Seroprevalence to Measles Virus after Vaccination or Natural Infection in an Adult Population, in Italy

 , ,
, , 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Cells and Viruses
2.3. Measles IgM/IgG Antibody Detection
2.4. Measles Microneutralization Test
2.5. Statistical Analysis
3. Results
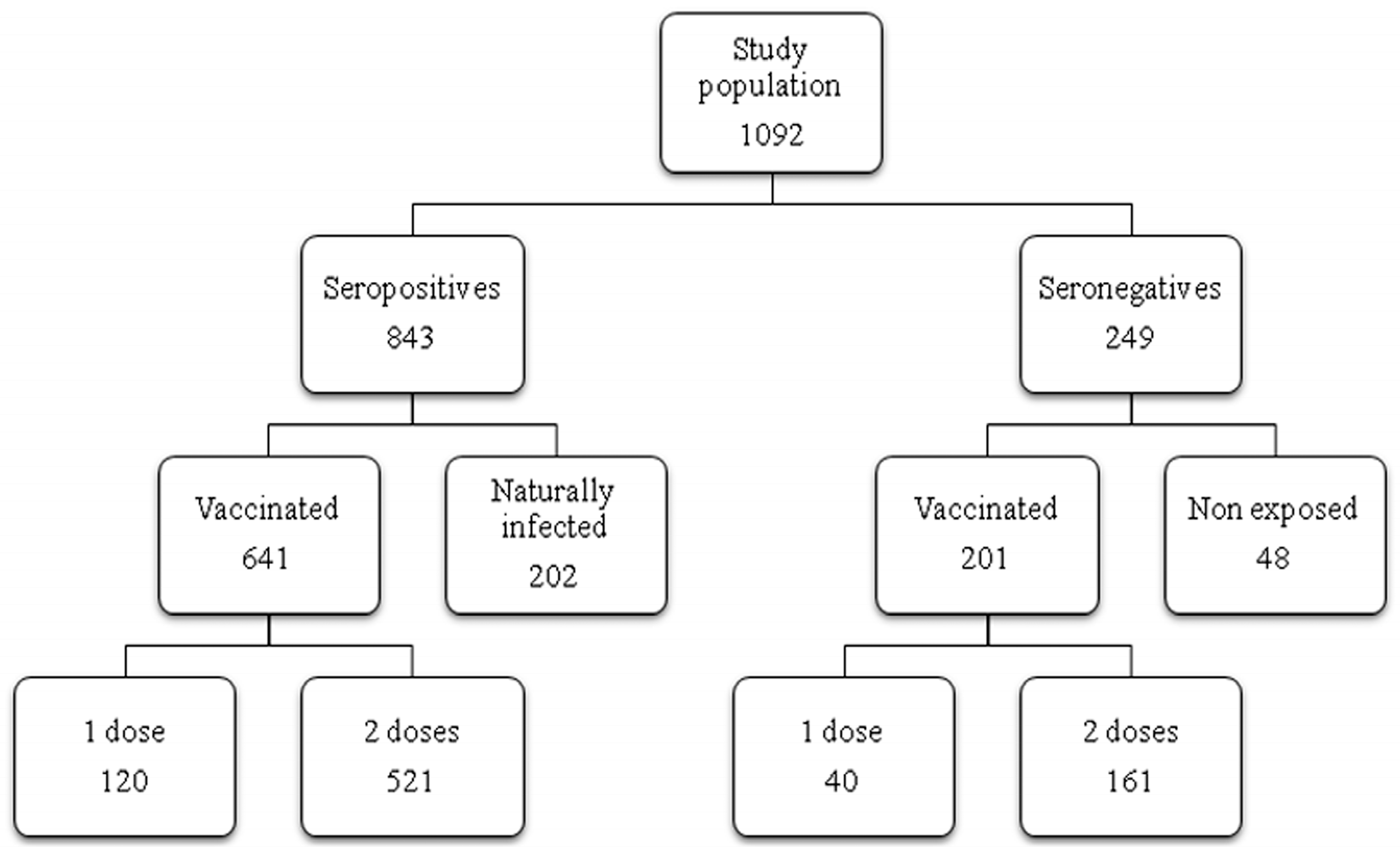
3.1. Study Group
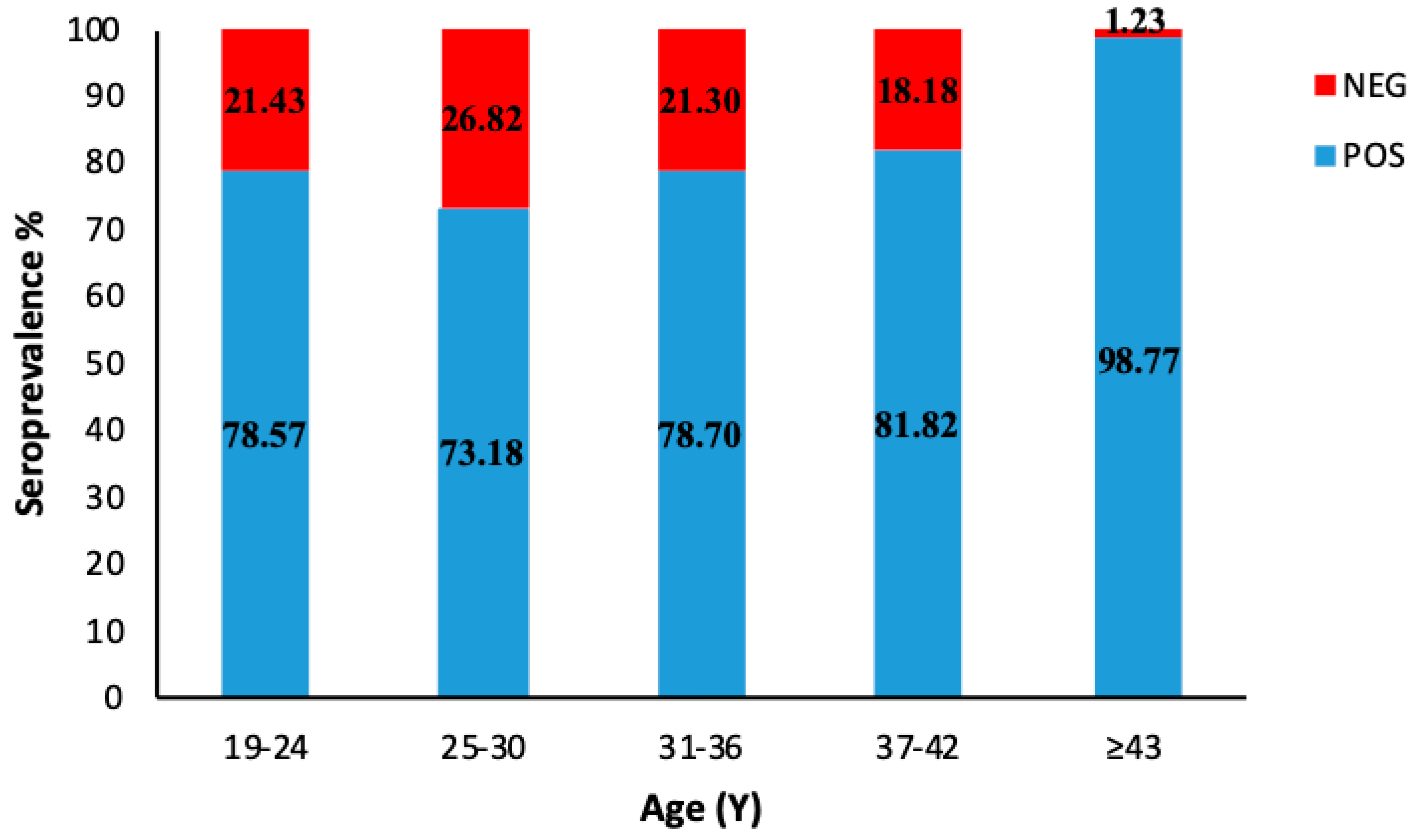
3.2. Age-Specific IgG prevalence
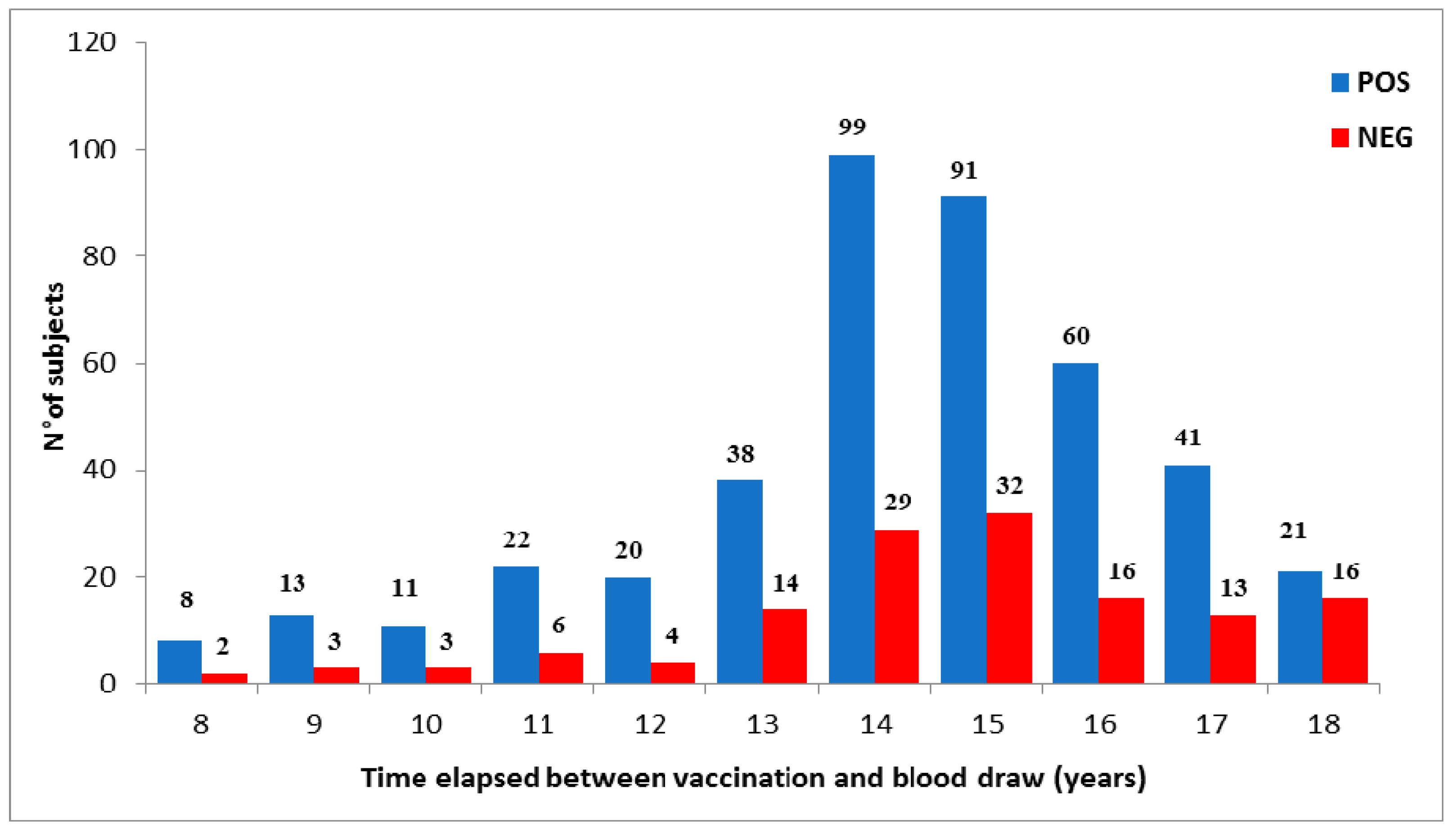
3.3. Decline of Humoral Response to Measles after Vaccination
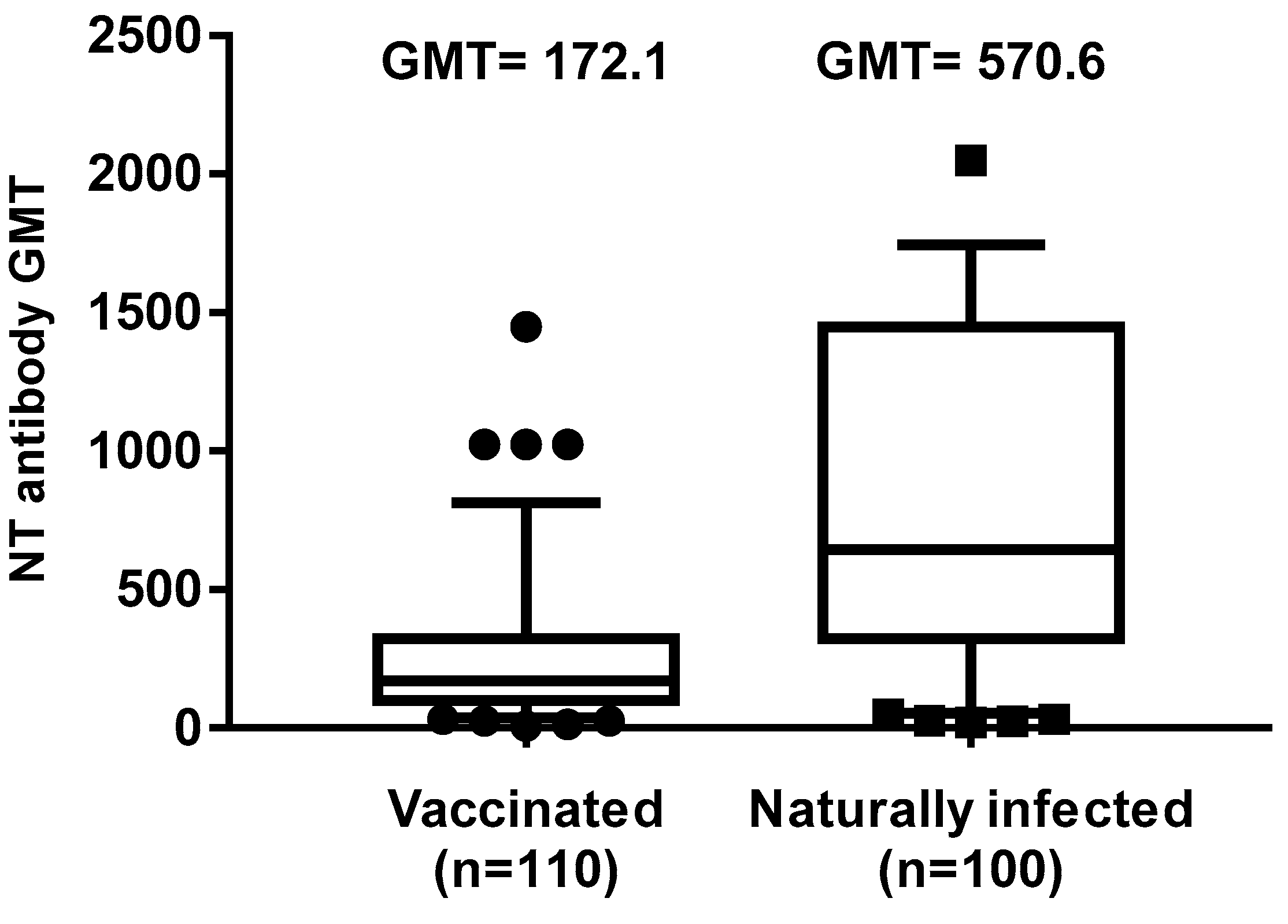
3.4. Evaluation of Neutralizing Ab Titers
