The Impact of Locoregional Treatment on Response to Nivolumab in Advanced Platinum Refractory Head and Neck Cancer: The Need Trial

 ,
,  ,
,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Treatment and Assessments
2.3. Statistical Analysis
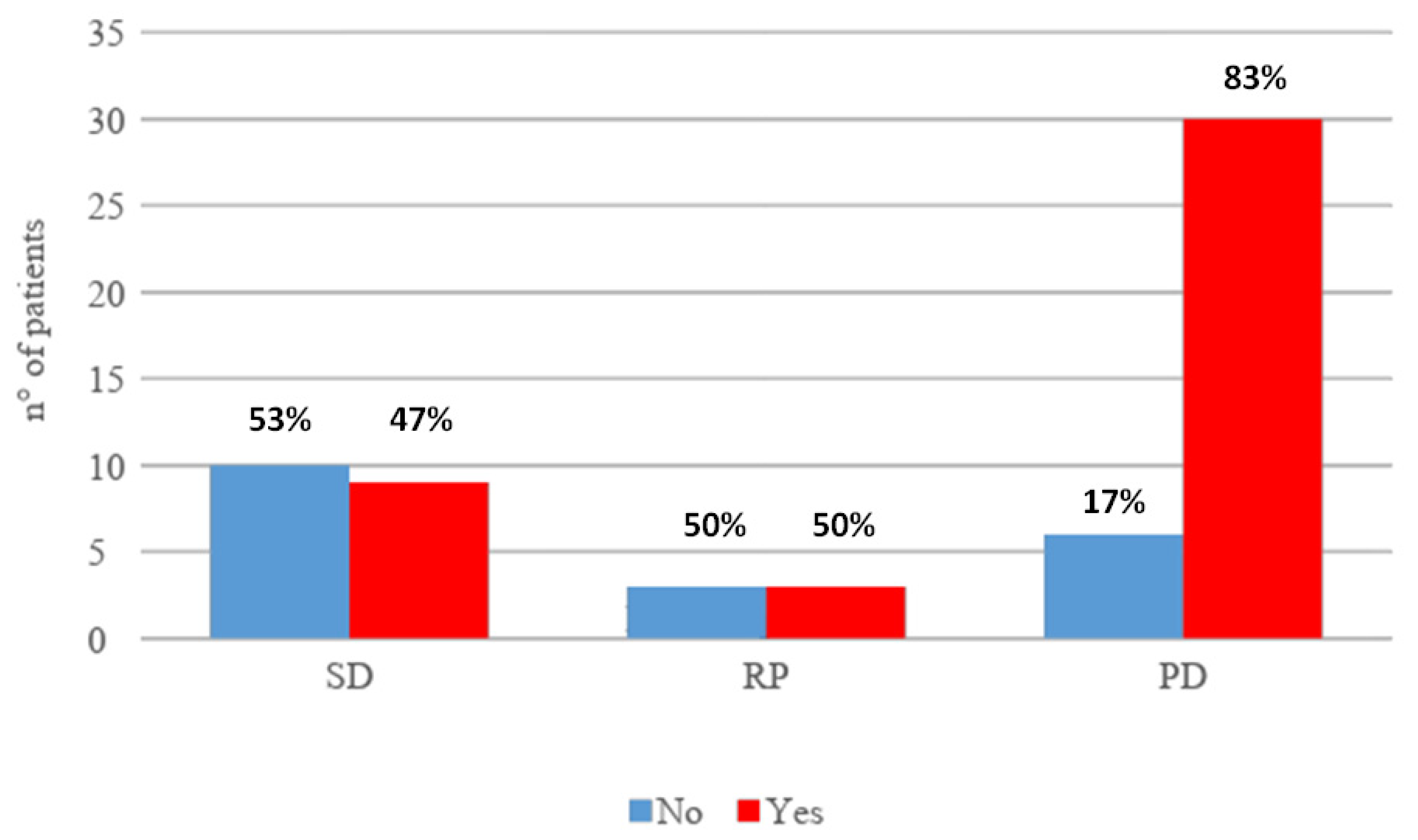
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Kreimer, A.R.; Clifford, G.M.; Boyle, P.; Franceschi, S. Human papillomavirus types in head and neck squamous cell carcinomas worldwide: A systematic review. Cancer Epidemiol. Prev. Biomark. 2005, 14, 467–475. [Google Scholar] [CrossRef] [PubMed]
- Marur, S.; Forastiere, A.A. Head and Neck Squamous Cell Carcinoma: Update on Epidemiology, Diagnosis, and Treatment. Mayo Clin. Proc. 2016, 91, 386–396. [Google Scholar] [CrossRef] [PubMed]
- El Rassy, E.; Assi, T.; Bakouny, Z.; El Karak, F.; Pavlidis, N.; Ghosn, M. Comparison of second-line treatment of recurrent and/or metastatic squamous cell carcinoma of the head and neck. Future Oncol. 2019, 15, 909–923. [Google Scholar] [CrossRef] [PubMed]
- Ferris, R.L.; Blumenschein, G., Jr.; Fayette, J.; Guigay, J.; Colevas, A.D.; Licitra, L.; Harrington, K.; Kasper, S.; Vokes, E.E.; Even, C.; et al. Nivolumab for Recurrent Squamous-Cell Carcinoma of the Head and Neck. N. Engl. J. Med. 2016, 375, 1856–1867. [Google Scholar] [CrossRef] [PubMed]
- Haratani, K.; Hayashi, H.; Chiba, Y.; Kudo, K.; Yonesaka, K.; Kato, R.; Kaneda, H.; Hasegawa, Y.; Tanaka, K.; Takeda, M.; et al. Association of immunerelated adverse events with nivolumab efficacy in non small-cell lung cancer. JAMA Oncol. 2018, 4, 374–378. [Google Scholar] [CrossRef]
- Teraoka, S.; Fujimoto, D.; Morimoto, T.; Kawachi, H.; Ito, M.; Sato, Y.; Nagata, K.; Nakagawa, A.; Otsuka, K.; Uehara, K.; et al. Early Immune-Related Adverse Events and Association with Outcome in Advanced Non-Small Cell Lung Cancer Patients Treated with Nivolumab: A Prospective Cohort Study. J. Thorac. Oncol. 2017, 12, 1798–1805. [Google Scholar] [CrossRef]
- Downey, S.G.; Klapper, J.A.; Smith, F.O.; Yang, J.C.; Sherry, R.M.; Royal, R.E.; Kammula, U.S.; Hughes, M.S.; Allen, T.E.; Levy, C.L.; et al. Prognostic factors related to clinical response in patients with metastatic melanoma treated by CTL-associated antigen-4 blockade. Clin. Cancer Res. 2007, 13 Pt 1, 6681–6688. [Google Scholar] [CrossRef]
- Freeman-Keller, M.; Kim, Y.; Cronin, H.; Richards, A.; Gibney, G.; Weber, J.S. Nivolumab in resected and unresectable metastatic melanoma: Characteristics of immune-related adverse events and association with outcomes. Clin. Cancer Res. 2016, 22, 886–894. [Google Scholar] [CrossRef]
