A Survey of Vaccine-Induced Measles IgG Antibody Titer to Verify Temporal Changes in Response to Measles Vaccination in Young Adults

 ,
, 
 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Laboratory Methods
2.3. Statistical Analysis
3. Results
3.1. Survey Participants
3.2. Measles-IgG Titer and Temporal Characterization
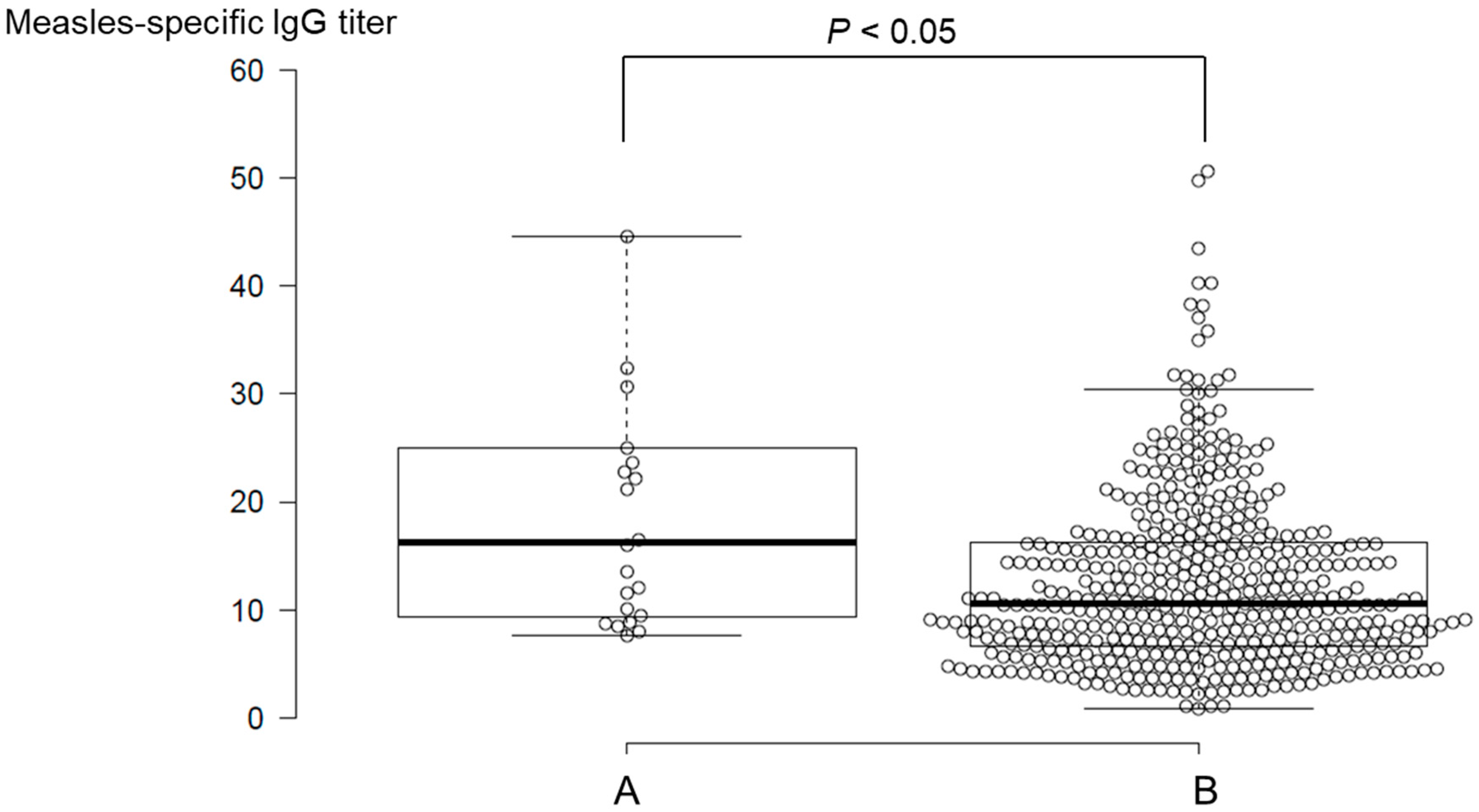
3.3. Divergence of Measles-IgG Antibody Titers by Medical History of Measles
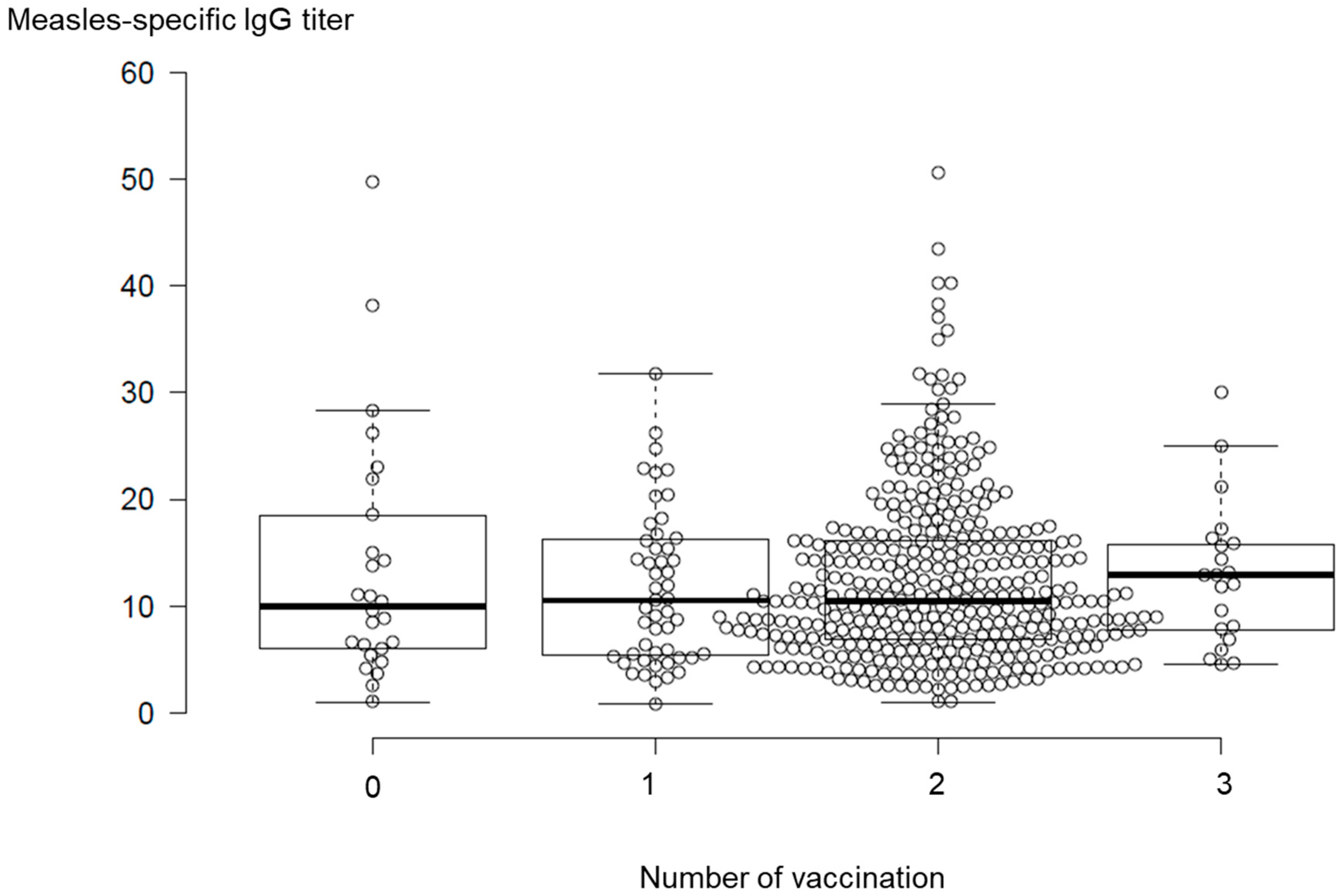
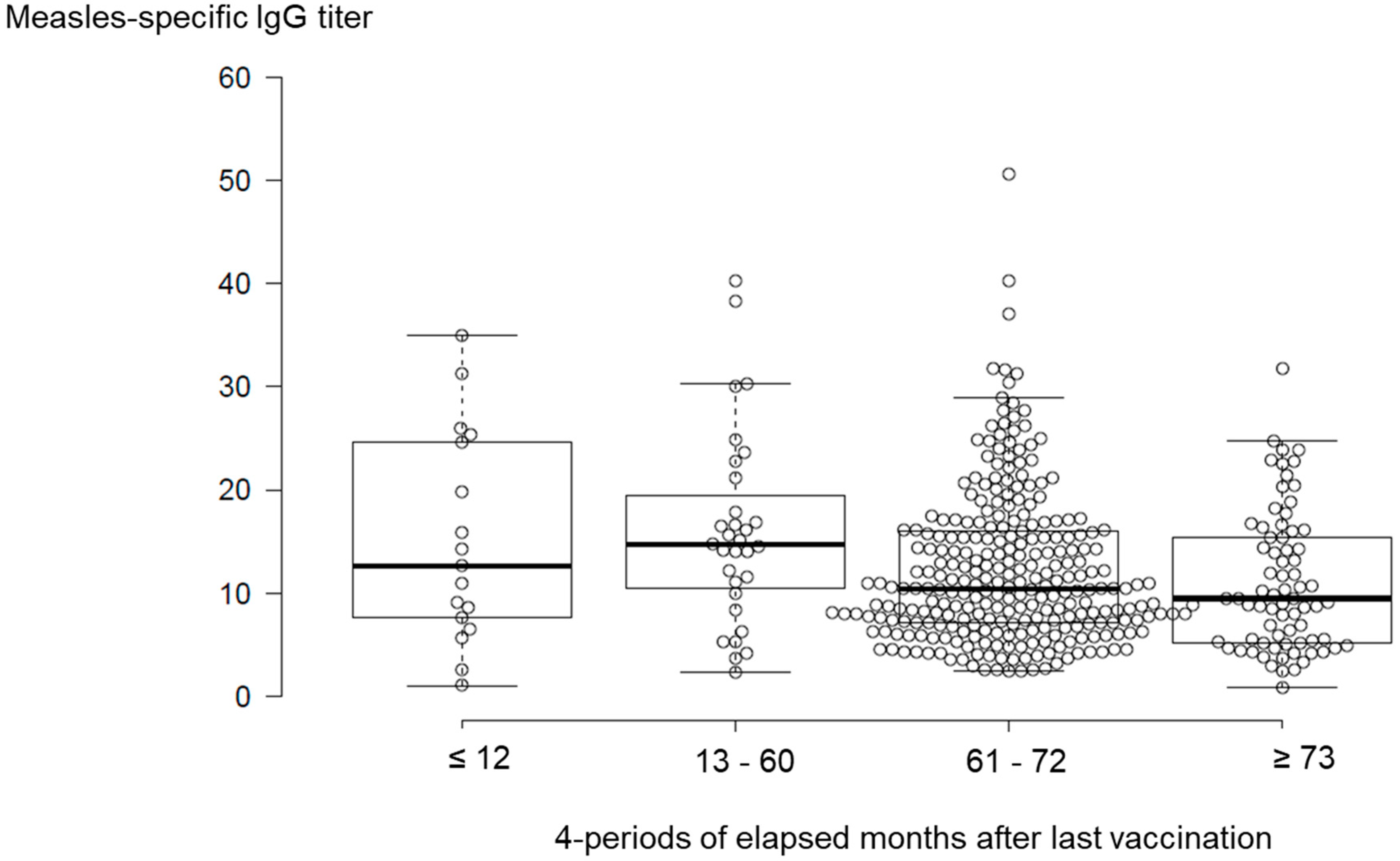
3.4. Temporal Changes in Measles-IgG Antibody Titers
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization Regional Office for the Western Pacific, BruneiDarussalam, Cambodia, Japan verified as achieving measles elimination. 2015. Available online: https://www.who.int/westernpacific/news/detail/27-03-2015-brunei-darussalam-cambodia-japan-verified-as-achieving-measles-elimination (accessed on 17 September 2019).