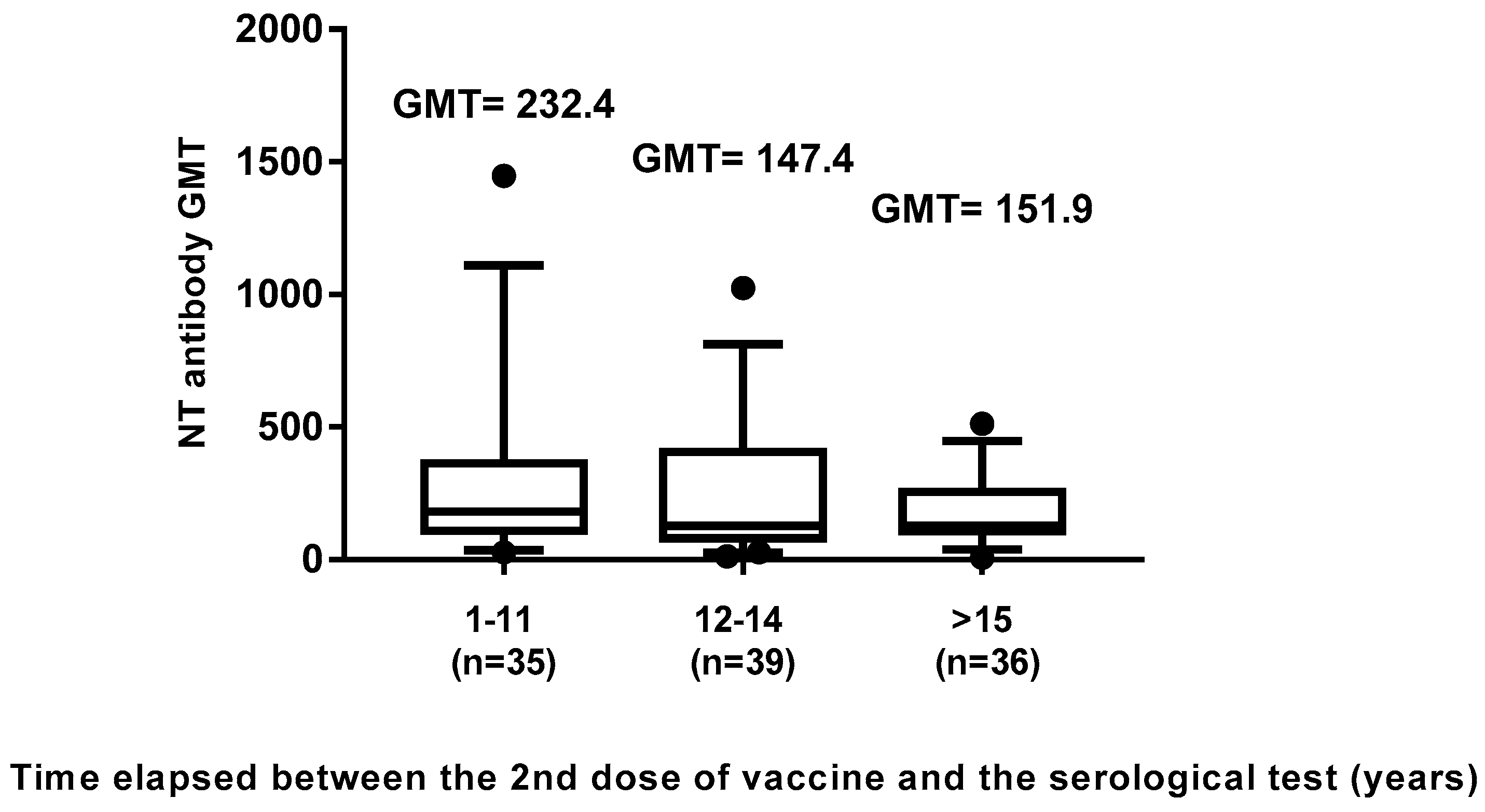
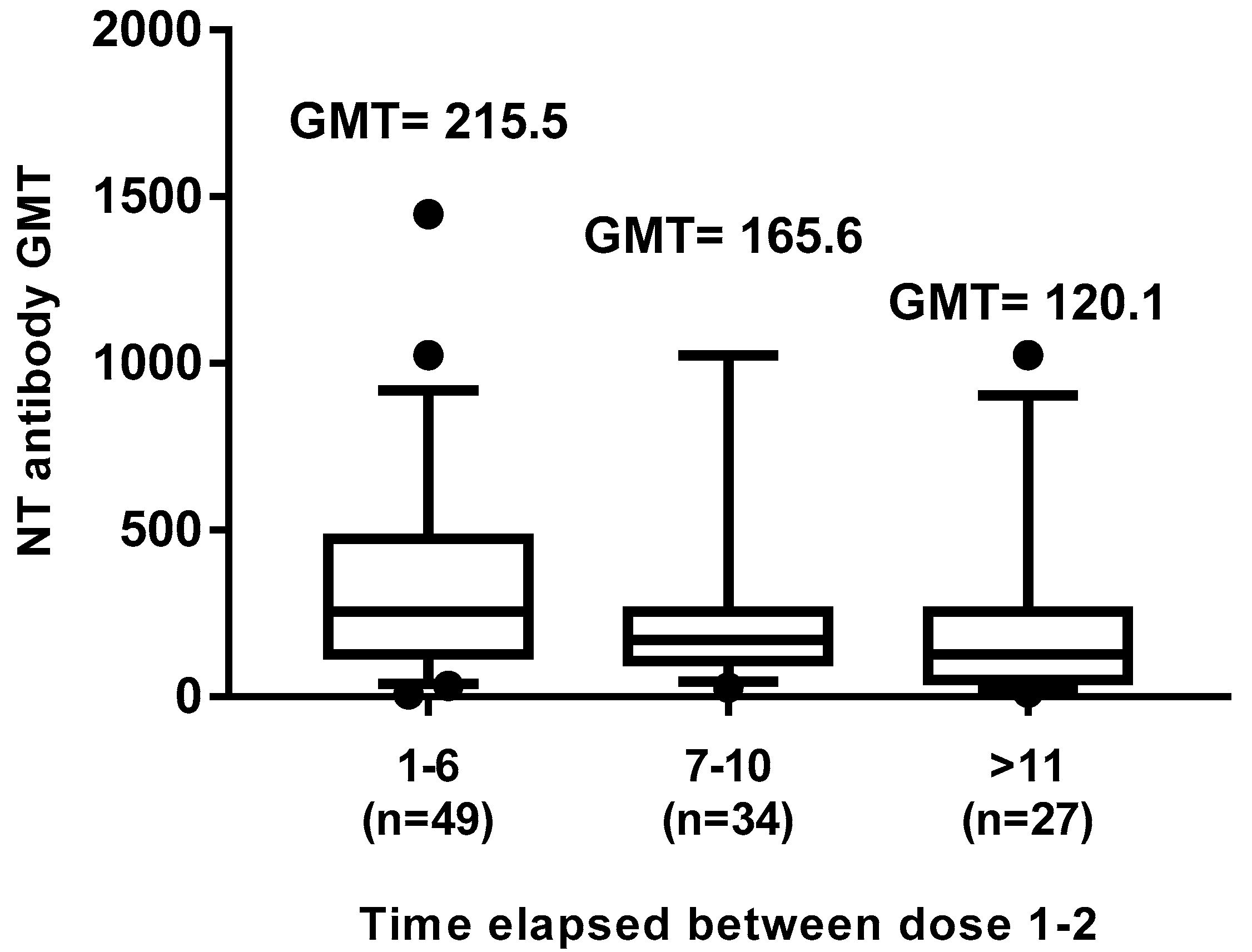
3.5. Decline of Neutralizing Ab Titers
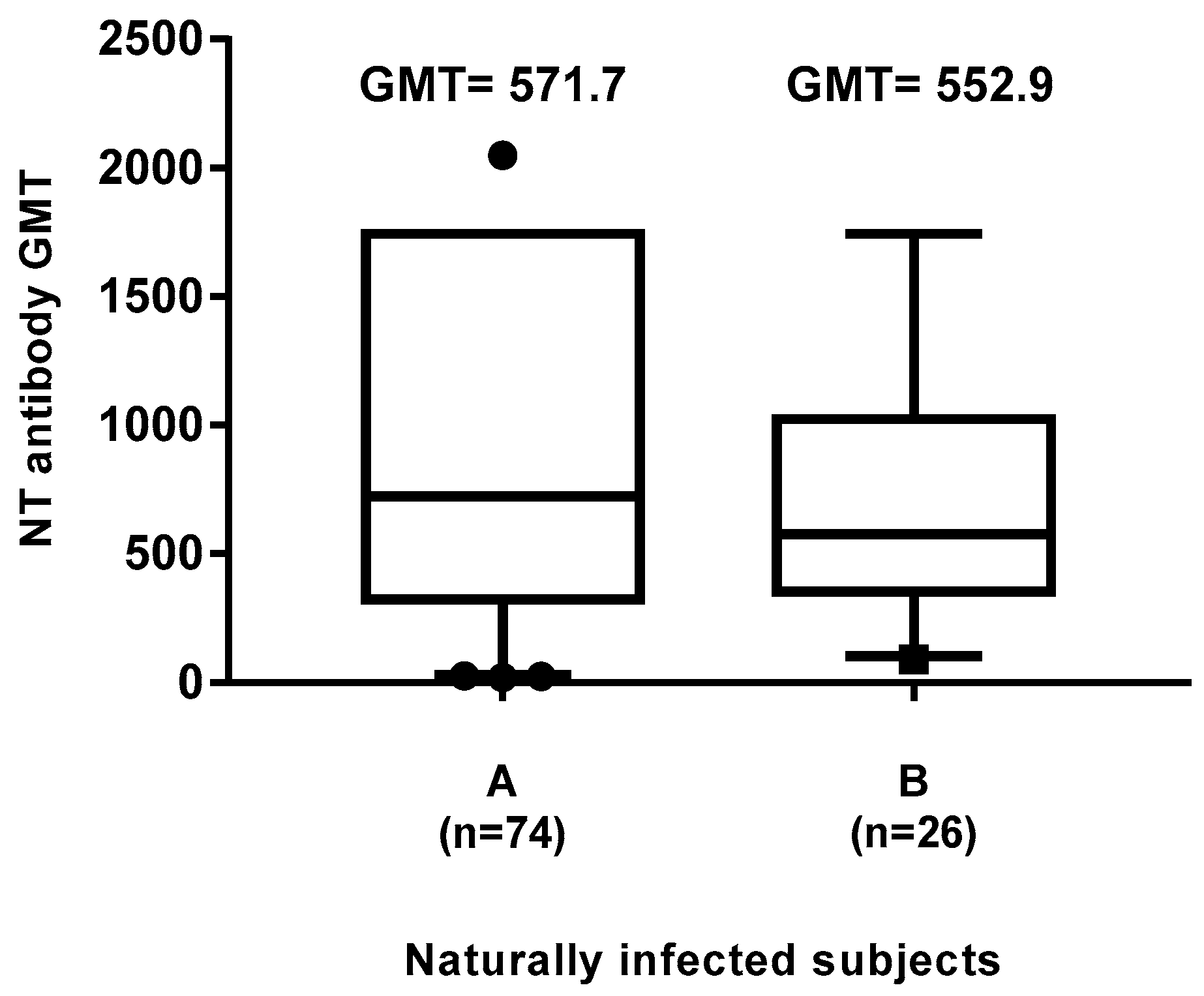
3.6. Neutralizing Antibody GMT in Natural Infected Subjects
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Griffin, D.E. Measles virus. In Fields Virology; Knipe, D.M., Howley, P.M., Eds.; Wolters Kluwer | Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013; Volume 6, pp. 1042–1069. [Google Scholar]
- de Vries, R.D.; Duprex, W.P.; de Swart, R.L. Morbillivirus infections: An introduction. Viruses 2015, 7, 699–706. [Google Scholar] [CrossRef] [PubMed]