- Gandhi, L.; Rodríguez-Abreu, D.; Gadgeel, S.; Esteban, E.; Felip, E.; De Angelis, F.; Domine, M.; Clingan, P.; Hochmair, M.J.; Powell, S.F.; et al. Pembrolizumab plus Chemotherapy in Metastatic Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 2078–2092. [Google Scholar] [CrossRef]
- Okamoto, I.; Sato, H.; Kondo, T.; Koyama, N.; Fushimi, C.; Okada, T.; Miura, K.; Matsuki, T.; Yamashita, T.; Omura, G.; et al. Efficacy and safety of nivolumab in 100 patients with recurrent or metastatic head and neck cancer—A retrospective multicentre study. Acta Otolaryngol. 2019, 139, 918–925. [Google Scholar] [CrossRef] [PubMed]
- Botticelli, A.; Salati, M.; Di Pietro, F.R.; Strigari, L.; Cerbelli, B.; Zizzari, I.G.; Giusti, R.; Mazzotta, M.; Mazzuca, F.; Roberto, M.; et al. A nomogram to predict survival in non-small cell lung cancer patients treated with nivolumab. J. Transl. Med. 2019, 17, 99. [Google Scholar] [CrossRef] [PubMed]
- Botticelli, A.; Onesti, C.E.; Zizzari, I.; Cerbelli, B.; Sciattella, P.; Occhipinti, M.; Roberto, M.; Di Pietro, F.; Bonifacino, A.; Ghidini, M.; et al. The sexist behaviour of immune checkpoint inhibitors in cancer therapy? Oncotarget 2017, 8, 99336–99346. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.D.; van der Most, R.; Vivian, J.B.; Lake, R.A.; Larma, I.; Robinson, B.W.; Currie, A.J. Loss of antigen cross-presentation after complete tumor resection is associated with the generation of protective tumor-specific CD8(+) T-cell immunity. Oncoimmunology 2012, 1, 1084–1094. [Google Scholar] [CrossRef] [PubMed]
- de Biasi, A.R.; Villena-Vargas, J.; Adusumilli, P.S. Cisplatin induced antitumour immunomodulation: A review of preclinical and clinical evidence. Clin. Cancer Res. 2014, 20, 5384–5391. [Google Scholar] [CrossRef]
- Zheng, Y.; Dou, Y.; Duan, L.; Cong, C.; Gao, A.; Lai, Q.; Sun, Y. Using chemo-drugs or irradiation to break immune tolerance and facilitate immunotherapy in solid cancer. Cell Immunol. 2015, 294, 54–59. [Google Scholar] [CrossRef]
- Hiniker, S.M.; Maecker, H.T.; Knox, S.J. Predictors of clinical response to immunotherapy with or without radiotherapy. J. Radiat. Oncol. 2015, 4, 339–345. [Google Scholar] [CrossRef]
- Weichselbaum, R.R.; Liang, H.; Deng, L.; Fu, Y.X. Radiotherapy and immunotherapy: A beneficial liaison? Nat. Rev. Clin. Oncol. 2017, 14, 365–379. [Google Scholar] [CrossRef]
- Seymour, L.; Bogaerts, J.; Perrone, A.; Ford, R.; Schwartz, L.H.; Mandrekar, S.; Lin, N.U.; Litière, S.; Dancey, J.; Chen, A.; et al. iRECIST: Guidelines for response criteria for use in trials testing immunotherapeutics. [published correction appears in Lancet Oncol. 2019 May;20(5):e242]. Lancet Oncol. 2017, 18, e143–e152. [Google Scholar] [CrossRef]
