of measles resurgence in a highly vaccinated population: Belgium anno 2013. Eurosurveillance 2015, 20. [Google Scholar] [CrossRef]
- Diekmann, O.; Heesterbeek, J.; Metz, J. On the Definition and the Computation of the Basic Reproduction Ratio R0 in Models for Infectious Diseases in Heterogeneous Populations. J. Math. Biol. 1990, 28, 365–382. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Scenario | Routine Vaccination in Expanded Program on Immunization (EPI) | Target Age Group for Routine Vaccination | Target Age Group for Initial Mass Campaign | Follow-Up Mass Campaigns | |
|---|---|---|---|---|---|
| Target Age Group | Timing | ||||
| 1 | No RCV in EPI | ||||
| 2 | RCV introduction | 1 year | No initial campaign | No follow-up campaign | N/A |
| 3 | RCV introduction | 1 year | 1 to 14 years | No follow-up campaign | N/A |
| 4 | RCV introduction | 1 year | 1 to 14 years | 1 to 4 years | One follow-up campaign 5 years after initial campaign |
| 5 | RCV introduction | 1 year | 1 to 14 years | 1 to 4 years | Six follow-up campaigns every 5 years after initial campaign for 30 years |
| 6 | RCV introduction | 1 year and 9 years | No initial campaign | No follow-up campaign | N/A |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Motaze, N.V.; Edoka, I.; Wiysonge, C.S.; Metcalf, C.J.E.; Winter, A.K. Rubella Vaccine Introduction in the South African Public Vaccination Schedule: Mathematical Modelling for Decision Making. Vaccines 2020, 8, 383. https://doi.org/10.3390/vaccines8030383
Motaze NV, Edoka I, Wiysonge CS, Metcalf CJE, Winter AK. Rubella Vaccine Introduction in the South African Public Vaccination Schedule: Mathematical Modelling for Decision Making. Vaccines. 2020; 8(3):383. https://doi.org/10.3390/vaccines8030383
Chicago/Turabian StyleMotaze, Nkengafac Villyen, Ijeoma Edoka, Charles S. Wiysonge, C. Jessica E. Metcalf, and Amy K. Winter. 2020. "Rubella Vaccine Introduction in the South African Public Vaccination Schedule: Mathematical Modelling for Decision Making" Vaccines 8, no. 3: 383. https://doi.org/10.3390/vaccines8030383
APA StyleMotaze, N. V., Edoka, I., Wiysonge, C. S., Metcalf, C. J. E., & Winter, A. K. (2020). Rubella Vaccine Introduction in the South African Public Vaccination Schedule: Mathematical Modelling for Decision Making. Vaccines, 8(3), 383. https://doi.org/10.3390/vaccines8030383