- Buchanan, R.; Bonthius, D.J. Measles virus and associated central nervous system sequelae. Semin. Pediatr. Neurol. 2012, 19, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Mina, M.J.; Metcalf, C.J.; de Swart, R.L.; Osterhaus, A.D.; Grenfell, B.T. Long-term measles-induced immunomodulation increases overall childhood infectious disease mortality. Science 2015, 348, 694–699. [Google Scholar] [CrossRef] [PubMed]
- de Vries, R.D.; McQuaid, S.; van Amerongen, G.; Yüksel, S.; Verburgh, R.J.; Osterhaus, A.D.; Duprex, W.P.; de Swart, R.L. Measles Immune Suppression: Lessons from the Macaque Model. PLoS Pathog. 2012, 8. [Google Scholar] [CrossRef] [PubMed]
- de Vries, R.D.; de Swart, R.L.; Lamouille, B.; Astier, A.; Rabourdin-Combe, C. Measles Immune Suppression: Functional Impairment or Numbers Game? PLoS Pathog. 2014, 10, e1004482. [Google Scholar] [CrossRef] [PubMed]
- Laksono, B.M.; de Vries, R.D.; McQuaid, S.; Duprex, W.P.; de Swart, R.L. Measles Virus Host Invasion and Pathogenesis. Viruses 2016, 8. [Google Scholar] [CrossRef] [PubMed]
- Uzicanin, A.; Zimmerman, L. Field effectiveness of live attenuated measles-containing vaccines: A review of published literature. J. Infect. Dis. 2011, 204, 133–148. [Google Scholar] [CrossRef]