- National Institute of Infectious Disease, Infectious Disease Surveillance Center. Infectious Diseases Weekly Report; National Institute of Infectious Disease, Infectious Disease Surveillance Center: Shinjuku City, Japan, 2019; Volume 19, pp. 8–9. [Google Scholar]
- Demicheli, V.; Rivetti, A.; Debalini, M.G.; Di Pietrantonj, C. Vaccines for measles, mumps and rubella in children. Cochrane Database Syst. Rev. 2012, 2, CD004407. [Google Scholar] [CrossRef] [PubMed]
- Moss, W.J.; Griffin, D.E. Measles. Lancet 2012, 379, 153–164. [Google Scholar] [CrossRef]
- Ministry of Health, Labor and Welfare. Measles. Available online: https://www.mhlw.go.jp/seisakunitsuite/bunya/kenkou_iryou/kenkou/kekkaku-kansenshou/measles_eng/index.html (accessed on 17 September 2019).
- Tanaka-Taya, K. Progress towards the 2012 measles elimination goal in Japan. Uirusu 2010, 60, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labor and Welfare. Available online: https://www.mhlw.go.jp/bunya/kenkou/kekkaku-kansenshou21/hashika.html (accessed on 17 September 2019).
- Durrheim, D. Measles elimination, immunity, serosurveys, and other immunity gap diagnostic tools. J. Infect. Dis. 2018, 218, 341–343. [Google Scholar] [CrossRef] [PubMed]
- Thompson, K.M.; Odahowski, C.L. Systematic review of measles and rubella serology studies. Risk Anal. 2016, 36, 1459–1486. [Google Scholar] [CrossRef] [PubMed]
- Kumakura, S.; Shibata, H.; Onoda, K.; Nishimura, N.; Matsuda, C.; Hirose, M. Seroprevalence survey on measles, mumps, rubella and varicella antibodies in healthcare workers in Japan: Sex, age, occupational-related differences and vaccine efficacy. Epidemiol. Infect. 2014, 142, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Haralambieva, I.H.; Salk, H.M.; Lambert, N.D.; Ovsyannikova, I.G.; Kennedy, R.B.; Warner, N.D.; Pankratz, V.S.; Poland, G.A. Associations between race, sex and immune response variations to rubella vaccination in two independent cohorts. Vaccine 2014, 32, 1946–1953. [Google Scholar] [CrossRef]
- Voigt, E.A.; Ovsyannikova, I.G.; Haralambieva, I.H.; Kennedy, R.B.; Larrabee, B.R.; Schaid, D.J.; Poland, G.A. Genetically defined race, but not sex, is associated with higher humoral and cellular immune responses to measles vaccination. Vaccine 2016, 34, 4913–4919. [Google Scholar] [CrossRef]
- Hatakeyama, S.; Moriya, K.; Itoyama, S.; Nukui, Y.; Uchida, M.; Shintani, Y.; Morisawa, Y.; Kimura, S. Prevalence of measles, rubella, mumps, and varicella antibodies among healthcare workers in Japan. Infect. Control Hosp Epidemiol. 2004, 25, 591–594. [Google Scholar] [CrossRef]
- Boulton, M.L.; Wang, X.; Zhang, Y.; Montgomery, J.P.; Wagner, A.L.; Carlson, B.F.; Ding, Y.; Li, X.; Gillespie, B.; Su, X. A population profile of measles susceptibility in Tianjin, China. Vaccine 2016, 34, 3037–3043. [Google Scholar] [CrossRef]
- Gohil, D.J.; Kothari, S.T.; Chaudhari, A.B.; Gunale, B.K.; Kulkarni, P.S.; Deshmukh, R.A.; Chowdhary, A.S. Seroprevalence of Measles, Mumps, and Rubella Antibodies in College Students in Mumbai, India. Viral Immunol. 2016, 29, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Takayama, N.; Saika, S.; Ichinohe, S. EIA-IgG antibody measles prevention level estimated from measles neutralizing, particle agglutination and hemagglutination-inhibition antibody titer. Kansenshogaku Zasshi 2009, 83, 519–524. [Google Scholar] [CrossRef] [PubMed][Green Version]
- World Health Organization. Disease outbreak news. Emergencies preparedness, response. Measles–Japan. Available online: https://www.who.int/csr/don/20-june-2018-measles-japan/en/ (accessed on 17 September 2019).