- Vermorken, J.B.; Mesia, R.; Rivera, F.; Remenar, E.; Kawecki, A.; Rottey, S.; Erfan, J.; Zabolotnyy, D.; Kienzer, H.R.; Cupissol, D.; et al. Platinum-based chemotherapy plus cetuximab in head and neck cancer. N. Engl. J. Med. 2008, 359, 1116–1127. [Google Scholar] [CrossRef]
- Wang, C.; Thudium, K.B.; Han, M.; Wang, X.T.; Huang, H.; Feingersh, D.; Garcia, C.; Wu, Y.; Kuhne, M.; Srinivasan, M.; et al. In vitro characterization of the anti-PD-1 antibody nivolumab, BMS-936558, and in vivo toxicology in non-human primates. Cancer Immunol. Res. 2014, 2, 846–856. [Google Scholar] [CrossRef] [PubMed]
- Hirano, F.; Kaneko, K.; Tamura, H.; Dong, H.; Wang, S.; Ichikawa, M.; Rietz, C.; Flies, D.B.; Lau, J.S.; Zhu, G.; et al. Blockade of B7-H1 and PD-1 bymonoclonal antibodies potentiates cancer therapeutic immunity. Cancer Res. 2005, 65, 1089–1096. [Google Scholar] [PubMed]
- Wong, R.M.; Scotland, R.R.; Lau, R.L.; Wang, C.; Korman, A.J.; Kast, W.M.; Weber, J.S. Programmed death-1 blockade enhances expansion and functional capacity of human melanoma antigen-specific CTLs. Int. Immunol. 2007, 19, 1223–1234. [Google Scholar] [CrossRef] [PubMed]
- Cheng, P.; Mottram, P.; Krzysiek, R.; Knutson, K.L.; Daniel, B.; Zimmermann, M.C.; David, O.; Burow, M.; Gordon, A.; Dhurandhar, N.; et al. Blockade of B7-H1 improves myeloid dendritic cell-mediated antitumor immunity. Nat. Med. 2003, 9, 562–567. [Google Scholar] [CrossRef]
- Liu, J.; Blake, S.J.; Yong, M.C.; Harjunpää, H.; Ngiow, S.F.; Takeda, K.; Young, A.; O’Donnell, J.S.; Allen, S.; Smyth, M.J.; et al. Improved efficacy of neoadjuvant compared to adjuvant immunotherapy to eradicate metastatic disease. Cancer Discov. 2016, 6, 1382–1399. [Google Scholar] [CrossRef] [PubMed]
- Gough, M.J.; Crittenden, M.R.; Sarff, M.; Pang, P.; Seung, S.K.; Vetto, J.T.; Hu, H.M.; Redmond, W.L.; Holland, J.; Weinberg, A.D. Adjuvant therapy with agonistic antibodies to CD134 (OX40) increases local control after surgical or radiation therapy of cancer in mice. J. Immunother. 2010, 33, 798–809. [Google Scholar] [CrossRef]
- Vanpouille-Box, C.; Pilones, K.A.; Wennerberg, E.; Formenti, S.C.; Demaria, S. In situ vaccination by radiotherapy to improve responses to anti-CTLA-4 treatment. Vaccine 2015, 33, 7415–7422. [Google Scholar] [CrossRef]
- Tai, L.H.; de Souza, C.T.; Bélanger, S.; Ly, L.; Alkayyal, A.A.; Zhang, J.; Rintoul, J.L.; Ananth, A.A.; Lam, T.; Breitbach, C.J.; et al. Preventing postoperative metastatic disease by inhibiting surgery-induced dysfunction in natural killer cells. Cancer Res. 2013, 73, 97–107. [Google Scholar] [CrossRef]