- Rota, P.A.; Moss, W.J.; Takeda, M.; de Swart, R.L.; Thompson, K.M.; Goodson, J.L. Measles. Nat. Rev. Dis. Primers 2016, 2. [Google Scholar] [CrossRef]
- Italian Ministry of Health. Circolare n.12 del 13 luglio 1999. Controllo ed eliminazione di morbillo, rosolia e parotite attraverso la vaccinazione. Available online: http://www.salute.gov.it/imgs/C_17_normativa_86_allegato.pdf (accessed on 13 July 1999).
- Italian Ministry of Health. Piano nazionale per l’eliminazione del morbillo e della rosolia congenita. 2003. Available online: http://www.salute.gov.it/imgs/C_17_pubblicazioni_730_allegato.pdf (accessed on 13 November 2003).
- Andrianou, X.D.; Del Manso, M.; Bella, A.; Vescio, M.F.; Baggieri, M.; Rota, M.C.; Pezzotti, P.; Filia, A. Spatiotemporal distribution and determinants of measles incidence during a large outbreak, Italy, September 2016 to July 2018. Euro. Surveill. 2019, 24. [Google Scholar] [CrossRef]
- Italian Ministry of Health. Decree Law 7 June 2017, n. 73, Urgent Provisions on Vaccination Prevention, as Amended by the Conversion Law. Available online: http://www.trovanorme.salute.gov.it/norme/dettaglioAtto?id = 60201 (accessed on 31 July 2017).