- Komabayashi, K.; Seto, J.; Tanaka, S.; Suzuki, Y.; Ikeda, T.; Onuki, N.; Yamada, K.; Ahiko, T.; Ishikawa, H.; Mizuta, K. The largest measles outbreak, including 38 modified measles and 22 typical measles cases in its elimination era in Yamagata, Japan in 2017. Jpn. J. Infect. Dis. 2018, 71, 413–418. [Google Scholar] [CrossRef] [PubMed]
- Miyoshi, M.; Komagome, R.; Yamaguchi, H.; Ohnishi, A.; Kikuchi, M.; Ishida, S.; Nagano, H.; Okano, M. Detection of measles virus genotypes B3, D4, D5, D8, and H1 in the surveillance system in Hokkaido, Japan, 2006-2015, the last decade toward the elimination. Jpn. J. Infect. Dis. 2017, 70, 317–319. [Google Scholar] [CrossRef] [PubMed]
- Nishiura, H.; Mizumoto, K.; Asai, Y. Assessing the transmission dynamics of measles in Japan in 2016. Epidemics 2017, 20, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, K.; Kinoshita, R.; Yoshii, K.; Akhmetzhanov, A.R.; Jung, S.; Lee, H.; Nishiura, H. An investigation of a measles outbreak in Japan and China, Taiwan, China, March-May 2018. Western Pac. Surveill. Response J. 2018, 9, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Nakatani, H.; Sano, T.; Iuchi, T. Development of vaccination policy in Japan: current issues and policy directions. Jpn. J. Infect. Dis. 2002, 55, 101–111. [Google Scholar]
- Gomi, H.; Takahashi, H. Why is measles still endemic in Japan? Lancet 2004, 364, 328–329. [Google Scholar] [CrossRef]
- Papania, M.J.; Wallace, G.S.; Rota, P.A.; Icenogle, J.P.; Fiebelkorn, A.P.; Armstrong, G.L.; Reef, S.E.; Redd, S.B.; Abernathy, E.S.; Barskey, A.E.; et al. Elimination of endemic measles, rubella, and congenital rubella syndrome from the Western hemisphere: The US experience. JAMA Pediatr. 2014, 168, 148–155. [Google Scholar] [CrossRef]
- Fiebelkorn, A.P.; Redd, S.B.; Gastañaduy, P.A.; Clemmons, N.; Rota, P.A.; Rota, J.S.; Bellini, W.J.; Wallace, G.S. A comparison of postelimination measles epidemiology in the United States, 2009–2014 versus 2001–2008. J. Pediatric Infect. Dis. Soc. 2017, 6, 40–48. [Google Scholar] [CrossRef][Green Version]
- Ehresmann, K.; Banerjee, E.; Kenyon, C.; Christianson, B.; Griffith, J.; Heath, J.; Roddy, M.; MDH IDEPC Measles Outbreak Team. Response to “It could have been much worse: The Minnesota measles outbreak of 2017”. Vaccine 2019, 37, 683–684. [Google Scholar] [CrossRef] [PubMed]
- Clemmons, N.S.; Wallace, G.S.; Patel, M.; Gastañaduy, P.A. Incidence of measles in the United States, 2001-2015. JAMA 2017, 318, 1279–1281. [Google Scholar] [CrossRef] [PubMed]
- Nelson, R. US measles outbreak concentrated among unvaccinated children. Lancet Infect Dis. 2019, 19, 248. [Google Scholar] [CrossRef]
- Clifford, H.D.; Hayden, C.M.; Khoo, S.K.; Naniche, D.; Mandomando, I.M.; Zhang, G.; Richmond, P.; Le Souëf, P.N. Polymorphisms in key innate immune genes and their effects on measles vaccine responses and vaccine failure in children from Mozambique. Vaccine 2012, 30, 6180–6185. [Google Scholar] [CrossRef] [PubMed]