- van der Bij, G.J.; Oosterling, S.J.; Beelen, R.H.; Meijer, S.; Coffey, J.C.; van Egmond, M. The perioperative period is an underutilized window of therapeutic opportunity in patients with colorectal cancer. Ann. Surg. 2009, 249, 727–734. [Google Scholar] [CrossRef]
- Bakos, O.; Lawson, C.; Rouleau, S.; Tai, L.H. Combining surgery and immunotherapy: Turning an immunosuppressive effect into a therapeutic opportunity. J. Immunother. Cancer 2018, 6, 86. [Google Scholar] [CrossRef]
- Buettner, M.; Bode, U. Lymph node dissection--understanding the immunological function of lymph nodes. Clin. Exp. Immunol. 2012, 169, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, H.A.; Villar, R.C. Radiotherapy and immune response: The systemic effects of a local treatment. Clinics 2018, 73 (suppl. 1), e557s. [Google Scholar] [CrossRef]
- Rodríguez-Ruiz, M.E.; Vanpouille-Box, C.; Melero, I.; Formenti, S.C.; Demaria, S. Immunological Mechanisms Responsible for Radiation-Induced Abscopal Effect. Trends Immunol. 2018, 39, 644–655. [Google Scholar] [CrossRef] [PubMed]
- Rosen, E.M.; Fan, S.; Rockwell, S.; Goldberg, I.D. The molecular and cellular basis of radiosensitivity: Implications for understanding how normal tissues and tumors respond to therapeutic radiation. Cancer Invest. 1999, 17, 56–72. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | All Patients N 61 (%) |
|---|---|
| Age (years) | |
| Median Age (range) | 67 (30–82) |
| Gender | |
| Male | 50 (82) |
| Female | 11 (18) |
| Baseline PS 1 before nivolumab | |
| 0 | 11 (18) |
| 1 | 34(55.7) |
| 2 | 16 (26.2) |
| Risk factors | |
| Smoking history | 32 (52.5) |
| Alcohol abuse | 17 (27.9) |
| Tumor Location | |
| Oral cavity | 14 (23) |
| Oropharynx | 14 (23) |
| Hypopharynx | 8 (13.1) |
| Larynx | 19(31.1) |
| Other | 6 (9.8) |
| Histology | |
| Squamous Cell Carcinoma | 61 (100) |
| Grading | |
| 2 | 9 (14.8) |
| 3 | 33 (54) |
| Missing | 19 (31.2) |
| HPV 2 | |
| Positive | 2 (3.3) |
| Negative | 11 (18) |
| Not reported | 48 (78.7) |
| Recurrent Disease Metastatic site | 11 (18) |
| 50 (82) | |
| Previous locoregional treatment | 42 (69) |
| Surgery | 9 (14.7) |
| Chemoradiotherapy | 9 (14.7) |
| Surgery and Chemoradiotherapy | 24 (39.3) |
| First line platinum-based chemotherapy | 53 (87) |
| Previous Carboplatin | 27 (44) |
| Previous Cisplatin | 28 (46) |
| Unknown | 6 (10) |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| Characteristic | OR 1 (95% CI 2) | p | OR (95% CI) | p |