- Cocchio, S.; Zanoni, G.; Opri, R.; Russo, F.; Baldo, V.; Collaborative group. A postmarket safety comparison of 2 vaccination strategies for measles, mumps, rubella and varicella in Italy. Hum. Vaccin. Immunother. 2016, 12, 651–654. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Monthly Measles and Rubella Monitoring Report; ECDC: Stockholm, Sweden, 2019; Available online: https://www.ecdc.europa.eu/en/publications-data/monthly-measles-and-rubella-monitoring-report-september-2019 (accessed on 13 September 2019).
- Yeung, L.F.; Lurie, P.; Dayan, G.; Eduardo, E.; Britz, P.H.; Redd, S.B.; Papania, M.J.; Seward, J.F. A limited measles outbreak in a highly vaccinated US boarding school. Pediatrics 2005, 116, 1287–1291. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, R.B.; Ovsyannikova, I.G.; Thomas, A.; Larrabee, B.R.; Rubin, S.; Poland, G.A. Differential durability of immune responses to measles and mumps following MMR vaccination. Vaccine 2019, 37, 1775–1784. [Google Scholar] [CrossRef] [PubMed]
- Carryn, S.; Feyssaguet, M.; Povey, M.; Di Paolo, E. Long-term immunogenicity of measles, mumps and rubella-containing vaccines in healthy young children: A 10-year follow-up. Vaccine 2019, 37, 5323–5331. [Google Scholar] [CrossRef] [PubMed]
- Davidkin, I.; Jokinen, S.; Broman, M.; Leinikki, P.; Peltola, H. Persistence of measles, mumps, and rubella antibodies in an MMR-vaccinated cohort: A 20-year follow-up. J. Infect. Dis. 2008, 197, 950–956. [Google Scholar] [CrossRef] [PubMed]
- Seagle, E.E.; Bednarczyk, R.A.; Hill, T.; Fiebelkorn, A.P.; Hickman, C.J.; Icenogle, J.P.; Belongia, E.A.; McLean, H.Q. Measles, mumps, and rubella antibody patterns of persistence and rate of decline following the second dose of the MMR vaccine. Vaccine 2018, 36, 818–826. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, G.; Frade, J.; Nunes, C.; Mesquita, J.R.; Nascimento, M.S. Persistence of measles antibodies, following changes in the recommended age for the second dose of MMR-vaccine in Portugal. Vaccine 2015, 33, 5057–5063. [Google Scholar] [CrossRef]
- LeBaron, C.W.; Beeler, J.; Sullivan, B.J.; Forghani, B.; Bi, D.; Beck, C.; Audet, S.; Gargiullo, P. Persistence of measles antibodies after 2 doses of measles vaccine in a post-elimination environment. Arch. Pediatr. Adolesc. Med. 2007, 161, 294–301. [Google Scholar] [CrossRef]
- Authorisation no. 9/2014—General Authorisation to Process Personal Data for Scientific Research Purposes. Available online: https://www.gazzettaufficiale.it/atto/serie_generale/caricaDettaglioAtto/originario?atto.dataP bblicazioneGazzetta = 2014-12-30&atto.codiceRedazionale = 14A09916&elenco30giorni = true (accessed on 30 December 2014).
- Law Decree 22 December 2017, No. 219, published in the Official Gazette No. 12 of 16 January 2018. Available online: https://www.gazzettaufficiale.it/eli/gu/2018/01/16/12/sg/pdf (accessed on 16 January 2016).
- Reed, L.J.; Muench, H. A simple method of estimating fifty per cent endpoints. Am. J. Hyg. 1938, 27, 493–497. [Google Scholar]
- Pacenti, M.; Maione, N.; Lavezzo, E.; Franchin, E.; Dal Bello, F.; Gottardello, L.; Barzon, L. Measles Virus Infection and Immunity in a Suboptimal Vaccination Coverage Setting. Vaccines 2019, 7, 199. [Google Scholar] [CrossRef]
- Patel, M.K.; Dumolard, L.; Nedelec, Y.; Sodha, S.V.; Steulet, C.; Gacic-Dobo, M.; Kretsinger, K.; McFarland, J.; Rota, P.A.; Goodson, J.L. Progress Toward Regional Measles Elimination—Worldwide, 2000–2018. MMWR Morb. Mortal. Wkly. Rep. 2019, 68, 1105–1111. [Google Scholar] [CrossRef]
- World Health Organization. Measles Cases Hit Record High in the European Region. 2018. Available online: http://www.euro.who.int/en/media-centre/sections/press-releases/2018/measles-cases-hit-record-high-in-the-european-region (accessed on 20 August 2018).
- World Health Organization. 8th Meeting of the European Regional Verification Commission for Measles and Rubella Elimination (RVC). Available online: http://www.euro.who.int/en/health-topics/communicable-diseases/measles-and-rubella/publications/2019/8th-meeting-of-the-european-regional-verification-commission-for-measles-and-rubella-elimination-rvc-2019 (accessed on 12 June 2019).