- Moss, W.J.; Strebel, P. Biological feasibility of measles eradication. J. Infect. Dis. 2011, 204, S47–S53. [Google Scholar] [CrossRef] [PubMed]
- Meissner, H.C.; Strebel, P.M.; Orenstein, W.A. Measles vaccines and the potential for worldwide eradication of measles. Pediatrics 2004, 114, 1065–1069. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, T.; Uchiyama-Nakamura, F.; Sugata-Tsubaki, A.; Yamada, Y.; Uno, K.; Kasahara, K.; Maeda, K.; Konishi, M.; Mikasa, K. Antibody response to live attenuated vaccines in adults in Japan. Open Med. (Wars) 2016, 11, 482–488. [Google Scholar] [CrossRef] [PubMed]
- Kakoulidou, M.; Ingelman-Sundberg, H.; Johansson, E.; Cagigi, A.; Farouk, S.E.; Nilsson, A.; Johansen, K. Kinetics of antibody and memory B cell responses after MMR immunization in children and young adults. Vaccine 2013, 31, 711–717. [Google Scholar] [CrossRef]
- Kennedy, R.B.; Ovsyannikova, I.G.; Thomas, A.; Larrabee, B.R.; Rubin, S.; Poland, G.A. Differential durability of immune responses to measles and mumps following MMR vaccination. Vaccine 2019, 37, 1775–1784. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Number | Percentage |
|---|---|---|
| Total | 506 | 100 |
| Age, Y | ||
| Range | ||
| 17–18 | 407 | 80 |
| 19–20 | 97 | 19 |
| ≥21 | 2 | 0 |
| Sex | ||
| Female | 160 | 32 |
| Male | 346 | 68 |
| Vaccination | ||
| 1 | 56 | 11 |
| 2 | 399 | 79 |
| 3 | 21 | 4 |
| Unvaccinated | 30 | 6 |
| Medical history of measles | 22 | 4 |
| Item | Mean | Range | Number |
|---|---|---|---|
| Measles-specific IgG titer | 13.4 | 0.8–128 | 506 |
| 1st vaccination month | 23.6 | 11–263 | 476 |
| 2nd vaccination month | 152.2 | 16–265 | 420 |
| 3rd vaccination month | 156.0 | 53–238 | 21 |
| Elapsed months after last vaccination | 83.3 | 0–237 | 476 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sasaki, H.; Fukunaga, T.; Asano, A.; Suzuki, Y.; Nakanishi, Y.; Kondo, J.; Ishikawa, H.; Shibata, N. A Survey of Vaccine-Induced Measles IgG Antibody Titer to Verify Temporal Changes in Response to Measles Vaccination in Young Adults. Vaccines 2019, 7, 118. https://doi.org/10.3390/vaccines7030118
Sasaki H, Fukunaga T, Asano A, Suzuki Y, Nakanishi Y, Kondo J, Ishikawa H, Shibata N. A Survey of Vaccine-Induced Measles IgG Antibody Titer to Verify Temporal Changes in Response to Measles Vaccination in Young Adults. Vaccines. 2019; 7(3):118. https://doi.org/10.3390/vaccines7030118
Chicago/Turabian StyleSasaki, Hiraku, Tomoko Fukunaga, Ai Asano, Yoshio Suzuki, Yuko Nakanishi, Junzi Kondo, Hiroki Ishikawa, and Nobuto Shibata. 2019. "A Survey of Vaccine-Induced Measles IgG Antibody Titer to Verify Temporal Changes in Response to Measles Vaccination in Young Adults" Vaccines 7, no. 3: 118. https://doi.org/10.3390/vaccines7030118
APA StyleSasaki, H., Fukunaga, T., Asano, A., Suzuki, Y., Nakanishi, Y., Kondo, J., Ishikawa, H., & Shibata, N. (2019). A Survey of Vaccine-Induced Measles IgG Antibody Titer to Verify Temporal Changes in Response to Measles Vaccination in Young Adults. Vaccines, 7(3), 118. https://doi.org/10.3390/vaccines7030118