| Sex | ||||
| female vs. male | 3.83 (0.75–19.56) | 0.106 | 4.82 (0.62–37.50) | 0.133 |
| Age | 0.99 (0.94–1.04) | 0.580 | 0.94 (0.87–1.02) | 0.151 |
| Alcohol history | 1.39 (0.44–4.44) | |||
| yes vs. not | 0.575 | 1.26 (0.26–7.96) | 0.775 | |
| Smoking | ||||
| Yes vs. not | 0.36 (0.12–1.11) | 0.075 | 0.32 (0.07–1.49) | 0.147 |
| Subsite | ||||
| Oropharynx | 1.31 (0.32–5.43) | 0.711 | 2.38 (0.31–18.18) | 0.403 |
| Hypopharynx | 0.73 (0.14–3.82) | 0.707 | 0.60 (0.07–4.89) | 0.635 |
| Oral cavity | 1.82 (0.42–7.94) | 0.427 | 1.42 (0.22–9.02) | 0.713 |
| Larynx | 1.00 (1.00–1.00) | 1.00 (1.00–1.00) | 0.382 | |
| Others | 0.36 (0.05–2.50) | 0.303 | 0.27 (0.01–5.03) | |
| Locoregional treatment | ||||
| yes vs. not | 5.42 (1.67–17.56) | 0.005 4 | 5.41 (1.02–28.74) | 0.048 5 |
| Platinum-CT 3 | ||||
| Cisplatin | 0.42 (0.14–1.28) | 0.127 | 0.31 (0.08–1.25) | 0.099 |
| Carboplatin | 1.00 (1.00–1.00) | 1.00 (1.00–1.00) | ||
| Unknown | 0.42 (0.07–2.55) | 0.347 | 0.30 (0.02–4.38) | 0.378 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Botticelli, A.; Mezi, S.; Pomati, G.; Sciattella, P.; Cerbelli, B.; Roberto, M.; Mammone, G.; Cirillo, A.; Cassano, A.; Di Dio, C.; et al. The Impact of Locoregional Treatment on Response to Nivolumab in Advanced Platinum Refractory Head and Neck Cancer: The Need Trial. Vaccines 2020, 8, 191. https://doi.org/10.3390/vaccines8020191
Botticelli A, Mezi S, Pomati G, Sciattella P, Cerbelli B, Roberto M, Mammone G, Cirillo A, Cassano A, Di Dio C, et al. The Impact of Locoregional Treatment on Response to Nivolumab in Advanced Platinum Refractory Head and Neck Cancer: The Need Trial. Vaccines. 2020; 8(2):191. https://doi.org/10.3390/vaccines8020191
Chicago/Turabian StyleBotticelli, Andrea, Silvia Mezi, Giulia Pomati, Paolo Sciattella, Bruna Cerbelli, Michela Roberto, Giulia Mammone, Alessio Cirillo, Alessandra Cassano, Carmela Di Dio, and et al. 2020. "The Impact of Locoregional Treatment on Response to Nivolumab in Advanced Platinum Refractory Head and Neck Cancer: The Need Trial" Vaccines 8, no. 2: 191. https://doi.org/10.3390/vaccines8020191
APA StyleBotticelli, A., Mezi, S., Pomati, G., Sciattella, P., Cerbelli, B., Roberto, M., Mammone, G., Cirillo, A., Cassano, A., Di Dio, C., Cortellini, A., Pizzuti, L., Ronzino, G., Salati, M., Vici, P., Polimeni, A., Merlano, M. C., Nuti, M., & Marchetti, P. (2020). The Impact of Locoregional Treatment on Response to Nivolumab in Advanced Platinum Refractory Head and Neck Cancer: The Need Trial. Vaccines, 8(2), 191. https://doi.org/10.3390/vaccines8020191