- D’Ancona, F.; D’Amario, C.; Maraglino, F.; Rezza, G.; Iannazzo, S. The law on compulsory vaccination in Italy: An update 2 years after the introduction. Euro. Surveill. 2019, 24. [Google Scholar] [CrossRef] [PubMed]
- McLean, H.Q.; Fiebelkorn, A.P.; Temte, J.L.; Wallace, G.S. Centers for Disease Control and Prevention. Prevention of measles, rubella, congenital rubella syndrome, and mumps, 2013: Summary recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm. Rep. 2013, 62, 1–34. [Google Scholar] [PubMed]
- Bianchi, F.P.; Stefanizzi, P.; De Nitto, S.; Larocca, A.M.V.; Germinario, C.; Tafuri, S. Long-term immunogenicity of Measles vaccine: An Italian retrospective cohort study. J. Infect. Dis. 2019. [Google Scholar] [CrossRef] [PubMed]
- Smetana, J.; Chlibek, R.; Hanovcova, I.; Sosovickova, R.; Smetanova, L.; Gal, P.; Dite, P. Decreasing Seroprevalence of Measles Antibodies after Vaccination—Possible Gap in Measles Protection in Adults in the Czech Republic. PLoS ONE 2017, 12, e0170257. [Google Scholar] [CrossRef]
- Christenson, B.; Böttiger, M. Measles antibody: Comparison of long-term vaccination titres, early vaccination titres and naturally acquired immunity to and booster effects on the measles virus. Vaccine 1994, 12, 129–133. [Google Scholar] [CrossRef]
- Modrof, J.; Tille, B.; Farcet, M.R.; McVey, J.; Schreiner, J.A.; Borders, C.M.; Gudino, M.; Fitzgerald, P.; Simon, T.L.; Kreil, T.R. Measles Virus Neutralizing Antibodies in Intravenous Immunoglobulins: Is an Increase by Revaccination of Plasma Donors Possible? J. Infect. Dis. 2017, 216, 977–980. [Google Scholar] [CrossRef]
- Rümke, H.C.; Loch, H.P.; Hoppenbrouwers, K.; Vandermeulen, C.; Malfroot, A.; Helm, K.; Douha, M.; Willems, P. Immunogenicity and safety of a measles-mumps-rubella-varicella vaccine following a 4-week or a 12-month interval between two doses. Vaccine 2011, 29, 3842–3849. [Google Scholar] [CrossRef]
- Middleman, A.B.; Kozinetz, C.A.; Robertson, L.M.; DuRant, R.H.; Emans, S.J. The effect of late doses on the achievement of seroprotection and antibody titer levels with hepatitis b immunization among adolescents. Pediatrics 2001, 107, 1065–1069. [Google Scholar] [CrossRef]
- Sabidó, M.; Gavaldà, L.; Olona, N.; Ramon, J.M. Timing of hepatitis B vaccination: Its effect on vaccine response in health care workers. Vaccine 2007, 25, 7568–7572. [Google Scholar] [CrossRef]
- Griffin, D.E. The Immune Response in Measles: Virus Control, Clearance and Protective Immunity. Viruses 2016, 8, 282. [Google Scholar] [CrossRef]
- Fiebelkorn, A.P.; Coleman, L.A.; Belongia, E.A.; Freeman, S.K.; York, D.; Bi, D.; Kulkarni, A.; Audet, S.; Mercader, S.; McGrew, M.; et al. Measles Virus Neutralizing Antibody Response, Cell-Mediated Immunity, and Immunoglobulin G Antibody Avidity Before and After Receipt of a Third Dose of Measles, Mumps, and Rubella Vaccine in Young Adults. J. Infect. Dis. 2016, 213, 1115–1123. [Google Scholar] [CrossRef]







© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anichini, G.; Gandolfo, C.; Fabrizi, S.; Miceli, G.B.; Terrosi, C.; Gori Savellini, G.; Prathyumnan, S.; Orsi, D.; Battista, G.; Cusi, M.G. Seroprevalence to Measles Virus after Vaccination or Natural Infection in an Adult Population, in Italy. Vaccines 2020, 8, 66. https://doi.org/10.3390/vaccines8010066
Anichini G, Gandolfo C, Fabrizi S, Miceli GB, Terrosi C, Gori Savellini G, Prathyumnan S, Orsi D, Battista G, Cusi MG. Seroprevalence to Measles Virus after Vaccination or Natural Infection in an Adult Population, in Italy. Vaccines. 2020; 8(1):66. https://doi.org/10.3390/vaccines8010066
Chicago/Turabian StyleAnichini, Gabriele, Claudia Gandolfo, Simonetta Fabrizi, Giovan Battista Miceli, Chiara Terrosi, Gianni Gori Savellini, Shibily Prathyumnan, Daniela Orsi, Giuseppe Battista, and Maria Grazia Cusi. 2020. "Seroprevalence to Measles Virus after Vaccination or Natural Infection in an Adult Population, in Italy" Vaccines 8, no. 1: 66. https://doi.org/10.3390/vaccines8010066
APA StyleAnichini, G., Gandolfo, C., Fabrizi, S., Miceli, G. B., Terrosi, C., Gori Savellini, G., Prathyumnan, S., Orsi, D., Battista, G., & Cusi, M. G. (2020). Seroprevalence to Measles Virus after Vaccination or Natural Infection in an Adult Population, in Italy. Vaccines, 8(1), 66. https://doi.org/10.3390/vaccines8010066